ד '' ר טניה שכטר בי '' ח איתנים. impaired attention concentration and memory...
58
ר''ר רררר רררר רר''ר רררררר
-
Upload
raymond-king -
Category
Documents
-
view
270 -
download
1
Transcript of ד '' ר טניה שכטר בי '' ח איתנים. impaired attention concentration and memory...

ד''ר טניה שכטר בי''ח איתנים

impaired attention
concentration and memory problems
slow processing of information
depressed mood
psychomotor retardation
fatigue
2

depressed moodanxietypanicphobiaobsessions and compulsionsfood craving, bulimiasleep disruption
3

1950s 1960s 1970s 1980s 1990s
Phenelzine
Isocarboxazid
Tranylcypromine
Imipramine
Clomipramine
Nortriptyline
Amitriptyline
Desipramine
Fluoxetine
Sertraline
Paroxetine
Fluvoxamine
Citalopram
Nefazodone
Mirtazapine
Venlafaxine
Duloxetine
Milnacipran
Reboxetine
Moclobemide
Escitalopram
Maprotiline
Amoxapine
Mianserin

More serotonin selective More noradrenaline selective
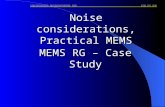
100
venlafaxine
fluoxetine
paroxetineparoxetine
sertralinesertraline
fluvoxaminefluvoxamine
amitriptyline
imipramine
maprotilinemaprotiline
nortriptyline
protriptyline
desipraminedesipramine
amoxapine
80 60 40 20 0 20 40 60 100 300 500
noradrenaline uptake Ki / serotonin Ki serotonin Ki / noradrenaline uptake Ki

ClassExamples
TCAs Clomipramine, imipramine, nortriptyline, desipramine,
amitriptyline
MAOIs Phenelzine, isocarboxazid
RIMA Moclobemide
SNRI Venlafaxine
SSRIs Escitalopram, citalopram, fluoxetine, fluvoxamine, paroxetine sertraline
Others Nefazodone, mianserin, reboxetine, tianeptine, bupropion, mirtazapine


TRICYCLIC ANTIDEPRESSANTS (TCA)- Parent Drug Imipramine Amitryptiline
Clomipramine (Primonil) (Elatrol) (anafranil) Desmethyl: Desipramine Nortryptiline derivative (Deprexan) (Nortyline)
TETRACYCLICS Mianserine Maprotiline (Bonserin) (Melodil, Lodiumil)
MONOAMINE OXIDASE INHIBITORS (MAO-I) Nonreversible: - Nonselective (MAO-A/B) e.g. phenelzine - MAO-A e.g. clorgyline - MAO-B e.g. Selegiline

SSRIs (Serotonin Selective Reuptake Inhibitors): fluoxetine 20 -40 mg (prozac, prizma, flutine,
affectine) Paroxetine 20-40 mg (seroxate Paxate) Citalopram 20-40 mg (cipramil, Recital) Escitalopram 10-20 mg (cipralex) Sertraline 50-100 mg (lusral) Fluvoxamine 100-200 mg (favoxil) SNRI’s (Serotonin\Norepinephrine Reuptake
Inhibitors): Venlafaxine 150-300 mg (Effexor, Viepax XR) Duloxetine 30-60 mg (cymbalta) Milnacipran 100-200 mg (Ixel) NRI’s (Norepinephrine Reuptake Inhibitors): Reboxetine 4-8 mg (Edronax)

Atypical Antidepressants:Mirtazapine 30 – 45 mg (Remeron, Miro) Nafazodone Trazodone 50 mg (sleep) 400+ mgs (Trazodil, Depyrel)
RIMA (Reversible Inhibitors of MonoAmine oxidase):
Moclobemide (Mobemide, Aurorix)
N\DRI (Norepinephrine Dopamine Reuptake Inhibitor):
Bupropion 300-450 mg (Zyban) Not labeled for depression
“Alternative” Remotiv St. John's Wort (Hypericum perforatum)

CHEMISTRY:
common tricyclic nucleus side chain on middle ring nitrogen:
tertiary amine > secondary amine (2 methyls) (1 methyl)
imipramine > desipramine
amitriptyline > nortriptyline

Conduction: QT^, PR^ / Alpha 1 blockade Antimuscarinic- peripheral: decreased salivation - dry mouth, decreased sweating-
hyperthermia, decreased bronchial secretions- asthma exacerbation, midriasis- photophobia, blurred vision, constipation, urinary retention, retrograde ejaculation, narrow angle glaucoma, sinus tachycardia, nausea and vomiting
- central: memory impairment, CNS anticholinergic syndrome: disorientation and delirium
Antihistaminic H1 (weight gain , sedation) Seizure threshold (1-4/1000 / overdose)Narrow therapeutic window (Target drug levels Suicidality risk) Induction of ManiaLow base rate: hepatitis, agranulocytosis

THERAPEUTIC INDICATIONS:
1. Major Depressive Disorder (MDD): Acute Treatment and prophylaxis (melancholic features, prior major depressive
episodes and a family history of MDD increase likelihood of response)
2. Panic Disorder with Agoraphobia
3. Obsessive-Compulsive Disorder (SSRI’s SNRI’s clomipramine)
4. Others: Dysthymia, Eating disorders, G AD, Chronic pain syndrome, Enuresis

MECHANISM OF ACTION:
1. MAO inhibition ir/reversible, non/selective
2. MAO-A inhibition (NA, 5-HT, DA) considered central to an antidepressant effect (e.g. clorgyline).
3. MAO-B inhibition (Phenylethylamine, DA) relevant for an antiprkinsonian effect (e.g. low dose selegiline).
(phenelzine nonselective)

4. MAO inhibition results in acutely enhanced synaptic availability of monoamines
5. serious adverse effects of MAOI
(particularly tyramine induced hypertensive crisis) are related to MAO-A inhibition.

CLASSICAL (IRREVERSIBLE) MAOIs ADVERSE EFFECTS :1. hypertensive reactions: paroxysmal headaches, hypertensive crisis, Tyramine (“cheese”) effect: headache, stiff
neck, sweating, nausea, vomiting (S.L. nifedipine)
2. autonomic reactions: dizziness, postural hypotension, dry mouth
delayed micturition, impotence

3. insomnia, behavioral activation, weight gain, edema, plasma glucose lowering
4. induction of mania in susceptible (Bipolar) patients
5. drug interactions:SSRIs -serotonin syndrome (tremor, rigidity,
myoclonus, autonomic signs >> halucinosis hyperthermia, death)TCA, stimulants, sympathomimetics

Moclobemide:
Reversible inhibition Selective for MAO AFew Drug interactions, No Dietary
Restrictions Antidepressant Efficacy?

fluoxetine, fluvoxamine Paroxetine, Citalopram, Sertraline
MECHANISM OF ACTION:
- specific inhibition of serotonin reuptake (no activity at NA or DA reuptake sites)
- Low affinity to neurotransmitter receptors

THERAPEUTIC INDICATIONS:
1. MDD acute and prophylactic treatment antidepressant efficacy equal to
conventional drugs, with less side effects and a high therapeutic window
2. OCD / Panic Disorder
3. other: Dysthymia, Borderline personality disorder, High dose (60 mg): Bulimia Nervosa (binges), Obesity (anorectic effect)

Tolerability / adherenceCNS: headache, agitation, anxiety, insomnia,
drowsiness
GIT: nausea, diarrhea, anorexia, dyspepsia,
Sexual dysfunction: decreased libido, anorgasmia, delayed ejaculation, impotence
Weight gain
Dyscontinuation Syndrome

Risk profile High therapeutic window Suicidality (FDA warning)Hyponatremia (SIADH) elderly Serotonin Syndrome Induction of maniaDrug interactions Bleeding tendency

Mechanism: Hyper stimulation of postsynaptic serotonin receptors (5-HT2A)
Serotonergic agents use \ overdose \ drug interactons
S&S:
Mental-status changes: agitation > delirium > coma
Autonomic hyperactivity: Hypertension tachycardia diaphoresis diarrhea hyperthermia midriasis
Neuromuscular abnormalities: tremor > muscular hypertonicity hyperreflexia > clonus
Complications: metabolic acidosis, rhabdomyolysis, seizures, renal failure, shock, DIC
Tx: Removal of offending drug Supportive Hyperthermia (BZD \muscular paralysis sedation and intubation) 5-HT2A blocker (cyproheptadine 12 -36 mg\ olanzepine\
chlorpromazine)

S/NRIs Mild blood pressure elevationnausea, somnolence, dry mouth, dizziness,
constipation, anorexia, asthenia, sexual dysfunction
Bupropion (Zyban) Labeled for smoking secession
Less Weight gain Sexual dysfunction seizures 0.1-0.4% increases >450 mg and
overdoseabuse potential (mild stimulant)Headaches, insomnia, dry mouth

SNRI + Postsynaptic 5-HT2ac 5-HT3 + Presynaptic Alpha2 blocker
Mianserin Weight gain Diabetes Sedation Agranulocytosis
Mirtazapine Weight gain Diabetes Sedation Agranulocytosis
Trazodone (alpha 1 and H1 blocker) Sedation postural hypotension priapism (rare)
Nefazodone Fulminate hepatic failure

Less systematic research - published or funded (variable purity potency preperations)
Strong marketing and belief by consumers that herbal supplements are 'natural', and therefore safe and effective, have resulted in increased use.
Efficacy: Mild to Moderate depression similar to antidepressants RCTs
Mechanism: S\N\D RI
Induction of CPY3A4 : cyclosporine, digoxin, warfarin, theophylline,
oral contraceptives, alprazolam, simvastatin. Serotonin Syndrome (over dose \Interaction with SSRIs) nausea, rash, fatigue, restlessness, photosensitivity, acute neuropathy, induction of mania

•Class D Paroxetine conflicting data on increased risk for VSD
•NAS Neonatal Abstinence Syndrome (NAS)
•Long Term Neurodevelopmental effects

Continuation: 6-12 months. same dose treatment to prevent relapse
Early discontinuation is associated with a 77 percent higher risk of relapse as compared with continuation treatment
Slow tapering down:
1. Minimizes discontinuation syndrome (days – 2 weeks) :
Physical: imbalance, gastrointestinal and influenza-like symptoms, sleep disturbances,
psychological: anxiety, agitation, crying spells, and irritability
2. Allows detection of early relapse
Continuation phase phase (6-12 months)
Maintenance phase (one-five years
•Residual symptoms (predict early relapse)•Severe previous episode (suicidal/hospitalization)•Recurrent episodes•Older age

- LITHIUM
- CARBAMAZEPINE
- VALPROIC ACID
- LAMOTRIGIN

MECHANISM OF ACTION: -naturally occurring alkali metal, not an endogenous
substance. No known physiological action. - possess antimanic antidepressant acute and
prophylactic effects. - acts on various nerotransmitter and second
messenger systems, as well as plasma membrane.- enhances presynaptic serotonin release. This may
explain AD augmentation in therapy resistant depression.
- inhibits inositol phosphate degradation and potentially depletes availability of inositol.
- inhibits adenylate cyclase activity by an action at Gs or the catalytic unit.

THERAPEUTIC INDICATIONS:
1. Bipolar I Disorder :- 1st line acute treatment: antimanic 80% 1-3
w. antidepressant -“- .-prophylaxis - 35% vs. 80% relapse rate on
placebo
2. Unipolar MDD non responder - 50% of AD non responders - respond to Li augmentation
3. Unipolar MDD maintenance

4. schizoaffective disorder - bipolar type- depressive type, cyclic
5. Other: intermittent aggressive outbursts,PMS, borderline personality disorder, Bulimia
nervosa

דיספוריה, חוסר ספונטניות, האטה מחשבתית הפרעות בזכרוןרעד – רעד עדין בידייםתופעות EP
תופעות נוירולוגיות טוקסיות
רעד גס, אטקסיה - ataxia, דיסארטריה -
dysarthria, התכווצויות שרירים, התכווצויות אפילפטיות, coma
33

:Thyroid- inhibition of hormone release >
hypothyroidism, goiter
Renal- reduced urine concentration (ADH antagonism), polyuria, polydypsia, nephrogenic Diabetes Insipidus
Rare: renal failure Cardiac- SAN depression (C/I in SSS), AV block ECG: T wave inversion (intracellular K displacement),
Hematologic: Leukocytosis
GIT: nausea, vomiting, decreased appetite, diarrhea

Dermatological - acne, pretibial ulceration, psoriasis, alopecia areata
Cognitive - dysphoria, lack of spontaneity, slowed reaction time, memory impairment
Teratogenic - class D. mainly cardiovacular malformations (Ebstein’s anomaly). Relative C/I during 1st trimester
Other - weight gain, edema, hyperpara, hypercalcemia
ROUTINE : (baseline and periodic)- Li blood levels, electrolytes, renal & thyroid
function tests, CBC, ECG .- effective contraception in women of
childbearing age

LITHIUM BLOOD LEVEL RANGE:indication mEq /Lacute mania 0.8 - 1.2prophylaxis 0.6 – 0.8augmentation 0.6 - 1.2
LITHIUM TOXICITY: (overdose >1.5-2)
early: coarse tremor, dysarthria, ataxia
late: impaired consciousness, fasciculations, myoclonus, seizures, coma

37
– מתן ליטיום בטרימסטר ראשוןסכנה למומים עובריים, בעיקר מומי
– נזק למסתם Ebsteinלב (תסמונת )tricuspidה-
הסכנה לנזק הטרטוגני מליטיום –באוכלוסיה , לעומת הסיכון 4-12%
2-3%הכללית – הנזק הטרטוגני מליטיום נמוך יותר
מאשר עקב מיצבי מצב רוח אחרים )carbamazepine, valproate(

CHEMISTRY:an iminodiabenzyl (tricyclic) drug, structurally
related to imipramine.MECHANISM OF ACTION:anticonvulsant effect 1. peripheral type benzodiazepine receptors
regulating Ca channels 2. alpha 2 receptor potentiation 3. stabilization of neuronal Na channels) - rapid onset, whereas antimanic effect
delayed.

THERAPEUTIC INDICATIONS:
1. temporal lobe epilepsy
2. trigeminal neuralgia
3. Bipolar I disorder (antimanic , prophylactic)
4. impulse control disorders

Aplastic-Anemia Agranulocytosis
תופעות דרמטולוגיות
HepatitisGITתופעות של
ראיה כפולה, טשטושראיה
(ורטיגו) סחרחרת הפרעות במערכת
העיכולהפרעות מוטוריות
הקשורות למינון:

ADVERSE REACTIONS:
1. hematological:- common leukopenia - rare agranulocytosis, pancytopenia, aplastic
anemia2. Hepatitis hypersensitivity - cholestatic (recurrent
on re challenge can be fatal)3. dermatological: - benign pruritic rash 10-15% (consider discontinuation or prednisone to prevent
complications)- rash rarely evolves to exfoliative dermatitis, erythema multiforme, Stevens- Johnson
syndrome, and toxic epidermal necrolysis

4. GIT: (common) nausea, vomiting, gastric distress, constipation diarrhea, anorexia
5. acute confusional state (confusion,ataxia, hyperreflexia, tremor)- most often when in combination with lithium\ psychotropics
6. CVS: decreased cardiac conduction
7. teratogenic : spina bifida, facial cranial abnormalities

43
טגרטול קשור למומי עוברCranial Facial Abnormalities אי הופעת צפורניים fingernail hypoplasia Spina Bifida אפשר להפחית את הסיכון ע"י טיפול בחומצה –
לפני ההתעברות מ"ג ביום 1-4פולית ,טגרטול נפרש בחלב אם
אך ההנקה עם טיפול בטגרטול נחשבת בטוחה

CHEMISTRY:branched chain carboxylic dipropylacetic acid
MECHANISM OF ACTION:
anticonvulant - GABAergic effect (alteration in synthesis and enhance post synaptic effect)
anti-manic - indirectly through GABA?

THERAPEUTIC INDICATIONS:
1. Epileptic conditions
2. Bipolar I antimanic, ( prophylactic -open trials)

ADVERSE REACTIONS:
1. GIT: nausea, vomiting, diarrhea2. CNS: sedation, ataxia, dysarthria, tremor3. weight gain 4. hair loss5. persistent transaminitis (resolves with
discontinuation)6. thrombocytopenia, thrombocytopathia (bleeding time
^) 7. pancreatitis (rare) 8. fatal hepatotoxicity in children ( .85: 100,000) (uncorrelated with transaminitis) 9. teratogenic: 1-2% neural tube defects

47
אסור להשתמש בתרופה זו בנשים הרות - נטילתvalproate -בזמן הריון כרוך בסיכון של נזק ל neural
tube בעובר – למשל spina bifida -1-2% בבמיוחד הסכנה גדולה בטרימסטר ראשון מ"ג 4-1ניתן להפחית את הסיכון ע"י טיפול בחומצה פולית
חדשים לפני הכניסה להריון, ובמהלך ההריון3ביום משך התרופה נפרשת בחלב ונמצא אצל היונקים כעשירית הרמה
שנמצאה אצל האם המיניקה, לרוב אין בכך נזק לתינוק

carbamazepineValproateLithium
4-12 g/mL50-100 g/mL0.6-1.2 mEq/Lרמות בפלסמה
400-1600 mg/d750-4200 mg/d600-1800 mg/dטווח מינון למבוגרים
תחילת פעילות ימים5-14 ימים5-15 ימים3-15 ש' בהתחלה25-65
ש' אחרי חודש12-17זמן מחצית חיים שעות24 שעות6-16
CYP 3A
CYP 2D6
קלוקורוניזציה, אוקסידציה
מטבוליזםאין
סילוקכליותכליותכליות, צואה
סחרחרת, טשטוש, אי יציבות
GI distress, diplopia, sedation, edema,
alopecia,, thrombocytopenia,
עליה במשקל
בחילות, הקאות, שלשול, פוליאוריה,
צמא, רעד, היפוטירואידיזם
תופ' לוואי שכיחות

49
תרופות אנטי-אפילפטיות שונות במנגנוני הפעולה, אך לכולןאינדיקציות נוספות
טיפול בהפרעה ביפולרית
טיפול במצבי כאב כרונייםהפרעות חרדההשמנהמיגרנה

50
טיפול יחיד, או בשילוב עם תרופות אחרות במצבים של הפרעה ביפולריתשלא הגיבה לטיפול אחר
bipolar I, bipolar II,הפרעה ציקלוטימית bipolar NOSהתרופה נוגדת מניה, וגם נוגדת דיכאון
-הפחתת כאב בנאורופתיה הנגרמת מHIVטיפול לכאבים לאחר ניתוחיםנאורלגיה של הטריגמינוס -לlamotrigineהשפעה אנטי-פסיכוטית
בחולי אפילפסיה -מפחיתה מחשבות חודרניות בPTSD

ערך דר' י. הרמן
51
,התופעות הנפוצות – סחרחרת,, אטקסיה, נמנום, כאבי ראש), בחילות, הקאות, פריחותdiplopiaראיה כפולה (
– בטיפול בעליה מהירה ומינונים גבוהים – פגיעות קשות בעור toxic epidermal necrolysis, Stevens-
Johnson syn
אם מופיעה פריחה – יש להפסיק טיפול

ערך דר' י. הרמן
52
Tab Lamictal 2, 5, 25, 50, 100mgTab Lamogine 5,25, 50, 100, 250mg
:דרך המתן מ"ג ביום25שבועיים ראשונים -500 (מקס' 100-200 מ"ג עד ל- 25להעלות כל שבועיים ב
ביום) בשילוב עםvalproate להפחית מינון בחצי (מקסימום –
ביום)200 בשילוב עםcarbamazepine– ניתן להכפיל מינון (עד
) ביום700

MECHANISM OF ACTION:
bilateral generalized seizure of adequate duration (>25 sec)- moderately suprathreshold (x1.5 )
seizure threshold elevation (anticonvulsant effect)
wide spread neurochemical effects:
- postsynaptic beta receptor down regulation
- 2nd messenger: G protein coupling to receptors, adenylyl cyclase, phopholipase C

THERAPEUTIC INDICATIONS:
1. MD (unipolar/bipolar) 80% response
2. manic episode
3. schizophrenia (acute affective/catatonic)
4. parkinson’s disease
5. intractable epilepsy
6. NMS

primary indications:1. need for rapid definitive response:2. c/i to pschotropic drugs (pregnancy)3. history of poor drug/ good ECT response
secondary indications: (after psychotropics)1. (adequate) treatment failure 2. adverse reactions with drug trial

no “absolute C/I to ECTrelative C/I: (substantially increased M&M)1. cerebral SOL or other condition with ICP^2. recent MI with unstable cardiac function3. recent intracerebral hemorrhage4. bleeding vascular aneurysm/ malformation5. retinal detachment6. pheochromocytoma7. anaesthetic risk rated at ASA level 4 or 5

ADVERSE EFFECTS:1. amnesia - short term anterograde, retrograde - long term: (rare) permanent memory
loss (lacunae) for certain events that occur over the months before during and after the treatment. Capacities for learning new information or remember information from past - generally not impaired.
2. post treatment confusion & disorientation
3. headache

4. infrequent: mania in susceptible (bipolar) patients, hypo/hypertension, arrhythmias, raised ICP
5. rare: CVA, ruptured cerebral aneurysm, acute MI, ruptured aortic aneurysm, spinal column fractures, adverse anesthetic effect
mortality < 1: 10,000 (less than with psychotropics)