201 Endocrine 1

of 99
Transcript of 201 Endocrine 1
-
7/29/2019 201 Endocrine 1
1/99
Chapter 11
Endocrine Glands -
Secretion & Action of Hormones
11-1
-
7/29/2019 201 Endocrine 1
2/99
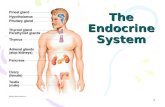
Endocrine Glands
Are ductless & secretehormones into
bloodstream
Hormones go to targetcells that containreceptor proteins for it
Neurohormones aresecreted into blood byspecialized neurons
Hormones affect
metabolism of targets
Fig 11.1
11-4
-
7/29/2019 201 Endocrine 1
3/99
Chemical Classification of Hormones
Amine hormones are derived from tyrosine or tryptophan
Include NE, Epi, thyroxine, melatonin
Polypeptide/protein hormones are chains of amino acids
Include ADH, GH, insulin, oxytocin, glucagon, ACTH, PTH
Glycoproteins
Long polypeptide bound to a carbohydrate group
Include LH, FSH, TSH
Steroids are lipids derived from cholesterol
Include testosterone, estrogen, progesterone & cortisol
11-7
-
7/29/2019 201 Endocrine 1
4/99
Common Aspects of Neural & Endocrine
Regulation
Both NS & endocrine system use chemicals tocommunicate
Difference between NTs & hormones is transport inblood & more diversity of effects in hormone targets
Some chemicals are used as hormones & NTs
Targets for both NTs & hormones must have
specific receptor proteins
Must be way to rapidly inactivate both
11-12
-
7/29/2019 201 Endocrine 1
5/99
A tissue usually responds to # of hormones 2 hormones are synergistic if work together to
produce an effect
Produce a larger effect together than individual effectsadded together
Effects of Epi and NE on heart rate
A hormone haspermissiveeffect if it enhances
responsiveness of a target organ to 2nd hormone
If action of 1 hormone inhibits effect of another, it isantagonistic
Hormone Interactions
11-13
-
7/29/2019 201 Endocrine 1
6/99
Hormone Levels & Tissue Responses
Half-life is time required for blood level to bereduced by half
Ranges from mins to hrs for most (days for thyroidhormones)
Normal tissue responses are produced only whenhormones are in physiological range
High (pharmacological) doses can cause # of sideeffects
Probably by binding to receptors of other hormones
11-14
-
7/29/2019 201 Endocrine 1
7/99
Priming effect (upregulation) occurs when a hormoneinduces more of its own receptors in target cells
Results in greater response in target cell
Desensitization (downregulation) occurs after long exposureto high levels of polypeptide hormone
Subsequent exposure to this hormone produces a lesser response
Due to decrease in # of receptors on targets
Most peptide hormones havepulsatilesecretion which preventsdownregulation
Hormone Levels & Tissue Responses continued
11-15
-
7/29/2019 201 Endocrine 1
8/99
Mechanisms of Hormone Action
11-16
-
7/29/2019 201 Endocrine 1
9/99
Mechanisms of Hormone Action
Target cell receptors show specificity, high affinity,& low capacity for a hormone
Lipid hormones have receptors in target's cytoplasm
&/or nucleus because can diffuse thru plasmamembrane
Receptors for water-solubles are on surface of targetcell
11-17
-
7/29/2019 201 Endocrine 1
10/99
Hormones That Bind to Nuclear Receptor
Proteins
Lipid hormones travelin blood attached tocarrier proteins
They dissociate from
carriers to pass thruplasma membrane oftarget
Receptors are callednuclear hormone receptors
Fig 11.4
11-18
-
7/29/2019 201 Endocrine 1
11/99
Nuclear Hormone Receptors
Serve as transcription factors when bound to hormone
ligands
Activate transcription
Constitute a "superfamily" composed of steroid family &thyroid hormone family (which includes vitamin D &retinoic acid)
11-19
-
7/29/2019 201 Endocrine 1
12/99
Nuclear Hormone Receptors
Have ligand (hormone)-binding & DNA-binding domains Binds hormone & translocates to nucleus
Binds to hormone-response element (HRE) on DNA located adjacent to targetgene
Fig 11.5
11-20
-
7/29/2019 201 Endocrine 1
13/99
Fig. 11.6
-
7/29/2019 201 Endocrine 1
14/99
Mechanism of Thyroid Hormone Action
continued
T3 & receptor bind to1 half-site
Other half-site bindsretinoic acid
Two partners formheterodimerthatactivates HRE
Stimulates
transcription of targetgene
Fig 11.7
11-23
-
7/29/2019 201 Endocrine 1
15/99
Hormones That Use 2nd Messengers
Water soluble hormones use cell surface receptorsbecause cannot pass through plasma membrane
Actions are mediated by 2nd messengersHormone is extracellular signal; 2nd messenger carries
signal from receptor to inside of cell
11-24
-
7/29/2019 201 Endocrine 1
16/99
Mediates effects of many polypeptide & glycoprotein hormones
Hormone binds to receptor causing dissociation of a G-protein subunit
Adenylate Cyclase-cAMP
Fig 11.8
11-25
-
7/29/2019 201 Endocrine 1
17/99
G-protein subunit binds to & activates adenylate cyclase Which converts ATP into cAMP cAMP attaches to inhibitory subunit ofprotein kinase
Adenylate Cyclase-cAMP continued
Fig 11.8
11-26
-
7/29/2019 201 Endocrine 1
18/99
Inhibitory subunit dissociates, activating protein kinase
Which phosphorylates enzymes that produce hormones effects
cAMP inactivated byphosphodiesterase
Adenylate Cyclase-cAMP continued
Fig 11.8
11-27
-
7/29/2019 201 Endocrine 1
19/99
-
7/29/2019 201 Endocrine 1
20/99
Pituitary Gland
11-34
-
7/29/2019 201 Endocrine 1
21/99
Pituitary Gland
Pituitary gland is located beneath hypothalamus at base of forebrain
Fig 8.16
11-35
-
7/29/2019 201 Endocrine 1
22/99
Pituitary Gland continued
Is structurally &functionally divided intoanterior & posterior lobes
Hangs below hypothalamusby infundibulum
Anterior produces ownhormones Controlled by hypothalamus
Posterior stores & releaseshormones made inhypothalamus
Fig 11.1211-36
-
7/29/2019 201 Endocrine 1
23/99
Anterior Pituitary
Secretes 6 trophichormones that
maintain size oftargets
High blood levelscause target to
hypertrophy Low levels cause
atrophy
11-37
-
7/29/2019 201 Endocrine 1
24/99
Anterior Pituitary continued
Growth hormone (GH) promotes growth, protein synthesis, &movement of amino acids into cells
Thyroid stimulating hormone (TSH) stimulates thyroid to produce &
secrete T4 & T3 Adrenocorticotrophic hormone (ACTH) stimulates adrenal
cortex to secrete cortisol, aldosterone
Follicle stimulating hormone (FSH) stimulates growth ofovarian follicles & sperm production
Luteinizinghormone (LH) causes ovulation & secretion oftestosterone in testes
Prolactin (PRL) stimulates milk production by mammaryglands
11-38
-
7/29/2019 201 Endocrine 1
25/99
Anterior Pituitary continued
Release of Anterior Pituitary hormones is controlledby hypothalamic releasing & inhibitingfactors & byfeedbackfrom levels of target gland hormones
11-39
-
7/29/2019 201 Endocrine 1
26/99
Anterior Pituitary continued
Releasing & inhibitinghormones fromhypothalamus arereleased from axonendings into capillary
bed in median eminence
Carried by hypothalamo-hypophyseal portal systemdirectly to anothercapillary bed in A. Pit.
Diffuse into A. Pit. ®ulate secretion of itshormones
Fig 11.15
11-40
-
7/29/2019 201 Endocrine 1
27/99
Feedback Control of Anterior Pituitary Involves short feedbackloop in which retrograde
flow of blood & hormonesfrom A. Pit. tohypothalamus inhibits
secretion of releasinghormone
Involves negative feedbackof target gland hormones
& during menstrual cycle,estrogen stimulates LHsurge bypositive feedback
Fig 11.17
11-41
Hi h B i F i & A i Pi i
-
7/29/2019 201 Endocrine 1
28/99
Higher Brain Function & Anterior Pituitary
Secretion
Hypothalamus receives input from higher braincenters that can affect A. Pit. secretion
E.g. psychological stress affects circadian rhythms,
menstrual cycle, & adrenal hormones
11-42
-
7/29/2019 201 Endocrine 1
29/99
Growth Hormone Secretion
Is from anterior pituitary; stimulated by GHRH, &inhibited by somatostatin, from hypothalamus
Follows a circadian pattern--is greater during sleep& lower during waking hours
Stimulates growth in children & adolescents
Has important metabolic effects in adults
Is stimulated by increased blood amino acids &decreased blood glucose
Is increased during fasting
Stimulates protein synthesis, fat breakdown, & decreases
glucose use by most tissues 19-61
-
7/29/2019 201 Endocrine 1
30/99
Growth Hormone (GH or somatotropin)
Stimulates uptake of amino acids; proteinsynthesis; growth in most tissues.
Stimulates breakdown of fats to be used as
an energy source but stimulates synthesis ofglycogen: glucose sparing (diabetogenic)
Promotes bone and cartilage growth
Regulates blood levels of nutrients after ameal and during periods of fasting
Stimulates glucose synthesis by liver
-
7/29/2019 201 Endocrine 1
31/99
Are similar to pro-insulin; produced by many tissues Are called somatomedins because mediate many of
GH's effects
Liver produces & secretes IGF-1 in response to GHIGF-1 in turn stimulates cell division & growth of
cartilage
These actions are supported by IGF-2 which has more insulin-
like actions Do not mediate effects of GH on lipolysis & glucose
sparing (i.e. metabolic effects)
Insulin-like Growth Factors (IGFs)
19-62
-
7/29/2019 201 Endocrine 1
32/99
Figure 16.6
Metabolic Action of Growth
Hormone
-
7/29/2019 201 Endocrine 1
33/99
Growth Hormone & Body Growth
Growth of skeleton occurs first as growth ofcartilage at epiphyseal discs which then becomeconverted to bone
Mediated by IGF-1 & 2 which stimulate chondrocytesto divide & secrete more cartilaginous matrix
Growth stops when epiphyseal discs are ossified
Gigantism produced by excess GH secretion in
children Dwarfism caused by inadequate secretion of GH
during childhood
19-64
-
7/29/2019 201 Endocrine 1
34/99
Growth Hormone & Body Growth
Excess GH secretion inadults, after epiphysealdiscs are ossified,results in acromegaly
There is no increase inheight
However soft tissue stillgrows
Causing elongation of
jaw, deformities in hands,feet, & bones of face
Fig 19.18 19-65
-
7/29/2019 201 Endocrine 1
35/99
Growth Hormone Stimulation:functions in
regulating growth, tissue maintenance, metabolismGHRHfrom hypothalamus causes release of
Growth hormonefrom anterior pituitary effects
Target tissues: most tissues of the body
Direct effect: GH binds to receptors on cells and causeschanges within the cells. Increased lipolysis and decreaseduse of glucose for energy
Indirect effect: causes liver and skeletal muscle to produce
somatomedins; e.g., insulinlike growth factors (IGFs) Insulinlike growth factors: bind to receptors on
membranes of target cells. Stimulate growth incartilage, bone; increased synthesis of proteins inskeletal muscle.
-
7/29/2019 201 Endocrine 1
36/99
Regulation of GH Secretion
1. Stress and decreased glucose
levels increase release ofGHRH and decreased re-
lease of GHIH.
2. GHRH and GHIN travel via
the hypothalamo-hypophyseal
portal system to ant. pituitary
3. Increased GHRH and reduced
GHIH act on AP and result in
increased GH secretion.
4. GH acts on target tissues.
5. Increasing GH levels have neg
feedback effect on hypothala.
-
7/29/2019 201 Endocrine 1
37/99
Growth Hormone: Inhibition
Hypothalamus produces growth hormone inhibitinghormone (GHIH = somatostatin)
Inhibits production of GH by anterior pituitary.
GHRH secretion in response to low blood glucose, stress,increase in certain a.a.
GHIH secretions in response to high blood glucose.
Peak GH levels during deep sleep; levels lower at other
times of day. Hyposecretion of GH may result in dwarfism
Hypersecretion may result ingiantism oracromegaly de-
pending on ossification of epiphyseal plates
P i Pi i
-
7/29/2019 201 Endocrine 1
38/99
Posterior Pituitary
Stores & releases 2 hormones produced inhypothalamus:
Antidiuretic hormone (ADH/vasopressin) whichpromotes H20 conservation by kidneys
Oxytocin which stimulates contractions of uterus duringparturition
& contractions of mammary gland alveoli for milk-ejectionreflex
11-43
-
7/29/2019 201 Endocrine 1
39/99
Hypothalamic Control of Posterior Pituitary
Supraoptic nuclei ofhypothalamus produceADH
Paraventricular nucleiproduce oxytocin
Both transported alonghypothalamo-hypophysealtract to posterior pituitary
Release controlled inhypothalamus byneuroendocrine reflexes
Fig 11.13 11-44
-
7/29/2019 201 Endocrine 1
40/99
Thyroid Gland
11-51
-
7/29/2019 201 Endocrine 1
41/99
Thyroid Gland
Is located just
below the larynx Secretes T4 & T3
which set BMR &
are needed forgrowth,
development
11-52
-
7/29/2019 201 Endocrine 1
42/99
Thyroid Gland Consists of microscopic thyroid follicles
Outer layer is follicle cells that synthesize T4
Interior filled with colloid, a protein-rich fluid
11-53
Production of Thyroid Hormones
-
7/29/2019 201 Endocrine 1
43/99
Production of Thyroid Hormones
Iodide (I-) in blood isactively transported intofollicles & secreted intocolloid
Where it is oxidized to
iodine (I2) & attached totyrosines ofthyroglobulin
A large storage molecule forT4 & T3
TSH stimulates hydrolysis
of T4 & T3s fromthyroglobulin & thensecretion
Fig 11.23
11-54
-
7/29/2019 201 Endocrine 1
44/99
Thyroid Hormones Produced by follicular cells
Triiodothyronine orT3-less produced Tetraiodothyronine orT4 orthyroxine-more
99.6% of thyroxine in the blood is bound to thyroxine-binding globulin (TBG) from the liver. Rest is free.
TBG has a higher affinity for T4
than for T3
; amt of freeunbound T3 in plasma is 10xs greater than free T4.
Only free thyroxine and T3 can enter cells; bound-thyroxine serves as a reservoir of this hormone
33-40% of T4 converted to T3 in cells: T3 more potent
Bind with intracellular receptormolecules and initiatenew protein synthesis
Increase rate of glucose, fat, protein metabolism inmany tissues thus increasing body temperature
Normal growth of many tissues dependent on presence
of thyroid hormones.
-
7/29/2019 201 Endocrine 1
45/99
Effects of T3 and T4
1. Maintain normal rate of metabolism.
2. Increase the rate at which glucose, fat, and protein are meta-bolized.
3. Increase the activity of Na+-K+ pump which increases body
temperature (calorigenic effect)
4. Can alter the number and activity of mitochondria resulting in
greater ATP synthesis and heat production.
5. Normal growth and maturation of bone, hair, teeth, c.t., and
nervous tissue require thyroid hormone.
6. Both T3 and T4 play a permissive role for GH and GH does not
have its normal effect on tissues if T3 and T4 are lacking.7. See Table 18.4 for effects of hypo- and hypersecretion
Diseases of the Thyroid Goiter
-
7/29/2019 201 Endocrine 1
46/99
Diseases of the Thyroid - Goiter
In absence of sufficient
dietary iodide, T4 & T3
cannot be made & levels
are low
Low T4 & T3dont providenegative feedback & TSH
levels go up
Because TSH is a trophic
hormone, thyroid gland
grows
Resulting in a goiter
Fig 11.2511-55
-
7/29/2019 201 Endocrine 1
47/99
People with inadequate T4 & T3 levels are
hypothyroid
Have low BMR, weight gain, lethargy, cold intolerance
& myxedema = puffy face, hands, feet
During fetal development hypothyroidism can cause
cretenism (severe mental retardation)
Diseases of the Thyroid - Hypothyroidism
11-56
-
7/29/2019 201 Endocrine 1
48/99
Goiters are also produced by Grave's disease
Autoimmune disease where antibodies act like TSH &
stimulate thyroid gland to grow & oversecrete =
hyperthyroidism Characterized by exopthalmos, weight loss, heat intolerance,
irritability, high BMR
Diseases of the Thyroid - Hyperthyroidism
11-57
-
7/29/2019 201 Endocrine 1
49/99
11-58
Calcitonin
-
7/29/2019 201 Endocrine 1
50/99
Calcitonin
Secreted by C cells of thyroid gland
Works with PTH & 1,25 Vit D3 to regulate bloodCa2+ levels
Stimulated by increased plasma Ca2+
Inhibits activity of osteoclasts
Stimulates urinary excretion of Ca2+ & P043- by
inhibiting reabsorption
Physiological significance in adults is notunderstood
19-72
Parathyroid Glands
-
7/29/2019 201 Endocrine 1
51/99
Parathyroid Glands
Are 4 glandsembedded in laterallobes of thyroid gland
Secrete Parathyroidhormone (PTH)
Most importanthormone for control of
blood Ca2+
levels
Fig 11.28
11-59
Parathyroid Hormone (PTH)
-
7/29/2019 201 Endocrine 1
52/99
Parathyroid Hormone (PTH)
Secreted by parathyroid glands
Is most important hormone in control of Ca2+ levels
Release is stimulated by low blood Ca2+ levels
Stimulates osteoclasts to reabsorb bone
Stimulates kidneys to reabsorb Ca2+ from filtrate, & inhibits
reabsorption of P043-
Promotes formation of 1,25 Vit D3 that stimulates Ca2+absorption by intestines
Many cancers secrete PTH-related protein that interacts
with PTH receptors producing hypercalcemia19-71
Parathyroid Hormone
-
7/29/2019 201 Endocrine 1
53/99
Parathyroid Hormone
Release stimulated bydecreased blood Ca2+
Acts on bones, kidney,& intestines to increase
blood Ca2+ levels
Fig 11.29
11-60
Effects of Parathyroid Hormone
-
7/29/2019 201 Endocrine 1
54/99
Figure 16.11
Effects of Parathyroid Hormone
-
7/29/2019 201 Endocrine 1
55/99
1 25 Vitamin D
-
7/29/2019 201 Endocrine 1
56/99
1,25 Vitamin D3
Synthesis begins in skin when cholesterol derivative is converted to
Vit D3 by sunlight
Fig 19.21
19-75
1 25 Vitamin D
-
7/29/2019 201 Endocrine 1
57/99
1,25 Vitamin D3continued
Directly stimulates intestinal absorption of Ca2+ &P04
3-
When Ca2+ intake is inadequate, directly stimulatesbone reabsorption
Stimulates kidney to reabsorb Ca2+ and P043
Simultaneously raising Ca2+ & P043- results in increased
tendency of these to precipitate as hydroxyapatite
Stimulated by PTH Inadequate Vit D in diet & body causes
osteomalacia & rickets (loss of bone calcification)
19-76
Overview of Hormonal Control of Ca2+
-
7/29/2019 201 Endocrine 1
58/99
Overview of Hormonal Control of Ca Fig 19.23 Fig 19.24
19-77
-
7/29/2019 201 Endocrine 1
59/99
Adrenal Gland
11-45
Adrenal Glands
-
7/29/2019 201 Endocrine 1
60/99
Adrenal Glands
Sit on top ofkidneys
Each consists ofouter cortex &inner medulla
2 arise differentlyduring
development
Fig 11.18
11-46
Adrenal Glands
-
7/29/2019 201 Endocrine 1
61/99
Adrenal Glands
Medulla synthesizes & secretes 80% Epi & 20% NE Controlled by sympathetic
Cortex is controlled by ACTH & secretes:
Cortisol which inhibits glucose utilization & stimulates
gluconeogenesis Aldosterone which stimulate kidneys to reabsorb Na+ and
secrete K+
& some supplementary sex steroids
11-47
Adrenal Medulla
-
7/29/2019 201 Endocrine 1
62/99
Adrenal Medulla
Hormonal effects of Epi last 10X longer than NE
Innervated by preganglionic Symp fibers
Activated during "fight or flight" response
Causes:
Increased respiratory rate
Increased HR & cardiac output
General vasoconstriction which increases venous return Glycogenolysis & lipolysis
11-49
Effects of Epinephrine Secretion from
-
7/29/2019 201 Endocrine 1
63/99
Effects of Epinephrine Secretion from
Adrenal Medulla
Metabolic Effects of Epi & Norepi
-
7/29/2019 201 Endocrine 1
64/99
Metabolic Effects of Epi & Norepi
Are similar to glucagon, stimulating glycogenolysis &lipolysis
Fig 19.15
19-57
H f Ad l C t
-
7/29/2019 201 Endocrine 1
65/99
Hormones of Adrenal Cortex
Mineralocorticoids: Zona glomerulosa
Aldosterone produced in greatest amounts. Increasesrate of sodium reabsorption by kidneys increasingsodium blood levels
Glucocorticoids: Zona fasciculata
Cortisol is major hormone. Increases fat and proteinbreakdown, increases glucose synthesis, decreasesinflammatory response
Androgens: Zona reticularis
Weak androgens secreted then converted to testosteroneby peripheral tissues. Stimulate pubic and axillary hairgrowth and sexual drive in females
-
7/29/2019 201 Endocrine 1
66/99
Regulation of Cortisol Secretion
-
7/29/2019 201 Endocrine 1
67/99
Help the body resist stress by:
Keeping blood sugar levels relatively constant
Maintaining blood volume and preventing water shift into tissue
Cortisol provokes: Gluconeogenesis (formation of glucose from noncarbohydrates)
Rises in blood glucose, fatty acids, and amino acids
Glucocorticoids (Cortisol)
Metabolic Effects of Cortisol
-
7/29/2019 201 Endocrine 1
68/99
Metabolic Effects of Cortisol
Cortisol is secreted in response to ACTH
Which is often released in response to stress, including
fasting & exercise
Where it supports effects of glucagon
Promotes lipolysis, ketogenesis, & protein breakdown
Protein breakdown increases amino acid levels for use in
gluconeogenesis in liver
19-58
Metabolic Effects of Cortisol continued
-
7/29/2019 201 Endocrine 1
69/99
Fig 19.16
Metabolic Effects of Cortisol continued
19-59
-
7/29/2019 201 Endocrine 1
70/99
Figure 16.15
Stress and the Adrenal Gland
Stress & the Adrenal Gland
-
7/29/2019 201 Endocrine 1
71/99
Stress & the Adrenal Gland
Stress induces anon-specificresponse calledgeneral adaptation
syndrome (GAS) Causes ACTH &
cortisol release
Often affects
physiologynegatively
Fig 11.20
11-50
Pancreas
-
7/29/2019 201 Endocrine 1
72/99
Pancreas
Located along small intestine and
stomach; retroperitoneal Exocrine gland
Produces pancreatic digestive
juices
Endocrine gland
Consists of pancreatic islets
Composed of
Alpha cells; secrete glucagon
Beta cells; secrete insulin
Delta cells; secrete somatostatin
-
7/29/2019 201 Endocrine 1
73/99
A 29-amino-acid polypeptide hormone that is a potent
hyperglycemic agent
Its major target is the liver, where it promotes:
Glycogenolysis the breakdown of glycogen to glucose
Gluconeogenesissynthesis of glucose from lactic acid and
noncarbohydrates
Release of glucose to the blood from liver cells
Glucagon
-
7/29/2019 201 Endocrine 1
74/99
Target tissue is the liver, adipose tissue, muscle, andsatiety center of hypothalamus
A 51-amino-acid protein consisting of two amino acid
chains linked by disulfide bonds
Synthesized as part of proinsulin and then excised byenzymes, releasing functional insulin
Insulin:
Lowers blood glucose levels
Enhances transport of glucose into body cells
Counters metabolic activity that would enhance blood glucose
levels
Insulin
Islets of Langerhans continued
-
7/29/2019 201 Endocrine 1
75/99
Betas secrete insulin inresponse to low bloodglucose
Promotes entry ofglucose into cells
& conversion of glucoseinto glycogen & fat
Decreases blood glucose
Islets of Langerhans continued
Fig 11.31
11-64
Insulin & Glucagon Secretion
-
7/29/2019 201 Endocrine 1
76/99
g
Fig 19.7
Normal fastingglucose level is 65105 mg/dl
Insulin & glucagon
normally preventlevels from risingabove 170mg/dlafter meals or falling
below 50mg/dlbetween meals
19-40
Regulation of Blood Glucose Levels
-
7/29/2019 201 Endocrine 1
77/99
g
The
hyperglycemic
effects ofglucagon and
the
hypoglycemic
effects of
insulin
Figure 16.17
-
7/29/2019 201 Endocrine 1
78/99
Regulation of Insulin Secretion
-
7/29/2019 201 Endocrine 1
79/99
Fig 19.10 19-44
Effects of ANS on Insulin & Glucagon
-
7/29/2019 201 Endocrine 1
80/99
g
ANS innervates islets
Activation of Parasymp NS stimulates insulinsecretion
Activation of Symp NS stimulates glucagon &inhibits insulin
This can cause "stress hyperglycemia"
19-45
Diabetes Mellitus
-
7/29/2019 201 Endocrine 1
81/99
Characterized by chronic high blood glucose levels(hyperglycemia)
Type I (insulin dependent orIDDM) is due to
insufficient insulin secretion Type II (insulin independent orNIDDM) is due to
lack of effect of insulin
19-49
-
7/29/2019 201 Endocrine 1
82/99
Results from hyposecretion or hypoactivity of insulin
The three cardinal signs of DM are:
Polyuriahuge urine output
Polydipsiaexcessive thirst
Polyphagiaexcessive hunger and food consumption
Hyperinsulinismexcessive insulin secretion, resulting in
hypoglycemia
Diabetes Mellitus (DM)
-
7/29/2019 201 Endocrine 1
83/99
Figure 16.18
Diabetes Mellitus (DM)
-
7/29/2019 201 Endocrine 1
84/99
Type I Diabetes
-
7/29/2019 201 Endocrine 1
85/99
yp
b cells of islets are destroyed by autoimmune attack Glucose is unable to enter resting muscle or adipose
cells
Rate of fat synthesis lags behind rate of lipolysis
Fatty acids are converted to ketone bodies, producingketoacidosis
Increased glucagon levels stimulate glycogenolysis
in liver
19-51
Effects of Uncontrolled Type I Diabetes
-
7/29/2019 201 Endocrine 1
86/99
y
Fig 19.12
19-52
Hypoglycemia
-
7/29/2019 201 Endocrine 1
87/99
yp g y
Reactive hypoglycemia is oversecretion of insulin due to anexaggerated response ofb cells to a rise in glucose
Occurs in people who are genetically predisposed to type II diabetes
Symptoms include tremors, hunger, weakness, blurred vision, & confusion
Fig 19.14
19-54
-
7/29/2019 201 Endocrine 1
88/99
Miscellaneous Glands &
Hormones
11-65
Pineal Gland
-
7/29/2019 201 Endocrine 1
89/99
Is located in basal
forebrain near
thalamus
Secretes melatonin
in response to
activity of
suprachiasmaticnucleus (SCN) of
hypothalamus
Fig 11.32
11-66
Pineal Gland continued
-
7/29/2019 201 Endocrine 1
90/99
SCN is primary timing center for circadian rhythms
Reset by daily light/dark changes
Melatonin is involved in aligning physiology withsleep/wake cycle & seasons
Secreted at night & is inhibited by light
Inhibits GnRH (antigonadotropic) in many animals
11-67
Thymus
-
7/29/2019 201 Endocrine 1
91/99
Is located aroundtrachea belowthyroid
Produces T cellsof immunesystem &hormones that
stimulate them
Fig 11.3311-68
Sex & Reproductive Hormones
-
7/29/2019 201 Endocrine 1
92/99
Gonads (testes & ovaries) secrete steroid hormonestestosterone, estrogen, & progesterone
Placenta secretes estrogen, progesterone, hCG, and
somatomammotropin
11-69
Estrogen
-
7/29/2019 201 Endocrine 1
93/99
Causes epiphyseal discs (cartilaginous growthplates) to seal (ossify) which stops growth
Is necessary for proper bone mineralization &
prevention of osteoporosis Stimulates osteoblast activity & suppresses
formation of osteoclasts
19-73
Autocrine & Paracrine Regulation
-
7/29/2019 201 Endocrine 1
94/99
Autocrine regulators are produced & act within
same tissue of an organAll autocrines control gene expression in target cells
Paracrine regulators are autocrines that are produced
within one tissue & act on different tissue in same organ.Autocrines & paracrines include:
Cytokines (lymphokines, interleukins)
Growth factors (promote growth & cell division)
Neutrophins (provides trophic support for normal ®enerating neurons)
11-71
-
7/29/2019 201 Endocrine 1
95/99
-
7/29/2019 201 Endocrine 1
96/99
Table 11.2
-
7/29/2019 201 Endocrine 1
97/99
-
7/29/2019 201 Endocrine 1
98/99
Table 11.7
-
7/29/2019 201 Endocrine 1
99/99
Table 11.8