






Languages
Pages
Legal


Judith Kallenberg
Vaccine Investment Strategy
GAVI Alliance Board meeting
Phnom Penh, Cambodia
21-22 November 2013

GAVI Alliance Board meeting
21-22 November 2013 1
Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec
Expert consultations, analytical work
Country consultations
at regional meetings
Technical
Consultation
Group
Phase I
recommendations
to Board
Phase I
recommendations
to PPC
Final VIS
recommendations
to Board
Final
recommendations
to PPC
Start of VIS
process
Online stakeholder survey
and in-depth country interviews
WHO
landscape
analysis
PPC guidance
on VIS scope
Technical
Consultation
Group
Independent
Expert
Group
Independent
Expert
Group
Technical
Consultation
Group
Vaccine Investment Strategy: evidence-based
process to identify new priority vaccines

GAVI Alliance Board meeting
21-22 November 2013
Step 1:
analysis
Step 2:
synthesis
Step 3:
recommendation
Direct health impact
Cost and value for money
(relative to current portfolio)
Market-shaping potential
Country views
Global/country
implementation requirements
Key benefits
Key challenges
and risks
Recommendation
and implications
Potential to prevent
disruptive epidemics
Assessment framework for shortlisted vaccine
investments
2

GAVI Alliance Board meeting
21-22 November 2013
5
Cumulative demand estimated to be
760M – 1.2B doses through 2030
2018201720162015
Demand (M doses)
150
100
50
0
203020292028202720262025202420232022202120202019
Expanded EPI with booster
Expanded EPI without booster
EPI with booster
EPI without booster
# countries
introducing0 0 2 3 3 5 5 5 3 4 2 2 0 0 0 0
Note: includes introductions in African countries only (both vaccine licensure and a WHO recommendation are highly
likely to be restricted to Africa; vaccine indication for use in Asia is not expected in the near term); Includes demand
from countries that graduate from GAVI support during 2015-2030 (following GAVI supported introduction)
7
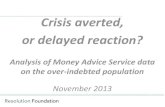
Malaria vaccine may have impact
comparable to Hib
Note: Model outputs shown for Expanded EPI with booster scenario, for illustrative purposes; error bars show highest and lowest value generated by malaria sensitivity analyses and are driven by decay rate of protection; point estimate represents midpoint of Imperial and Swiss TPH models
5,000 1,500
768
668
576541
198
147
63 45 31 2924
0
200
400
600
800
1,000
Rabies HPV Hep B Pneumo Hib Malaria Rota YellowFever
Rubella Influenza Cholera Men A JE
Disruptive epidemic potential(deaths averted less relevant metric)
Future deaths averted per 100k vaccinated1
2
1. Based on deaths averted over 2015-2030; 2. VIS only
Detailed vaccine assessments
11
Vaccine duration of protection is biggest
sensitivity of high impact
Imperial College Swiss TPH
Access to care (25%
decrease or increase)
-600 -400
Transmission (25% - 80% ITN
& treatment coverage)163-220
Vaccine efficacy 50-60% -155 122
Decay rate against
infection (1-5 years)-528 229
-200 200 400
Future deaths averted ('000)
0
Eligibility of
Nigeria-315
Base: 1.3M
200
61
Future deaths averted ('000)
0-200 400
-66
-227
-125 124
-600 -400
Base: 960,000
No sensitivity
analysis run
No sensitivity analysis run
No sensitivity analysis run
Note: For illustrative purposes base case is shown as expanded EPI with booster scenario (midpoint between Imperial College and Swiss TPH model outputs)
21
37 countries in scope for malaria (Africa)
In scope for malaria
Eligible for GAVI support
15
# of responses
80
60
40
20
0
Challenging
and not
desirable
11
Challenging
but beneficial
52
Feasible
and could be
beneficial
76
Respondents positive on ability
to add new visits for 5-17M age group
Respondents emphasized that vaccine could not
displace other malaria interventions
# of responses
100
0
Vaccine
would have
no effect on
other
interventions
3
Vaccine
would likely
boost other
interventions
6
Vaccine may
reduce need
for other
interventions
11
Vaccine
would reduce
need for other
interventions
14
RTS,S is impt
add, but still
need for other
interventions
102
50
150
Country openness to new schedule and awareness
that vaccine cannot replace other interventions
Question: Please indicate the
statement(s) that most closely
apply in your country
Question: Please indicate the statement(s) that
most closely apply in your country
Source: 2013 GAVI Phase II country consultation survey
Note: question only posed to 136 respondents ranking malaria as first or second priority for introduction
16
Area of focus Unique implementation requirements Unique costs
Policies and
processes
WHO position TBD; few required GAVI policy changes currently
foreseen; coordination with the GFATM required N/A
Supply Account for supply constraints through 2020 (impact likely small) No direct costs
Health workforce HR/training requirements for RTS,S similar to those for vaccines
already in health system
N/A
Social mobilisation,
education,
communication
Manage risk to program credibility if efficacy lower than other
vaccines in use (eg. rota)
Additional training/social mobilisation/programmatic investments
for initiating new routine visits for immunisation (expanded EPI
scenario only)
Cost accounted
for in
operational
costs1
Supply chain
infrastructure and
logistics
Requirements for RTS,S similar to those for vaccines already in
health system N/A
Surveillance No unique surveillance requirements N/A
Planning,
coordination,
integration
Expanded EPI scenario would require infrastructure to support at
least one additional touch point
Manage potential for older (not eligible) age groups to present for
vaccination (implications for forecasting in intro year)
Coordinate with malaria control program to ensure vaccine does
not undermine the use of other malaria interventions
Focused
organizational
effort
Glo
ba
l
leve
lC
ou
ntr
y l
eve
l
Unique but manageableMay not be manageable in short
term / within current GAVI model
Implementation would require managing possible
global supply shortage and communication needs
1. Expected to be covered by GAVI Vaccine Introduction Grant, MoH, partners
3

GAVI Alliance Board meeting
21-22 November 2013
Yellow fever: fund additional campaigns
ASSESSMENT
Continued risk of outbreaks in Africa
WHO: additional mass campaigns to cover remaining
unvaccinated populations in high-risk countries
Future populations protected through routine YF use
RECOMMENDATION
Fund additional campaigns from 2015 (~USD140M)
Secretariat to review planning / funding process, including
risk assessment mechanism, in coordination with WHO
4

GAVI Alliance Board meeting
21-22 November 2013
Cholera: make catalytic investment in global
stockpile
ASSESSMENT
Disruptive epidemics, inequitable burden
Low global demand and severe supply shortage relative to
estimated need
RECOMMENDATION
Enlarge stockpile to fight outbreaks, gain experience with
vaccine use, shape the market
Insufficient evidence for broad rollout through recurring,
preventive campaigns in endemic settings: re-evaluate in
next VIS
5

GAVI Alliance Board meeting
21-22 November 2013
Rabies and maternal influenza: re-evaluate in
next VIS
RABIES
Operational feasibility and effectiveness of GAVI support for
rabies vaccines unclear
Re-evaluate in next VIS, and
Fund observational study to fill critical knowledge gaps and
catalyse progress
Mitigate risk of preserving status quo
INFLUENZA
Limited evidence base for impact beyond pregnant woman
Data forthcoming on effects on foetus and infants
Re-evaluate in next VIS
6

GAVI Alliance Board meeting
21-22 November 2013
Malaria: re-assess investment case in
2015/16
ASSESSMENT
A leading cause of death in young children, strong demand
Bednets and spraying can prevent up to 55% of deaths
Vaccine targets remaining burden; complements other malaria
control interventions
Analysis: incremental impact in Africa ≈ Hib/rotavirus
Expert Committee: supportive based on preliminary data
RECOMMENDATION:
Note reasonable case for support based on current analysis;
await final trial data
Back to PPC/Board for decision in 2015/16
7

GAVI Alliance Board meeting
21-22 November 2013
Programme funding implications of
recommendations
2014-2020: ~$200M for YF and cholera
2% of vaccine spending
2016-2020: ~$300M for malaria; US$ 230M/year from 2021
Pending future Board approval
Projected programme costs in US$ millions (vaccine + introduction grant + operational cost)
Budget period: 2014-2015 2016-2020 2021-2030
Cholera stockpile 26 89 -
Yellow fever campaigns 14 95 31
Subtotal 40 184 31
Malaria - 287 2,274
Total VIS incl. malaria 40 471 2,305
Current GAVI portfolio* 3,014 6,895 ~10,000
*Based on demand forecast version 8 8

GAVI Alliance Board meeting
21-22 November 2013
Decide to support new yellow fever vaccine campaigns and request
the Secretariat to develop a process for the funding of individual
campaigns on the basis of robust risk assessments.
Approve a contribution to the global cholera stockpile for use in
epidemic and endemic settings and to that end:
Endorse a net increase in programme budgets for the global cholera
stockpile by US$ 114.5 million for the period 2014-2018. (This
endorsement would constitute acknowledgement of such budget amounts
as an indication of potential future expenditures but would not constitute a
funding approval, decision, obligation or commitment of the GAVI Alliance
or its contributors.);
Approve a net increase of near-term programme liabilities for the global
cholera stockpile (a sub-component of endorsed programme budgets) by
US$ 8.5 million for 2014;
Note the opportunity for the GAVI Alliance to generate impact data based
on the use of the cholera stockpile in emergency settings.
9
The PPC and, where appropriate, the AFC and the EC
recommended to the GAVI Alliance Board that it:

GAVI Alliance Board meeting
21-22 November 2013
Approve an assessment of the feasibility of GAVI support for
rabies vaccines (to be evaluated in the next Vaccine
Investment Strategy process). A funding request for the
outsourced assessment will be included as part of the
Business Plan in 2015.
Note that based on the current assessment there is a
reasonable case for GAVI support for a malaria vaccine, and
that the Board will consider opening a window if and when
the vaccine is licensed, recommended for use by the joint
meeting of the WHO Strategic Advisory Group of Experts and
the Malaria Programme Advisory Committee (expected in
2015) and WHO pre-qualified, taking into account updated
projections of impact, cost and country demand as reviewed
by the PPC.
10
The PPC and, where appropriate, the AFC and the EC
recommended to the GAVI Alliance Board that it:

GAVI Alliance Board meeting
21-22 November 2013
Note the potential public health impact of vaccinating
pregnant women against seasonal influenza and the
need to assess the emerging evidence of impact of
vaccination on neonates, but decides not to open a
funding window for influenza vaccines at this time.
Approve an amount up to US$ 1.5 million to be
added to the 2014 Business Plan to implement the
Board’s VIS decisions through Secretariat and
partner activities as described in section 5.2 of Doc
07.
11
The PPC and, where appropriate, the AFC and the EC
recommended to the GAVI Alliance Board that it:

12
12
Top Related