





Languages
Pages
Legal

When Is A Colonoscopy Not a Colonoscopy
Dr Linus ChangGastroenterologist
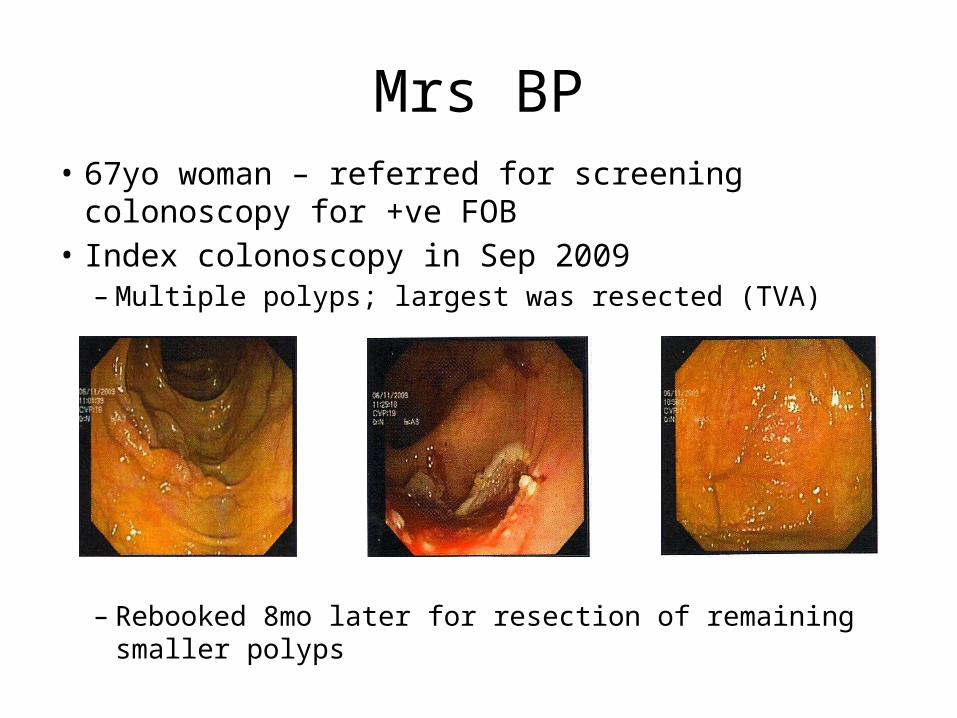
Mrs BP• 67yo woman – referred for screening colonoscopy for
+ve FOB• Index colonoscopy in Sep 2009– Multiple polyps; largest was resected (TVA)
– Rebooked 8mo later for resection of remaining smaller polyps
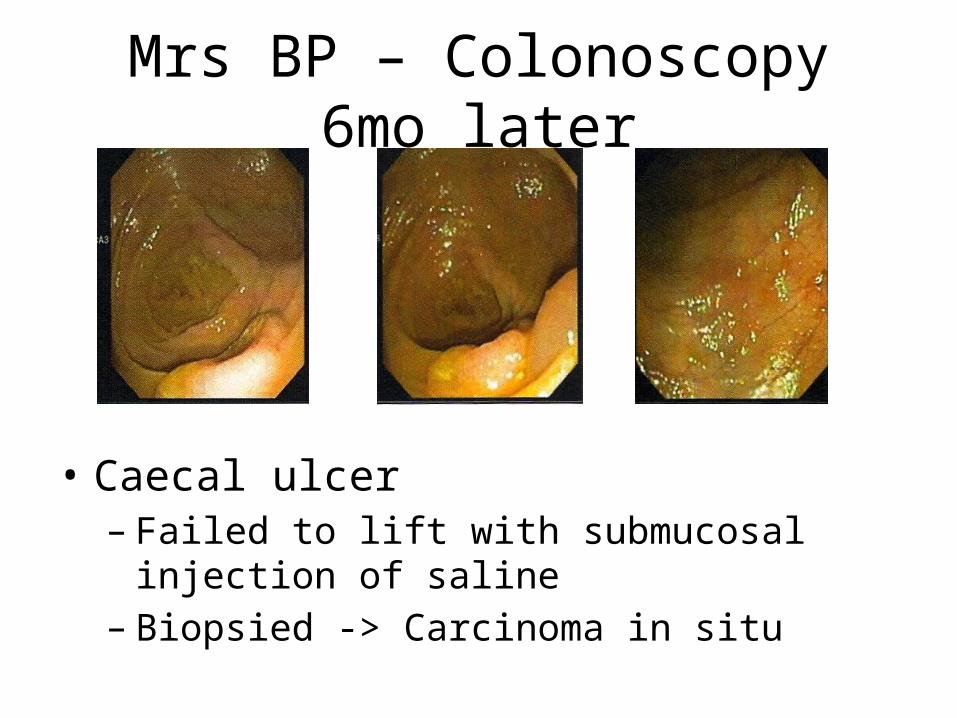
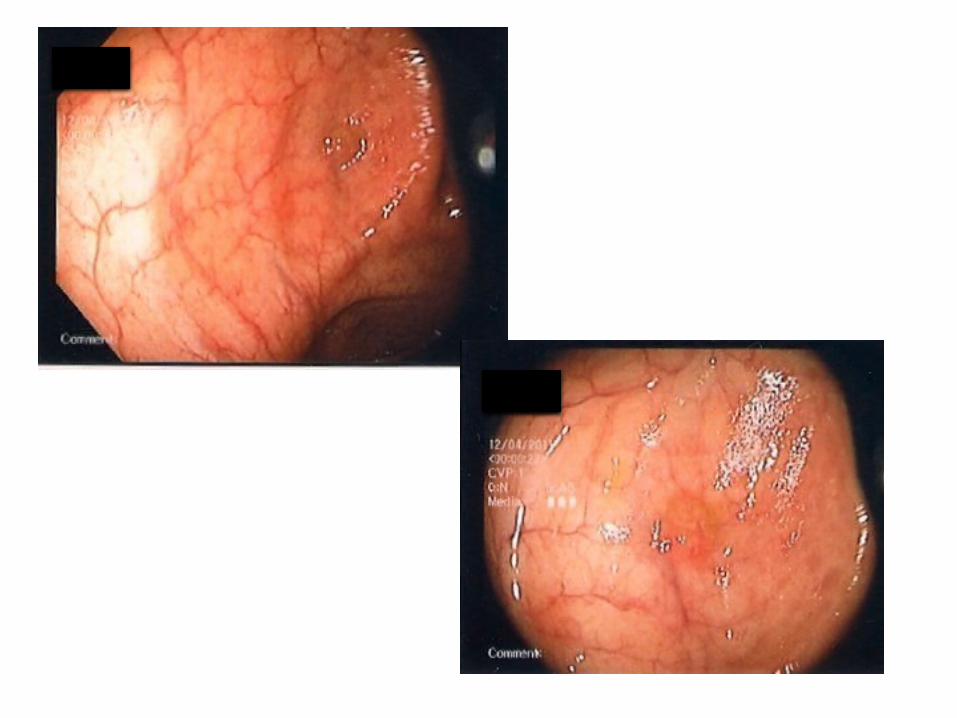
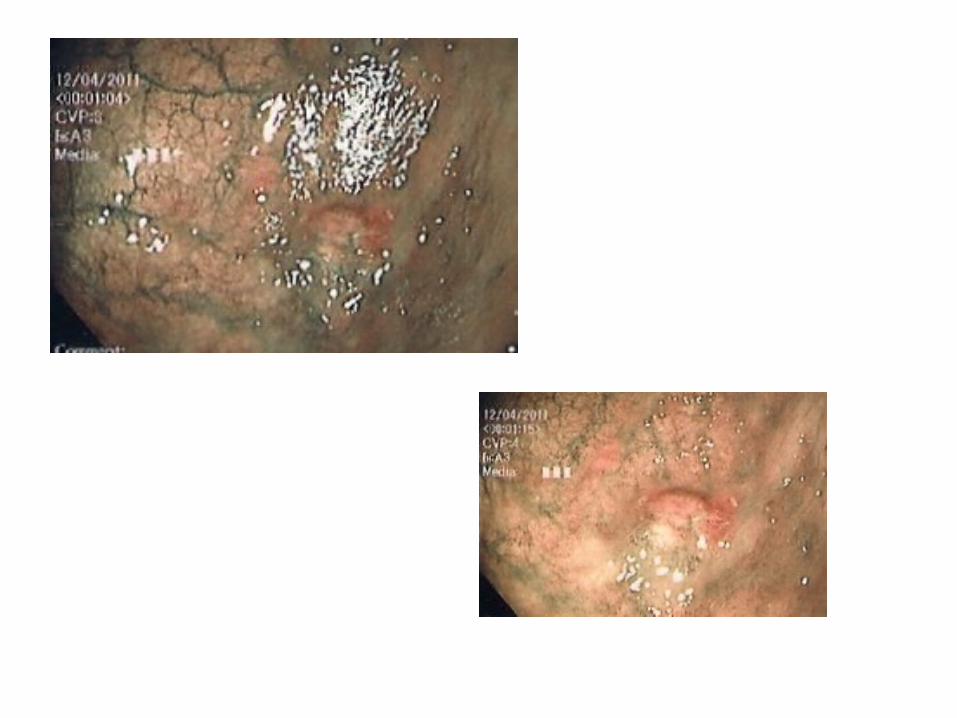
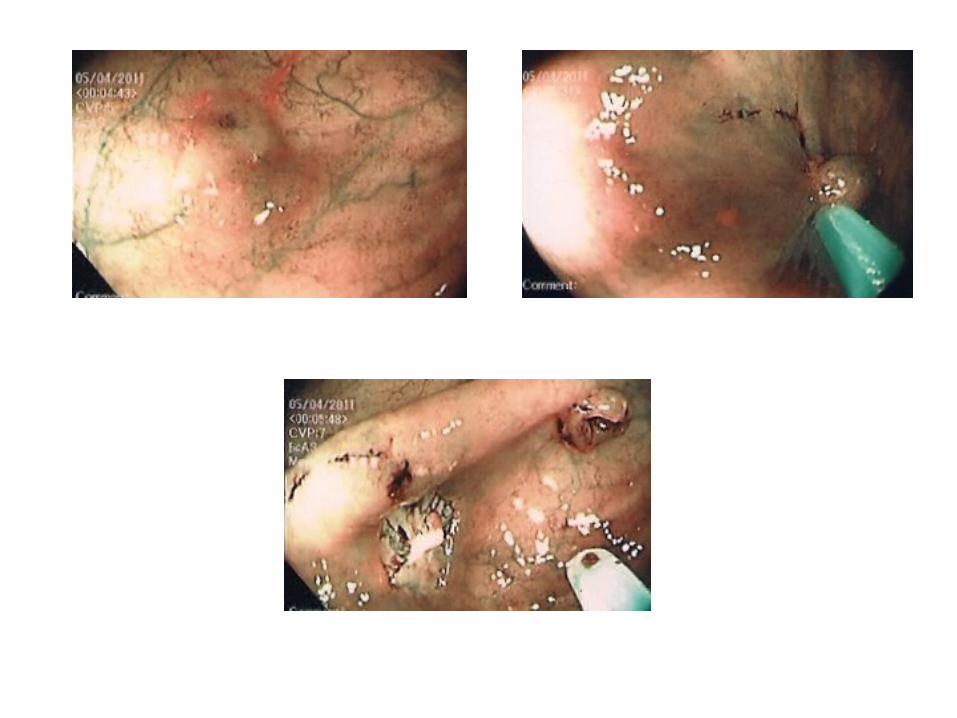
Mrs BP – Colonoscopy 6mo later
• Caecal ulcer– Failed to lift with submucosal injection of saline– Biopsied -> Carcinoma in situ
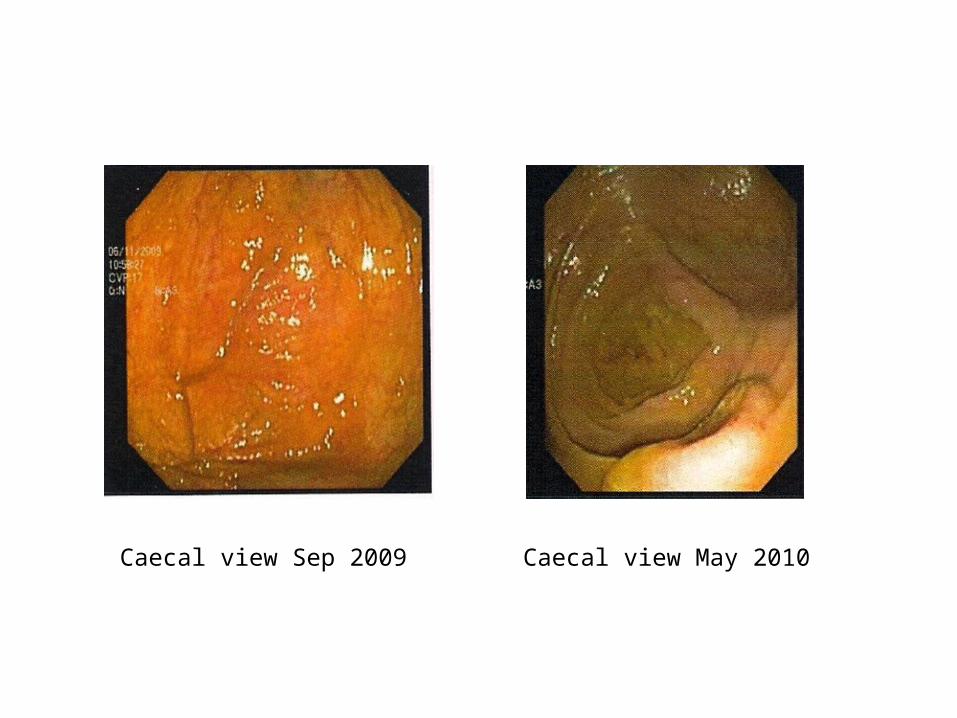
Caecal view Sep 2009 Caecal view May 2010
Mrs BP - Surgery
• Proceeded to R hemicolectomy– Early T2 CRC -> just infiltrating muscularis propria– Loss of nuclear staining seen for MLH1 and PMS2
(consistent with microsatellite instability)– 0/10 lymph nodes involved– No adjuvant chemo recommended
• Tumour was surrounded by flat lesions which were sessile serrated adenomas (SSA)
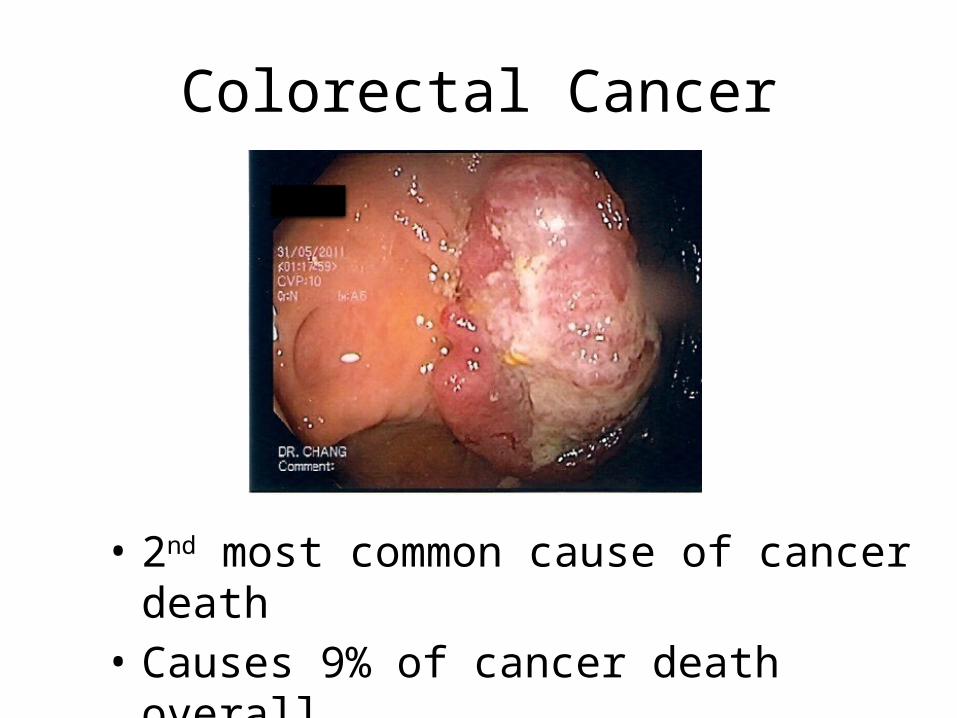
Colorectal Cancer
• 2nd most common cause of cancer death• Causes 9% of cancer death overall
Colonoscopy in screening for CRC
• Screening colonoscopy in 1994 asymptomatic adults– 5.7% had advanced neoplasms
Lieberman DA, et al N Engl J Med. 2000;343(3):162
• Asymptomatic individuals (mean age 61) colonoscoped then followed for 8 years have reduced CRC incidence and death compared to expected incidence and SEERS data
Kahi CJ, et al. Clin Gas Hepat. 2009;7(7):770
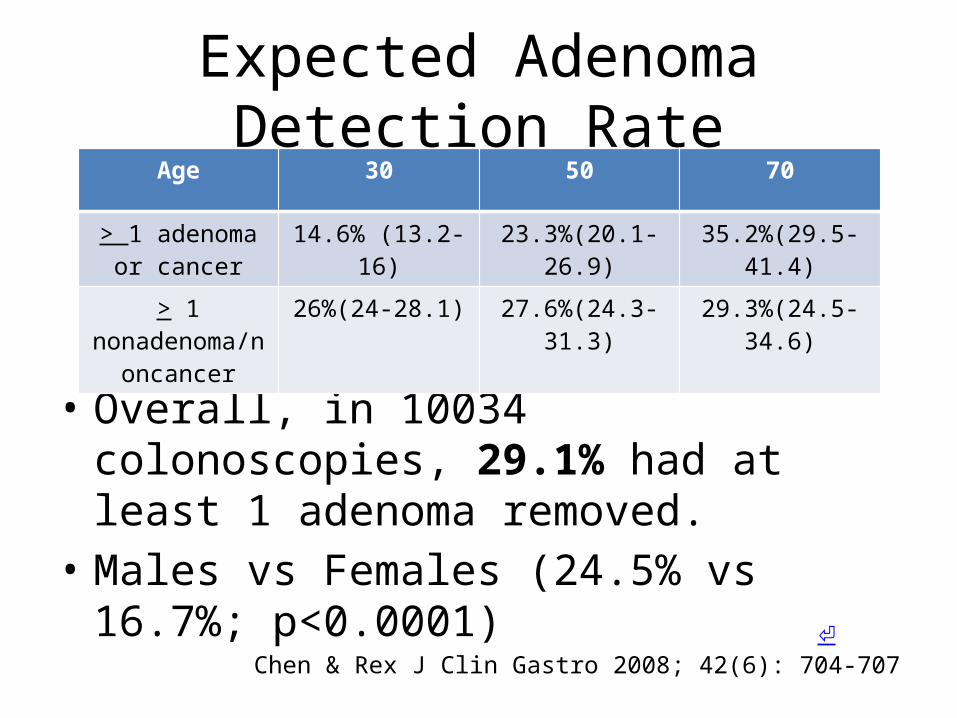
Expected Adenoma Detection Rate
• Overall, in 10034 colonoscopies, 29.1% had at least 1 adenoma removed.
• Males vs Females (24.5% vs 16.7%; p<0.0001)Chen & Rex J Clin Gastro 2008; 42(6): 704-707
Age 30 50 70
> 1 adenoma or cancer
14.6% (13.2-16) 23.3%(20.1-26.9) 35.2%(29.5-41.4)
> 1 nonadenoma/non
cancer
26%(24-28.1) 27.6%(24.3-31.3) 29.3%(24.5-34.6)
⏎
Risks of Colonoscopy
• 1 in 1000 of perforation or major bleeding• 0.8/1000 if no biopsy• 7/1000 if polypectomy or biopsy
Polyp detection depends on endoscopist
• Risk of interval cancer between screening colonoscopy and repeat procedure depends on endoscopist’s adenoma detection rate
• Withdrawal time of 6 minutes or more increases adenoma detection rate
Barclay RL, et al. N Engl J Med. 2006;355(24):2533
Less effective in R sided lesions?
• Colonoscopy reduces deaths mainly from L sided CRC, but not R sided lesions:
Baxter NN, Ann Intern Med. 2009;150(1):1.Singh H, Gastroenterology. 2010;139(4):1128
• 5% of CRCs arise as “interval” cancers following a colonoscopy
Sessile Serrated Adenomas
• Distal polyps usually follow conventional adenoma-carcinoma sequence
• Up to 20% of all CRCs may arise from serrated polyps
• Only recognised as recently as 2003• Serrated pathway polyps become cancers with
high levels of microsatellite instability (MSI)• Can become cancers more rapidly than
conventional adenomas
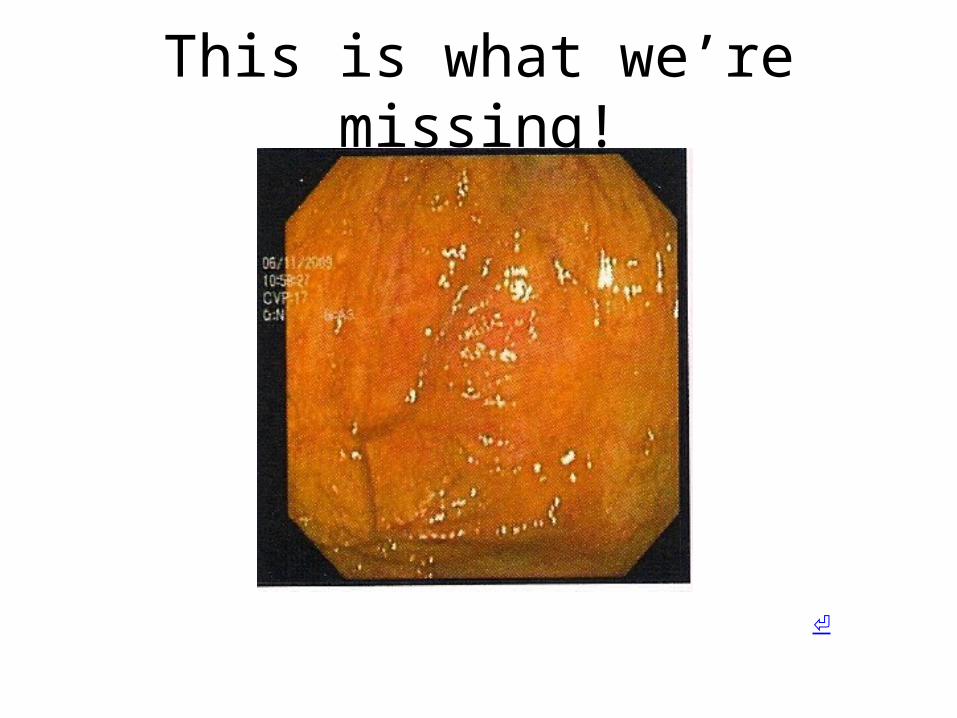
This is what we’re missing!
⏎
Sessile Serrated Adenomas (2)
• SSAs represent 1-9% of all polyps• Present in 1-4% of the general population• Median age of patients 61• Trend toward female gender bias• More commonly in the proximal colon• Endoscopic appearance:
– 5mm or larger– Flat or depressed– Covered by adherent layer of yellowish mucus
• In patients with at least one SSA– 12% have LGD; 2% have HGD; 1% have adenocarcinoma
Huang CS, et al. Am J Gastro 2011; 106: 229-240⏎
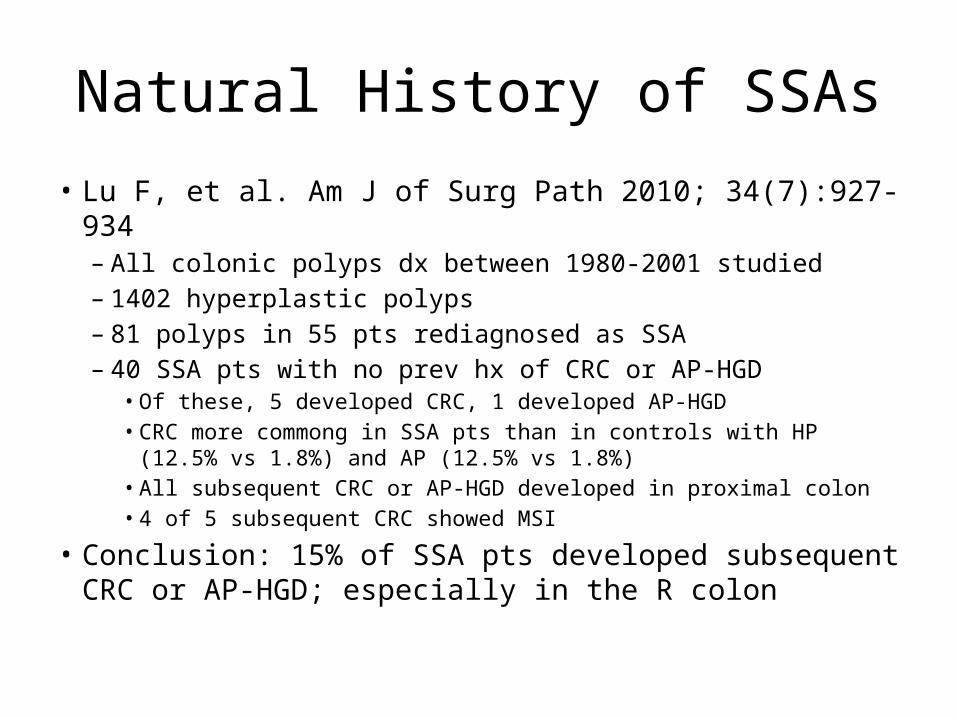
Natural History of SSAs
• Lu F, et al. Am J of Surg Path 2010; 34(7):927-934– All colonic polyps dx between 1980-2001 studied– 1402 hyperplastic polyps– 81 polyps in 55 pts rediagnosed as SSA– 40 SSA pts with no prev hx of CRC or AP-HGD
• Of these, 5 developed CRC, 1 developed AP-HGD• CRC more commong in SSA pts than in controls with HP (12.5% vs
1.8%) and AP (12.5% vs 1.8%)• All subsequent CRC or AP-HGD developed in proximal colon• 4 of 5 subsequent CRC showed MSI
• Conclusion: 15% of SSA pts developed subsequent CRC or AP-HGD; especially in the R colon
Risk factors for developing SSAs
• Cigarette smoking• Obesity• Female gender• Family history of CRC or polyps
How quickly to SSAs progress to cancer
• We don’t know• Case study suggesting SSA-> CA in 8 months• Mrs BP
Surveillance post-resection
• SSA with no dysplasia– 5 years if <3 lesions, all <1cm in size– 3 years if 3 or more, or any 1cm or more in size
• SSA with dysplasia– 3 years
• Screening of first-degree relatives at age 40, or 10y prior to age of diagnosis
We are missing SSAs!
• Mortality rates from R sided CRC not decreasing despite increasing use of screening colonoscopy
• Interval cancers more likely to occur in proximal colon and demonstrate microsatellite instability suggesting they arise from SSAs
• Adherent mucus coating is not a useful endoscopic sign unless prep is very good
Recognising SSAs
• Colonoscopy is the only reliable technique• Increasing recognition of SSA • 6 min withdrawal time• Split dose bowel preparation• Advanced imaging techniques– Narrow Band Imaging– Indigo Carmine spray
Split dose Colonic Preparation
• Traditional colonic preparation consists of solution given day prior to colonoscopy
• Split dose prep involves giving for example, 2L of prep the day prior, and 1L on the morning of colonoscopy
Clear superiority of Split Dose Prep
• Achieves better cleansing than conventional– Good/excellent views 75% vs 43% (p=.00001)– Best views within 8 hours of last fluid intake
• Adenoma detection rates higher– 24% vs 12%, (p=0.001)
• Lower rates of failed caecal intubation– 1% vs 11%; (p=0.00001)
• Fewer aborted procedures– 7% vs 21%, (p<0.0001)
Marmo R, et al. Gastrintest Endosc. 2010 Aug; 72(2):313-20.
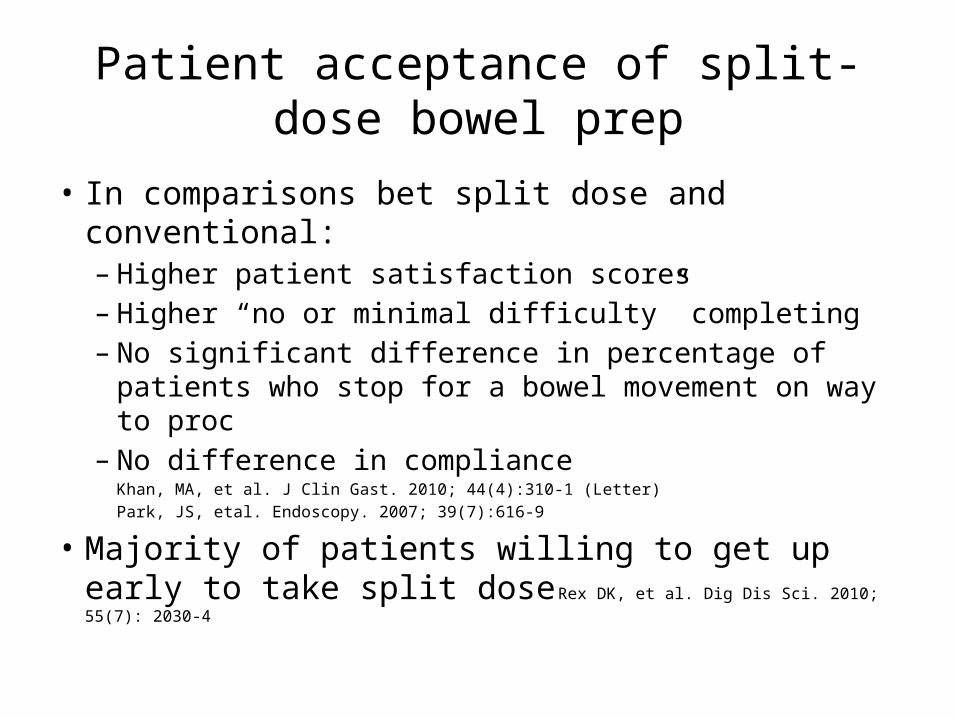
Patient acceptance of split-dose bowel prep
• In comparisons bet split dose and conventional:– Higher patient satisfaction scores– Higher “no or minimal difficulty” completing– No significant difference in percentage of patients who
stop for a bowel movement on way to proc– No difference in compliance
Khan, MA, et al. J Clin Gast. 2010; 44(4):310-1 (Letter)
Park, JS, etal. Endoscopy. 2007; 39(7):616-9
• Majority of patients willing to get up early to take split dose Rex DK, et al. Dig Dis Sci. 2010; 55(7): 2030-4
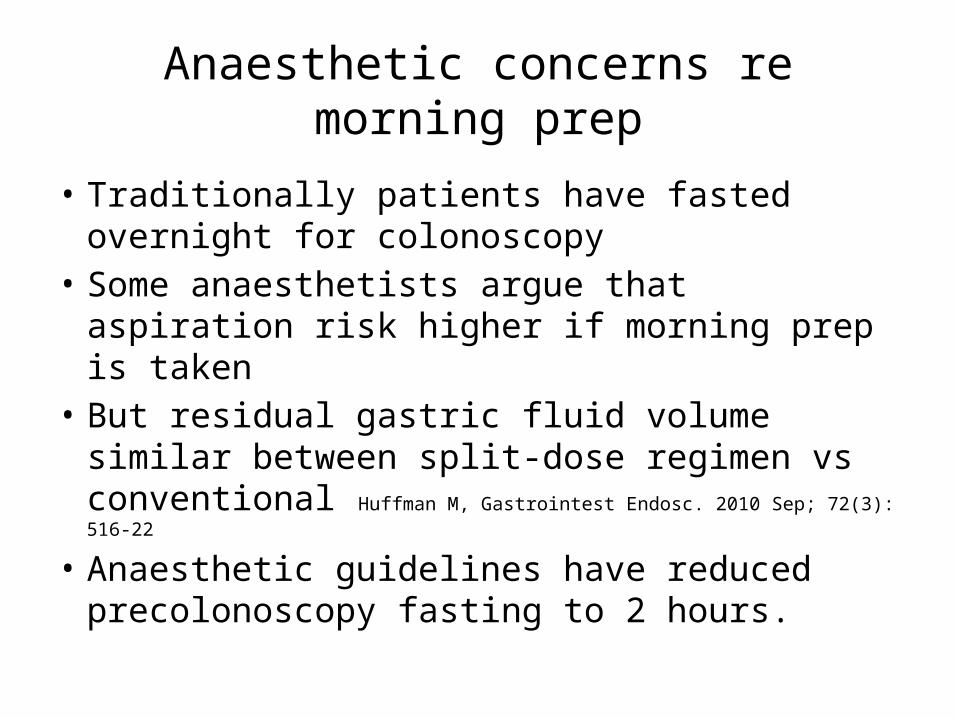
Anaesthetic concerns re morning prep
• Traditionally patients have fasted overnight for colonoscopy
• Some anaesthetists argue that aspiration risk higher if morning prep is taken
• But residual gastric fluid volume similar between split-dose regimen vs conventional
Huffman M, Gastrointest Endosc. 2010 Sep; 72(3): 516-22
• Anaesthetic guidelines have reduced precolonoscopy fasting to 2 hours.
Image Enhanced Colonoscopy
• Includes:– Endoscope based image enhancing:• NBI (Olympus)• iScan(Pentax)
– Chromoendoscopy• Indigo carmine dye
NBI/FICE/iScan
• iScan (Pentax) increases detection of neoplasia over white light (38% vs 13%)
• FICE (Fuji) showed no difference in adenoma detection over white light
• NBI (Olympus) increases detection of flat adenomas over white light, but not adenomas overall.
• FICE (Pentax) vs Indigocarmine – no difference in adenoma detection rates
Hoffman A. et al. Endoscopy. 2010 42(10):827-33Chung SJ, et al. Gastrointestinal Endoscopy. 2010; 72(1):136-42
Paggi S, et al. Clin Gas & Hep. 2009; 7(10) 1049-54Pohl J, et al. Gut. 2009; 58(1):73-8
Chromoendoscopy
• Spraying of indigo carmine through the flushing channel of the colonoscope
• Increases detection of flat lesions and hyperplastic polyps, but not of adenomas overall. Le Rhun M, et al. Clin Gas & Hep. 2006; 4(3):349-54
What makes a colonoscopy a (good) colonoscopy?
• SPLIT DOSE COLONIC PREP• At least 6 minutes withdrawal• +/- image enhancing in the R colon (NBI or
indigo carmine)• Endoscopist consciously looking for flat R
sided lesions
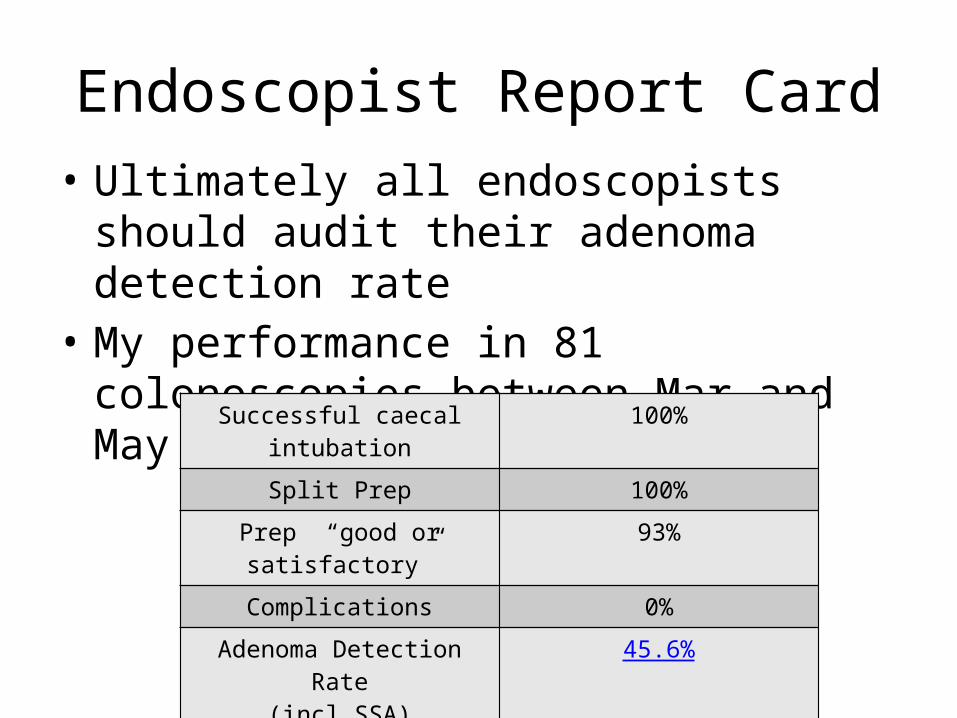
Endoscopist Report Card• Ultimately all endoscopists should audit their
adenoma detection rate• My performance in 81 colonoscopies between
Mar and May 2013 at 1 facility:Successful caecal intubation 100%
Split Prep 100%
Prep “good or satisfactory” 93%
Complications 0%
Adenoma Detection Rate(incl SSA)
45.6%
SSA percentage of all polyps 18.9%
SSA detection rate 8.7%
Top Related