




Languages
Pages
Legal


Vitamins & Trace elements –What is evidence based?
Micronutrients in clinical nutrition How much evidence is required?
Pr. Mette M BergerAdult Intensive Care & Burns CentreCHUV – Lausanne - Switzerland

Paleolithic nutrition revisitedEstimated daily paleolithic intake vs. actual
Eaton SB et al, Europ J Clin Nutr, 51: 207, 1997
Paleolithic RDA Current USEnergy (kcal) 3000 2200-2900 1750-2000Fiber (g) 104 20-30 10-20Riboflavin (mg) 6.5 1.3-1.7 1.3-2.1Folate 0.36 0.2 0.15-0.2Thiamin 3.9 1.1-1.5 1.1-1.8Ascorbate 604 60 77-109 Carotene (RE) 2870 800-1000 1170Tocopherol 32.8 8-10 7-10Iron 87.4 10-15 10-11Calcium 1960 800-1200 750Zinc 43.4 12-15 10-15
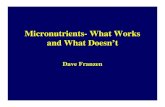
MICRONUTRIMENTS et IMMUNITÉ CELLULAIRE
ZnB6
thymuline
thymulineactive
thymus
ZnB6
Vit A
synthèse IL-2, IL-3
maturation des LT
lymphocyte T
Zn
polynucléaires
macrophages
IL - 1
chimiotactismephagocytosebactéricidie
ZnSeCuB9
Vit C
action mitogéniquedirecte
ZnSeB6B9
Vit AVit EJF Zazzo

Malnutrition and InfectionAlternative model - Beck MA 1999
MalnutritionMicronutrient deficiency
Oxidative stress
Immunity virus virulenceSusceptibility to pathogens
(viral, bacteria, fungi)
Infections

Micronutrients – in clinical nutrition- in clinical settings?
Micronutrients = integral part of nutritionProportionality between macro-and micro-nutrientsAnswer 1 – Evidence Level A
Micronutrients = pharmacologic agentsaiming at AOX reinforcementAnswer 1 – Evidence Level A
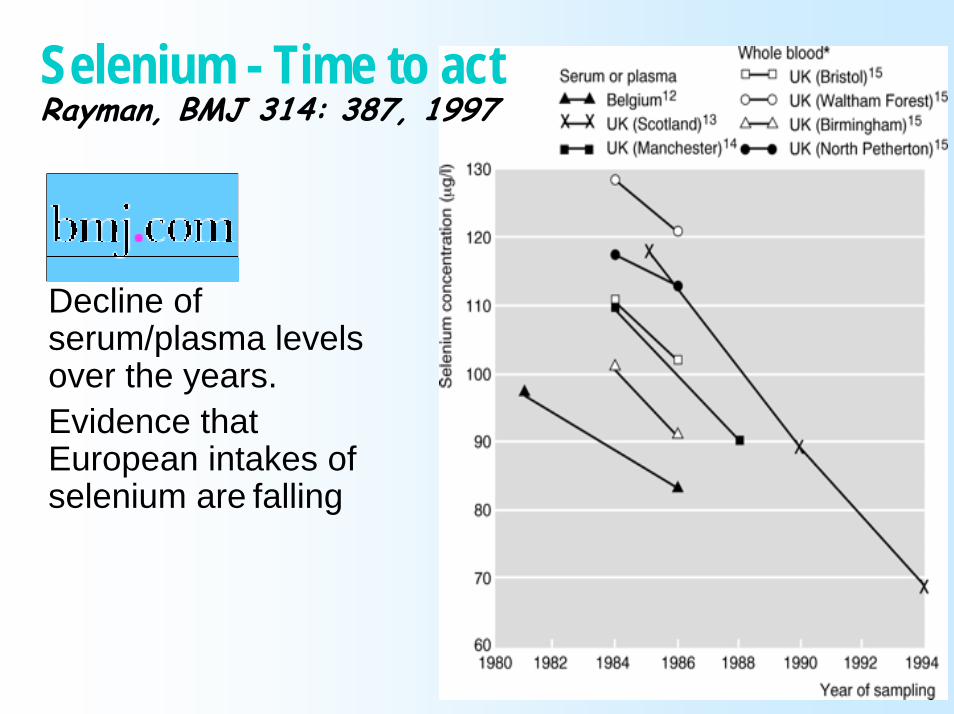
Decline of serum/plasma levels over the years.Evidence that European intakes of selenium are falling
Selenium - Time to act Rayman, BMJ 314: 387, 1997

The argument for ⇑ selenium intakeRayman MP, Proc Nutrition Society 61: 203 2002
Recent mean levels of serum or plasma Se in Europe compared with (---), bottom tertile in Nutritional Prevention of Cancer (NPC) trial of Clark et al. (1996); (·····), level required for optimal plasma GPx activity

Status in Critical illnessOxidative stressTrace elements

Plasma redox status relates to severity in critically ill patients
Alonso de Vega J et al, CCM 28:1812, 2000
APACHE III scores and plasma redox status (r2 = 0.56; p < .001) as defined by the ratio total antioxidant capacity (mM) /lipoperoxides (uM)
APACHE III scores and plasma myeloperoxidase concentrations (r2 = 058; p < .001)
73 patients at admission to a mixed ICU: 8 deaths

Reactive oxygen species production in the critically ill
Infection, acute illnessSurgery (major thoracic, abdominal)Trauma, burn
Local +systemic response
SIRS
ICU ttt- mech vent
- cvvh- drugs
Secondary organ failure:
gut, liver, kidney, lung,
Brain …
ShockReperfusion
injury

TE status challenges in critically illBorderline/actual deficiency: frequentCausesAcute phase response stress
redistribution to liver, spleendepletion of vascular compartment
Losses ⇐ condition (exudates, drains, urines, digestive losses)
Losses ⇐ treatment (CVVH, ..)⇑ requirements (hypermetabolism, oxidative stress)Low intakes (EN < 2000 kcal, poor absorption, no IV supplements)

Antioxidants status in the critically illSelenium in plasma
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
µmol/L
ICU ICU SIRS SIRS Sepsis Trauma D2 Burns D2n = 175 134 42 94 40 43 45
Ref Hawker F. Angstwurm Forceville 98 Berger 96 Berger 92-98
Se pl
asma
leve
ls

Negative balances – the causes in critically illBerger, NCP 21:438, 2006
Pre-admission deficit

Trace elements in burns : Balance studyZinc losses
Berger et al, Burns 1992, 18:373
n = 10TBSA 33 %
0
50
100
150
200
Zn (m
g)
0 1 2 3 4 5 6 7Days post-injury
Cutaneous exsudate
Aspirations
Feces
Urine

TE in TraumaSe Balances (without supplements)
Berger MM et al, J Trauma, 40:103, 1996
n = 11x ± sd
-100
-75
-50
-25
0
25
µg /
24h
0 1 2 3 4 5 6 7Days post-injury
Berger et al 1994
Selenium
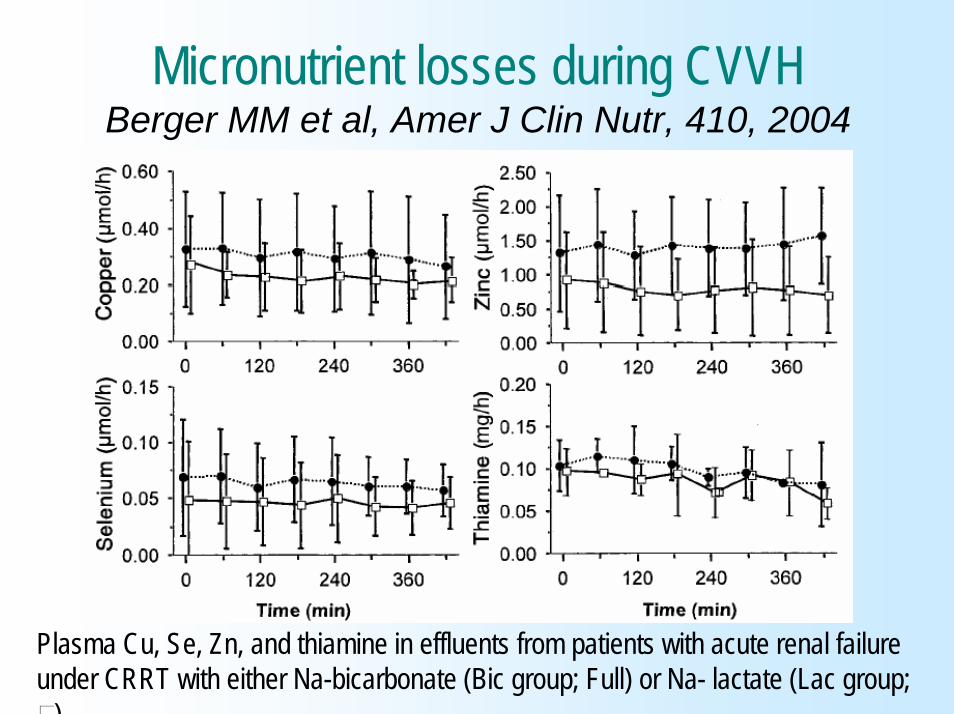
Micronutrient losses during CVVHBerger MM et al, Amer J Clin Nutr, 410, 2004
Plasma Cu, Se, Zn, and thiamine in effluents from patients with acute renal failure under CRRT with either Na-bicarbonate (Bic group; Full) or Na- lactate (Lac group;
)
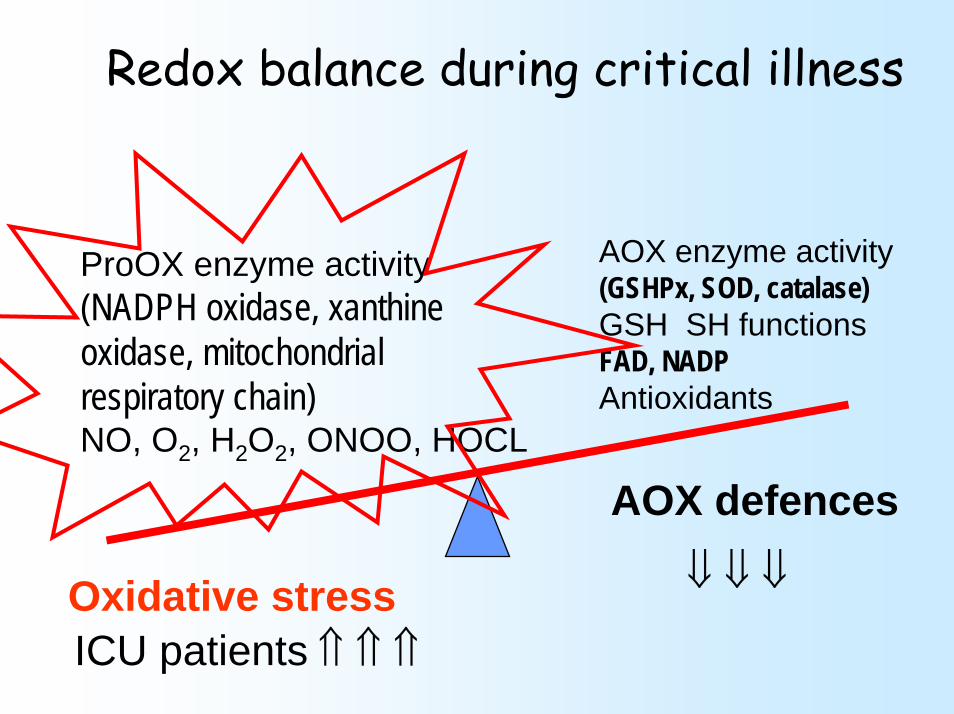
Redox balance during critical illness
ProOX enzyme activity(NADPH oxidase, xanthine oxidase, mitochondrialrespiratory chain)NO, O2, H2O2, ONOO, HOCL
AOX enzyme activity(GSHPx, SOD, catalase)GSH SH functionsFAD, NADPAntioxidants
Oxidative stressICU patients ⇑ ⇑ ⇑
⇓ ⇓ ⇓
AOX defences

AntioxidantDefinition
Any substance that significantly delays or inhibits oxidation of a substrate, when present at low
concentrations compared to those of that substrate
Halliwell B & Gutteridge JMC, 1989

Antioxydants endogènesd’origine nutritionnelle
Eléments traces Cuivre (pro-)ManganèseSéléniumZinc
Vitamines Vitamine CVitamine ERétinol (A)Vitamine Q10

Can oxidative damage be ttt nutritionally?Berger MM Clin Nutr, 2005
NutritionalAOX intakeAOX defence
Qua
ntity
Oxidative damage
Normalrange
Time (minutes → years)
Injury – Acute disease
1
2

Evidences in the critically illFrequent pre-illness precarious conditionIncreased metabolic requirementsNegative micronutrient balances are frequent in the ICU due to
losses of biological intakes and hypocaloric feeding
Oxidative stress +++AOX Micronutrients are depleted
What should we do?

PRCT TE supplementation trial in major burns- Outcome
Berger et al, Am J Clin Nutr, 1998, 68:365
Group Placebo Group TEn = 10 n = 10
Death 0 1Infections 3.0 ± 1.0 * 1.9 ± 0.8 *LOS 66 ± 31 54 ± 27LICU/ BSA 0.6 ± 0.3 0.4 ± 0.2LBU / BSA 0.9 ± 0.3 * 0.6 ± 0.2 *LOS / BSA 1.5 ± 0.8 1.1 ± 0.7* p < 0.02, BU = Burns Unit

TE supplements in burns3 consecutive trials – Se doses
Berger & Chiolero, Crit Care & Shock, 2002, 2:91
0.00
0.50
1.00
1.50µmol/L
0 5 10 15 20 25Days
Selenium
Trial2Trial 1Trial 3Placebo
Se dose1: 0.6 µmol
2: 2.93 µmol
3: 4.8 µmol

Burns : Tissue Se, Zn & GSH…Berger et al, Amer J Clin Nutr, 2007
p < 0.01
p < 0.02

Trace element (Cu,Se,Zn) substitution in Burns - Nosocomial pneumoniaBerger et al, 2006, Crit Care e-pub
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
3 8 13 18 23 28 Days
ETP
65% reductionof pneumonia
risk
Aggregation of 2 consecutiveRandomizedtrials
Log Rank p=0.0014Wilcoxon p=0.0019
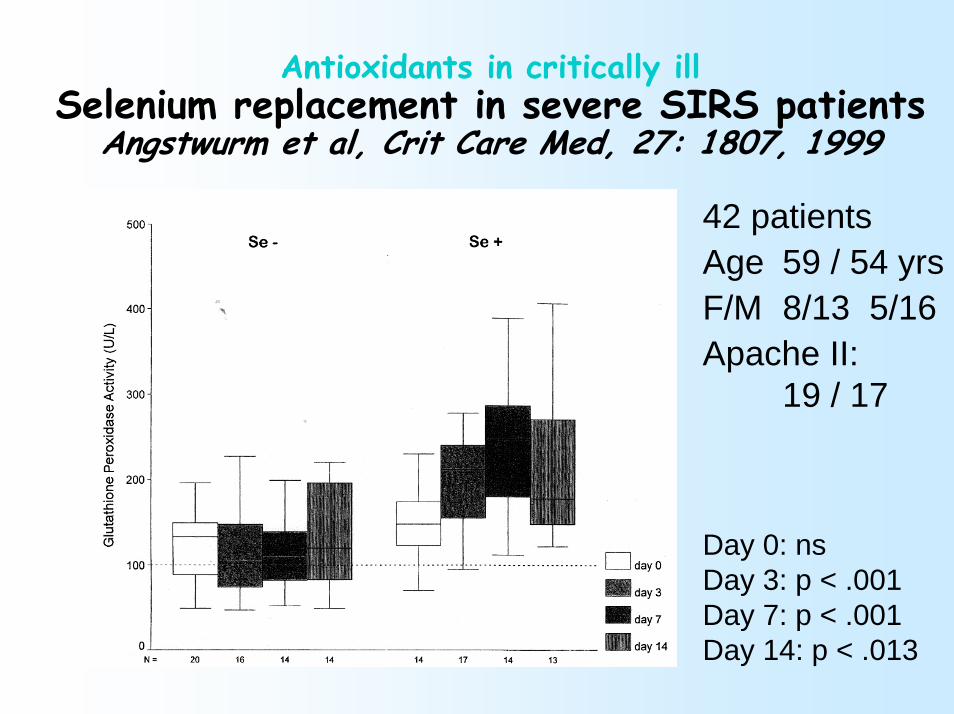
Antioxidants in critically illSelenium replacement in severe SIRS patients
Angstwurm et al, Crit Care Med, 27: 1807, 1999
42 patientsAge 59 / 54 yrsF/M 8/13 5/16Apache II:
19 / 17
Day 0: nsDay 3: p < .001Day 7: p < .001Day 14: p < .013

AOX Trace elements reduce mortality in ICU patients - Selenium
Heyland et al, Intensive Care Med, 31:321, 2005
199119961997
RR 0.52 – 95% confidence intervals 0.28-0.94, p = 0.04Trials with positive impact used TE (Se and Zn)Vitamins alone: no impact
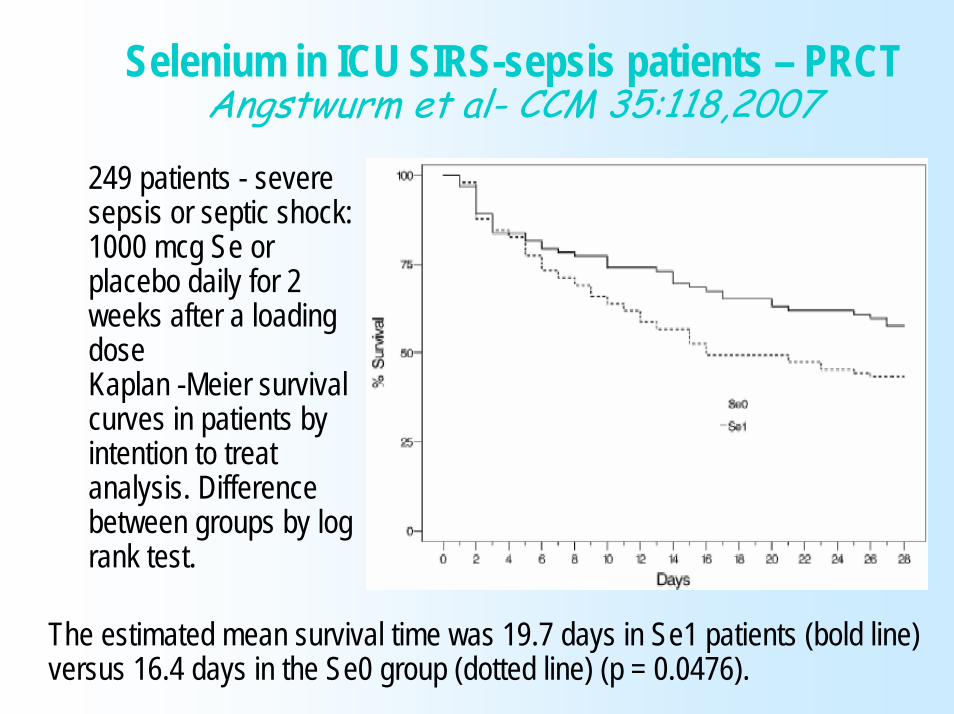
Selenium in ICU SIRS-sepsis patients – PRCTAngstwurm et al- CCM 35:118,2007
249 patients - severe sepsis or septic shock: 1000 mcg Se or placebo daily for 2 weeks after a loading doseKaplan -Meier survivalcurves in patients by intention to treatanalysis. Differencebetween groups by log rank test.
The estimated mean survival time was 19.7 days in Se1 patients (bold line) versus 16.4 days in the Se0 group (dotted line) (p = 0.0476).

AOX trial – 200 ICU patients: trauma-cardiacSe-Zn, Vit E, Vit C, Vit B1Berger et al in preparation
0.00.10.20.30.40.50.60.70.80.91.0
Prob
abili
ty o
f hsp
ital s
tay
0 10 20 30 40 50 60 70 80 90 100 120 140Total LOS (days)
Prob>Chi2
Log Rank p=0.248Wilcoxon p=0.180
Pro
abilit
y of
hos
pita
l sta
y
0.00.10.20.30.40.50.60.70.80.91.0
0 10 20 30 40 50 60 70 80 90 100 110 120Total LOS (days)
Log-Rank p=0.0177Wilcoxon p=0.0039
PlaceboAOX
Pro
abilit
y of
hos
pita
l sta
y
0.00.10.20.30.40.50.60.70.80.91.0
0 10 20 30 40 50 60 70 80 90 100 110 1200.00.10.20.30.40.50.60.70.80.91.0
0.00.10.20.30.40.50.60.70.80.91.0
0 10 20 30 40 50 60 70 80 90 100 110 1200 10 20 30 40 50 60 70 80 90 100 110 120Total LOS (days)
Log-Rank p=0.0177Wilcoxon p=0.0039
PlaceboAOXPlaceboAOX
All 200:
Kaplan-Meyer analysis of length of hospital stay in all 200 and trauma surviving patients –trend (p=0.18) to shorter stay in supplemented patients – significant in trauma

Supplementation
Enteral or I.V.or both?

Intestinal absorption of micronutrientsTrace elements Absorption Body pool
Fe 5-15% 3-5 gZn 10-30% 3 gCu 20-50% 150 mgSe 80-90% 9 mgMn 1.3%M, 3.6%F 2.5 mgCr III 0.4-2.5% < 1 mg
Vitaminsthiamine - B1 90%A 70-90%K 80-100%

Influence of fluid resuscitation on visceral edema
Kinsky MP et al, J Trauma, 49: 844 2000Tissue water content for colon, ileum, kidney, liver, pancreas, and skeletal muscle. Mean ± SEM from 9 to 12 animals per group. Asterisk indicates p < 0.05, HSD (7.5% NaCl/6% dextran70) versus LR; [psi], p < 0.05, HSD vs nonburned skin; [delta], p < 0.05, LR vsnonburned skin.

0
50
100
150µg/L
Se-1 Se+1 Se+3 Se+5
Selenium
Mean
14
13
12
11
10
9
8
7
6
5
4
3
2
1
0
1
2
µmol/l
Cr-1 Cr+1 Cr+3 Cr+5
Chromium
0
5
10
15
20
Preop Op +1 +3 +5
Time (days)
Zinc
Patients
0
50
100
150µg/L
Se-1 Se+1 Se+3 Se+5
Selenium
Mean
14
13
12
11
10
9
8
7
6
5
4
3
2
1
0
50
100
150µg/L
Se-1 Se+1 Se+3 Se+5
Selenium
Mean
14
13
12
11
10
9
8
7
6
5
4
3
2
1
0
1
2
µmol/l
Cr-1 Cr+1 Cr+3 Cr+5
Chromium
0
1
2
µmol/l
Cr-1 Cr+1 Cr+3 Cr+5
Chromium
0
5
10
15
20
Preop Op +1 +3 +5
Time (days)
Zinc
0
5
10
15
20
Preop Op +1 +3 +5
Time (days)
Zinc
Patients
N = 14Age 65 yrs - Weight 70 kg4 days of SupplementationEarly EN with:Chromium 400 ugSelenium 300 ugZinc 20 mg
Safety and intestinal tolerance
of high-dose enteral AOX and
glutamine peptides after upper
gastrointestinalsurgery
Schroeder et alEur J Clin Nutr (2005,
59:307)

0
20
40
60
AT-1 AT+1 AT+3 AT+5
α-tocopherol
Mean
14
13
12
11
10
9
8
7
6
5
4
3
2
1
0
25
50
75µmol/l
AA-1 AA+1 AA+3 AA+5
Ascorbic acid
0
0.2
0.4
0.6
Preop Op +1 +3 +5
Time (days)
ß-carotene
Patients
0
20
40
60
AT-1 AT+1 AT+3 AT+5
α-tocopherol
Mean
14
13
12
11
10
9
8
7
6
5
4
3
2
1
0
20
40
60
AT-1 AT+1 AT+3 AT+5
α-tocopherol
Mean
14
13
12
11
10
9
8
7
6
5
4
3
2
1
0
25
50
75µmol/l
AA-1 AA+1 AA+3 AA+5
Ascorbic acid
0
0.2
0.4
0.6
Preop Op +1 +3 +5
Time (days)
ß-carotene
Patients
0
25
50
75µmol/l
AA-1 AA+1 AA+3 AA+5
Ascorbic acid
0
25
50
75µmol/l
AA-1 AA+1 AA+3 AA+5
Ascorbic acid
0
0.2
0.4
0.6
Preop Op +1 +3 +5
Time (days)
ß-carotene
Patients
0
0.2
0.4
0.6
Preop Op +1 +3 +5
Time (days)
ß-carotene
0
0.2
0.4
0.6
Preop Op +1 +3 +5
Time (days)
ß-carotene
Patients
Safety and intestinal tolerance
of high-dose enteral AOX and
glutamine peptides after upper
gastrointestinalsurgery
Schroeder et alEur J Clin Nutr (2005,
59:307)

Micronutrients: alone or in combination?
ROO-, RO-
ROOH, ROHGSSG
2 GSH
NADPH
NADP+
Ascorbate
Dehydro-Ascorbate
Tocopheryl-
Tocopherol
Glutamic acid+Cysteine+Glycine
α-ceto-glutarate → Glutamate → Glutamine ↔
Selenium +Cysteine+.. ↓GSH-peroxydase
Dihydrolipoic acid
Lipoic acid
ROO-, RO-
ROOH, ROHGSSG
2 GSH
NADPH
NADP+
Ascorbate
Dehydro-Ascorbate
Tocopheryl-
Tocopherol
Glutamic acid+Cysteine+Glycine
α-ceto-glutarate → Glutamate → Glutamine ↔α-ceto-glutarate → Glutamate → Glutamine ↔
Selenium +Cysteine+.. ↓GSH-peroxydase
Selenium +Cysteine+.. ↓GSH-peroxydase
Dihydrolipoic acid
Lipoic acidDihydrolipoic acid
Lipoic acid
Berger & Chiolero CCM 2007

PRCT AOX trial in critically ill surgical patientsNathens AB et al, Ann Surg, 236: 814, 2002
Patient characteristics (mean SD)n = 575 / 770 Placebo (294) AOX (301)Age 39 ± 15 38 ± 15Trauma 268 (91%) 274 (91%)ISS 20 ± 11 19 ± 10APACHE II 14 ± 6 14 ± 6Shock 93 (31%) 78 (26%)LICU 6.4 5.3MOF 18 (6.1%) 8 (2.7%)Mortality hospital 9 (3.1%) 5 (1.7%)

PRCT AOX trial in critically ill surgical patientsRisk of pulmonary morbidity (ARDS or pneumonia)Nathens AB et al, Ann Surg, 236: 814, 2002
Trend to lower likelihood of pulmonary morbidity (p = 0.2)Solid: placebo; ---: AOX
301 patients on AOX supplement294 patients on standard care

Effect of micronutrient supplements on quality of life and ventricular function in elderly CHF patientsWitte K et al, Europ Heart J, 2005, 26:2238Long term (9 months) micronut supplements (Ca,
Mg, Zn, Cu, Se, VitA, B1, riboflavine, B6, folate, B12, vit C, E, D, coenz Q10) vs placebo
30 patients aged 75 yearsLVEF < 35%Results: patients well matched, 2 deathsLV volumes in micronut (-13.1% vs –3.8% in P)LVEF in micronut by 5.3% (no change in P): p <
0.05QoL in micronut by 9.5 (-1.1 in placebo)
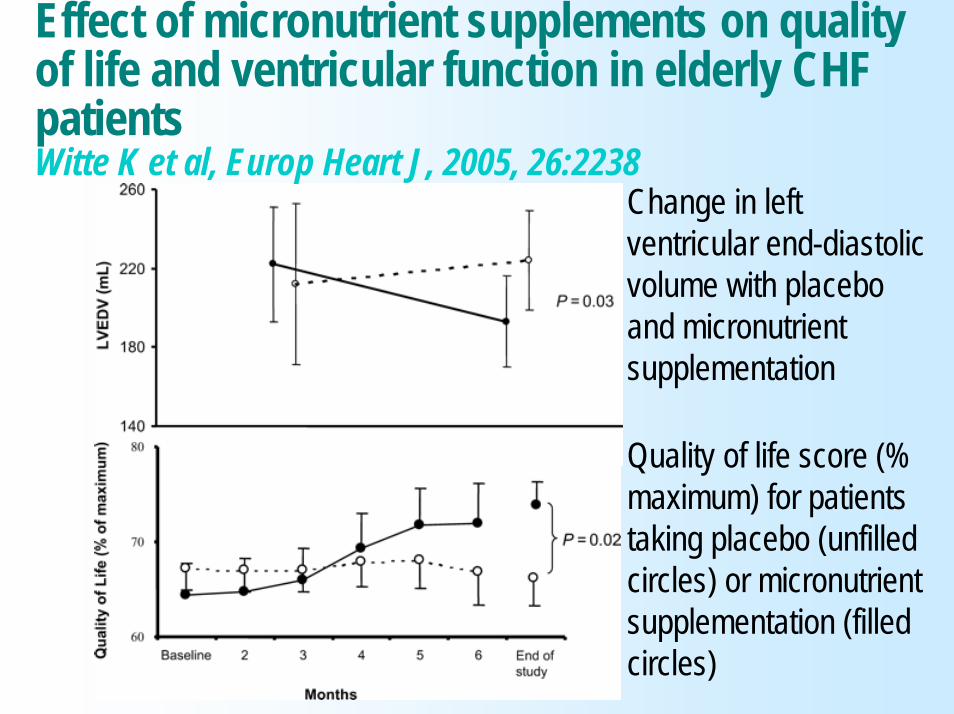
Quality of life score (% maximum) for patients taking placebo (unfilled circles) or micronutrient supplementation (filled circles)
Change in left ventricular end-diastolic volume with placebo and micronutrient supplementation
Effect of micronutrient supplements on quality of life and ventricular function in elderly CHF patientsWitte K et al, Europ Heart J, 2005, 26:2238
Micronutrients in clinical nutrition?How much evidence? Conclusion
Nutrition includes Micronutrients Hypermetabolic patients have requirements of all of them - no further evidence is required
Intakes should with other nutrientsCritically ill have an altered micronutrient status, with a depletion of the circulating compartment
acute phase responselosses
Losses should be SubstitutedTiming: immediately ♣

Micronutrients in ICU patientsConclusions
Oxidative stress is present in in most acute ICU patients
Micronutrients and particularly Se are essential AOX activity can be restored by supplements
Large supplements => better clinical outcome = enough arguments for early intervention
Supplementation is rationalTiming: early therapeutic window

Micronutrients in clinical nutrition?How much evidence? Conclusion
Route: bioavailability - IV only certain Open questions:Which Combinations of micronutrients?
TE: Selenium, ZincVitamins: C, EGlutamine, glutathione, omega-3
Doses? Avoid prooxidation
Trauma, burn & septic ICU patients should receive additional supplementsMinimal combination: Se, Zn, B1
♣

SeleniumA lunatic element3rd millenium: “ THE “ antioxidant
Top Related