





Languages
Pages
Legal


Urinary System

Excretory vs. Urinary System –
what is the difference?

Urinary System – 3 functions
• Excretion
• Remove nitrogenous wastes from the blood
• Elimination
• Micturition
• Discharge of wastes to the environment
• Maintains homeostasis of the plasma
• Electrolyte balance
• Water balance
• Acid-base balance of blood

MicturitionProcess that expels urine from the bladder
• Stretch receptors activated as urine accumulates (at 150 mL); fullness continues to intensify
Detrusor muscle contracts
• Forces urine past the internal urethral sphincter
• External urethral sphincter is under voluntary control until 600 mL
Micturition reflex center
• triggered by distension of the bladder
• located in the spinal cord
Neural and emotional factors may lead to incontinence
• Inability to control voiding
• Normal in infants until they learn to control external sphincter
Automatic bladder
• Complete loss of voluntary control over urination
• Catheritization

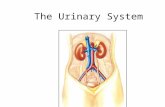
Urinary System
•Pair of kidneys• Produce urine
•Pair of ureters•Use peristalsis to pass urine
to bladder
•Urinary bladder• Temporarily stores the urine
•Urethra• Sends urine to exterior
•8 in. males; 1.5 in. females

Urinary System
HW Check

Urinary System
HW Check



Kidneys
Characteristics
•Reddish brown in color, bean shaped, smooth surface
Location
•Either side of vertebral column
•Positioned retroperitoneally
•Posterior wall of abdominal cavity
•Near back muscles in a depression
•Adipose and connective tissue

Kidneys - Structure• Lateral side (convex)• Medial side (concave)• Medial depression (hilum) leads
to renal pelvis Two distinct regions• Renal medulla (inner)
• Renal columns• Renal pyramids
• Loop of Henle• Collecting Ducts
• Renal cortex (outer)• Glomerulus• PCT• DCT
Capsule• Fibrous membrane
surrounding the kidney
• Pelvis
• Basin like area of kidney; joins the ureter
• Calyx
• Extensions of the pelvis that drains the apex of the pyramid
• Renal Columns
• Cortex like tissue that runs through the medulla


Kidneys - General Functions• Remove nitrogenous wastes from the blood to
form urine
• Filtration, reabsorption, secretion
• Regulate metabolic processes
• Maintains electrolyte and water balances
• Maintains the acid-base balance of the blood
• Secretes erythropoietin for blood cell formation
• Use of renin
• regulates blood pressure
Renal Disease
• Kidney transplant
• result of end stage renal disease
• Hemodialysis
• Direct with blood
• Peritoneal dialysis
• Within abdominal cavity

Kidney Vessels
Renal arteries
• supply kidneys with blood
• enters at the hilum
Renal veins
• carries blood from the kidneys back to the heart
• Exits at hilum

Kidney Vessels
or cortical radiate arteries
or cortical radiate veins

Nephrons
“Functional unit of the kidney”
Renal corpuscle
• composed of a glomerulus• cluster of blood capillaries
• surrounded by Bowman’s/glomerular capsule
Renal Tubule
•PCT, Loop of Henle, DCT• increase SA & efficiency of
the kidney

Urinary System
HW Check

Nephrons – Urine Formation
1. glomerular filtration (glomerulus to Bowman’s capsule)
2. tubular reabsorption (PCT and Loop of Henle)
3. tubular secretion (DCT )

Glomerular Filtration
Water and dissolved substances are filtered out of the glomerulus
•Diffusion & active transport
Glomerular filtrate
• Similar to plasma
•mostly water, salt, glucose, amino acids, and urea
• Sent into the proximal convoluted tubule

Rate of Filtration• Related to pressure
• 125 mL/minute
• 180,000 mL/24 hours (~45 gallons)
• Most of the fluid is reabsorbed into the plasma
• Glomerulonephritis• Protein in urine and
edema
• Shock• result of bp dropping• causes pressure in
glomerulus to drop

Regulation of Filtration
Increases when excess fluid is present
Decreases when fluid needs to be conserved
Renin
• acts with angiotensinogen angiotensin II
• angiotensin II maintains sodium and water balances and blood pressure by vasoconstricting the efferent arteriole
• Also stimulates release of aldosterone for Na to be reabsorbed
Too much renin results in hypertension
• Ace inhibitor to inhibit angiotensin II

Tubular Reabsorption
Primarily in the proximal convoluted tubule
• Contain dense microvilli
Substances are transported out of the filtrate and back into the blood
• Glucose, H2O, amino acids, albumin
R
ole of Na+ in transport of negative ions• chloride, phosphate, bicarbonate
Glucosuriaglucose in the urineIndicator of possible diabetes

Tubular Secretion• Certain substances leave the plasma and enter the renal
tubule
• H and K ions are usually added to filtrate
• Occurs in the PCT and DCT
• Increases some urinary excretions

Osmoregulation (begin at 3:45)
• What organ do we use for osmoregulation?
• What is inside our kidneys?
• What happens on the descending side of the loop of Henle?
• What happens on the ascending side of the loop of Henle?
• What hormone regulates water reabsorption in the collecting duct?
• What is responsible for urine’s color?
http://www.bozemanscience.com/osmoregulation

The Entire Process – This diagram will be VERY useful in Lab

Components of Urine•Blood composition dependent on diet, cellular
metabolism, and urine output
•Urine content dependent on diet and exercise• 180 liters of blood filtered producing 1-1.8 liters of urine produced daily
•95% water, urea, uric acid, amino acids, electrolytes• 3 main components urea, uric acid, creatine
Regulation of Urine ConcentrationADH (antidiuretic hormone)released when concentration of water in the blood decreases
• water retaining hormone; water leaves the collecting duct
• If too low polyuria

Regulation of Urine ConcentrationAldosterone
•hormone that stimulates additional reabsorption of sodium from the collecting duct
• Increases bp
•Can be released in the presence of angiotensin II

Urine Content
Uric acid
• Nucleic acid catabolism
• 10% excreted
• gout
Urea
• Amino acid catabolism
• 50% reabsorbed
Urine Production
1-1.8 liters/day
Volume influenced by
• fluid intake
• environmental and body temp.
• emotional condition
• respiratory rate
Water loss determined by kidneys depends on …
• Evaporation of water from lungs or perspiration on skin

Start Lab
Turn in what you have finished before leaving

Changes in Urine Production
Polyuria
• excess production of urine
• > 2.5 liters in 24 hours
Oliguria
• scanty amounts of urine
• < 500 ml in 24 hours
Anuria
• absence of urine
• < 70 ml in 24 hours

Prostate Cancer Kidney Stones• uric acid, calcium, or magnesium
• collecting ducts and renal pelvis
• pain from ureter stretching
• 60% pass on their own
• Sound waves (lithotripsy)

Cystitis
•bladder infection
•bacterial or from residual urine
More common in females – Why?

Urinalysis• Reveal diseases
• diabetes, glomerulonephritis, chronic UTI
• Paper or plastic dipstick
• Microscopic observations
• Uric acid crystals – normal
Begins with a visual observation
Normal:
• Pale to dark yellow
• Clear
• 750-2000 ml/24 hour
Not normal but not disease
• Turbidity
• Excessive cellular material or protein
• Red or red-brown color
• Food dye
• Increased RBC
Uric acid crystals are increased pathologically in
urine in gout and in leukemia being treated with
chemotherapy

UrinalysisDipstick screening:
pH
•6 is normal
•Range is 4.5 – 8.0
Protein
Glucose
Ketones
•diabetes or starvation
Nitrite
•Presence of bacteria

Microscopic Analysis:RBC
• Should not be present
• Could indicate: glomerular damage, tumors of the urinary tract,
kidney trauma, urinary
tract stones, renal infarcts,
UTI infection
WBC
• UTI infections
or associated
STI’s
There are white blood cells,
bacteria and mucus present.
The number of white blood
cells could suggest the
presence of a urinary tract
infection. If the white blood
cells were not present,
the bacteria could indicate a
poorly collected or
unpreserved specimen.

Microscopic Analysis:Epithelial Cells (black arrows)
• Present in small numbers
• Indicates tubular degeneration
CASTS
• Formed in distal convoluted tubule or the collecting duct
• RBC cast indicative of glomerulonephritis
• WBC cast indicative of end stage renal disease

Microscopic Analysis:Crystals
• Calcium oxalate (blue arrow)
• Triple phosphate
• Cystine• Severe liver diseases Calcium oxalate crystals (shown above blue
arrow) can be present in urine when oxalate-rich
foods such as tomatoes, spinach, garlic, oranges,
and asparagus are ingested.
Top Related