1. SCOTTISH NEPHROLOGISTS' DIALYSIS PREFERENCES: EXPOSING THE ...
49
1. SCOTTISH NEPHROLOGISTS’ DIALYSIS PREFERENCES: EXPOSING THE GAP BETWEEN WHAT WE OFFER AND WHAT WE WOULD CHOOSE. Siobhan K. McManus and Robert A. Mactier Western Infirmary, Glasgow and Glasgow Royal Infirmary, Scotland, UK In Scotland more than 95% of patients on haemodialysis attend for three times a week 4 to 5 hour hospital based dialysis. They have significant morbidity and poor survival. The HEMO trial did not suggest that increasing dialysis dose as measured by Kt/V improved survival. Evidence of better outcomes on home haemodialysis, long nocturnal and daily haemodialysis has been coloured by patient selection and randomised controlled trials (RCTs) have been difficult to perform. Pending the outcome of the Frequent Hemodialysis Network Trial we wanted to canvass Scottish nephrologists regarding their dialysis preferences and see how these correlated with the therapies we currently offer our patients. We invited all consultant nephrologists in Scottish renal units and other career nephrologists (associate specialists and trainees) to complete an online questionnaire. We asked: If you were to find yourself with end stage renal failure in need of renal replacement therapy with no prospect of a renal transplant which of the following dialysis options would you prefer? Options of haemodialysis and haemodiafiltration (HDF) of varying frequency and duration, CAPD/APD and conservative treatment were offered. Respondents also indicated whether they would prefer treatment at home or in-centre (full or minimal/self care). Information regarding geographical location and the types of therapy offered at each unit was collected. All responses were anonymous. Of 92 nephrologists contacted, 70 completed the survey (76% response rate). Of these 60% were consultants. Only 16% chose peritoneal dialysis whereas 83% chose haemodialysis/HDF at a higher frequency and/or longer duration than standard. Approximately equal numbers chose haemodialysis and haemodiafiltration. Most wanted a home based treatment (94%). There was no association between those units with home dialysis programmes or HDF and the frequency of these choices. There was no significant difference between the choices of consultants and trainees. In spite of the lack of RCT evidence, the majority of Scottish nephrologists wanted a haemodialysis duration or frequency greater than standard, a treatment option we do not generally offer our patients, and wanted to do this at home. That they are prepared to spend more time on dialysis probably reflects their interpretation of non-RCT evidence in the literature to date and, in some cases,
Transcript of 1. SCOTTISH NEPHROLOGISTS' DIALYSIS PREFERENCES: EXPOSING THE ...

1. SCOTTISH NEPHROLOGISTS’ DIALYSIS PREFERENCES: EXPOSING THE GAP BETWEEN WHAT WE OFFER AND WHAT WE WOULD CHOOSE.
Siobhan K. McManus and Robert A. MactierWestern Infirmary, Glasgow and Glasgow Royal Infirmary, Scotland, UK
In Scotland more than 95% of patients on haemodialysis attend for three times a week 4 to 5 hour hospital based dialysis. They have significant morbidity and poor survival. The HEMO trial did not suggest that increasing dialysis dose as measured by Kt/V improved survival. Evidence of better outcomes on home haemodialysis, long nocturnal and daily haemodialysis has been coloured by patient selection and randomised controlled trials (RCTs) have been difficult to perform. Pending the outcome of the Frequent Hemodialysis Network Trial we wanted to canvass Scottish nephrologists regarding their dialysis preferences and see how these correlated with the therapies we currently offer our patients.
We invited all consultant nephrologists in Scottish renal units and other career nephrologists (associate specialists and trainees) to complete an online questionnaire. We asked: If you were to find yourself with end stage renal failure in need of renal replacement therapy with no prospect of a renal transplant which of the following dialysis options would you prefer? Options of haemodialysis and haemodiafiltration (HDF) of varying frequency and duration, CAPD/APD and conservative treatment were offered. Respondents also indicated whether they would prefer treatment at home or in-centre (full or minimal/self care). Information regarding geographical location and the types of therapy offered at each unit was collected. All responses were anonymous.
Of 92 nephrologists contacted, 70 completed the survey (76% response rate). Of these 60% were consultants. Only 16% chose peritoneal dialysis whereas 83% chose haemodialysis/HDF at a higher frequency and/or longer duration than standard. Approximately equal numbers chose haemodialysis and haemodiafiltration. Most wanted a home based treatment (94%). There was no association between those units with home dialysis programmes or HDF and the frequency of these choices. There was no significant difference between the choices of consultants and trainees.
In spite of the lack of RCT evidence, the majority of Scottish nephrologists wanted a haemodialysis duration or frequency greater than standard, a treatment option we do not generally offer our patients, and wanted to do this at home. That they are prepared to spend more time on dialysis probably reflects their interpretation of non-RCT evidence in the literature to date and, in some cases, experience related by patients on higher frequency or overnight haemodialysis.

2. A PROSPECTIVE CROSSOVER STUDY OF SHORT DAILY HOME HAEMODIALYSIS.
Siobhan K. McManus and Robert A. MactierWestern Infirmary, Glasgow and Glasgow Royal Infirmary, Scotland, UK
The majority of published studies of daily dialysis suggest an improvement in small solute clearance, blood pressure, anaemia/ESA dose, health related quality of life and post-dialysis recovery time though there is a paucity of randomised controlled trial evidence. Recent data show the life expectancy of patients on daily dialysis is 2-3x better than that of matched USRDS haemodialysis (HD) patients and that home-based daily HD patients had a survival similar to that of age-matched recipients of deceased donor renal transplants 1. Daily dialysis, however, involves an increase in time spent setting up and clearing up and leaves patients with only one non-dialysis day per week.
We designed a single centre, prospective crossover study to establish the role of short daily (6x week) dialysis in our home haemodialysis population. This was an ABA crossover study where A= usual thrice weekly dialysis and B= 6x week half usual time; each period lasted 3 months. Data collected included pre/post urea, pre-dialysis BP, K+, haemoglobin (Hb), albumin, drug doses (ESA, phosphate binders and anti-hypertensive drugs), quality of life (KD-QoL) data, time to recovery and patient preference for dialysis frequency. We also monitored access problems and hospitalisations.
Eight of twenty eight home HD patients were enrolled. The mean standard Kt/V rose from 2.34 to 3.04 by increasing the frequency of dialysis without altering total weekly hours. This compares with a standard Kt/V of 2.39 in the HEMO study ‘high dose’ arm. The most notable improvement was the reduction in post dialysis recovery time from 8 to 1.5hours (p=0.016). There were also improvements in some aspects of quality of life in both physical and mental domains. Seven of the eight patients preferred daily dialysis and six elected to continue this at the end of the study (the seventh having received a kidney transplant). There was no significant increase in access problems. Daily HD did not affect Hb/ESA dose, pre-dialysis phosphate or potassium or total weekly ultrafiltrate over the time period of this study.
We conclude that short daily haemodialysis is a desirable and feasible option for some patients on home haemodialysis.
1. Kjellstrand et al NDT (2008) 23: 3283-3289

3. MYOCARDIAL FIBROSIS DETECTED WITH CARDIAC MAGNETIC RESONANCE IMAGING AND RISK OF CARDIOVASCULAR MORTALITY IN END STAGE RENAL DISEASE.
Patrick B Mark, Nicola Johnston, Rajan K Patel, Tracey Steedman, John E Foster, Henry J Dargie, Alan G JardineBHF Glasgow Cardiovascular Research Centre, University of Glasgow, Glasgow
Background
Patients with end stage renal disease (ESRD) are at extremely high risk of premature cardiovascular events. Left ventricular (LV) abnormalities are common in this population and confer adverse prognosis. Cardiac magnetic resonance imaging (CMR) can identify the presence of myocardial fibrosis which may be associated with increased cardiovascular risk. This study examined the prognostic implications of myocardial fibrosis in patients with ESRD.
Methods
199 patients with stage 5 chronic kidney disease being assessed for renal transplantation (157 on dialysis) were studied with contrast enhanced CMR. Patients were followed up for a median of 61.1 months.
Results
Myocardial fibrosis was demonstrated in 61 (30.7%) patients indicated by late gadolinium enhancement (LGE) on CMR images. 32 (16.1%) had a pattern of subendocardial LGE in keeping with previous myocardial infarction while 29 (14.6%) had diffuse LGE in keeping with diffuse myocardial fibrosis. 142 (71.4%) patients had left ventricular hypertrophy and 29 (14.6%) had LV systolic dysfunction. During follow up, there were 61 (30.7%) deaths of which 36 (59.0% of deaths) were cardiovascular deaths. The presence of LGE at CMR was an independent predictor of both cardiovascular and all cause mortality whilst receiving a kidney transplant was associated with better survival. Diabetes, increasing age and prior ischaemic heart disease were also associated with mortality. Two patients in this cohort developed nephrogenic systemic fibrosis.
Conclusions
The presence of LGE at CMR identifies patients at highest risk of death. As gadolinium based studies will not be possible in this population, alternative methods to identify myocardial fibrosis are required.
Funding: British Heart FoundationConflict of interest: none

4. HYPOMAGNESAEMIA IS ASSOCIATED WITH THE USE OF PROTON PUMP INHIBITORS IN PATIENTS WITH CKD.
Rajni Tejwani, Chris Deighan, Renal Unit, Glasgow Royal Infirmary
Introduction
Hypomagnesaemia is a common entity occurring in up to 12% of hospitalised patients. In populations with reduced renal function, serum magnesium (Mg) levels are often normal or high. Recently, a number of case reports have been published suggesting a causal relationship between proton pump inhibitors (PPI) and hypomagnesaemia.
Aims
To assess the incidence of hypomagnesaemia in a group of patients with chronic kidney disease (CKD) attending a renal out-patient clinic and to investigate any association between proton pump inhibitors, diuretic use and serum Mg levels.
Methods and materials
A cross sectional analysis of patients attending a renal out-patient clinic. An automated search was performed for patients seen at Falkirk Renal Out-patient clinics over a 1 year period from 1/3/08 to 28/02/09. Data for serum magnesium was recorded along with drug history for PPI and diuretic use.
Results
209 out of 695 patients reviewed during the study period had a serum Mg checked. Serum Mg in all patients was 0.82 + 0.12mmol/l (mean + SD). 23 patients (11%) were found to have hypomagnesaemia (<0.7mmols/l). Serum Mg levels were < 0.5mmol/l in 3 patients and between 0.51 to 0.6mmol/l in a further 9 patients.65 / 209 (31%) of patients were treated with PPIs. Of the 23 patients with hypomagnesaemia, 12 (52%) were on PPIs. In contrast 11/144 (8%) of patients in the group not on PPIs had a low Mg (p=0.02 X2 test). 100/209 (48%) of patients were on diuretics. Of the 23 patients with low Mg, 15 (65%) were on diuretics whereas 8/109 (7%) of patients in the group not on diuretics had a low Mg (p=0.08 X2 test). 10/23 patients (43%) with hypomagnesaemia were on both a PPI and a diuretic.Overall, serum Mg levels did not differ in the patients treated with PPI compared with those not on PPIs: serum Mg 0.80+ 0.15 vs 0.83 + 0.11mmol/l, p=nsd (PPI vs No PPI: All mean + SD). No significant difference in serum Mg was found in patients treated with diuretics compared with those not on diuretics (0.84+0.14 vs 0.81+0.10, p=nsd (diuretic vs no diuretic). Patients on both PPIs and diuretics had the lowest Mg levels : 0.79+ 0.17 mmol/l.
Conclusions
11% of patients with CKD attending a hospital renal out-patient clinic had hypomagnesaemia. Low serum Mg is found more frequently in patients treated with PPIs however serum Mg levels in patients on PPIs did not differ compared with those not on PPIs. The mechanism by which PPIs contribute to hypomagnesaemia needs further evaluation. Further study is required to determine whether these findings are clinically relevant. Larger studies may determine if overall Mg levels in patients on PPIs are significantly lower. It remains to be determined if more frequent measurement of Mg levels in patients with CKD being treated with PPIs is required.

5. AN ATYPICAL CASE OF WEGENER’S GRANULOMATOSIS: CASE REPORT AND REVIEW OF THE LITERATURE.
Claire Nolan, Scott Morris, Chris Deighan, Bruce Mackinnon, Cath Stirling Renal Unit, Glasgow Royal Infirmary
Case Report
Mr K presented with fatigue, myalgia, cough and haemoptysis which did not improve with antibiotics. Bronchoscopy and CT scanning confirmed mediastinal lymphadenopathy, cavitating pulmonary nodules, and an inflammatory cuff surrounding the aorta throughout its length. He had normal renal function and a PCR of 20mg/mol and so a renal biopsy was not performed. However, PR3-ANCA titre was >100 and a diagnosis of Wegener’s Granulomatosis with large vessel involvement was made. He was initially treated with conventional immunosuppression and has subsequently been treated with a number of second line agents, including rituximab, mycophenolate and methotrexate. Despite this,he has never achieved a sustained remission. He has also exhibited many side effects of treatment and continues to show progression of disease.
Literature Review
There are few similar case reports in the literature. Chirinos1 has published a comprehensive review of small vessel vasculitis associated with large vessel involvement. Of thirteen cases, seven had Wegener’s Granulomatosis, and three had no renal compromise. The large vessel involvement took many forms, including perivasculitis, luminal stenosis or occlusion, aneurysm formation, or dissection. Individual case reports of co-existing pauci-immune glomerulonephritis with temporal arteritis or Takayasu arteritis have also been published. It is possible the presence of large vessel disease in these patients is part of a spectrum of ANCA-associated small vessel vasculitis.
Summary
Wegener’s granulomatosis is a systemic vasculitis predominantly affecting medium and small arteries, and classically involving the respiratory tract and kidneys. Sub types are recognised, however, large vessel involvement is uncommon. We present the case of a PR3-ANCA positive vasculitis affecting lungs and aorta, but with little renal involvement. This combination of disease is not accounted for by current classifications of vasculitides. In addition, the small number of similar reported cases means that optimal therapy, including knowledge of progression and outcome, is uncertain. We believe this case illustrates that large vessel vasculitis can be a feature in patients with classical ‘small vessel’ vasculitis. We would advocate a high clinical suspicion of this potentially life-threatening large vessel involvement and recognise that these patients may be resistant to conventional immunosuppression.
1. Chirinos, JA, Tamariz, LJ, Lopes, G et al. Large vessel involvement in ANCA-associated vasculitides : report of a case and review of the literature. Clin Rheum 2004;23:152

6. AZATHIOPRINE MAINTENANCE THERAPY IN PAUCI-IMMUNE RENAL VASCULITIS.
Kate K Stevens, Siobhan K. McManus, Patrick B Mark, Jonathan G Fox & Cath StirlingRenal Unit, Glasgow Royal Infirmary, Glasgow
Background
Pauci-immune renal vasculitis is an important cause of end stage renal failure in the UK, often affecting elderly patients who have a particularly poor prognosis. Previously we have looked at patient and renal survival and factors which predict outcome. Standard treatment comprises of steroids and cyclophosphamide to induce remission; followed by a period of maintenance therapy with a less toxic immunosuppressant, usually azathioprine. There is a lack of consensus over both the optimal dose and the duration of azathioprine maintenance therapy. This study looked at azathioprine dosing, relapse rate and complications.
Method
The computerised records and case notes of all patients diagnosed with pauci-immune renal vasculitis between 1996 to 2006 at the Glasgow Royal and Stobhill Hospitals were reviewed. Patient demographics and laboratory parameters at presentation were recorded including age, serum creatinine and ANCA status. Treatment regimes, related complications, disease relapse and the need for renal replacement therapy were noted. Infection and relapse was defined by both clinical and serological evidence.
Results
In this 11 year period there were 71 patients with pauci-immune renal vasculitis, with a median age of 67.2 years (range 15-85 years); 55% were male and 93% were ANCA positive. Sixty four had histological evidence of pauci-immune renal vasculitis. Following induction of remission, 32 patients (46%) were commenced on azathioprine as maintenance therapy. Median age was 61 years (range 16-79 years) and 10 patients had a diagnosis of microscopic polyarteritis. Median follow up was 1572 days (range 48-4865 days) from the date azathioprine commenced. Azathioprine was started at a median time of 98 days from diagnosis (range 1-318 days). 12 patients were PR3/MPO positive on commencing azathioprine. Median creatinine was 250micmol/L at diagnosis (range74-742micmol/L) and 170micmol/L (range 65-350micmol/L) at time of azathioprine therapy. 47% of patients suffered a relapse at a median of 539 days (range 76-2769 days) from starting azathioprine. Of these, 87% suffered more than one relapse. The mean starting dose of azathioprine in the relapse group was 1.47mgs/kg compared with 1.57mgs/mg in the group who did not. The mean maximum dose in those who relapsed was 1.3mgs/kg compared with 1.7mgs/kg in those who did not. 14 patients (5 of whom relapsed) had clinical/serological evidence of infection whilst on azathioprine; these patients were on a mean dose of 1.56mgs/kg of azathioprine compared with 1.4mgs/kg in those who did not suffer infection. 12 patients (4 of whom relapsed) experienced side effects with azathioprine; 9 of these patients were taking more than 1.5mgs/kg of azathioprine. 10 patients died during the follow up period. In univariate analysis, age and serum creatinine at presentation were predictors of death.
Conclusion
A high percentage of our patients suffered a relapse compared with figures quoted in the literature. This may relate to the age of our population, the severity of vasculitis (our patients all had evidence of renal involvement) and the majority of our patients received less than 2mgs/kg of azathioprine. Additionally, we relied upon clinical judgement for identification of relapse and not a formal scoring system. Although not statistically significant, the patients who relapsed received both a lower starting dose and maximum dose of azathioprine. Those who were on higher initial and maximum doses of azathioprine suffered fewer relapses but a higher number of these patients experienced side effects and infective episodes.

7. PARATHYROIDECTOMY: AN AUDIT OF PRE- AND POST-CARE.
Heather Kerr, Department of Nephrology, Edinburgh Royal Infirmary
Introduction
Hyperparathyroidism is a common complication of chronic kidney disease. The incidence of ‘hungry bone syndrome’ – causing profound hypocalcaemia – after surgical parathyroidectomy is high in patients who are on dialysis for end-stage kidney disease. The renal unit at Edinburgh Royal Infirmary has a short protocol for the management of calcium in these patients, but anecdotal experience suggests management varies enormously, both in pre-loading and post-operative medications. An audit was undertaken looking at our pre-operative loading of calcium, with post-operative timing of blood tests and subsequent management. This was with the view to writing a full protocol with clear management guidelines for junior team members.
Method
A list of patients who had undergone a parathyroidectomy for tertiary hyperparathyroidism between August 2008 and July 2009 was obtained from the Lothian Surgical Audit. Of 16 patients, 13 of whom were on haemodialysis at the time, 10 sets of notes were obtained. Using our renal ‘Proton’ system, laboratory results system and patients’ notes/drug charts, several key points were reviewed, including pre-operative loading, frequency of post-operative blood tests (including calcium levels) and post-operative calcium medications, with reference to local and/or KDOQI guidelines.
Results
Patients who received a higher level of pre-operative calcium loading had less hypocalcaemia. 4/10 patients required calcium infusions - of these four, the two that were symptomatic of their hypocalcaemia both had values of <1.8 corrected (both 1.74).
All calcium nadirs were in the 24-36 hour post-operative period. 5/10 patients had adequate post-operative calcium checks (4-6 hourly KDOQI). Of the three with 12 hour plus gaps in checks, all were in patients with CoCa <2, with falling levels, and were overnight.
Calcium supplementation varied, from 1mcg alfacalcidol on discharge, to 4mcg bd alfacalcidol with sando-cal 1000 2 tab tds. Sando-cal 400 was also used. 5/10 patients only got calcium supplements the first post-operative day once calcium was already falling. Patients who required more supplementation had it started later in the post-operative period (Day 1-3 post-op). No patients had problems with hypercalcaemia despite large doses of oral calcium.
Conclusion
Patients were less likely to become hypocalcaemic if they received adequate pre-operative loading, as well as early post-operative oral supplementation. Post-operative calcium checks were done as per protocol in 50% of patients, but concerningly the three with the largest gaps were all hypocalcaemic. Junior doctors are often prescribing for these patients out of hours and a clear, step by step protocol is required for the management of these patients. This can be placed both on the renal ward as well as our online reference www.edren.org for easy access out of hours.

8. A RETROSPECTIVE ANALYSIS OF NEPHROGENIC SYSTEMIC FIBROSIS IN A POPULATION UNDERGOING RENAL MAGNETIC RESONANCE ANGIOGRAPHY STRATIFIED BY EGFR.
Tara Collidge 1 , Anirudh Rao 2 , Peter Thomson 2 , Michaela Brown 2 , Keith Simpson 2 Scott Morris 2 , Giles Roditi 3 . 1. Renal Unit L7, Western Infirmary, Glasgow. 2. Renal Unit 3rd Floor Walton Building, Glasgow Royal Infirmary, Glasgow. 3. Department of Radiology, Glasgow Royal Infirmary, Glasgow.
IntroductionNephrogenic Systemic Fibrosis (NSF) is a rare, debilitating condition that associates with the administration of gadolinium-based contrast agents (GBCA) used for magnetic resonance angiography (MRA). Only individuals with renal impairment develop NSF. The incidence in patients with end stage renal failure exposed to the highest risk GBCA (gadodiamide) is 3-7%. European Guidelines contraindicate the use of high risk GBCAs in AKI and CKD < 30ml/min and advise caution for those with eGFR < 60ml/min. American guidelines suggest a class ban on GBCAs. We considered a population with varying eGFR exposed to renal artery MRA to determine the distribution of NSF with reference to renal function.
MethodsA list of all patients who under went renal MRA in Glasgow was obtained from radiology records. Those with renal unit electronic patient records (EPR), follow up for at least 90 days post imaging, an eGFR measurement within 90 days of MRA and documented follow up within 90 days of MRA were included. Information on diagnosis, in patient and out patient follow ups, outcome and the presence of NSF was determined. NSF was diagnosed after review of diagnosis, clinical history, timeline and correspondence screens within the EPR with cross reference to the pathology database.
Results1551 people underwent renal MRA, each with a dose of 30ml 0.5 Molar gadodiamide (approximately 1.0 mmol/kg) between the start of 1998 and the end of 2005. Of these 481 met the inclusion criteria. The spread of eGFR is shown below. CKD stage eGFR(ml/min) number %5 <15 69 14.64 15-29.9 168 35.53b 30-44.9 144 30.43a 45-59.9 52 11.01/2 60>= 40 8.5
Eight were identified as having acute kidney injury at the time of imaging and not included in CKD staging. 38.1% had renovascular disease and 2.1% were potential live kidney donors. The median time from MRA to follow up was 20 days with a median of 3.7 years follow up. The median number of out patient follow ups with correspondence was 12. At the end of the study period 35.6% were dead, 24.9% discharged or transferred, 33.3% continued as out patients and 6.2% were receiving renal replacement therapy. 3 patients were identified as having NSF. 2 had AKI at the time of imaging and NSF developed following renal MRA. The third had deteriorating CKD with an eGFR of 16.1ml/min at the time of renal MRA but developed NSF three years later following a second MRA with gadodiamide. Peritoneal dialysis was established for 16 months prior to the second scan. All three were alive at the end of the study period. All cases of gadodiamide-associated NSF from our unit (n=16) were reviewed with respect to eGFR at the time of MRA preceding diagnosis. 13 were established on dialysis, 2 had AKI and one had an eGFR of 8.3ml/min.
ConclusionsThese findings suggest that individuals at greatest risk of developing NSF have AKI or stage 5 CKD at the time of gadodiamide exposure. We identified no NSF cases linked to GBCA use with an eGFR >=15ml/min despite looking at a population with a wide range of eGFR.
No conflict of interest to declare. No funding was obtained.

9. MORTALITY AND FREQUENCY OF NEPHROGENIC SYSTEMIC FIBROSIS.
Tara Collidge 1 , Peter Thomson 2 , Patrick Mark 1 , Jamie Traynor 4 , Keith Simpson 2 , Scott Morris 2 , Giles Roditi 3 .
1. Renal Unit L7, Western Infirmary, Glasgow. 2. Renal Unit 3rd Floor Walton Building, Glasgow Royal Infirmary, Glasgow. 3. Department of Radiology, Glasgow Royal Infirmary, Glasgow.4. Renal Unit, Monklands Hospital, Glasgow
Introduction
Nephrogenic Systemic Fibrosis (NSF) is a rare, debilitating condition affecting individuals with severe renal impairment that associates with the administration of high doses of gadolinium-based contrast agents (GBCA) used for magnetic resonance imaging, in particular for magnetic resonance angiography (MRA). Mortality is high in reported case series but little information exists on mortality compared to a matched population.
Methods
1. The electronic patient records (EPR) for two Glasgow renal units were searched to identify all patients on renal replacement therapy (RRT) from 01.01.2000 to 30.06.2006. Those with a functioning transplant and acute kidney injury were excluded. NSF and GBCA exposure were identified using EPR ‘textfinder’ and radiology screen searches, case note review, dermatology and pathology contact, eCRIS searches and biopsy review. Onset of RRT and outcome including date of death were recorded. Survival to death or census (01.07.06) was determined from either RRT onset or scan date and analysed using SPSS software.2. To identify if changing patterns of MRA referral have impacted on NSF case frequency, numbers and date of Glasgow wide referrals for all types of MRA from either ‘all’ or ‘renal’ referrers was recorded together with the date of onset of NSF cases.
Results
1. 1826 patients were identified as having RRT within the 6.5 year study period. 425 received GBCAs and 14 developed NSF, 13 following gadodiamide exposure. 1812 had outcome data. 704 (38.9%) patients died and median survival from RRT onset to death or census for the whole cohort was 2.6 years. Median survival for the GBCA exposed cohort was also 2.6 years and median survival from scan to death or census was 2.0 years. Median survival for the gadodiamide exposed NSF population was not significantly different measured by RRT onset or post scan survival. No significant difference could be found when survival for the total RRT cohort minus gadodiamide exposed cohort was compared to the NSF population. 2. In total 17 cases of NSF are known to our unit presenting between January 2001 and January 2007. 16 cases were associated with gadodiamide. No further cases have been reported despite increased awareness. Between 1998 and 2002 MRA requests from renal referrers steadily increased year on year from 13 to 113. They remained steady and then declined following the link with GBCA and NSF to 32 in 2008. The frequency of NSF cases follows the frequency of MRA requests by renal referrers.
Conclusions
1. Despite poor survival, no significant difference in mortality could be demonstrated between our NSF patients and an RRT population also selected for GBCA exposure. 2. The frequency of NSF cases closely follows the number of MRA scans requested by renal referrers suggesting that GBCA exposure is causally implicated in the development of NSF
No conflict of interest to declare. No funding was obtained.

10. MORTALITY STUDY OF PATIENTS WITH STAGE 4 AND 5 CHRONIC KIDNEY DISEASE IN EDINBURGH.
Fiona Duthie, Johanna MacKenzie, Wendy Metcalfe, Royal Infirmary of Edinburgh.
Aim
To examine the deaths of patients with stages 4 or 5 chronic kidney disease (CKD) who had been seen at least once in the outpatient clinics of the Edinburgh renal unit, in order to determine the usage of our conservative care programme.
Methods
The details of all patients who died between 1/1/2008 and 30/6/2009 were retrieved from the electronic patient record of the RIE Renal Unit. All patients who had stage 4 or 5 CKD at their last outpatient clinic visit prior to death were identified by excluding those who died with stages 1-3 CKD and those who had not been seen in the outpatient clinic on at least one occasion. Patients receiving renal replacement therapy (RRT) were also excluded.Demographics, cause and location of death, cause and degree of kidney disease and planning for management of stage 5 CKD were analysed for each patient.
Results
122 patients with CKD 4 (88 patients, 72%) and CKD 5 (34 patients) were indentified. 68 (56%) were male and 54 female. Age at death ranged from 22 to 93 years, median 78 (IQR 71-85).The cause of CKD was unknown (EDTA code 00) for 53 patients (43%), atherosclerotic renal artery disease for 21 (17%), diabetes for 19 (16%) and acquired obstructive uropathy for 5 (4%). Estimated GFR (MDRD) at the time of last clinic review prior to death ranged from 4.3 – 29.9 ml/min, mean 18.3 (SD 6.02). The period of follow-up from first referral to renal services until last clinic visit ranged from <1 to 152 months, median 18 (IQR 8-48). The period between last clinic visit and death ranged from <1 to 95 months, median 2 (IQR <1-4).Conservative care had been identified as the treatment of choice for 39 (32%) patients, with management from the conservative care specialist nurse. Of these 24 (62%) had CKD4. 22(18%) patients had a positive plan for HD but of these 6(5%) had palliative approach adopted when admitted with their terminal illness. 7(6%) had planned for PD. 13(11%) patients had an AV fistula at time of death, and a further 7(6%) had been referred for AV fistula formation. For 45 patients there had been no discussion of RRT nor conservative care, only 3 of these patients had CKD stage 5.Cause of death was available for 72 (59%) patients. Ischaemic heart disease was the most common cause, leading to death in 24 patients (20%). Infection caused death in 14 (11%), 11(9%) died of malignancy, 6(5%) were certified with renal failure as primary cause.
Conclusions
154 patients started RRT in RIE between 1/1/08 – 30/6/09. During the same time period 122 patients died with stages 4 and 5 CKD, 39 of whom were on the conservative care programme. If all patients on this programme started RRT instead, there would need to be a 20% increase in capacity for incident patients to RRT. 20 patients had vascular access surgery or assessment for such surgery but never had haemodialysis. 3 patients with CKD 5 at their last clinic visit had no discussion to formulate a plan for management of their end stage renal disease.

11. RENAL FUNCTION IN PATIENTS FOLLOWING LIVE DONOR NEPHRECTOMY.
Galbraith NJ 1 , Brown K 2 , Geddes CC 3 , Buist LJ 2 1 SSM Medical Student, University of Glasgow; 2 Renal Transplant Unit, Western Infirmary, Glasgow; 3 Dept of Nephrology, Western Infirmary, Glasgow.
BackgroundFollowing living kidney donation there is compensatory hypertrophy in the remaining kidney. The aim of this study was to determine the level of glomerular filtration rate (GFR) compensation in the year after kidney donation and to determine if gender, age or pre-nephrectomy GFR influence this compensation.
Method103 people donated a kidney between January 2004 and September 2008 in the West of Scotland. All patients had isotopically measured GFR pre-donation. We estimated GFR in the year following kidney donation using the following formula: GFR = Preoperative Isotope GFR x (Serum creatinine/Preoperative Serum Creatinine) which will be accurate if muscle mass does not change in this time.
ResultsMedian age for the sample was 45.9 years (Range 24.4 – 77.2 years) and 49 were male. 53 had full 1 year follow up. Mean GFR pre-donation was 100.1 ml/min/1.73m2 (SD 18.2 ml/min/1.73m2).GFR calculations were 76.5% (3 days), 74.2% (2 weeks), 76.4% (3 months) and 79.4% (1 year) of pre - donation level during follow up.
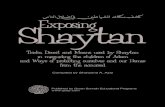
Mean GFR Changes Following Donor Nephrectomy
79.4
76.474.276.5
100
0
20
40
60
80
100
-28 0 28 56 84 112 140 168 196 224 252 280 308 336 364 392
Days since transplant
GFR expressed as % of pre-op isotopically
measured value
There were no statistically significant differences in the rate of change in GFR over 1 year when subanalyses by gender, age or pre-nephrectomy GFR were performed.
Conclusion:In conclusion, patients who have undergone donor nephrectomy have a GFR of 79.9% (SD 10.1%) of that before they donated a kidney. This compensation occurs mostly within the first few days after donation.

12. PHOSPHATE LEVEL, GRAFT FAILURE AND MORTALITY IN RENAL TRANSPLANT RECIPIENTS.
Kate K Stevens, Raj K Patel , Colin C Geddes, Alan G Jardine, Christian Delles Renal Unit, Western Infirmary, Glasgow G11 6NTBHF Cardiovascular Research Centre, University of Glasgow, G12 8QQ
Background
There is an increased prevalence of cardiovascular disease in renal transplant recipients; traditional risk factors do not explain this adequately. Phosphate has been identified as an independent predictor of mortality in both dialysis patients and renal transplant recipients. Additionally an elevated phosphate has been linked with increased risk of graft dysfunction. This retrospective study looked at renal transplant recipients and at factors which predict graft loss and death.
Method
The computerised records and case notes of all patients who received a first cadaveric transplant between 01/01/1999 and 31/12/2004 were reviewed. Demographic data including primary renal diagnosis, date of first dialysis and age at transplantation was recorded. Blood pressure, weight, renal function, bone biochemistry and haemoglobin were recorded at one year, five years and ten years (where available) from the date of transplant. Cause of death and graft failure were also noted.
Results
In this 6 year period, 239 patients received a first cadaveric transplant of whom 35% (n=86) were female. At the time of transplantation the mean age was 45.3 ±13.4 years, 17.2% (n=41) were smokers, 10.4% (n=25) were diabetic and 17.6% (n=42) had a history of cardiovascular disease. Median time on dialysis pre transplant was 1006 days (0-5077) and median follow up time was 2749 days (379-3919). At follow up, 207 patients were alive and 32 were dead. Compared with those who were still alive at the end of the follow up period, those who died were older at the time of transplantation (p=0.005) and had higher serum creatinine (p=0.001) and phosphate (p=0.023) at 1 year. They were also more likely to have graft failure (p=0.004). In Kaplan-Meier analysis, serum phosphate ≥1.15mmol/L at 1 year post transplant was a significant predictor of death (p=0.018). In Cox regression analysis, adjusting for serum creatinine at 1 year, diabetes, smoking status, presence of cardiovascular disease at transplantation, sex and age, serum phosphate ≥1.15mmol/L remained a significant predictor of survival. Patients with diabetes and smokers were significantly more likely to have died during follow up. (Median survival 3650 days v 2798 days and 3635 days v 3339 days respectively). In 40 patients, the transplant failed. 11 of these patients died. Serum phosphate levels both at 1 and 5 years post transplant were significantly higher in the graft failure group compared with those whose graft continued to function (1.19±0.06 v 0.96±0.23 (p=<0.001) at 1 year and 1.3±0.6 v 0.98±0.25 (p=<0.001) at 5 years).
Conclusion
Serum phosphate levels at the upper end of the normal reference range are associated with increased mortality and graft failure in renal transplant recipients. The effect of phosphate is independent of some of the other traditional cardiovascular risk factors. However, serum phosphate is modifiable with dietary and pharmacological measures and might be an important therapeutic target to help reduce mortality in the renal transplant recipients.

13. CYTOMEGALOVIRUS: A MAJOR CONCERN FOR THE OUTCOMES OF RENAL TRANSPLANTATION?
C J Stewart, L K Henderson, L P Marson, W Metcalfe, The University of Edinburgh, East of Scotland Renal Transplant Unit
Background
Despite the reduction in acute rejection post-transplantation (PT) with changing immunosuppression, there has been no substantial improvement in long-term graft and patient survival over recent years. One modifiable risk factor that has not been fully elucidated is the impact of Cytomegalovirus (CMV) infection.
Aims
To examine the indirect effects of CMV on graft survival, patient survival, graft function and opportunistic infection 0-18 months PT a retrospective review of all renal transplant recipients was conducted at the Royal Infirmary of Edinburgh from January 2006-May 2009. Patients & Methods
215 renal transplants were analysed (Group I patients with CMV, n=30; Group II patients non-CMV, n=185, CMV Infection defined as CMV PCR ≥100 + clinical signs/symptoms of infection). The four transplantation outcomes were compared between each group by SPSS14, 2005 (using chi-squared analysis, two-way ANOVA and independent samples t-tests as appropriate, p<0.05 considered statistically significant). There was no significant difference between the two groups in terms of %MMF immunosuppression, donor age, cold ischaemic time, graft type, DR mismatch or rejection.
Results
Graft survival was lower in Group I (80.0%, n=24/30) compared to Group II (88.6%, n=164/185) without showing significance. Patient survival was significantly lower (p=0.003, odds ratio (OR)=10.2) in Group I (90.0% 27/30) compared to Group II (98.9% 183/185). The average graft function 3-15 months PT was significantly lower in Group I compared to Group II (p<0.01). Opportunistic Infection (OI) was significantly higher (p=0.027, OR=2.5) in Group I (66.7%, 20/30 with >1 OI) compared to Group II (44.9%, 83/185 with >1 OI).Discussion: This evidence supports growing concern that the indirect effects of CMV infection have a significant impact on patient survival, graft function and opportunistic infection 0-18 PT. Although we have improved our prophylaxis, treatment and detection of CMV, persistent infection and viraemia are likely contributing to co-morbid immunological events.

14. THE ROLE OF TRANSPLANT NEPHRECTOMY FOLLOWING GRAFT FAILURE
Pete C Thomson, Colin C Geddes , Renal Unit, Western Infirmary, Dumbarton Road, Glasgow
IntroductionPatients with failed renal transplants do not routinely undergo transplant nephrectomy following their return to dialysis. In some instances, however, transplant nephrectomy is required. This may be soon after graft failure when associated with acute illness or in the context of a more chronic inflammatory illness related to transplant rejection. The aim of this study was to identify the incidence of patients undergoing transplant nephrectomy following a return to dialysis, determine why nephrectomy was conducted and compare the clinical characteristics of those who underwent transplant nephrectomy with those who did not.
MethodsAll patients who had attended the Glasgow Western Infirmary renal transplant unit between 01/01/1968 and 01/08/2009, were registered on the unitary electronic patient record (EPR) and were noted to have a failed renal transplant were identified. Baseline clinical, laboratory and demographic data were recorded. This included age, sex, primary renal diagnosis, date of transplant, type of transplant, date of transplant failure, cause of transplant failure and whether transplant nephrectomy was undertaken. Duration of follow-up within the renal unit and subsequent mortality were recorded. Comparison of nephrectomy and non-nephrectomy groups was made by parametric and non-parametric testing with a significance level of <0.05.
ResultsA total of 774 patients experienced 994 episodes of renal transplant failure between 01/01/1968 and 01/08/2009. 468/774 (60.1%) of patients were male with a mean age at first transplant of 35.9yrs. Primary renal diagnosis was determined as glomerulonephritis in 243/774 (31.4%) cases, interstitial nephropathy 295/774 (38.1%), multisystem disease 78/774 (10.1%), diabetes 39/774 (5.0%) and unknown causes 119/774 (15.4%).
A total of 919/994 (92.4%) failed transplants were from cadaveric donors whilst 75/994 (7.6%) were from live donors. 384/994 (38.6%) episodes of transplant failure were followed by transplant nephrectomy. 223/384 (58.1%) nephrectomies occurred within 4 weeks of transplant failure with 21/384 (5.5%) occurring >52 weeks after failure.
Discounting those patients with transplant nephrectomy within 4 weeks of failure, those who subsequently underwent transplant nephrectomy were found to be similar in age at transplantation (33.4yrs v 33.3yrs, p=0.95), duration of renal transplant (5.1yrs v 4.6yrs, p=0.32), rates of transplant rejection causing failure (42.1% v 36.9%, p=0.26) and rates of mortality (13.4yrs v 14.5yrs, p=0.585) to those in whom the transplant was left in-situ. Transplant nephrectomy was found to occur more commonly in patients with chronic allograft nephropathy as opposed to those without (7.1% v 3.3%, p=0.045).
ConclusionNearly 40% of patients with a failed renal transplant are likely to undergo transplant nephrectomy. In up to 60% of cases this will occur in the first 4 weeks following transplant failure and return to dialysis. Patients who underwent transplant nephrectomy after 4 weeks from transplant failure were found to share similar clinical characteristics to those whose renal transplant was left in situ. A diagnosis of chronic allograft nephropathy appeared to be associated with a significantly higher risk of undergoing subsequent transplant nephrectomy.

15. GENE VARIANTS OF THE RENIN-ANGIOTENSIN SYSTEM IN KIDNEY TRANSPLANTATION – ARE THEY IMPORTANT?
John Irvine 1 , Katrina Ellis 1 , Chris Frampton 1 Mark Richards 1 , Zoltan Endre 2 Murray Leikis 3 and Vicky Cameron 1 1Christchurch Cardioendocrine Research Group, Department of Medicine, University of Otago, Christchurch, New Zealand2Renal Research Group, Department of Medicine, University of Otago, Christchurch, New Zealand3Department of Renal Medicine, Wellington Hospital, Wellington, New Zealand
Introduction
Increased activity of the renin-angiotensin system (RAS) has been implicated in decreased long-term survival of renal allographs. Single nucleotide polymorphisms (SNPs) of the angiotensin II type I receptor (AGTR1) have been associated with increased RAS activity. The aim of this study was to investigate whether haplotypes (DNA variants within a gene inherited in combination) in the AGTR1 gene provide prognostic information for long-term outcome of kidney transplants.
Methods
This is a retrospective study. Grafts not functioning at 90 days were excluded. Kidney transplants (n=338) and living donors (n=166) from two transplant centres were genotyped for 3 ‘tag’ SNPs (rs718858, rs1492099, rs12721331) from the AGTR1 block 2 haplotype. Haplotypes for each chromosome pair were stratified into two groups based on a phylogeny tree diagram estimating the genealogical relationships amongst recipient transplant haplotype combinations. The primary outcome was graft survival at 10 years.
Results
All 3 SNPs were in Hardy Weinberg equilibrium. Haplotype frequency did not differ when stratified by ethnicity. Eleven different haplotype paired combinations were identified in this transplant cohort of whom 7 accounted for 97.9% of the total variation observed. Cumulative survival by Kaplan-Meier survival curve showed a trend for transplant recipients with two copies of the wild-type allele haplotype to have a better graft survival (p=0.07) at 10 years, compared with living donors having one or no copies.Transplants from living donors with two copies of the wild-type allele haplotype had a significantly improved recipient 10-year graft-survival (p=0.042). A low-risk group of transplants with the recipient, living donor or both having a wild type allele haplotype for both genes, had significantly better graft outcome at 10 years compared with a high-risk group having no wild-type allele haplotypes (p=0.023). Univariate analysis between the low and high-risk groups comparing known variables that influence graft outcome at the time of transplantation did not identify any risk factors significantly associated with haplotype. Cox proportional hazard analysis revealed the association between the AGTR1 haplotype block 2 risk-groups was independent of established predictive factors of graft survival at transplantation, including PRA, peak PRA and HLA DR mismatch (p=0.041, HR 3.6, 95% CI 1.1 – 12.7).
Conclusion
In this cohort of kidney transplant recipients, AGTR1 haplotype block 2 may provide prognostic information for 10-year graft survival.

16. TRANSPLANTS IN TRANSITION - RENAL TRANSPLANT PATIENTS MOVING FROM PAEDIATRIC TO ADULT CARE IN GLASGOW.
Sheena Morrison, Frank Willis, on behalf of the Renal Units, Royal Hospital for Sick Children, Yorkhill, and the Western Infirmary, Glasgow
Introduction
This project aims to look at the outcomes of renal transplant patients moving from the Royal Hospital for Sick Children (Yorkhill) to the Western Infirmary, Glasgow. By its very nature, the period of transition from paediatric to adult health sectors coincides with the onset of adolescence and its associated risk taking behaviours. In looking at the over all outcomes of these patients the aim was to identify any apparent trends occurring at the time of transition which would merit further investigation in future projects.
Methods
Patients were identified from the relevant databases: the Western PROTON system and the combination of HISS, PROTON and archived notes at Yorkhill. The information extracted was gender, diagnosis, age at time of transplant and transfer, serum creatinine at one year pre transition, transition and 1 year post transition.
Results
Of 42 patients initially identified, complete data were available for 32 (18 male, 14 female). 17 (53%) transplants failed post transition and 15 (47%) were still functioning with median follow-up 5 years after transition. Patients with more recent transplants appeared more likely to lose their grafts, but the trend did not reach statistical significance.
Conclusions
These results are consistent with previous reports of high graft loss in this age group. The suggestion of a worse outcome after transition for more recent transplants merits further study, in order to optimise arrangements for transition.
Funding:NoneConflict of interest: None

17. DELIVERY OF RENAL CARE AND SERVICES IN ADULT RENAL UNITS: THE VIEWS OF SCOTTISH TRANSPLANT PATIENTS ON THEIR CLINIC ENVIRONMENT DURING LONG TERM FOLLOW UP.
Pearce Cusack, Wendy Forbes, Fiona Russell, Karen Ritchie, Chris Isles on behalf of the NHS QIS Adult Renal Services Steering Group
Background
Recent Renal QIS surveys were designed to assess the views of dialysis and transplant patients on the delivery of renal care and services in adult renal units. A preliminary report of the transplant survey was given to the SRA by Dr Caroline Whitworth in March 2009. We have since conducted further analyses of the data and now present the views of patients on their clinic environment in the nine units in which transplant follow up is undertaken.
Methods
The Scottish Renal Registry provided the names and postal addresses of all adult renal transplant patients in Scotland. All 1938 transplant patients received a postal questionnaire in November 2008. Response rates varied from 55% in Inverness to 74% in Aberdeen. Overall response was 63% which is high for a postal survey. Respondents were asked to grade different aspects of their out-patient area as good, average or poor. Those rating their units as ‘good’ are shown in the table which also includes an overall rating of the clinic environment which we derived by adding the percentages and dividing by the number of domains.
Cleanlinessof the area%
Comfort
%
Accessibility
%
Generalsurroundings%
Toilets
%
Waiting area%
Overall%
ARI 69 45 78 47 54 39 55XH 86 75 87 73 62 76 76DGRI 97 93 100 100 100 90 97MONK 97 79 92 76 87 76 85NINE 75 59 87 57 54 54 64QMH 64 36 71 34 47 45 50RAIG 73 44 66 45 43 39 52RIE 80 60 84 66 75 62 71WIG 54 35 61 34 37 31 42
Results
Responses indicate considerable variation in patient experience between units. Units scoring highly in one environmental domain were likely to score highly in another and tended to maintain the same ranking within each domain. The most recently upgraded unit, Dumfries, appeared to offer the best out-patient clinic environment, while patients attending the Western Infirmary in Glasgow were least satisfied. We note that these patients, representing 40% of respondents in our survey, have since transferred to new transplant clinics at the New Victoria and New Stobhill Hospitals in Glasgow. The differences between units were statistically significant by chi-squared test, for each domain shown.
Conclusion
The QIS transplant survey suggests there are large differences in the quality of the environment of the transplant follow up clinics in Scotland.

18. IDIOPATHIC MEMBRANOUS NEPHROPATHY (IMN) – HAS PRACTICE OR OUTCOME CHANGED IN THE LAST 10 YEARS?
Emily P McQuarrie 1 , Catherine Stirling 2 . 1. Renal Research Group, University of Glasgow. 2. Renal Unit, Glasgow Royal Infirmary
Aim
Who, when and how to treat IMN remains contentious and the results of the MRC trial are awaited. We examined our practice in a single renal unit over the last 10 years and compared it with a previous cohort.
Methods
All patients with biopsy proven membranous nephropathy diagnosed between 1997 and 2007 were retrieved from our electronic database. Baseline and follow-up data were obtained, including details about immunosuppression and outcome. This was compared with a previously published series from the same unit, 1986 to 1996, n=53.
Results
65 patients were identified, of whom 48 had IMN. At diagnosis, mean age was 61.3y, mean eGFR 61 ml/min and mean proteinuria 6.4g/24hr. 58% were nephrotic and 80% were male. 12 patients (25%) were treated with immunosuppression, all of whom were nephrotic. 23 patients (52%) were in complete or partial remission at follow up (mean 5.1 y). 16 patients (36%) had a spontaneous remission. 3 progressed to ESRD (7%) and 5 died (11%). Patients who were treated with immunosuppression were significantly younger, more likely to be male, nephrotic and had better renal function at diagnosis. Median time to treatment was 329 days. 3 patients (25%) failed to complete treatment due to complications. Compared with the previous cohort, fewer patients were immunosuppressed (25% vs 36%). However they were also older (61.3 v 53.8y) and has less severe renal disease at diagnosis (mean QP 6.4g/24hr v 8.3g/24hr). Renal outcomes improved with 52% achieving remission at follow up (v 47%) and fewer patients developed end stage renal failure (7% v 13%) or died (11% v 15%).
Discussion
This study demonstrates that we are still conservative in our use of immunosuppression in patients with IMN (25% of patients), but that outcomes are similar or better compared with historical controls. There are a number of reasons for our selective approach to immunosuppression which include an older population and uncertainty about the evidence of benefit of immunosuppression. We believe that the high spontaneous remission rate may be related to ACE/ARB use (94% patients) and that results from the MRC trial will help direct future treatment decisions.

19. URINARY IGG:CREATININE RATIO IS SUPERIOR TO URINARY PROTEIN EXCRETION IN PREDICTING RENAL OUTCOMES IN PRIMARY GLOMERULONEPHRITIS.
E.P. McQuarrie 1 , L Shakerdi 2 , A.G. Jardine 1 , J.G. Fox 2 , B. Mackinnon 2 . 1. Renal research group, University of Glasgow. 2. Renal Unit, Glasgow Royal Infirmary
Aim
Established predictors of progression in CKD include blood pressure, proteinuria and baseline renal function. We have previously shown that high molecular weight proteinuria correlates best with the rate of progression of CKD. One such molecule is IgG (molecular weight 150 kDa) and this study aimed to assess whether the ratio of urinary immunoglobulin G to urinary creatinine (IgG:Cr ratio) was superior to baseline proteinuria in predicting renal outcome.
Methods
128 patients with primary glomerulonephritis (GN) (39 IgAN, 36 membranous GN, 29 FSGS, 24 others) were prospectively recruited between November 2001 and April 2002 from the renal clinics at Glasgow Royal Infirmary. Baseline demographic and clinical data were collected. Total proteinuria was measured by nephelometric assay, urinary IgG excretion by ELISA. The primary composite outcome measure was GFR falling below 15 ml/min, need for renal replacement therapy or death.
Results
Patients were followed up for a mean period of 7.3 years. 87 (68%) were male. Mean age at recruitment was 54.0y (SD 16.3), mean eGFR (by 4 point MDRD) was 50ml/min (SD 24.2ml/min). Median 24h protein excretion was 1100mg/24h (IQR 213-2911), median urinary IgG excretion was 12.7mg/l (IQR 4.4-65.3) and median urinary IgG:Cr ratio 2.0mg/mmol (IQR 0.7-11.4). Over the period of follow up 34 patients progressed to the primary outcome. Median decline in GFR for the whole cohort was 0.7ml/min/yr.
The urinary IgG:Cr ratio correlated significantly with the primary endpoint (Spearman’s rho 0.467 p=0.000) and slope decline in GFR (r=0.384 p<0.001). 24 hour proteinuria also correlated significantly with the primary endpoint (r=0.452 p<0.001) and slope decline (r=0.404 p<0.001). Both variables also highly correlated with each other (r=0.828, p<0.001). Receiver operating characteristics (ROC) curves were constructed to determine the area under the curve (AUC), assessing the utility of both variables in predicting the primary outcome. The AUC for the IgG:Cr ratio was 0.806 (95% CI 0.727-0.871); AUC for protein excretion was 0.795 (95% CI 0.714-0.862). Logistic regression established that both variables predict outcome when entered separately into the model, however to establish whether urinary IgG:Cr ratio predicted outcome, independent of total urinary protein excretion, Cox proportional hazards model was performed. Urinary IgG:Cr ratio remained predictive (p=0.024, HR 1.013, 95% CI 1.002-1.025) whilst proteinuria was not (p=0.694).
Conclusion
The urinary IgG:creatinine ratio is a simple, novel marker for risk of progression to end stage renal failure or death, and is superior to urinary protein excretion, in a prospective cohort of patients with primary GN with extensive follow-up.

20. RENAL DYSFUNCTION IN AN ELDERLY POPULATION PRESENTING FOR ELECTIVE ORTHOPAEDIC SURGERY.
Christopher Hawthorne, Department of Anaesthetics, Hairmyres Hospital, East Kilbride and William Smith, Renal Unit, Monklands Hospital, Airdrie, Lanarkshire.
I ntroduction
In a previous database survey of 1300 elderly primary care patients we found that 43% had an eGFR of less than 60 ml/min using the MDRD-4 formula (1). A recent analysis of renal dysfunction in over 1500 patients with fractured neck of femur found that 36% of patients had an eGFR of less than 60 ml/min (2). This has significant implications for peri-operative management. We investigated the prevalence of renal dysfunction in patients presenting for elective orthopaedic surgery.
Methods
We analysed eGFR values in 100 consecutive elderly patients (>65 years), presenting for elective orthopaedic surgery using the MDRD-4 and Cockcroft Gault formulae. A retrospective review of pre-operative assessment documentation revealed details of co-morbidities and the patient’s weight. If patients had a follow-up serum creatinine measured between 6 and 24 months then this was used to calculate a post-operative eGFR for comparison.
Results
Documentation was available for 99 out of 100 patients. Using the MDRD-4 formula, 28% of patients presenting for elective orthopaedic surgery had an eGFR <60ml/min. These patients were more likely to suffer from diabetes, hypertension or ischaemic heart disease. There was sufficient data to calculate pre-operative and follow-up eGFR using both the MDRD-4 and Cockcroft Gault formulae for 82 patients. Twenty five of the 82 patients (30%) had a pre-op eGFR of <60ml/min by the MDRD-4 formula. Using the Cockcroft Gault formula, 21 of the 82 patients (26%) had an eGFR of <60ml/min. There was no deterioration in eGFR on the follow-up sample. Indeed, in patients with a pre-operative eGFR of <60ml/min, only 52% had a follow-up eGFR of <60ml/min.
Discussion
This study demonstrates a prevalence rate of chronic kidney disease in elderly patients presenting for elective orthopaedic surgery of between 26% and 30% depending on the calculation used. This has implications for peri-operative management. However, from the cohort of patients who had a follow-up creatinine, there was no evidence of deterioration in eGFR at 6-24 months. Indeed there was an apparent improvement in some, perhaps due to the reduction in non-steroidal analgesic use. Therefore, it may not be appropriate to refer all elderly patients with impaired eGFR to renal services.
References
1. Shah IM, Barber JM, Simpson E and Smith WGJ. Prevalence of renal dysfunction in an elderly Scottish population. British Geriatric Society 2008: abstract 54
2. White SM, Rashid N and Chakladar A. An analysis of renal dysfunction in 1511 patients with fractured neck of femur: the implications for peri-operative analgesia. Anaesthesia 2009; 64: 1061-1065.

21. COMBINED ACUTE EOSINOPHILIC INTERSTITIAL NEPHRITIS AND MINIMAL CHANGE DISEASE INDUCED BY CLARITHROMYCIN.
Aileen Helps, Wendy Russell and William SmithRenal Unit, Monklands Hospital, Airdrie ML6 0JS, Lanarkshire, UK
We describe a case of acute eosinophilic interstitial nephritis and minimal change nephropathy
induced by the macrolide antibiotic, clarithromycin. The patient showed features of acute non-
oliguric kidney injury, nephrotic syndrome, microscopic haematuria, eosinophilic pneumonitis
and a maculopapular skin rash.
The combination of minimal change nephropathy and interstitial nephritis secondary to
clarithromycin has not been documented previously although drug-induced acute interstitial
nephritis is well recognised. The simultaneous occurrence of minimal change disease and
interstitial nephritis as described above has been cited on rare occasions with non steroidal
anti-inflammatory agents and amoxicillin, but not with clarithromycin.
The optimum treatment of acute interstitial nephritis is controversial although steroids are the
accepted treatment of minimal change nephropathy. Steroid therapy and cessation of
clarithromycin in this patient resulted in complete clinical resolution of both pathologies within 3
months.

22. CHARACTERISATION OF THE CELLULAR AND MOLECULAR PATHWAYS OF ARTERIOVENOUS FISTULA FAILURE.
Jackson AJ, Geddes C, Kingsmore DB, Coats PDepartment of Renal Transplant, Western Infirmary, Glasgow
Introduction
Failure of arteriovenous fistulae (AVF), the preferred mode of haemodialysis, represents a huge clinical problem. At 6 months patency rates are estimated at 71 and the cost to the NHS of fistula failure £84.1m per annum. The commonest cause of AVF failure is occlusion of the venous segment. Despite the magnitude of the problem, little is known regarding the pathobiology of this process. We present novel preliminary data highlighting key mechanisms underlying AVF failure.
Methods
Cephalic vein tissue from failed AVF was obtained and sections were wax embedded or cultured to obtain vascular smooth muscle cells (VSMC) by explant method. Healthy saphenous vein obtained from patients undergoing varicose vein surgery was processed similarly and used as a control. The architecture of failed AVFs was determined using haematoxylin and eosin staining. Proliferation of VSMC’s from AVFs was compared to healthy controls using thymidine incorporation. P42/44 MAP kinase expression in response to growth factors PDGF and PMA in VSMC from AVFs and saphenous vein was determined by western blot. IL-6 secretion from AVF and control VSMC was measured by ELISA.
Results
As expected, failed AVF demonstrated luminal occlusion of the cephalic vein segment. VSMCs derived from AVF demonstrated significant upregulation of proliferation in response to foetal calf serum (FCS) in a concentration-dependent manner when compared to control. The proliferation response in VSMCs obtained from AVF tissue was significantly greater when compared with saphenous vein control. (n=4 p<0.05)
The increased proliferative responses could be correlated with a significant increase in MAP kinase expression in response to PDGF and PMA stimulus (AVF-derived VSMC vs. Control; n=3 p<0.5).
IL-6 a key inflammatory cytokine was measured. Despite no difference in background production of IL-6 when challenged with PMA VSMCs derived from AVF cells secreted significantly more IL-6 when compared with saphenous vein control (n=3 p<0.05).
Conclusion
We present novel data derived form failed human AVFs. The occlusion of the vein lumen can be characterised by invasion -actin positive cells; likely VSM and myofibroblasts. Cells derived from the AVF display a hyperproliferative phenotype with enhanced proliferation and expression of the proliferation-associated p42/44 MAP Kinase pathway. Interestingly we observed increased capacity of AVF derived cells to secrete IL-6. This is an important observation and suggests a potentially significant involvement for inflammatory pathways in AVF failure.
Research is underway to further characterise the pathobiology of AVF failure and identify potential pharmacological inhibitors of this process.

23. CHRONIC ENDOTHELIN-A RECEPTOR ANTAGONISM REDUCES PROTEINURIA, BLOOD PRESSURE & ARTERIAL STIFFNESS IN CHRONIC KIDNEY DISEASE.
Iain MacIntyre, Neeraj Dhaun, Debbie Kerr, Vanessa Melville1, Neil Johnston,Jane Goddard, David WebbClinical Pharmacology Unit, University of Edinburgh, Queen's Medical Research Institute Edinburgh, EH16 4TJ, UK.
Background
Blood pressure (BP) and proteinuria reduction slow chronic kidney disease (CKD) progression. Acute ETA receptor antagonism reduces BP and proteinuria in CKD. We investigated if these effects are maintained longer term.
Methods
In a randomised double-blind, 3-way crossover study 27 subjects received 6 weeks of placebo, sitaxsentan 100mg and nifedipine 30mg. All subjects were optimally treated with renin-angiotensin system blockade. 24h proteinuria, protein:creatinine (PCR), 24h BP, and pulse wave velocity (PWV), as a measure of arterial stiffness (AS) were measured at baseline and week 6 of each treatment period.
Results
All subjects completed the study. Compared to placebo, sitaxsentan significantly reduced proteinuria (24h proteinuria: -31±23%, p<0.005; PCR: -29_23%, p=0.01), BP (24h mean arterial BP: -4±6mmHg, p<0.01), and AS (PWV: -5±9%, p<0.01). Nifedipine matched the BP reduction with sitaxsentan (p=0.65) and produced a similar fall in PWV. Despite this sitaxsentan reduced proteinuria to a greater extent than nifedipine (24h proteinuria: -31±23 vs 10±46%, p<0.01, PCR: -29±23 vs -5±33%, p=0.01). Sitaxsentan did not cause clinically significant side effects, or weight gain.
Conclusion
6 weeks sitaxsentan treatment produces significant, clinically relevant reductions in proteinuria and BP in CKD subjects. These effects appear, in part, to be BP independent. AS also improves. Overall, sitaxsentan is well tolerated. Larger, longer-term studies are warranted.

24. A RETROSPECTIVE STUDY OF THE TREATMENT OF ADULT ONSET MINIMAL CHANGE NEPHROPATHY.
Catherine Maclean, Bruce MacKinnon, Jonathan Fox, Renal Unit, Glasgow Royal Infirmary
Introduction
Minimal change nephropathy (MCN) is one of the causes of idiopathic nephrotic syndrome characterised by foot process effacement, the absence of immune deposits and a functional defect in glomerular permeability. The pathogenesis is unclear. MCN is well studied in the paediatric population where complete remission occurs in up to 90% of cases. Similar response rates in adults have not been achieved.
Methods
We carried out a retrospective study looking at the treatment of idiopathic adult onset MCN in the database of patients from 4 Scottish hospitals using a combination of electronic retrieval (patient demographics and basic clinical data) and manual retrieval (results and prescription records). Criteria for proteinuria were ACR>20, PCR>30, QP>0.3. Any proteinuria above this was a relapse.
Results
149 patients with a diagnosis of MCN were identified. Fourteen were excluded as secondary MCN. Twenty five were excluded as paediatric MCN. The total number of adult onset MCN cases was 110 patients. Where data was incomplete, the subset of patients with available data was considered. Ninety two percent had biopsy confirmation recorded on the database; mean age was 46.6 years; 57% were male; mean duration of follow up 8 years. Thirty nine percent had non-visible haematuria at presentation; mean BP at presentation 137/82; 14% had acute kidney injury at presentation (serum creatinine >120% of baseline creatinine). All patients received prednisolone, average dose 56mg (0.81mg/kg), median duration of treatment was 113 days. Twenty two percent relapsed before completing a course of prednisolone; 32% received second line agents (cyclophosphamide, cyclosporin) and five patients received “third line” agents (cyclophosphamide, cyclosporin, mycophenolate, tacrolimus).There were 232 episodes of proteinuria. Forty nine percent of patients had a single episode of proteinuria without further relapse. The average number of episodes of proteinuria was 2.5 per patient.
Funding: None Conflict of Interest: None

25. PROTEIN:CREATININE RATIO IS SUPERIOR TO ALBUMIN:CREATININE RATIO AS A PREDICTOR OF PATIENT OUTCOMES IN CHRONIC KIDNEY DISEASE.
Shona Methven 1 , Mark S MacGregor 1 , Jamie P Traynor 2 , Mario D Hair 3 , Denis StJ O’Reilly 4 , Christopher J Deighan 5 1 John Stevenson Lynch Renal Unit, Crosshouse Hospital 2 Renal Unit, Monklands Hospital 3 University of the West of Scotland 4 Department of Biochemistry, Glasgow Royal Infirmary 5 Renal Unit, Glasgow Royal Infirmary.
Introduction In patients with chronic kidney disease (CKD) proteinuria is the most important predictor of both progression and the development of end-stage renal disease. The relative importance of total protein: creatinine ratio (TPCR) and albumin: creatinine ratio (ACR) in non-diabetic kidney disease is not well established. Only TPCR takes account of both albumin and non-albumin proteinuria. Our laboratory measures ACR and TPCR on all urine samples from the kidney clinic.
MethodsWe retrospectively assessed the performance of ACR and TPCR to predict outcomes in 5,586 patients attending our clinic between 1999 and 2008, using a hierarchical Cox regression survival analysis with age, gender, blood pressure and serum creatinine as co-variates entered in the first block and either ACR or TPCR entered in the second block. .
ResultsAge (mean ± standard deviation) was 59±17 years, and 50% were male. Baseline serum creatinine (median [interquartile range]) was 140 [100-190] micromol/L, eGFR 42 [28-63] ml/min/1.73m2. Blood pressure was 144/78 27/14 mmHg, ACR 10 [2 - 48] mg/mmol, and TPCR 35 [17 - 106] mg/mmol. Patients were followed up for median 3.5 [2.1-6.0] years, during which 844 (15%) died at 3.0 [1.8-4.7] years and 468 (8%) started renal replacement therapy (RRT) at 1.7 [0.6-3.4] years. Unadjusted and adjusted (for covariates) hazard ratio (aHR) for all cause mortality, commencement of RRT and doubling of serum creatinine (sCr) are shown in Table 1. In every case TPCR has a higher hazard ratio. To assess performance in the microalbuminuria range, proteinuria was also assessed as a categorical variable. Compared to normoalbuminuria (ACR <3mg/mmol) microalbuminuria (ACR 3 – 30mg/mmol) conferred a hazard ratio of 1.59 (1.28 – 1.98) and the equivalent TPCR (15 – 50mg/mmol) conferred a hazard ratio of 1.63 (1.27 – 2.11).
ConclusionTPCR is superior to ACR as a predictor of outcomes in CKD. This may reflect the importance of non-albumin proteinuria. Measuring ACR as well as TPCR increases costs but adds no additional prognostic information. TPCR performed well at low values in this study, and merits further investigation.
Table 1 Hazard ratios (95% confidence intervals) for ACR and TPCR to predict outcomes in patients with CKD
ACR TPCRUnadjusted HR Adjusted HR Unadjusted HR Adjusted HR
Death 1.49 (1.37 – 1.61)
1.43 (1.30, 1.57)
1.96 (1.76 – 2.18)
1.73 (1.52, 1.96)
RRT* 3.56 (3.14 – 4.04)
2.60 (2.26, 3.01)
5.43(4.67 – 6.30)
2.93 (2.47, 3.49)
Doubled sCr**
2.27 (2.09 – 2.46)
2.08 (1.91 – 2.27)
3.16 (2.85 – 3.50)
3.13 (2.74 – 3.58)

aHR adjusted for age, gender, blood pressure and serum creatinine as co-variates.* Serum creatinine is a time dependent co-variate for RRT ** Age is a time dependent co-variate for doubled sCr26. AN AUDIT OF THE USE OF CINACALCET IN THE WESTERN INFIRMARY RENAL UNIT, GLASGOW.
Joanna Hall, Heather Black, Colin Geddes, Neal Padmanabhan Renal Unit, Western Infirmary, Dumbarton Road, Glasgow, G11 6NT
Aims Cinacalcet is a calcimimetic licensed for treatment of secondary hyperparathyroidism in patients with ESRD on maintenance dialysis. Although cinacalcet improves biochemical control it has not been shown to reduce mortality in ESRD and its use is restricted according to strict criteria set by NICE and by local guidelines. These guidelines largely limit the use of cinacalcet to patients in whom parathyroidectomy is contraindicated and also require careful titration of the dose and early recognition of non-responders. We performed a retrospective audit of compliance with NICE and local criteria for cinacalcet use within the Western Infirmary Renal Unit.
MethodsWe used pharmacy records to identify patients treated with cinacalcet between June 2005 and February 2009 From the electronic database we obtained information relating to patient demographics, reason for initiation, cinacalcet dose and PTH levels at initiation and at 1, 3, 6 and 12 months, and whether parathyroidectomy was considered.
Results Eighty-four patients received cinacalcet within the audit period. Thirty-five patients were male and 49 female. The mean age was 54.3 years (range 18-87). Forty-eight (57%) were on dialysis, 29 (34.5%) were transplant patients and 7 (8.33%) were pre-dialysis. Seventy-two (85.7%) were initiated on cinacalcet for hyperparathyroidism, 7 (8.33%) for calciphylaxis and in 5 (5.95%) the reason was unknown. Five patients out of 55 (9.1%) met NICE selection criteria. Twenty-eight out of 84 (33.3%) met renal unit criteria.
The mean cinacalcet doses (mg) were 33 at initiation, 36.7 at 1 month, 46.3 at 3 months, 52.6 at 6 months and 65.8 at 12 months. Median cinacalcet doses (mg) were 30 at initiation, 30 at 1 month, 30 at 3 months, 60 at 6 months and 60 at 12 months. Mean PTH levels (pmol/l) were 79 at initiation, 60.7 at 1 month, 63.3 at 3 months, 67.3 at 6 months and 56.2 at12 months.
Reduction in PTH of >30% was documented in 22 (44.9%) patients at 1 month, 19 (42.2%) at 3 months, 16 (37.2%) at 6 months and 14 (56.0%) at 12 months. Dose titration for individuals with a PTH reduction of <30% from baseline was documented in 22 patients (14.8%) at 1 month, 19 (34.6%) at 3 months, 37.0% at 6 months and 27.3% at 12 months.
Thirty-two patients (44.4%) were discussed for parathyroidectomy: 17 (23.6%) underwent surgery and in 15 (20.8%) surgery was contraindicated. Thirteen (18.1%) were not referred: 3 (4.4%) chose not to have surgery and 10 (14.7%) were assessed by nephrologists as unfit. In 27 (37.5%) referral was not documented.
Five patients showed a PTH reduction of <30% with cinacalcet despite adequate dose titration but in only 2 was cinacalcet discontinued. Twenty-seven patients discontinued cinacalcet prior to 12 months: 2 discontinued by nephrologists due to lack of response, 5 due to adverse effects, 5 subsequently underwent parathyroidectomy, 1 underwent transplant and in 14 no reason for discontinuing could be identified.
ConclusionsThe majority of patients did not meet NICE or local criteria for the initiation of cinacalcet therapy. In less than half of the patients was there evidence that parathyroidectomy had been discussed, but this is likely to be an under-estimate. However, the monitoring of response to

therapy and dose-titration were also poor. Cinacalcet was frequently not stopped despite a lack of response after adequate titration. Strategies should be considered to improve adherence to guidelines and improve the use of this medication27. QUALITY OF LIFE IN MATCHED OLDER PERITONEAL AND HAEMODIALYSIS PATIENTS: RESULTS FROM THE BOLDE STUDY.
Lina Johansson, MSc 1 , Nigel Beckett, MD 1 , Michelle Clemenger 2 , Maria Da Silva-Gane 3 , Ken Farrington, MD 3 , Hugh Gallagher, MD 4 , Mary Hickson, PhD 2 , Tom Sensky, MD 1 and Edwina A Brown, MD 2 1 Imperial College London, UK; 2 Imperial College Kidney & Transplant Institute, UK; 3 Lister Hospital, Stevenage, UK; 4 St Helier Hospital, Carshalton, UK.
Aim
Broadening Options for Long-term Dialysis in the Elderly (BOLDE) is a 3 part study with the aim of extending choice of PD to older patients. To inform this choice, quality of life (QoL) has been assessed in matched HD and PD patients
Methodology
HD patients ≥65 years were matched to PD patients by age (± 2.5 years), gender, time on dialysis (± 1 year), ethnicity and socio-economic status (Index of Deprivation based on postcode). As well as several QoL measures, cognitive function (Mini Mental State Examination and Trail Making Test-B), nutritional status (Subjective Global Assessment) and intake were determined.
Results
70 pairs were studied. Matching was successful as shown by the following comparisons for HD and PD groups respectively: age (73.1 ± 5.5 vs 73.4 ± 5.1 years), gender (70% male), ethnicity (96% vs 90% British or European White), time on dialysis (30.5 ± 28.3 vs 31.4 ± 26.5 months), Index of Deprivation (13.7 ± 11.3 vs 13.7 ± 8.7), education (11.9 vs 11.7 years) and percentage living alone (27 vs 23 %). Stoke Davies co-morbidity score was higher in HD group with a median of 1.0 (IQR 1.0) vs 2.0 (IQR 2.0), p=0.009. Outcomes are shown in the table below:
Adjusted means scoresOutcomes (adjusted for comorbidities) PD HD p-valueSF12 Mental Component Score† 54.4 52.0 0.201SF12 Physical Component Score† 35.8 34.9 0.635Illness Intrusion Ratings Scale 25.2 30.1 0.017*HADS Anxiety 3.5 5.1 0.009*HADS Depression 4.2 5.4 0.019*Symptom severity 14.6 16.1 0.218Categorical outcomes PD% HD% p-valueDepression 10 25.7 0.013*Cognitive dysfunction 38.6 30.4 0.313At risk of malnutrition 16 24 0.205* significant at p=<0.05; † the higher the score the better the assessed QOL.
Conclusion
This study provides evidence that older patients on PD experience fewer depressive and anxiety symptoms and less illness intrusion in relation to the dialysis process compared to HD patients. We are now investigating the reasons for these differences, how older patients decide about dialysis modality and whether this information will enhance choice of PD in older people.

This is a 3 year study funded by Kidney Research UK via Baxter Healthcare with collaboration of the Renal Association and British Renal Society.

28. NATIONAL AUDIT OF PERITONEAL DIALYSIS RELATED PERITONITIS IN SCOTLAND, 2000-2007.
Michaela Brown, Keith Simpson, Jan Kerssens, Robert Mactier on behalf of the SRR
Peritoneal dialysis (PD) related peritonitis is the major cause of morbidity and technique failure in PD patients. UK Renal Association (RA) guidelines recommend: <1 peritonitis episode for every 18 months PD treatment, a primary cure rate >80%, and culture negative rate <20% . In Scotland all 10 adult renal units collect data prospectively relating to peritonitis, PD treatment failure and other clinical parameters, reporting data to the Scottish Renal Registry (SRR) 6 monthly. Complete audit data from all units 01/01/2000-31/12/2007 have been analysed for this study.
During 8 years there were 1918 peritonitis episodes in 38,106 PD treatment months giving a rate of 1 episode every 19.9 months. This represents a slight improvement from the SRR report 1999-2002. 8.4% of episodes were recurrences. The median peritonitis-free survival for incident PD patients was 526 days (95% confidence interval 463-589 days) from starting PD.
The peritonitis rate varied up to two-fold between units from an average of 1 episode every 15.7 months to 1 episode every 31.8 months. When averaged over the 8 years, 7 of 10 units met the RA target for peritonitis rate. Only 3 units have consistently met the RA standard every year for peritonitis rate. There has been no discernible, consistent improvement in peritonitis rate nationally or within units.
The 1918 episodes of peritonitis occurred in 965 patients. Of these, 671 patients had first started PD on or after 01/01/2000 (incident patients). The total incident PD population during this period was 1324 patients, therefore 50.4% of incident PD patients had experienced PD-related peritonitis during the audit period. The median number of episodes per patient was 1 (range 1-12 episodes).
For the 1324 incident PD patients we compared the groups who experience peritonitis with those who did not. There was no difference between groups for primary renal diagnosis (PRD), body mass index (BMI), deprivation category, age at starting RRT, age at starting PD or presence of diabetes mellitus (as PRD or co-morbid diagnosis) in terms of risk of experiencing peritonitis or in the duration of peritonitis-free survival.
At 19.4%, national culture negative rates meet the RA target of <20%. The relative proportion of causative organism has not changed over the 8 years of the audit. However, there is marked variation within and between units.
Nationally, the primary cure rate was 75%, 22.1% of cases were refractory to treatment and 2.8% resulted in death. Although individual units have managed to achieve primary cure rates >80% in specific years, this has not been sustained, and the target has not been met at a national level.
No unit met all three UK RA guidelines. Over the 8 year audit period there was significant variation in the peritonitis rate, proportion of causative organisms and outcome within and among individual units. Possible reasons for these differences may be identified by further study.