







Languages
Pages
Legal

Horizontal Violence or Generational Conflict: Is Care-Fronting the Answer
Yvonne Wesley, RN, Ph.D., FAANIndependent Health Consultant
www.ywesleyconsulting.com
Overview
Upon completion of this session, participants will be able to:
Define Horizontal Violence and Generational Conflict
Compare and contrast HV and GC similarities and differences
Illustrate the effect of Care-Fronting on HV and GC
Horizontal Violence
Antagonistic behaviors such as:
Gossiping, undue criticism,
Innuendo, scapegoating,
Undermining, passive aggression,
Bickering , blaming behaviors
Sabotage
Emotional dumping, indiscriminate venting
Weinand, M. R. (2010). Horizontal violence in
nursing: history, impact, and solution. JOCEPS: The
Journal Of Chi Eta Phi Sorority, 54(1), 23-26.
Weinand, M. R. (2010)
Why susceptibility among nurses• Antagonistic behaviors among oppressed people i.e.:
women• Nursing predominately women• Antagonistic behaviors, a form of self-hate• Demonstrated in the classroom with faculty
dominating student nurses.• Nurse managers and supervisors cited as frequent
users of bullying culture & top down style
Weinand, M. R. (2010)
End Product from HV• Overwhelming sense of negativity cultivated• Aggression breeds aggression• Low morale• High turnover• Increased absence• Low productivity
Weinand, M. R. (2010)
Solutions to the problemEmbrace transformational leadership
Inspire and challenge staff;
Utilize active listening,
Advise and coach staff;
Have a positive vision
Reward resolution vs. identification of problems
Formal training in teamwork, positive feedback, conflict
management and confrontation
skills
King-Jones, M. (2011)
•overt and covert nonphysical hostility,
•criticism, sabotaging, undermining, infighting, scapegoat, and bickering
•unkindness, discourtesy, divisiveness, and lack of cohesiveness
•belittling gestures, verbal abuse, gossiping, sarcastic comments, faultfinding, devaluing comments,
•disinterest and discouragement, and controlling behaviors
King-Jones, M. (2011).
Horizontal Violence and
the Socialization
of New Nurses. Creative
Nursing, 17(2), 80-86.
King-Jones, M. (2011)
HV stems from oppression
HV is how oppressed people cope with powerlessness
HV, a display of powerlessness & negative emotions
Knowledge is power -- a cycle of power and resistance
To resolve HV, address the dynamics of power and conflict
Generational Conflict
•Increased numbers of generations working together creates more opportunity for misunderstanding•Veterans, [born
before 1945]•Baby Boomers,
[born 1946-1964]•Generation X,
[1965-1976]•Gen Y/Millennials
[1977-1997]
Hahn, J.A. (2011), Managing Multiple
Generations: Scenarios From the Workplace. Nursing Forum, 46(3), 119-127.
Hahn, J.A. (2011)
Veterans – before 1945
Grew up in times of political and economic uncertainty,
lived experience of the Great Depression and World War II
Nursing as a helping profession and unselfish
Expect rewards for hard work
Baby Boomers – ‘46 to ‘64
Strong sense of duty, called workaholics
Lived experience of prosperity
Look to empower
Arrive early to work
Hahn, J.A. (2011)
Generation X – ’65 to ‘76
Independent, self-directed, and techno-savvy
Latchkey kids
Grew-up quicker and stayed adolescents longer
Quality of life important their parents work long hours and experienced downsizing
Millennium/Gen Y – ’77 to ‘97
Technology and instant communication
Accepting multiculturalism
After-school activities, such as swimming, soccer, dance
Want work-life balance
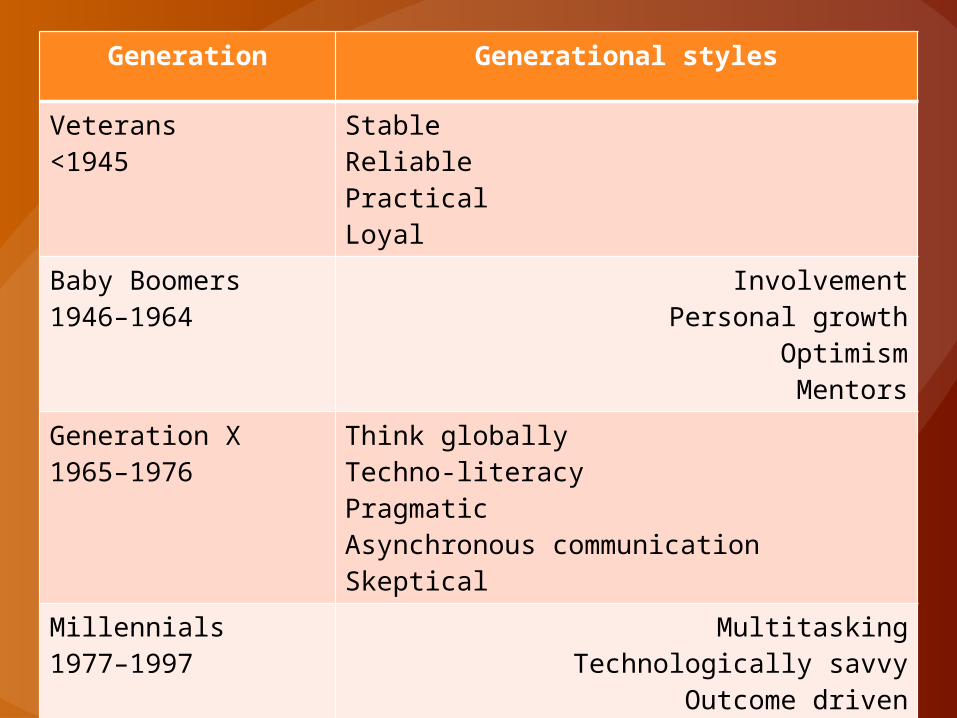
Generation Generational styles
Veterans<1945
StableReliablePracticalLoyal
Baby Boomers1946–1964
InvolvementPersonal growth
OptimismMentors
Generation X1965–1976
Think globallyTechno-literacyPragmaticAsynchronous communicationSkeptical
Millennials1977–1997
MultitaskingTechnologically savvy
Outcome drivenDetermined
Carefronting
Kupperschmidt, B. (2006). Addressing multigenerational conflict: mutual respect and carefronting as strategy. Online Journal Of Issues In Nursing, 11(2),
• Kupperschmidt argues that professional nurses must care enough about their patients, profession, colleagues, and themselves to ‘carefront’ disrespectful behavior

Kupperschmidt, B. (2006).
Treating each other with respect is a nurse's ethical responsibility
Carefronting, a model of communication used when professional nurses care enough about themselves and their patients to confront disrespectful behavior face-to-face
Kupperschmidt, B. (2006)
Failure to
confront is
dishonest
communicationCarefronting embodies forgiveness, caring and valuing, while addressing the anger in the disrespectful behavior, and focuses on the here and now
Kupperschmidt, B. (2006)
The goal is the ability to work together to provide safe patient care in an environment based upon mutual respect
Kean University GraduatesBivins & Primus 2012 Developed the:Perceived Carefronting Ability Questionnaire
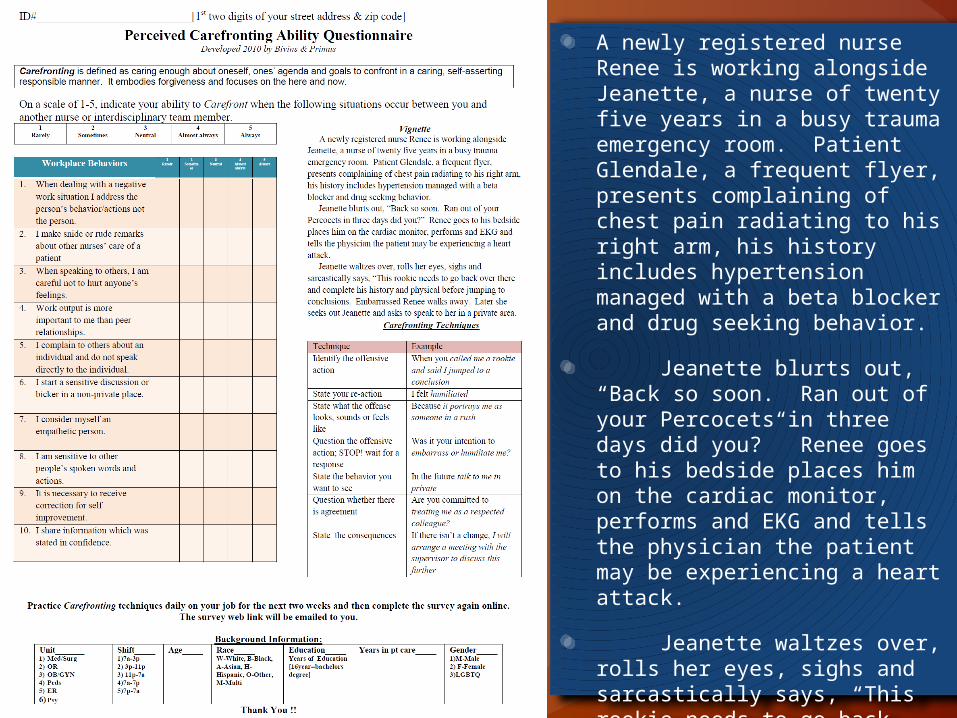
A newly registered nurse Renee is working alongside Jeanette, a nurse of twenty five years in a busy trauma emergency room. Patient Glendale, a frequent flyer, presents complaining of chest pain radiating to his right arm, his history includes hypertension managed with a beta blocker and drug seeking behavior.
Jeanette blurts out, “Back so soon. Ran out of your Percocets in three days did you?” Renee goes to his bedside places him on the cardiac monitor, performs and EKG and tells the physician the patient may be experiencing a heart attack.
Jeanette waltzes over, rolls her eyes, sighs and sarcastically says, “This rookie needs to go back over there and complete his history and physical before jumping to conclusions. Embarrassed Renee walks away. Later she seeks out Jeanette and asks to speak to her in a private area.
Yvonne Bivins MSN RNNadia Primus MSN RN
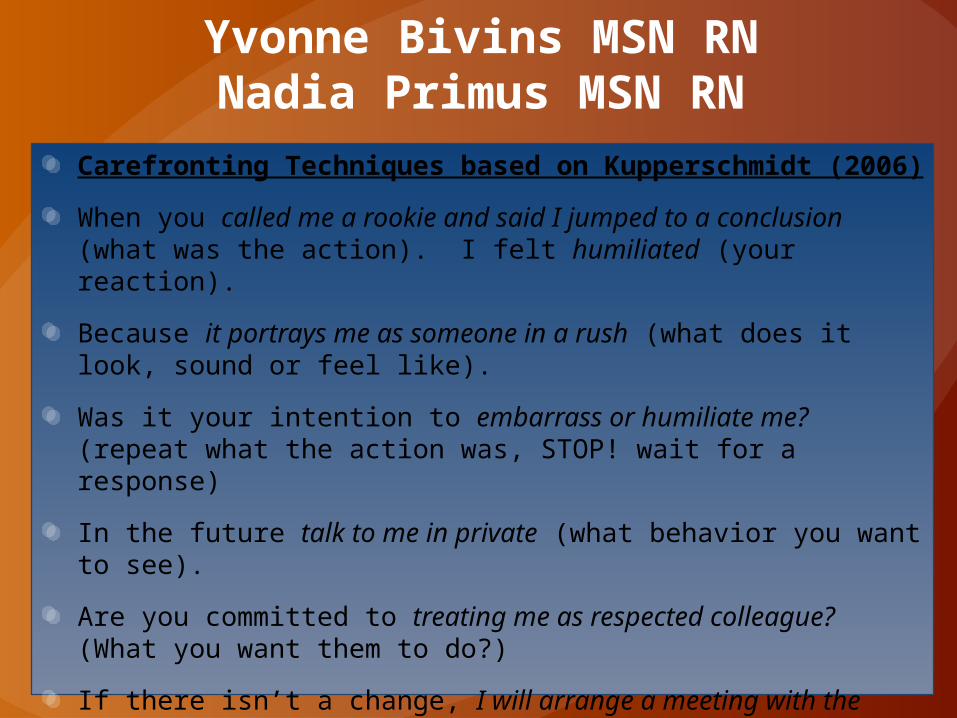
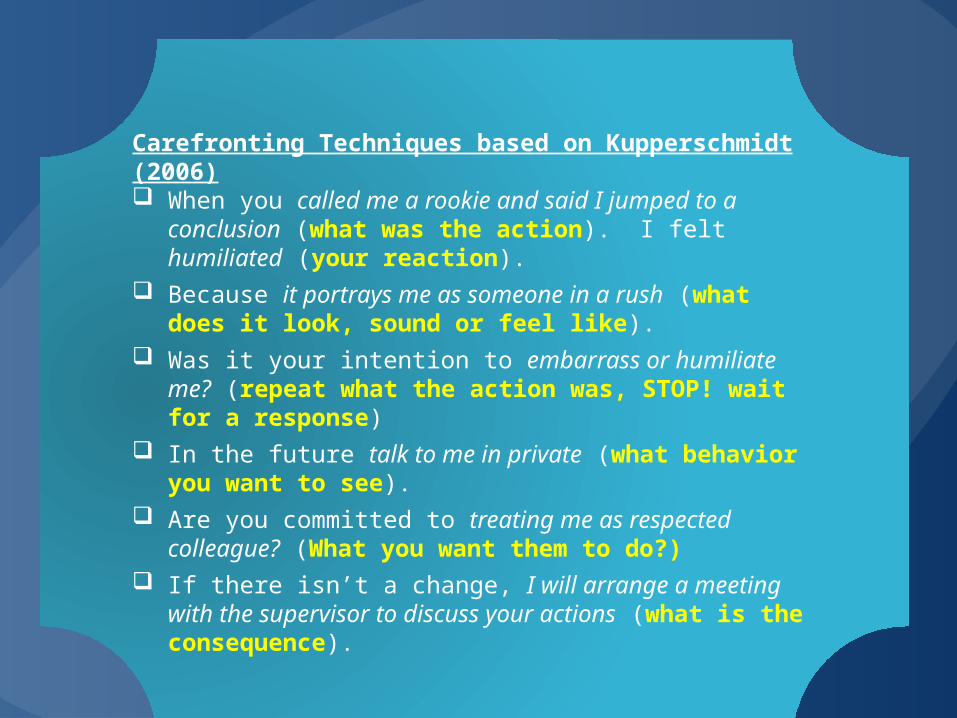
Carefronting Techniques based on Kupperschmidt (2006)
When you called me a rookie and said I jumped to a conclusion (what was the action). I felt humiliated (your reaction).
Because it portrays me as someone in a rush (what does it look, sound or feel like).
Was it your intention to embarrass or humiliate me? (repeat what the action was, STOP! wait for a response)
In the future talk to me in private (what behavior you want to see).
Are you committed to treating me as respected colleague? (What you want them to do?)
If there isn’t a change, I will arrange a meeting with the supervisor to discuss your actions (what is the consequence).
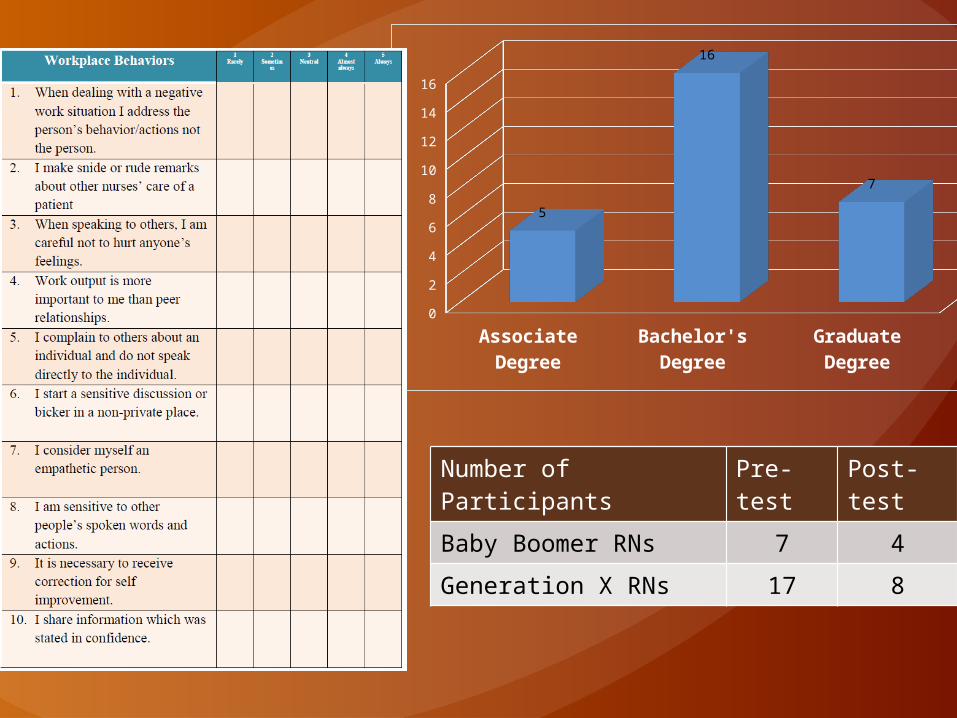
Number of Participants Pre-test Post-test
Baby Boomer RNs 7 4
Generation X RNs 17 8
Associate Degree
Bachelor's Degree
Graduate Degree
0
2
4
6
8
10
12
14
16
5
16
7
Yvonne Bivins MSN RNNadia Primus MSN RN
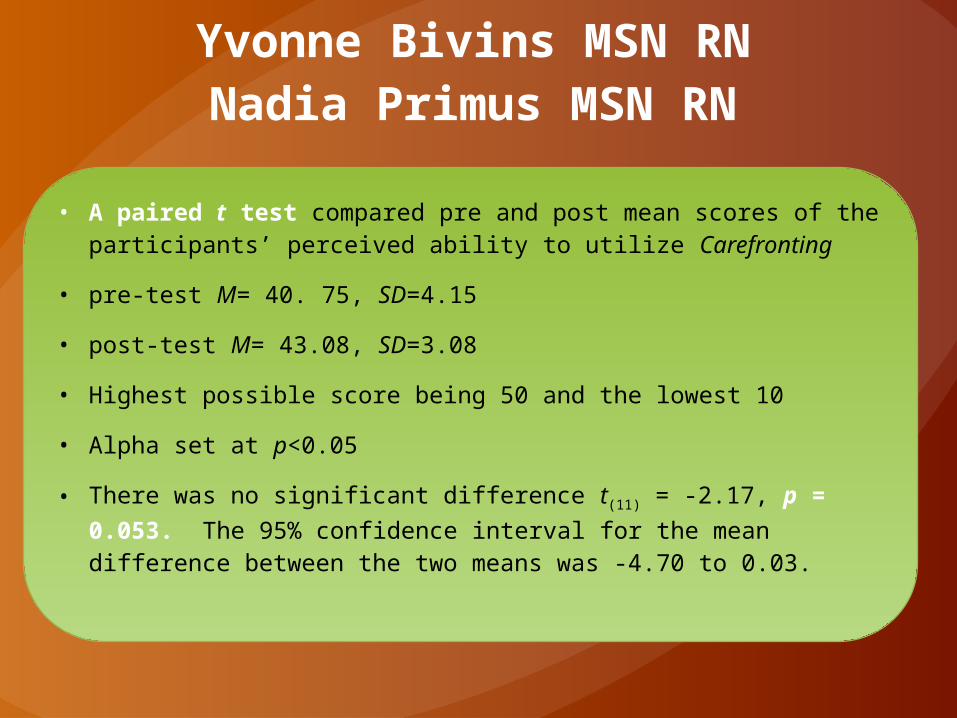
• A paired t test compared pre and post mean scores of the participants’ perceived ability to utilize Carefronting
• pre-test M= 40. 75, SD=4.15
• post-test M= 43.08, SD=3.08
• Highest possible score being 50 and the lowest 10
• Alpha set at p<0.05
• There was no significant difference t(11) = -2.17, p = 0.053. The 95% confidence interval for the mean difference between the two means was -4.70 to 0.03.
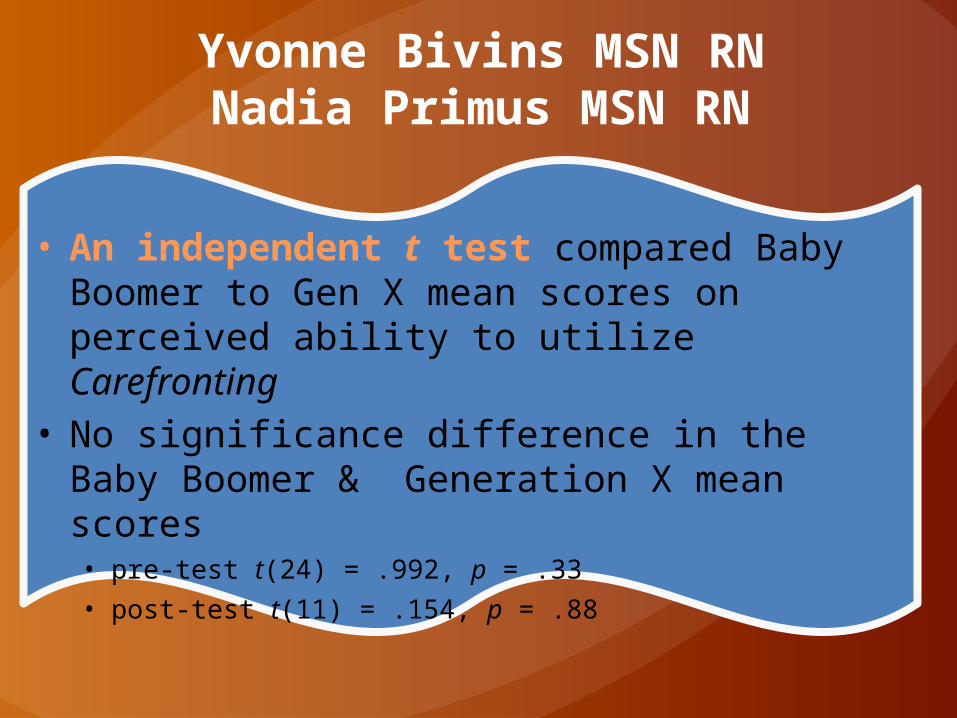
• An independent t test compared Baby Boomer to Gen X mean scores on perceived ability to utilize Carefronting
• No significance difference in the Baby Boomer & Generation X mean scores • pre-test t(24) = .992, p = .33 • post-test t(11) = .154, p = .88
Yvonne Bivins MSN RNNadia Primus MSN RN
Carefronting Techniques based on Kupperschmidt (2006) When you called me a rookie and said I jumped to a conclusion
(what was the action). I felt humiliated (your reaction). Because it portrays me as someone in a rush (what does it look,
sound or feel like). Was it your intention to embarrass or humiliate me? (repeat what
the action was, STOP! wait for a response) In the future talk to me in private (what behavior you want to
see). Are you committed to treating me as respected colleague? (What
you want them to do?) If there isn’t a change, I will arrange a meeting with the supervisor
to discuss your actions (what is the consequence).

Take homeMessage
Caring enough to confront may help
Carefronting comes from a place of love, not bitterness or hate
1. Horizontal Violence and Generational Conflict are a problem within nursing
2. Both are highly detrimental to the body of Black nurses
Top Related