_ 2820630119_ftp LLa infant

of 9
-
Upload
erick-mattos -
Category
Documents
-
view
219 -
download
0
Transcript of _ 2820630119_ftp LLa infant
-
8/13/2019 _ 2820630119_ftp LLa infant
1/9
Biologic and Cytogenetic Characteristics of Leukemiain Infants
BATIA STARK, MD,* RUTH VOGEL, MD, IAN J. COHEN, MD,* TEHILA UMIEL, PHD,*ZIPPORA MAMMON, MSc,t GIDEON RECHAVI, MD, PHD,* CHAIM KAPLINSKY, MD,*
DANIEL POTAZNIK, MD, AMALIA DVIR, MD,' YITZHAK YANIV, MD,YAKOV GOSHEN, MD,' NURlT KATZIR, PHD,* BRACHA RAMOT, MD,*
AND RlNA ZAIZOV. MD'
Clinical features, leukemic cell characterization, chrom osomal findings, an d treatm ent outcome were an-alyzed in a retrospective study of 30 cases with acute leukemia of infancy, 24 infants with acute lympho-blastic leukemia (ALL ), and six cases with acute nonlympho blastic leukemia (AN LL). Extensive bulkydisease with organomegaly, central nervous system CNS),and sk in involvement were prominent fe aturesat diagnosis with a higher frequency in ANLL as compared to ALL. Four of s ix AN LL pat ients wereclassified a s monocytic or myelomonocytic. In the AL L group nine of 24 (36 ) were non-L1 morphologyand six of 17 (33 ) were common ALL antigen (CAL LA) negative, th e majority of them (five of six)were included in th e non-L l group. Imm unopheno typing revealed four cases with early B-cell (threepatients: Ia+ B4+ , and one patient: Ia+ ) and two cases with T-cell. Mixe d lineage leukemia was foundin five infants. Heavy chain immunoglobulin gene rearrangement was present in six cases tested, twoCALLA+, two with Ia+B4+, and two were undifferentiated mixed lineage leukemia. Chromosomal ab-erra tion s were detected in ten of 18patients, mostly in AN LL an d CALLA negative ALL. Translocationswere detected in six patients, involving 4q21-23 and l l q 2 3 in three and two cases, respectively. Theprobability of five-year D FS was 27 for the whole group. The worst prognosis was observed in infantsyounger than 6 months of age, in whom th e leukem ia cell characteristics was compatible with stem cell:ANLL , very early pre-B, o r undifferentiated mixed type. Th e chromosom al aberrations found in all casesincluded translocation with the seemingly nonrandom breakpoints at 4q21 and 1 q23 , and breakpointstha t corresponded to known fragile sites. T his finding m ay be suggestive of a n underlying genetic predis-position associated with the poor prognosis of leukemia of infancy.
Cancer 63:117-125, 1989.CUTE LYMPHOBLASTIC and myeloid leukemias areA clinically and biologically heterogeneous diseases
for which specific therapeutic regimens should be de-signed. -4
In acute lymphoblastic leukemia (ALL) numerous fac-tors were found to have a prognostic ~ignificance,~-~among which age and initial leukocyte count are the majorinldicators of outcome and are used for stratifying patients
Presented in part at the SIOP meeting, Belgrad, Yugoslavia, 1986.From the *Sambur Center for Pediatric Hematology Oncology andthe ?Laboratory of Clinical Cytogenetics, Beilinson Medical Center, Pe-tach Tikvah, and the Hematology Department, Sheba Medical Center,Tel Hashomer, Sackler School of Medicine, Tel Aviv University, TelAviv, Israel.The authors thank Pearl Lilos of the Statistics Laboratory, Tel AvivUniversity, for the statistical evaluation of the results, and Emanuel Nir,PhD, Kaplan Hospital, Rehovot, Israel, for the election microscopy in-veirtigation.Address for reprints: Batia Stark, MD, Sambur Center for PediatricHematology Oncology, Beilinson Medical Center, Petach Tikvah, 49100Israel.Accepted for publication July 11 , 1988.
for treatment selection. In contrast to the high cure rateachieved in children with ALL,8 a much lower rate isreported in infants less than 1 year of age (60% ver-
In acute nonlymphoblastic leukemia (ANLL) as a con-sequence of the overall poor outcome, the prognostic sig-nificance of biologic parameters remains equi~ocal.~.'Nevertheless, the young age seem to fare worse than theolder children (20% versus 50% three-year continuouscomplete remission [CCR]).4
The young age adverse effect may be partially explainedby the segregation of known high-risk factors such ashigh and extensive leukemic blast burden at presenta-t i ~ n , ' - ' ~ ~orphology of myelomonocytic or monocytictype,14-16 and high incidence of negative common ALLantigen (CALLA) phenotype. 7 Some investigators attrib-uted the poor outcome to excessive toxicity and subop-timal therapy, whereas others disagree with these ob-servations. Intensive regimens introduced recentlymay lead to improved result^.^^-^^ Host factors influencing
u 20%).9-12
117
-
8/13/2019 _ 2820630119_ftp LLa infant
2/9
118 CANCERanuary 1 1989 Vol. 63the milieu of the blasts or drug metabolism cannot beruled out and require appropriate analysis with fullymatched older control patients. A retrospective study isreported, analyzing clinical and biologic characteristics ofacuted leukemia in infants in whom the malignant cloneis unique and characterized by a clone of stem cell originand nonrandom chromosomal translocations. The fea-tures may be suggestive of a special genetic event under-lying the malignant transformation, which may contributeto the poor prognosis.
Materials and MethodsPatients and Treatment
This retrospective study material comprised 30 infantsyounger than 2 years of age diagnosed with acute leuke-mia, admitted to the Sambur Center of Pediatric He-matology Oncology, Beilinson Hospital from 1966 to1986. The group represents all leukemic patients underthe age of two years treated at this center. Ten patientswere younger than 1 year of age, six of them were youngerthan 6 months of age.
During the 20 years of the study period, different ther-apy regimens were used, which can be roughly dividedinto three main treatment categories:
1 The ANLL protocol (six patients) using inductionwith cytozin arabinoside (CZ), rubidomycin (RB), 6-thioguanin (6-TG), cyclophosphamide (CTX), and vin-cristin (VCR) and monthly pulses with lower doses of CZ,RD, and 6-T6.
2. The acute leukemia protocol used from 1966 to 1969(four patients), which included induction of 6-mercap-topurine (6MP), and prednisone (P) and monthly pulseswith VCR,P, and oral therapy with 6MP and MTX withno CNS prophylaxis.3. Acute lymphoblastic leukemia (ALL) protocol dur-ing 1971- 1986(2 1 patients) using induction with VCR,P,with the addition of either CTX (two patients), or CTXand adriamycin (AD) (six patients) or CTX, AD, and CZ(18 patients). Consolidation included asparginase (ASP)(1 8 patients), occasionally with high-dose IV MTX (threepatients) and in the last two years an additional four pulseswith VCR, MTX, ASP (seven patients).24Maintenancepulses were given six monthly and then an additional sixbimonthly including VCR, CTX, AD, CZ, and P. Centralnervous system (CNS) prophylaxis comprised of IT MTX(five patients) or IT triple with MTX, CZ, P (16 patients).Cranial irradiation was given to seven infants older than9 months of age, 1500 to 2400 cGy.Morphologic and Cytochemical Studies
Wright Giemsa stain morphology of bone marrow (BM)aspiration was examined in all patients. The French-
American-British (FAB) morphologic criteria25were as-signed in 18 patients, whereas in the previous patientsclassification was limited to either lymphoid (L) or my-eloid (M) morphology. Cytohistochemical staining in-cluding periodic-acid-schiff (PAS), acid phophatase(ACPH), myeloperoxidase (MPO), Sudan black (SB),chloracetate esterase (CAE), and nonspecific esterases(NSE) were performed in 23 patients using standard tech-nique. Definition of the leukemia type for treatment as-signment was based on the morphology on light micros-copy and cytohistochemistry.
Immunologic CharacterizationImmunologic characterization was performed in 20
patients.27328 panel of monoclonal antibodies definingT-cell-restricted antigens: CD7-3A1 29 CD2-T11, CD3-0KT330; B-cell restricted antigens: CD19-B4,3 CD20-B1 32 CD21-B233; myeloid restricted antigens: CD 13-MY7,8,34CD33-My9, C D W ~ ~ - M Y ~ , ~ ~ ;nd B-cell asso-ciated antigens: HLA-DR-Ia36 and CD 10-J5 CALLA37were utilized to determine the phenotype of the leukemiacells. Cell surface antigens were analyzed by indirect im-munofluoresence or flow cytofluorometry as previouslyde~cribed.~.~~Immunoglobulin Gene Analysis
DNA was extracted from leukemic blasts, digested bythe restrictive enzyme ECO-RI and analyzed by Southernblot hybridi~a tion~~ith immunoglobulin heavy chain Jregion radioactive probe (kindly donated by Dr. P. Leder)in six patients.
KaryotypingBM aspirate cells and peripheral blood blasts were pro-
cessed both directly and after methotrexate synchronizedculture in 18 patients. Air dried preparations were storedfor a few days and routinely stained for G bands by themethod of Seabright.39 n four patients only conventionalGiemsa staining was performed.Statistical Analysis
Disease-free survival (DFS) was estimated with the useof Kaplan-Meier methods. The notable event was failureto achieve remission and relapse (death during remissionoccurred only in one patient late in the course of the dis-ease). To test the quality of survival curves we used gen-eralized savage (Mantle-Cox) test.40 Pearson chi-squarewas used to measure the association between variables.In cases of 2 X 2 tables, Fisher exact test was used.40
-
8/13/2019 _ 2820630119_ftp LLa infant
3/9
No. 1 ACUTE LEUKEMIAN INFANTS Stark et a/. 119TABLE . Clinical and Laboratory Characteristics of Leukemic Infants (1966-1977)
I* 2 3 4 5 6 7 8 9 10Age (mo)Origin/sexLiver (cm)CNSLeukocyte count (X lo9 1Morphology (FAB)PA:SNS EMF'O1st relapseCCR (mo)
21O/M5N D7LN DN DN DBM8
6O/F6N D39L2N DN DN DBMSK0.5
18O/F6N D70L2N DN DN DBM8
3A/F10N D18M4N DN DN DBM0
21A/F319LN DN DN DCN12
9A/F3148L1/2N DN DN D140t
24 19A/F AIM0 025 20LI M 3N D N DN D N DN D +BM110+ 5
4.5AIM5139M4+++BM0
15BIM6+350LN DBM11
N D not done; M: male; F female; 0: Oriental Jew; A: AshkenaziJew; B: Beduin Arab; L: lymphoid; M: myeloid; BM: bone marrow; S Kskim; CNS: central nervous system; CCR: duration of continuous com-
ResultsClinical and Laboratory Features at Diagnosis
Among the 30 evaluated leukemic patients youngerthan 2 years of age the female/male ratio was 15/15. Fe-male predominance (F/M of 7/3) occurred under the ageof 1 year, whereas male predominance (M/F of 13/7) oc-curred at the age of 1 to 2 years (Tables 1 and 2).
Ethnic origin was distributed between ashkenazi (1 5patients) and oriental Jews (12 patients) or mixed (twopatients), with only one patient of Beduin extraction, andit was similar to that observed in the older childhood leu-kemic population. Among the very young infants (youn-ger than 6 months of age) five of six patients were of as-kenazi jewish extraction.
Prenatal history included maternal medication withthyroxin, antihypertensive drugs, intramuscular iron in-jection during pregnancy, and paternal medication withanti-psychotic drugs, one of each. Three patients hadhealthy twin siblings, one had a brother with Down syn-drome, and another one had a sister with heterochromia.Physical abnormalities in the patients included one withhorseshoe kidney and one with heterochromia.
Clinical findings at presentation of hepatomegaly,spllenomegaly (>3 cm below the costal margin), and CNSinvolvement occurred in 50 , 56%, and 20% of the pa-tients, respectively. The incidence of CNS involvementw,as significantly higher than in the older population (aged2 to 17 years, 4.1%; P < 0.01). A higher frequency ofhepatosplenomegaly 1OO , and CNS involvement 50 ,although statistically not significant, was observed in theyounger subgroup (younger than 6 months). In one patient(no. 20) leukemic CNS involvement preceded by a feww'eeks BM involvement. Subcutaneous infiltrations werefound in three of six very young (younger than 6 months)patients, (nos. 2 ,2 1, and 22) and in one of 24 of the olderones (no. 3). In two infants it preceded peripheral blood
plete remission; +:alive in remission.* Patient nos.
dissemination by 12 and 3 weeks (nos. 2 and 22). Highleukocyte count >100,000 cells/mm3 was presented in20% of the patients, low hemoglobin level
-
8/13/2019 _ 2820630119_ftp LLa infant
4/9
120 CANCERanuary 1 1989 Vol. 63l a
o
m
II
::,
r
0
m
ative cases, two patients had T-cell phenotype (T11+),three patients had Ia+ B4+ CALLA-, compatible withthe earliest recognizable phenotypic stage of B-cell differ-entiation, and one patient had undifferentiated Ia+ blasts.Three patients had myelomonocytic phenotype. Mixedphenotypes, manifested by overlapping of antigenicexpression of myeloid and lymphoid antigens, were foundin five patients. In two young infants with undifferentiatedmorphology (nos. 2 1 and 24), the first one revealed a phe-notype of Ia+ My9+ My7+ and B4+ by double stainingtechnique,27328nd in the second patient with only Ia+ atpresentation, B4 antigen was acquired during relapse andMy7 antigen in in vitro culture. Two other patients withmorphologic defined ALL CALLA+ (nos. 28 and 29)coexpressed My4 antigen and additional patient withmonocytic leukemia (no. 20) coexpressed My9+ My7+My4+ and B4+ antigen.Heavy Chain Immunoglobulin Gene Analysis
This analysis showed in all six examined patients rear-ranged genes in addition to one germ line allele. It includedtwo cases with CALLA positive ALL, two with early B-cell phenotype Ia+ B4+, and the two infants with theundifferentiated mixed leukemia.Karyotype
Evaluable cytogenetic analyses were performed in 14patients (Table 3). Abnormal karyotype was identified inten cases and included all examined (six of six) infantsyounger than 7 months, the majority of the ANLL patients(five of six), and the CALLA negative ALL patients (fiveof six). Aberration could not be exactly defined in threepatients in whom only conventional Giemsa staining wasperformed. In one patient with T-cell leukemia 6q- wasfound during relapse, and in six other patients translo-cations could be identified.Response to Therapy and Complications
Complete remission (CR) was achieved in 27 of 30 pa-tients (90%). The ANLL and the younger subset faredworse than the ALL group and older subsets, attainingcomplete remission of 50% and 66% versus 100% and95%, respectively. The patients who failed to enter re-mission died five to 16 weeks from diagnosis.
Outcome of the patients is summarized in Table 4. Ofthe 27 patients who entered complete remission, 16 re-lapsed, of whom 14 died. Additionally, one patient diedduring remission from a secondary tumor. CNS relapsesoccurred in seven patients, in four of them as an isolatedevent. They included two young ANLL patients with CNSinvolvement at presentation and the other five patientswith ALL, two of whom with T ALL. No significant risk
-
8/13/2019 _ 2820630119_ftp LLa infant
5/9
No. 1 ACUTE LEUKEMIAN INFANTS Stark et al. 121factors for CNS relapse could be identified including thevarious CNS prophylaxis regimens. The estimated prob-abiility of DFS for all leukemic infants was 27% at fiveyears, with median follow-up of 36 months. The mostsignificant poor prognostic factor found by univariatean,alysiswas age (younger than 6 months) and ANLL typeof leukemia with close association between them. Oneyear DFS for the ANLL and the very young group was0741,whereas that of the ALL and the older infants was70% and 65%, respectively (P < 0.00001) (Figs. 1A andB). The very young infants comprised a unique groupwith a high incidence of known poor prognostic charac-teristics such as ANLL (four of six), non-L 1 CALLA neg-ative ALL (two of two), and chromosomal translocations(three of three). Of the older infants the two ANLL patientsand the ALL non-L1, CALLA negative patients all re-lapsed within 39 months from diagnosis, whereas the five-year DFS of ALL L1 and CALLA+ was 70% and 50%,respectively. The three patients with initial CNS involve-ment also fared poorly and died within one year of di-agnosis.
Severe late sequelae occurred in two patients (nos. 6and 7), who were diagnosed at the age of 9 and 24 months,and received cranial irradiation of 1500 and 2400 cGy,respectively, and IT MTX. Both developed meningomasfive and six years following radiation to the skull. In thefirst patient meninginoma was resected and recently re-curred. She is alive in remission for 12 years from diag-nosis with moderate brain damage. In the second patienta malignant transformation to meningosarcoma occurredand she died three years later, nine years in continuouscomplete rem i~s ion .~'
DiscussionLeukemia in early infancy has a most grave out-
n our series the five-yearDFS was 32%for ALL younger than the age of 2 years. For ANLL only50 achieved remission and this lasted no more than fivemonths. Similar results were reported in ALL and ANLLby other investigator^.^. o-' 2 13 The role of the variousparameters contributing to the poor outcome in acuteleukemia in infancy is not as yet clearly defined. The in-fants with ALL in our series and as reported by othersexhibited bulky and extensive disease at presentation,along with higher incidence of hepatosplenomegaly, CNSinvolvement, high leukocyte counts, lower platelet count,and lower Hb level^.^- In ANLL extensive disease waseven more pronounced with a high frequency of extremeleukocytosis and extramedullary involvement of skinand CNS.',14,16
lo,,k.4,9-12,i9-21,42,43 I
MorphologyThe morphology of the leukemic cell in infants differs
from that of older children. The non-L1 lymphoblasts
TABLE. Cytogenetic FindingsPatient % ABNno. Source Status cells Karyotype4914
192021'
22
23'2430
PBBMBMBMBMM XBMPBBM
BMBMBMBMBMPBBM
D I ID 100RIRI 65D 81D 100D I00D LOORI 4536
19RI 0RI 21RI 14RI 80RI 0RI 85D 75
46XX-A-6+MI+M2 t(l :21)?45XY-A+small metacentric M tr il9?46XY 6q-47XY+t( I :3)(q,,:P I4)?46XYt(ll:14)(q13-21:q24 or 32)46XXt(I I:14)(q13-21:q24 or32)46XYt(I I:17)(q23:P13)46XYt( I I:17)(q23:p13)46XY46XYt( I:17)(q23:P13)47XYtri8:t(l 1:17)46X X46XXt(4:7)(q2 :P 13) 7P+45XXt(4:7)(q2 :PI 3)- I7P+47XXtri846XXt(4:I l)(q21:q23)46XY46XYde14q23-28:19q+t(4:19)?47XY+M t r i l7?
ABN: abnormal: PB: peripheral blood; BM: bone marrow: MX: maxilla: M:marker chromosome. Status: D, diagnosis: RI, relapse.* Patients 21 and 23 were previously reported2'.**.'*.
being significantly more frequent' are either an indepen-dent variable of poor prognosis44or associated with otherpoor risk features.45The distribution of myeloid leukemiadiffers in infants as compared to older children, with ahigher prevalence of the poor prognostic subtypes, themyelomonocytic M4, and the monocytic M5.4 In the cur-rent study four of six infants exhibited M4-M5, one M3,and one undifferentiated mixed subtype.
TABLE. Outcome of Leukemic Infants Relatedto Age Group and Subtype of Leukemia0-24 mo0-24 mo 0-6 mo 7-241110A N L L + A L L A N LL ALL
(30) (6) (24) (6) (24)Slow responders*Induction failureEntered remissionDeath in remissionRelapsesBMBM I CN S
CNSTestBM/SkinLive in remissionOn treatmentOff treatment
6/27327I t73411
848
214 4/23 313 3/242 I 3 04 23 3 240 It 0 ItI 6 I 62 1 2 I0 4 0 40 1 0 11 0 0 10 8 0 80 4 0 4
Results are expressed in number of patients; number of patients in parentheses.* Slow responders were defined as those infants who did not attain completeremission by 28 days.t The patient (no. 7) died nine years from diagnosis of secondary meningios-arcoma.All patients are in first complete remission except for patient no. 27 who is insecond remission after CNS relapse.Patients are in first remission 65, 104, and 140 months from diagnosis. Onepatient (no. 16) is in second remission two years after BM and CNS relapse, followingbone marrow transplantation.
-
8/13/2019 _ 2820630119_ftp LLa infant
6/9
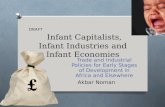
Vol. 6322 CANCERanuary 1989-Age 0 6 mo(N-6)-----Age-7-24 mo(N=24)
211
01B 28 42 ' 8 ss 112 126 140TIME (Months)
FIGS.1A A N D 1B. The estim ated probability of DFS curves estimatedby the Kaplan-Meier methods. Relapse or failure to ach ieve completeremission were includ ed in the de finition of the disease. A, top) DFSrelated to age at diagnosis. B, bottom ) DFS in infants older than 6months 7 to 2 4 months) related to subtype of leukemia and FAB mor-phology.
Immunologic PhenotypeWe and others reported a low incidence of both
CALLA+ lymphoblasts and T-cell phenotypes in infantscompared to older children.'.' '3'2-'7,46347 In four patients,early null pre-pre-By cell phenotype Ia+ B4+ CALLA-was encountered. This is the most frequent leukemic sub-type reported in in fa n~ y' *' '* '~ ,~ ~, ~ ~nd represents the ear-liest phenotypically identifiable stage of the B-cell lineage.At this early stage evidence for B-cell commitment at theDNA level is provided by the uniform presence of im-munoglobin heavy chain gene rearrangement, retainingthe germ line light chain gene,46.48-5's found in the twoinfants with Ia+ B4+ leukemia. Recent data5' demon-strated Ig heavy chain without light chain gene rearrange-ment providing further evidence for an earlier stage of B-cell lineage in ALL of infancy.
Undifferentiated leukemia is characterized by electronmicroscopy and immunophenotypically coexpressed fea-tures of mixed lymphoid myeloid origin in two babies. Inboth cases blasts could be induced to differentiate o eithermyeloid-macrophage, or to CALLA+ B-cell, dependingon the growth factors administered in vitro. Immunoglo-bin heavy chain gene was also rearranged. Undifferen-tiated leukemia is a rare subgroup of acute leukemia, with
lineage defined by blast cell characterizationSome of the undifferentiated Ia positive leukemias maycorrespond to the earliest stage of B-cellin which immunoglobulin heavy chain gene may havealready been rearranged.48349his subtype may be equiv-alent to the TdT positive acute lymphoblastic null cellleukemia, defined by Hoflbrand et al? Other subgroupsmay correspond to the early myeloid series.53Alterna-tively, those undifferentiated blasts may coexpress earlymarkers of both lineages, indicating a multi-potential stemcell origin. As reported, examples were provided by theexistence of myeloblasts positive for TdT lymphoid en-zyme or/and with rearranged DJ region of the immuno-globulin heavy chain gene and T-cell receptor alpha chaingene.56Those early markers and genetic steps are necessarybut possibly insufficient for the lymphoid lineage com-mitment, and may reflect an immortalization of a tran-sient promiscuous phase in a normal multi-potential pro-gen i t ~ r .~ ' .~~he two babies with the early undifferentiatedmixed characteristic leukemia may correspond to such astem cell origin. Mixed leukemia in an otherwise moredifferentiated blast may reflect an abberrant gene expres-sion i.e. lineage ir~fidelity).~~xamples for this alternativecould be illustrated in three of the older infants, in whomthe lymphoblastic CALLA+ leukemia expressed myeloidantigens and vice versa.56s9.60 The distribution of myeloidleukemia differs in infants as compared to older children,with a higher prevalence of the poor prognostic subtypesthe myelomonocytic M4 and the monocytic M5.4 In thecurrent study four of six infants exhibited M4-M5, oneM3, and one undifferentiated mixed subtype.Cytogenetics
Cytogenetic abnormalities were found in ten of 18 pa-tients examined, in all infants under the age of 7 months.The six translocations identified included t( 11:17), t(4:1 l) , t(4:7), and t(4: 19) in four babies and t( 1:3) and t( 11:14) in older infants. Nonrandom chromosomal aberra-tions are associated with specific types of leukemias, withcertain morphologic features and/or with certain agegroups indicating different and consistent etiologic mech-anisms. The specific chromosomal aberration has beencorrelated with the course of the disease and prog-no~is .~ ' -~ '
In a recent report structural chromosomal aberrationswere found most commonly in infants younger than 9months of age, those involving the following chromo-somes in order of frequency7*:1 lq, 9p, 16q, lop. 1 lq23band seems to be the most frequently involved in infantsleukemia and includes translocation with various chro-m o s o m e ~ . ~ ~ * ~ ~ - ~ ~he leukemias associated with thosetranslocations varies according to the recipient chromo-some revealing a wide spectrum of morphologic and im-munologic phenotypic feature^.^^,^^-^^ Translocations in-
-
8/13/2019 _ 2820630119_ftp LLa infant
7/9
ACUTELEUKEMIAN INFANTS Stark et al. 123No. 1volving chromosome 11 were found in two patients, twoweeks and five months old, t( 1 1: 17), t(4: 11). The t(4:1 l)(q2 1:q23) was described in all ages but more frequentlyin infants (mainly was reported eitherin undifferentiated, mixed, or very early B-cell acute lym-phoblastic leukemia (as in our study), or rarely was foundin CALLA+ ALL and in ANLL.78379he broad spectrumof phenotypic lineage provides evidence for a multi-potentstem cell in which the leukomogenic event involved11~123.
Chromosomal translocations involving 4q2 1 werefound in three of four babies (younger than 7 months ofage). In addition to the aforementioned pre-B-ALL witht(4:1l), the translocations found were t(4:7)(q2 1 :pl3) inmyelomonocytic leukemia and t(4: 19)(q23-28:ql3) in anundifferentiated mixed leukemia; 4q involvement was alsoreported with a wide spectrum of leukemias such as t(4:17) in unclassified leukemia with lymphoid and myeloidantigens and trisomy 4 in ANLL with multi-lineage in-volvement and in myelodysplastic syndrome.8 It istherefore suggested that 4q2 1 and 1 lq23 may be involvednorirandomly in the transformation of a multi-potentialprogenitor.
The recipient chromosomes for translocations of 4q or1 lcl were 7p, 19q, and 17q. Translocation (11:17) involv-ing 17q was found in our series in a newborn with mixedundifferentiated leukemia and was reported in adults withmyeloid leukemia of all the FAB morphologic spectrumor with myelodysplastic Chromosome 19was involved in our study in t(4:19) in an infant withUndifferentiated mixed leukemia. Aberrations involvingchromosome 19q in t( 11:19) and t(1:19) has been reportedfrequently in childhood leukemia with a wide range ofphenotype^,^^*^^-^^ mainly pre-B-ALL with t( 1: 9)67;7pwas associated with myeloproliferative disorder in one in-fant, as reported in adultss3
Iroto-oncogenes located at various breakpoints havebeen demonstrated to play a role in the evolution of themalignant transformation. Proto-oncogene Hu-ets- 1 lo-cated on band 1 lq23 has been shown to translocate, rear-range, or amplify in human hematologic malignanciesinvolving 11q23.66,76,84,85n viral leukemia E26 Ets-1 wasshown to block differentiation in transformed myelo-b l a : ~ t s . ~ ~ , ~ ~he coding gene for protein p53 mapped tochromosome 1 7 ~ 1 3 as found to be overexpressed inlyniphoproliferative disorders where it is claimed to par-ticipate in the neoplastic proliferati~n.~~onversely, inmyeloproliferative disease and ANLL including our pa-tient, p53 was not expressed.87
Genes encoding for growth factors and their receptorshave been mapped to chromosomal regions in the vicinityof ithe breakpoints mentioned above, for example, epi-dermal growth factor (EGF), T-cell growth factor (TCGF-interleukin-2) on 4q2 1,88Erb-B oncogene, the closely re-lated epidermal growth factor receptor (EGFR) on 7p13,
and the transforming growth factor beta type (T6FP) on19q13.88 Autocrine growth regulation by inappropriatequalitative and quantitative alteration of growth factorsand/or their receptors has been considered to play a pri-mary and/or permissive role in carcinogene~is.~~~~~herole of growth factors has not been explored as yet ininfant leukemia.
Neoplastic transformation, a conditioned multi-stepprocess that usually develops s10w1y,86-91-93hen occumngin a very early age may assign to an underlying geneticpredisposition or other embryonic event, the first hitof tumorigenesis. Fragile sites, hereditary or constitutive,could serve a predisposing factor of such a first hit. Theseregions are susceptible to somatic recombinations and re-side in proto-oncogenes and other active genes of cell dif-f e r e n t i a t i ~ n . ~ ~ . ~ ~n five of six infant patients chromosomaltranslocations had remarkable concordance with the lo-calization of the heritable (h-fra) and constitutive-com-mon fragile (c-fra) sites: 1 lq23, 1 lq13, 17~ 12 ,pl1, and14q24, respectively. Deletion or mutation of anti-onco-genes, defined as tumor suppressor or differentiationgene^,^^-^ could serve as another mechanism for the pre-cipitation of a neoplastic transformation in the perinatalperiod. These events are usually associated with devel-opmental malformations as observed in hereditary em-bryonal turn or^.^^-^^ Regulatory genes could reside on1 lq23, the most frequently involved band in infant leu-kemia. This band is involved in malignant proliferation,developmental aberrations, or a combination ofAmong the malignant neoplasms, it was reported in he-matopoietic and nonhematopoietic malignancies, such asEwings sarcoma or neuroepithelioma with t( 11 :22).99Developmental aberration was reported in constitutionalchromosomal rearrangement t( 1 1 22).IooBoth processescombined are illustrated in the congenital leukemia witht(4:11) and congenital In our patientwith such translocation it was associated with hetero-chromia. Other supportive evidence is provided by theexperimental setup of human cell hyrbrid (HeLa X fibro-blast) where chromosome 11 was found to have a sup-pressor influence on tumor growth.Io2 Investigation onthe molecular levels may clarify the role of each factorand their intercorrelation in the evolution of infant leu-kemia. Chromosomal aberrations were found primarilyin the very young infants. This finding is known as a poorprognostic marker. The most striking observation in thisstudy was that infants younger than 7 months of age ex-hibited the most aggressive and resistant leukemia. More-over, blast cell morphoimmunology were unique, mono-cytic, early B-cell, or undifferentiated mixed, reflecting aselection of stem cells in active proliferative hemopoiesistypical in the neonatal period. It is anticipated that furtherinvestigations may shed additional insight into the specificmechanism governing the unique drug-resistant stem cellleukemia of early infancy.
-
8/13/2019 _ 2820630119_ftp LLa infant
8/9
124 CANCERanuary 1989 Vol. 63REFERENCES
1. Chessells JM. Acute leukaemia in children. Clin Haematol 1986;2. Poplack DG cute lymphoblastic leukemia in childhood. PediatrCIin North Am 1985; 32:669-697.3. Lampkin BC, Woods W, Strauss R et al. Current status of thebiology and treatment of acute non lymphocytic leukemia in children(report from the ANLL Strategy Group of the Childrens Cancer StudyGroup). Blood 1983; 6 1:2 15-228.4. Crier HE, Weinstein HJ. Acute nonlymphocytic leukemia. PediatrClin North Am 1985; 32:653-668.5. Hammond D, Sather H, Nesbit M et al. Analysis of prognosticfactors in acute lymphoblastic leukemia. Me d Pediatr Oncol 1986; 1 46. Crist W, Boyett J, Pullen J, Van Eys J, Vietti T. Clinical an d biologicfeatures predict poor progn osis in acute lymphoid leukemias in childrenand adolescents: A Pediatric Oncology Grou p Review. Me d Pediatr Oncol7. Kalwinsky DK, Roberson P, Dahl G et al. Clinical relevance oflymphob lasts biologic features in children with a cute lympho blastic leu-kemia. J Clin Oncol 1985; 3:477-484.8. Niemeyer CM, H itchcock-Bryan S, Sallan SE. Comparative analysisof treatment. Programs for childhood acute lymphoblastic leukemia.
Semin Oncol 1985; 12:122-130.9. Sather HN. Age at diagnosis in childhood a cute lymphob lastic leu-kemia. Med Pediatr Oncol 1986; 14:166-172.10. Reaman G , Zeltzer P, Bleyer WA et al. Acute lymph oblastic leu-kemia in infants less than one year if age: A cumulative experience ofChildrens Cancer Study Grou p. J Clin Oncol 1985; 3: 15 13- 152 .11. Crist W, Pullen J, Boyett J et al. Clinical and biologic featurespredict a poor prognosis in acute lymphoid leukemias in infants: A Pe-diatric Oncology Grou p Study. Blood 1986; 67: 135-140.12. Leiper AD, Chessells JM. Acute lymphoblastic leukemia under2 years. Arch Dis Child 1986; 61:1007-1012.13. Gale RP, Foon KA. Therapy of acute myelogenous leukemia.Semin Hematol 1987; 24:40-54.14. Lampkin B, Buckley J, Nesbit M, Hammond D. Clinical andlaboratory findings and responses to therapy in infan ts less than o ne yearof age with acute non lymphocytic leukemia (ANLL) (Abstr). Proc AmSoc CIin Oncol 1984; 3:201.15. Darbyshire PJ, Smith JNF, Oakhill A, Mott MG. Monocytic leu-kemia in infancy. A review of eight children. Cancer 1985; 561584-1589.16. Van Wering ER, Kam ps W . Acute leukemia in infants. A uniquepattern of acute nonlympho cytic leukemia. A m J Pediatr Hematol Oncol17. Dinndorf PA, Reaman GH. Acute lymphoblastic leukemia ininfants: Evidence for B cell origin of disease by use of monoclonal an-tibody phenotyping. Blood 1986; 68:975-978.18. Woods WG, O Lea ry M , Nesbit ME. Life threatening neuropathyand hepatoxicity in infants during induction therapy for acute lympho-blastic leukemia. J Pediatr 198 ; 98:642-645.19. Cangir A, George S, Sullivan M. Unfavorable prognosis of acuteleukemia in infancy. Cancer 1975; 36:1973-1978.20. Steinherz P, Gaynon P, Reaman G et al. Intensive multiagentchemotherapy for infants with acute lymphoblastic leukemia (Abstr).
Proc Am SOCClin Oncol 1985; 4:157.2 1. Leverger G , Bancillon A, Schaison G, Ally N, Bo iron M. A cutelymphoblastic leukemia in very young children. Diagnostic and thera-peutic aspects of 43 cases. A m J Pediatr Hematol Oncol 1986; 8:2 13-219.22. Odom LEF, Gordon EM. Acute monoblastic leukemia in infancyand early childhood: Successful treatment with epipodop hyllotoxin.Blood23. Estrov Z, Tawa A, Wang XH et al. n vitro and in vivo effects ofdeferoxamine in neonatal acute leukemia. Blood 1987; 69:757-76 I24. Baum E, Nachman J, Sather H et al. Prolonged second remissionsin childhood acute lymphocytic leukemia. A report from the childrenscancer study group. Med Pediatr Oncol 1983; 11:1 .25. Bennett JM, Catovsky D, Daniel MT et al. Proposals for classi-fication of the ac ute leukem ias. French-American-British (FAB) Co-op-erative Group . Br J Haematol 1976; 33:45 1-458.
15:727-753.
124- 134.
1986; 14: 135-139.
1986; 8:220-224.
1984; 64:875-882.
26. Williams WJ, Beu tler E, Erslev A, Lichtm an M. Leukem ic studies.In: Hematology. New Yor k McGraw-Hill, 1983; 1646-1654.27. Umiel T, Nadler LM, Cohen IJ ef al. Undifferentiated leukemiaof infancy with t( 11 17) chromosomal rearrangement coexpressing my-eloid and B cell restricted antigens. Cancer 1987; 59:1143-1149.28. Umiel T, Nadler LM, Levine H, Cohen IJ, Stark B, Zaizov R.Acute leukemia with mixed lymphoid and myeloid phenotype. Br JHaematol 1986; 62: 196- 197.29. Haynes B. Human T lymphocyte antigens as defined by mono-clonal antibodies. Immunol Res 1981; 57:127.30. Reinherz EL, Kung PC, Goldstein G , Levey RH, Schlossman SF.Discrete stages of human intrathym ic differentiation: Analysis of normalthymocy tes and leukem ic lymphoblasts of T cell lineage.Proc Natl AcadSci USA 1980; 77:1588-1592.31. Nadler LM, Anderson KC, M arti F ef al . B4. A human B lym-phocyte-associated and malignant B lymphocytes. J Immunol 1983; 131:244-250.32. Nadler LM, Ritz J, Hardy R, Pesando LM, Schlossman SF. Aunique cell surface antigen identifying lymph oid m alignancies of B cellorigin. JClin Invest 1981; 67:134-140.33. Nadler LM, Stashenko P, Hardy R, Van Agthoven A, Terhost C,Schlossman SF. Characterization o fa hum an B cell specific antigen (B2)distinct from B1. J Immunol 1981; : 1941-1947.34. Griffin JD, Ritz J, Nadler LM, Schlossman SF. Expression ofmyeloid cell differentiation antigens on normal and malignant myeloidcells. J Clin Invest 1981; 68:932-94 I .35. Griffin JD, Linch D, Sabbath K, Larcom P, Schlossman SF. Amonoc lonal antibody reactive with normal an d leukemic hum an myeloidprogenitor cells.Leuk Res 1984; 8:25 1-94 I.36. Nadler LM, Stashenko P, Hardy R, Pesando JM, Yunis EF,Schlossman SF. Monoclonal antibodies defining serologically distinctHLAD /DR related Ia antigens in man. Hum Immunol 1981; 1:77-90.37. Ritz J, Pesando JM, Notis-McConarty J, Lazarus H, SchlossmanSF. A monoclonal antibody to h uman acute lymphoblastic leukemiaantigen. Nature 1980; 283583-585.38. Southern E. Detection of specific sequences among DNA frag-men ts separated by gel electrophoresis. J M o l Biol 1975; 98:503-5 17.39. Seabright M. A rapid banding technique for human ch romosom es.Lancet 1971; 2:971-972.40. BMD P Statistical Software Program. In: D ixon WJ, ed. Berkeley:University of California Press, 1985.4 I . Tiberin P, Maor E, Zaizov R et al. Brain sarcoma of meningealorigin after cranial irradiation in childhood acute lymphatic leukemia.J Neurosurg 1984; 61:772-776.42. Kardos G, Revese T, Koos R, Petroczky A, Schuler D. Infantleukemia in Hungary. Me d Pediatr Oncol 1982; 10:201.43. Finkelstein JZ. A cute leukemia during the first year of life. Pre-sentation, chemotherapy and clinical course. CIin Pediatr 1972; 11:236-240.44. Miller DR, Krailo M, Bleyer WA et al. Prognostic implicationsof blast cell morpholog y in childhood acute lym phoblastic leukemia: Areport from the C hildrens Cancer Study Gro up. Cancer Treat Rep 1985;69:1211-1221.45. Van Eys J, Pullen J , Head D e f al. The French-American-British(FAB) classification of leukemia. The Pediatric Oncology Group expe-rience with lymphocytic leukemia. The Pediatric Oncology Group ex-perience with lymphocytic leukemia. Cancer 1986; 57: 1046-105 1.
46. Nadler LM, Korsmeyer SJ, Anderson KC et al. B cell origin ofnon-T cell acute lym phoblastic leukem ia. A mo del for discrete stages ofneoplastic and n ormal pre-B cell differentiation. J CIin Invest 1984; 74:47. Greaves MF, Janossy G, Pet0 J. Immunologically defined subclasses of acute lymphoblastic leukemia in children: Their relationshipto presentation features and prognosis. Br J Haematol 1981; 48:179-197.48. Korsmey er SJ, Arnold A, Bakh shi A ef al. Immunoglobulin generearrangement and cell surface antigen expression in acute lymphocy ticleukemia of T cell and B cell precursor origins. J Clin Invest 1983; 71:49. Ha K , Ho zum i N, H rincu A, Gelfand EW. Lineage specific clas-sification of leukemia: Results of the analysis of sixty cases of childhoodleukemia. Br J Haematol 1985; 61:237-249.50. Greaves MF, Mizutani S, Furley AJW ez al. Differentiation-linked
332-340.
301-3 13.
-
8/13/2019 _ 2820630119_ftp LLa infant
9/9
ACUTELEUKEMIAN INFANTS Stark et al. 125No. 1gene rearrangement and expression in acute lymphoblastic leukemia.Clin Haematol 1986; 15:621-639.
5 1 Foon KA, Gale RP, Todd RF. Recent advances in the immu-nologic classification of leukemia. Semin Hematol 1986; 23:257-283.52. Felix CA, Reaman GH, Korsmeyer SJ et al. Immunoglobulinand T cell receptor gene configuration in acu te lymphoblastic leukemiaof infancy. Blood 1987; 70:536-541.53. Kita K, Nasu K, Kamesaki H et al. Phenotypic analysis of acutelymphob lastic leukemia (AL L) cells which are classified as non-T non-B and negative for commo n ALL antigen. Blood 1985; 66:47-52.54. Raghavachar A, Bartram CR, Ganser A, Heil G, Kleihauer E,Kubanek B. Acute undifferentiated leukemia: Implications for cellularorigin and clonality suggested by analysis of surface markers and im-munoglobulin gene rearrangement. Blood 1986; 68:658-662.55. Ho firan d AV, Drexler HG, Goneshaguru K , Piga A, Wickre-mardnghe RG. Biochemical aspects of acute leukemia. Clin Haematol56. Stass SA, Mirro J. Lineage heterogeneity in acu te leukaem ia: Acutemixed-lineage leukaemia and lineage switch. Clin Haematol 1986; 15:57. Greaves MF, Chan LC, Furley AJW, Watt SM, Molgaard HN.Lineage romiscuity in hemop oietic differentiation and leukemia. Blood58. McCulloch EA. Stem cells in norm al an d leukemic hem opoiesis.(Henry Stratton lecture, 1982). Blood 1983; 62 : 1-13.59. Mirro J, Zipf TF, Pui CH et al. Acute mixed lineage leukemia:Cliriicopathologic correlations an d prognostic significance. Blood 1985;60. Sobol RE, Mick R, Royston I et al. Clinical importance of myeloidantigen expression in adult acu te lymphob lastic leukemia. NEngl JMed6 I . Sallan SE, Ritz J, Pesand o J et al. Cell surface antigens: Prognosticimplications in childhood acute lymphoblastic leukemia. Blood 1980;62. First M IC Cooperative Study Group. Morphologic, immu nologic,and cytogenetic (MIC) working classificationof acute lymphob lastic leu-kemias. Cancer Genet Cytogenet 1986; 23: 189- 197.63. Look AT, Melvin SL, Williams DL t al. Aneuploidy and per-centage of S-phase cells determined by flow cytometry correlate with cellphenotype in childhood acute leukemia. Blood 1982; 60:959-967.64. Rowley JD, Alimena G , Garson OM , Hagemeijer A, M itelmanF, Irigogina EL. A collaborative study of the relationship of the mor-phcllogical type of acute non lymphocy tic leukemia with patient age andkaryotype. Blood 1982; 59:1013-1022.65. Kaneko Y, Rowley JD, M aurer HS, Variakojis D, Moohr JW.Chromosome pattern in childhood acute nonlymphocytic leukemia66. Yunis JJ, Brunn ing RD. Prognostic significance of chromoso malabnormalities in acute leukaemias and m yelodysplastic syndrom es. CIinHamnatol 1986; 15:597-620.67. Williams DL, Look AT, Melvin SL et al. New chromocomaltrarislocations correlate with specific immunophenotypes of childhoodacute lympho blastic leukemia. Cell 1984; 36:lOl-109.68. Williams PL, Harber J, Murphy SB et al. Chromosomal trans-locations play a unique role in influencing prognosis in childhood acutelymphoblastic leukemia. Blood 1986; 68:205-2 12.69. Sandberg AA. The chromosomes in human leukemia. Semin He-
ma. ol 1986; 23:201-217.70. Bloomfield CD, Goldman AT, Alimena G et al Chromosomalabn.ormalities identify high-risk an d low-risk patients with ac ute lym-phoblastic leukemia. Blood 1986; 67:415-420.7 1. Woods WG, Nesbit ME, Buckley J et al. Correlation of chro-mosome abnormalities with patient characteristics, histologic subtypeandl induction success in children with ac ute non lymphocy tic leukemia.J Clin Oncol 1985; 3:3-12.72. Pui CH, Raimondi SC, Murphy SB et al. An analysis ofleukemiccell chromosomal features in infants. Blood 1987; 69: 1289-1293.53. Kaneko Y, Maseki N, Takasaki N et al. Clinical and hematologiccharacteristics in acute leuk emia w ith 1lq23 translocations. Blood 1986;74. Abe R, Ryan D, Gecalupo A, Cohen H, Sandberg AA. Cytogeneticfindings n congen ital leukemia: Case report an d review of the literature.Cancer Genet Cytogenet 1983; 9:139-144.
1986; 15:669-694.
81 1-827.
1986; 67~1-11 .
66: I 1 15-1 123.
1987; 316:1111-1117.
551395-402.
(APJLL). Blood 1982; 601389-399.
67:484-49 1.
75. Abe R, Sandberg AA. Significance of abnormalities involvingchromosomal segment 11q22-25 in acute leukemia. Cancer Genet C y-togenet 1984; 13:12 1- 127.76. Katz FE, Malcolm S, Gibbons B et al. Cellular and molecularstudies on infant null ALL (Abstr). Blood 1986; 67:258.77. DeBraekeleer M. t (4 1 1) translocation-associated acute leukemia:An update. Cancer Genet Cytogenet 1986; 23:333-335.78. Stark B, Umiel T, Mammon Z et al. Leukemia of early infancy.Early B-cell lineage associated with t 4 : l l ) . Cancer 1986; 58:1265-1271.79. Mirro J, Kitchingma n G, Williams D e t a / .Clinical and laboratorycharacteristics of acute leukemia with 4: I 1 translocation. Blood 1986;80. Ganser A, Heil G, Bohm T et a/. Human acute unclassified leu-kemia with a unique 4: 17) chromoso mal translocation expresses T lym-phoid and myeloid surface antigens after in vitro culture. Blood 1987;81. Mecucci C, Van Orshoven A, Tricot G, Michaux JL, DelannoyA, Van-Den-Berghe H. Trisomy 4 identifies a subset of acute n on lym-phocytic leukemia. Blood 1986; 67: 1328-1332.82. Borgstrom G. Abnormalities of chromosome 17. Cancer GenetCytogenet 1984; 11:314-315.83. Scheres J, Hustink T, Geraedts J, Keeksma HW, Meltzer PS.Translocation 1:7 in hematologic disorders: A brief review of 22 cases.Cancer Genet Cytogenet 1985; 18:207-213.84. Sacchi N, Watson D K, Gu erts Van Kessel AHM t al. Hue-ete-1 and Hu-ets-2 genes are transposed in acute leukemias with 4:l I ) and8:21) translocations. Science 1986; 231:379-382.85. Rovigatti U Watson DK , Y unis JJ. Am plification and rearrange-men t of Hu-ets-I in leukem ia and lym phoma with involvement of 1 lq23.Science 1986; 232:398-400.86. Bishop JM. The molecular genetics of cancer. Science 1987; 235:87. Prokocimer M, Shaklai M, Ben Bassat H, Wolf D, Goldfinger N,Rotter V. Ex pression of p53 in human leukemia and lymphoma. Blood88. McKusick VA. The morbid anatomy of the human genome: Areview of gene m apping in clinical medicine. Medicine 1986; 65: 1-33.89. Growth factors and malignancy. Lancet 1986; 2:3 17-318.90. Goustin A, Leof EB, Shipley GD , Moses HL. Growth factors andcancer. Cancer Res 1986; 46:1015-1029.9 1. Greaves MF, Chan LIC. Is spontaneous mutation the major causeof childhood acute lymphoblastic leukemia? Br J Haematol 1986; 64:92. Klein G, Klein E. Conditioned tumorigenicity of activated on-cogenes. Cancer Res 1986; 46:3211-3224.93. Croce CM. Chromosom e translocations and hum an cancer. Can-cer Res 1986; 46:6019-6023.94. Yunis JJ. Chromosomal rearrangements, genes and fragile sitesin cancer: Clinical and biologic implications. In: DeVita VT, HellmanS, Rosenberg SA, eds. Important Advances in Oncology. Philadelphia:J. B. Lippincott, 1986; 93-128.95. LeBeau MM . Chromoso mal fragile sites and c ancer-specific ear-rangements. Blood 1986; 67:849-858.96. Knudso n AG . Hereditary cancer, oncogenes, and anti-oncogenes.Cancer Res 1985; 45:1437-1443.97. Sagar R. Genetic suppression of tumo r formation: A new frontierin cancer research. Cancer Res 1986; 46:1573-1580.98. Marx JL . Th e yin an d yang of cell growth control. Science 1986;99. Turc-Carel C, Philip I, Berger MP, Philip T, Lenoir GM. Chro-mosom e study o f Ewings sarcoma (ES) cell lines. Consistency of re ci procal translocation t( 11:22) q24:q12). Cancer Genet Cytogenet 1984; 12:1-19.100. Iselius L, Lindsten J , Aurias A et al. The 1 lq:22q translocation:A collaborative study of 20 new cases and analysis of 1 10families. HumGenet 1983; 64:343-355.101. Morrow RC, D ickerman JD, Clem mons JJ. Infantile lympho-blastic leukemia with t( 4 11 and septate uterus, double cervix, and doublevagina: Case report a nd review of the literature.Med P ediatr Oncoll985;102. Srivansan ES, Benedict WF, Stanbridge EF. Implication ofchro-mosome 1 I in the suppression of neoplastic expression in human cellhybrids. Cancer Res 1986; 46:6174-6179.
67:689-697.
69:271-277.
305-3 1
1986; 68:113-118.
1-13.
232: 1093-1096.
13~366-369.