20 ans de Réanima-on: le choc sep-que - JIVD - AER · 20 ans de Réanima-on: le choc sep-que. En...
69
Didier Payen, MD, Ph D [email protected] Lariboisière Hospital – Université Paris 7 UMR INSERM 1160 20 ans de Réanima-on: le choc sep-que
Transcript of 20 ans de Réanima-on: le choc sep-que - JIVD - AER · 20 ans de Réanima-on: le choc sep-que. En...

Didier Payen, MD, Ph D
Lariboisière Hospital – Université Paris 7 UMR INSERM 1160
20 ans de Réanima-on: le choc sep-que

En 20 ans, que s’est-‐il passé? • Sepsis defini-on more or less stable • Epidemiology è
– incidence, age, comorbidi-eskk – Big data èè large cohort
• BeBer educa-on, faster diagnosis, reasonable recomenda-ons (SSC x 3)
• Huge technological progresses: genotyping; transcriptomic; proteomic; metabolomic…
• More clear aspects of immuno-‐inflammatory processes • Reasonable suppor-ve therapy: Fluid amount; pressors; ven-la-on; RRT; ECorp Circ…

En 20 ans, qu’en ai-‐je -ré? • Over simplis-c view leads to mistakes: è RCTs always failed despite solid basic science background
• Infec-on does not kill by itself but by host response – Concept of sep-c phases – Inflamma-on BM; organ damage BM, etc…
• Time for infec-on treatment is crucial (SSC x 3) – Golden hours; AB administra-on; fluid is necessary but not too much! Pressors YES but for what BP level?
• Huge technological progresses: – genotyping; transcriptomic; proteomic; metabolomic… – More rapid detec<on of pathogens
• Elderly pa-ents SHOULD be treated. • Exp models are not easily transposable to human beings

SEVERE SEPSIS
• Sepsis + hypotension (÷÷APSyst > 20 mmHg or APsyst <80 mmHg) or symptoms of hypo-‐perfusion or organ failure :
• AND at least ONE among following criteria
-‐ hypotension (systAP< 90 or ÷÷> 40)
-‐ lac-c acidosis
-‐ oliguria
-‐ encephalopathy
-‐ hypoxemia
-‐ coagulopathy

Le Sepsis: un pb de Santé Publique Mondial…


Budget 1% of US PIB

The W-shaped mortality curve seen in the 1918 influenza pandemic curves for incidence of clinical illness vs. fatality rate markedly differ Same age-dependent mortality pattern is seen for TB, pneumococcal infection, trauma, Yellow fever, malaria, streptococcal Toxic shock, etc. èè What accounts for this difference?
Fedson D. An-viral Research 2013; 99,(3), 417-‐ 435

Sepsis: a syndrome with mul-ples facets… mul-ple determinants for outcome
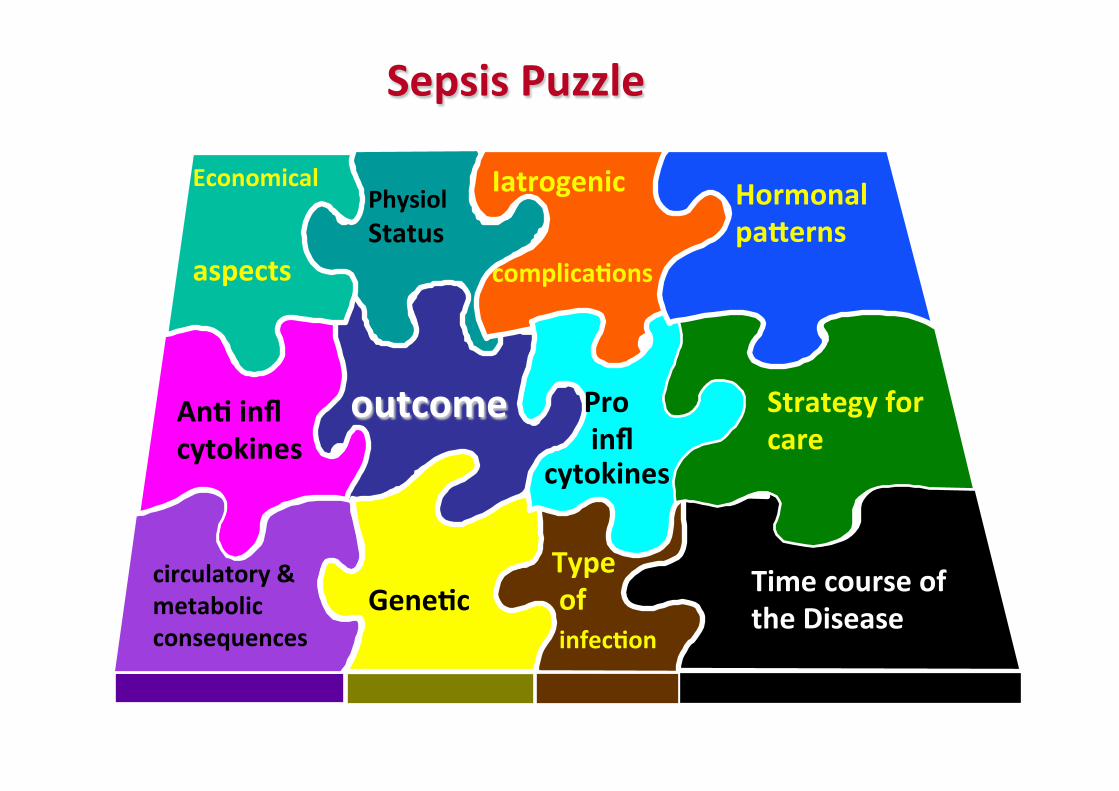
Sepsis Puzzle
outcome An- infl cytokines
Physiol Status
Type of infec-on
circulatory & metabolic consequences
Iatrogenic complica-ons
Economical aspects
Gene-c Time course of the Disease
Pro infl cytokines
Strategy for care
Hormonal paBerns

Sepsis: we beBer understand and conceptualize …
From the last 20 years, concept have moved on a lot… especially in immuno-‐
inflammatory processes

Impact of sepsis on innate and adaptive immune cells

PAMPS èè mu-ple; PRR DAMPS èè mul-ple; DAMP rec -‐ Necro<c cells à DAMPs -‐ Criteria for DAMPs
-‐ Alone è biological response without contamina<on (PAMPs = 0)
-‐ Being efficient at physiological [ ] -‐ Their blockade èè inhibates their ac-on -‐ Examples: HMGB1; Calgranulines…
From Matzinger theory

APC

• PAMP: Proteins from pathogens are processed in the lysosomes to generate an-genic pep-des, which form a complex with MHC class II on the surface of APC, recognized by T cell receptors (TCR)
APC = ANTIGEN PRESENTING CELLS

• LPS complex has 3 components: CD14, TLR4, and MD-‐2. • TLR4 interacts with CD14. Protein MD-‐2 is required for TLR4-‐mediated recogni-on of LPS • TLR4 and MD-‐2 are cons-tu-vely associated with each other. (CD14 is presumably recruited aNer binding LPS) • Limited informa-on about allelic variants of human toll genes and impact on suscep-bility to infec-on
The signalisation

From Cell death to inflamma-on and OF - Necrotic cell death è DAMPs è receptors
è+ prod of inflam cytokines (IL‑1). - Other molecules proteases; hydrolases act on EC components è + mediators (complement fragments) or DAMPs è prod of inflam cytokines by host cells.
- Pro-inflam mediators è local vascular endothelium lesions è ‘leaky’, attracts neutrophils and monocytes/macrophages è soluble (antibody) and cellular defences in the tissue (cell infiltration) neutralize or contain pathogens



The reaction to the sepsis-induced stress…

Medzhitov et al. Science 2012; 355:936-‐41
• ““Threat”” vs. non-threat
• Tolerating pathogens
• Limiting host response
• Stress hormones • Anti-inflammatory
actions • Pro-resolving
actions

Organ-‐specific tolerance capacity to pathogen-‐ or immune-‐induced pathology
Medzhitov et al. Science 2012; 355:936-‐41
Organs largely differ in term of : -‐ Suscep-bility -‐ Repair capabili-es -‐ Func-onal autonomy -‐ sequela

Mortality
-‐ Is early mortality (1st Wk) similar to late mortality?
-‐ Is inflamma-on moving along -me? -‐ What is sepsis-‐induced mortality?
-‐ Crude mortality? -‐ ACributable mortality?

0 5 10 15 20 25 30
0 0.
1 0.
2 0.
3 0.
4 0.
5 0.
6
0 5 10 15 20 25 30
0 0.
1 0.
2 0.
3 0.
4 0.
5 0.
6
0 5 10 15 20 25 30
0.1
0.2
0.3
0.4
Low IL -‐ 10/ Low comorbidi-es (n=67) High IL -‐ 10/ Low comorbidi<es (n=71) Low IL -‐ 10/High comorbidi-es (n=42) High IL -‐ 10/High comorbidi<es (n=38)
Pro
babi
lity o
f deat
h
Days Days
Pro
babi
lity o
f deat
h Low IL -‐ 6/ Low comorbidi-es (n=64) High IL -‐ 6/ Low comorbidi<es (n=75) Low IL -‐ 6/High comorbidi-es (n=46) High IL -‐ 6/High comorbidi<es (n=34)
IL-10 IL-6
202 SS Patients (multicentric)
Early death (<7days) relates mainly to inflammation intensity, but not to comorbidity
level but
Late death (>7days), relates mainly comorbidity

This concept obtained from a training cohort (202 pts) was tested in large testing cohort N = 989 SS patients from Prowess data base

N = 989 pa-ents in sep-c shock
0 5 10 15 20 25
0.0
0.1
0.2
0.3
0.4
0.5
0.6
Days
Prob
abili
ty o
f dea
th
Low Il6/Low comorbidities n=167 Low IL6/High comorbidities n=297 High Il6/Low comorbidities n=215 High IL6/High comorbidities n=253
P value < 0.001

Theore<cal crude mortality of 40% in the absence of therapy. Since matched controls had a crude mortality of 20%, è the es<mate of aBributable mortality is 20% (40% -‐20%). è The best Bmt can reduce mortality about max 20% but cannot reduce the mortality due to the underlying diseases.
ATTRIBUTABLE MORTALITY 20 %

NEJM 2013; 369: 840
To summarize: The Host Response to Sepsis canbe seen as

The -me phases of sepsis

Phase 1 Phase 2 Phase 3

Phase 1

The host response to sepsis
Days
Pro
-in
flam
mat
ory
re
s po
nse
s A
nti
-in
flam
mat
ory
re
s po
nse
s Excessive inflammation causing collateral damage (tissue injury)
Immune suppression resulting in enhanced susceptibility for nosocomial pathogens

The Host Response to Sepsis

The Host Response to Sepsis

The Host Response to Sepsis

0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 0.4
0.5
0.6
0.7
0.8
0.9
1.0
Survival
Study Day
Log-‐rank test P value: 0.5789
Hazard ra-o (95% CI): 1.05 (0.88, 1.26)
Placebo
Eritoran
Placebo Censored
Eritoran Censored
ACCESS trial: TLR4/MD2 inhibition in severe sepsis
28-day mortality
28.1%
26.9%

The Host Response to Sepsis
Activated Protein C Antithrombin
Tissue factor pathway inhibitor

PROWESS-SHOCK (NEJM 2012)
Ranieri et al NEJM 2012
Percent in study hospital 28d: DrotAA 305 (49%) Placebo 279 (43%)

-‐ fast track process (short windows: hrs…)
-‐ mul- interac-ve processes
-‐ lack of validated BM to rapidly characterize host
reponse
Early phase is challenging because of:
Why not being inspired by cancer strategies?

cecal liga<on and puncture (CLP) mouse model: 80% of C57BL/6 mice succumbed within 48 hr Ø epirubicin i.p. at the time of CLP and again 24 hr later reproducibly and significantly (p < 0.001) increased the survival Ø Independently from mouse strain Ø “ “ “ “ of sepsis of origins in addition to peritoneal sepsis
Ø epirubicin-treated + CLP has similar bacterial load in blood and organs 24 hr post-CLP
Ø a substantial reduction in the levels of inflammatory mediators TNF, IL-1b, IL-6, and HMGB1

Ø Epirubicin protection against Sepsis is mediated by ATM, a master regulator of the DDR (DNA damage response)
Ø ATM-deficient(Atm-/-) mice were not
protected by epirubicin against CLP and died with similar kinetics to wild-type (WT, Atm+/+) animals
Epirubicin has a 24 hr Therapeu-c Window to Protect against Sepsis

The Host Response to Sepsis
Urgent need for biomarkers that reflect the predominant type of the host response to sepsis in an individual patient. ü Aid in identification of patients that might
benefit from a specific intervention. ü Aid in titrating the intervention and
monitoring the response. ü Rapid: “point-of-care”.

The kidney: a good example

Pathophysiology: Kidney is perfused by inflamed blood: èè activated Immune
Cells + elevated mediators plasma levels èè infiltration
Systemic inflamma-on èè AKI via vascular compartment

Is there any difference between AKI groups for inflamma-on ?


PHASE 2

Phase 1 Phase 2 Phase 3
Post-‐Agressive Immuno-‐Depression (PAID) Syndrome

q Loss of delayed type hypersensi-vity response to common recall an<gens
q Apoptosis-‐induced deple-on of immune effector cells, loss of CD4, CD8, B, and dendri-c cells q Reac-va-on of latent viruses (CMV; herpes virus in roughly 25–35% of pa<ents with sepsis)
q autopsy èè most pa-ents admiBed to ICUs for treatment of sepsis had unresolved sep-c foci at post mortem, èèpa-ents unable to eradicate invading pathogens and were more suscep-ble to nosocomial organisms, or both q Blood studies from pa<ents with and without sepsis show decreased produc-on of proinflammatory cytokines, decreased monocyte HLA-‐DR expression, increased numbers of regulatory T cells (Treg Fox P3), increased produc-on of PD-‐1 or PD-‐L1
Clinical or laboratory evidence for sepsis being an immunosuppressive disorder

Venet et al. Crit Care Med 2013; 41(1):111-‐119
T cell repertoire rapidly decreases in sepsis

Is this immunodepression also observed in -ssue infiltra-ng immune cells?
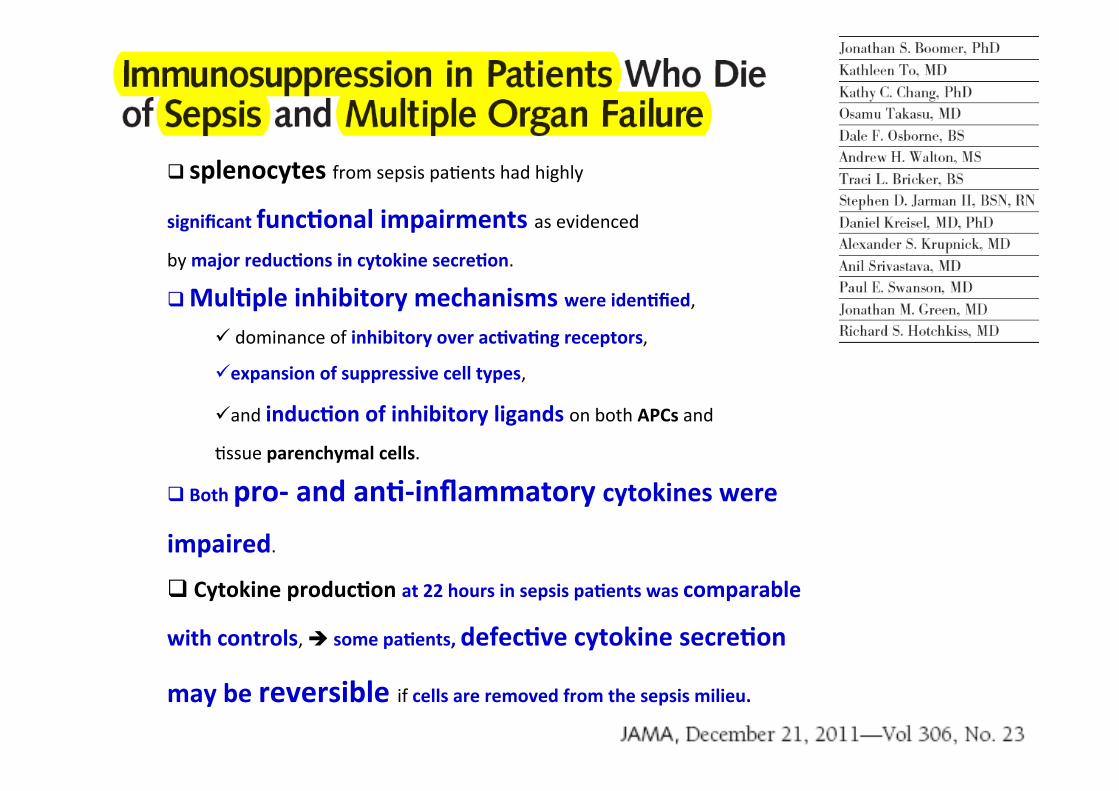
q splenocytes from sepsis pa<ents had highly
significant func-onal impairments as evidenced by major reduc-ons in cytokine secre-on.
q Mul-ple inhibitory mechanisms were iden-fied, ü dominance of inhibitory over ac-va-ng receptors,
ü expansion of suppressive cell types,
ü and induc-on of inhibitory ligands on both APCs and
<ssue parenchymal cells.
q Both pro-‐ and an--‐inflammatory cytokines were
impaired.
q Cytokine produc-on at 22 hours in sepsis pa-ents was comparable
with controls, è some pa-ents, defec-ve cytokine secre-on
may be reversible if cells are removed from the sepsis milieu.

Sepsis èè Profound Loss of CD4 and CD8 Cells the loss of CD 4 T cells mimics HIV in severity èè
in ineffec-ve adap-ve immunity
Non-‐ sep-c Sep-c
Boomer, Chang, Takasu, et. al Journal of the American Med. Associa;on (JAMA) 306:2594 2011

(In press)

1
10
100
1000
10000
100000
BLOOD BM
Mon
ocyt
e H
LA-D
R (A
B/C
)
p<0.0001 p=0.0009
A ICU Patients; Non ICU patients; HV
Blood and BM mHLA-‐DR expression in pa-ents vs controls
1
10
100
1000
10000
100000
BLOOD BM
Mon
ocyt
e H
LA-D
R (A
B/C
)
B Sshock, Septic, non septic; non ICU, HV
p<0.0001
p=0.0006
p<0.0001 p=0.0008
p=0.0412
p=0.0056
PlosOne (In press)

Conclusion
The downregula-on of HLA-‐DR in BM monocyte
lineage is present in ICU pa-ents without major
changes in myeloid cells. It may result from a
regula-on mediated by soluble and/or neuro-‐
endocrine factors present in BM cell
microenvironment.

at least 1500 patients

Can We treat this immunosuppression?

59 2013
PMN, Mono phagocytose mHLA-‐DR TNFαα
Fct Mono Phagocytose
Prolif. Tcell IFNγγ An--‐apoptose êêPD-‐1, ãã molec adhesion êêTreg Diversité récepteurs TCR
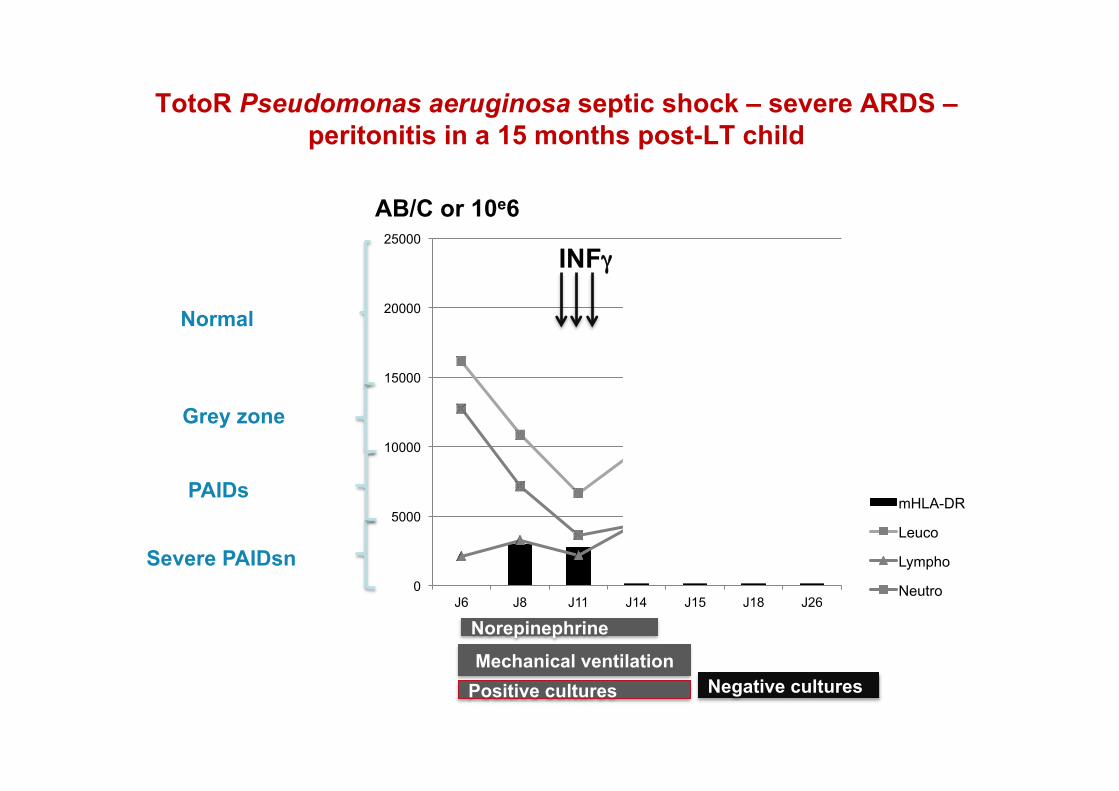
TotoR Pseudomonas aeruginosa septic shock – severe ARDS – peritonitis in a 15 months post-LT child
0
5000
10000
15000
20000
25000
J6 J8 J11 J14 J15 J18 J26
mHLA-DR
Leuco
Lympho
Neutro
Severe PAIDsn
Normal
Grey zone
PAIDs
AB/C or 10e6
INFγγ
Norepinephrine
Mechanical ventilation Positive cultures Negative cultures

To conclude • PAIDs is a fact that concerns all acute situations, particularly severe sepsis is
always present after 1 or 2 days post injury
• IMMUNOSCOPE – Blood measurements: WBC (fractions), NCLRatio; semi-quantitative cytokine level
– Flowcytometry: HLA-DR; Ly sub-populations
• è IMMUNOSCOPE! èè Personalized therapy
• HLA-DR is a good candidate and is cheap and fast to be measured with
semi-quantitative IL-6, IL-10.
• Immuno-stimulation can be proposed on solid criteria
• RCT are on going testing different targets and molecules (INFγγ, GM-CSF; IL-7…)



interferon γγ
0
5000
10000
15000
20000
25000
30000
35000
Day3 Day6 Day7
Day9 Day11
Day12 Day13
Day15 Day17 discharge
BAL pseudomonas aeru 109 +++ +++ + 0 0
2603 570
mHLA-‐DR
(AB/C)
Days awer ICU admission (post cardiac arrest)
Lukaszewicz et al.Crit Care Med 2009; 37: 2746–2752
Nl
Risk factors for severe sepsis or sep-c shock
Brun-‐Buisson et al, JAMA 1995
• Ageing • Male sex (63 %) • Emergency admission: medical or surgical • Admission in a large hospital: > 400 beds • immunodepression or underlying pathologies with a short term bad prognosis.


Le Sepsis: Stratégie de recherche basée sur l’inflamma-on…

EXPRESSION OF ADHERENCE MOLECULES ON ENDOTHELIAL CELL CULTURE èè TOO LONG
SERA WHOLE
BLOOD
SURFACE ANTIGEN EXPRESSION (FLOW
CYTOMETRY)
2hrs
CYTOKINE SECRETION Quick semi-quantitative method IMMEDIATE
WHOLE
BLOOD
PATIENTS
Post-agressive Immuno-Depression Syndrome: PAIDs STRATEGY FOR IMMUNOSCOPING!
Blood as « tissue Biopsy » - WBC - Fractional count - PMN/Ly ratio

Phase 1 Phase 2 Phase 3