







Languages
Pages
Legal


Towards Understanding Users’ Motivation toShare Health Information on Facebook
by
Sadegh Torabi
B.Sc. in Computer Engineering, Kuwait University, 2005
M.Sc. in Computer Engineering, Kuwait University, 2009
A THESIS SUBMITTED IN PARTIAL FULFILLMENT
OF THE REQUIREMENTS FOR THE DEGREE OF
Master of Applied Science
in
THE FACULTY OF GRADUATE AND POSTDOCTORAL STUDIES
(Electrical and Computer Engineering)
The University of British Columbia(Vancouver)
April 2016
c© Sadegh Torabi, 2016

Abstract
Motivated by the two-way benefits, people have used a variety of web-based
services to share health information (HI) online. Among these services, Face-
book, which enjoys the largest population of active subscribers, has become a
common place for sharing various types of HI. At the same time, Facebook was
shown to be vulnerable to various attacks, resulting in unintended information
disclosure, privacy invasion, and information misuse. As such, Facebook users
face the dilemma of benefiting from HI sharing and risking their privacy.
In this work, we investigate HI sharing practices, preferences, and risk
perceptions among Facebook users. Our exploration focused on two main
goals: (1) to identify the key factors that influenced users’ motivation to share
HI on Facebook, and (2) to highlight a number of features that could motivate
people toward engaging in effective HI sharing on Facebook.
To achieve these goals, we first surveyed 166 active Facebook users about
their HI sharing practices and risk perceptions. We quantified HI sharing prac-
tices and confirmed that it has become a common practice among users. More-
over, we found that the type of the shared HI and its recipients, can highly
ii

influence users’ perceived privacy risks when sharing HI. Following our pre-
liminary survey, we interviewed 21 participants with chronic health conditions
to identify the key factors that influence users’ motivation to share HI on Face-
book. Then, we conducted an online survey with 492 Facebook users in order
to validate, refine, and extend our findings.
The results suggest that the gained benefits from prior HI sharing experi-
ences, and users’ overall attitudes toward privacy, correlate with their motiva-
tion to disclose HI. Furthermore, we identify other factors, specifically users’
perceived health and the audience of the shared HI, that appear to be linked
with users’ motivation to share HI. Finally, we suggest design improvements—
such as anonymous identity as well as search and recommendation features—
for facilitating HI sharing on Facebook and similar sites.
iii
Preface
The author of this thesis conducted all the presented user studies (Chapters 4–
6). He was responsible for collecting and analyzing the data. He also au-
thored the corresponding publication(s) under the supervision of Dr. Kon-
stantin Beznosov, who provided feedback and guidance throughout the re-
search. The preliminary user study presented in chapter 4 of this thesis was
presented in the 2013 USENIX Workshop on Health Information Technologies
(HealthTech’13):
S. Torabi and K. Beznosov. Privacy Aspects of Health Related Information
Sharing in Online Social Networks. In USENIX Workshop on Health Informa-
tion Technologies (HealthTech’13). USENIX Association, August 2013.
All three user studies presented in this work were reviewed by the Univer-
sity of British Columbia’s Behavioural Research Ethic Board (BREB). Three hu-
man ethics applications were submitted with the BREB numbers H13-00370,
H13-03277, and H15-02520 for chapters 4 to 6 respectively. The approval
certificate are available in Appendices A to C.
iv

Table of Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ii
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iv
Table of Contents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
List of Tables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . x
List of Figures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xii
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xiv
Dedication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xv
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2 Background and Related Work . . . . . . . . . . . . . . . . . . . . . . 5
2.1 Social networking sites (SNSs) . . . . . . . . . . . . . . . . . . . . . 5
2.2 Sharing HI on SNSs . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
2.2.1 Perceived benefits . . . . . . . . . . . . . . . . . . . . . . . . 7
v

2.2.2 Perceived health status . . . . . . . . . . . . . . . . . . . . . 8
2.2.3 Perceived privacy . . . . . . . . . . . . . . . . . . . . . . . . 8
3 Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3.1 Preliminary study: privacy perceptions and risk-mitigating be-
haviors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3.2 Exploratory study: interviews . . . . . . . . . . . . . . . . . . . . . 12
3.3 Confirmatory study: online survey . . . . . . . . . . . . . . . . . . 13
3.4 Limitations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
3.5 Ethical considerations . . . . . . . . . . . . . . . . . . . . . . . . . . 15
4 Preliminary Study: Privacy Perceptions and Risk-Mitigating Be-
haviors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
4.1 Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
4.1.1 Participant recruitment . . . . . . . . . . . . . . . . . . . . . 18
4.1.2 Data collection . . . . . . . . . . . . . . . . . . . . . . . . . . 19
4.1.3 Survey items . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
4.2 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
4.2.1 Participant demographics and SNS usage . . . . . . . . . . 21
4.2.2 HI sharing practices . . . . . . . . . . . . . . . . . . . . . . . 21
4.2.3 Perceived privacy risks . . . . . . . . . . . . . . . . . . . . . 26
4.2.4 Risk-mitigation behaviors . . . . . . . . . . . . . . . . . . . 32
4.2.5 Results summary . . . . . . . . . . . . . . . . . . . . . . . . . 33
4.3 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
vi

5 Exploratory Study: Interviews . . . . . . . . . . . . . . . . . . . . . . 37
5.1 Methodology and research questions . . . . . . . . . . . . . . . . . 37
5.1.1 Sampling and participants recruitment . . . . . . . . . . . 38
5.1.2 Data collection . . . . . . . . . . . . . . . . . . . . . . . . . . 39
5.1.3 Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
5.2 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
5.2.1 HI sharing practices on SNSs . . . . . . . . . . . . . . . . . 42
5.2.2 Perceived benefits . . . . . . . . . . . . . . . . . . . . . . . . 43
5.2.3 The recipients of the shared HI . . . . . . . . . . . . . . . . 43
5.2.4 Perceived health status . . . . . . . . . . . . . . . . . . . . . 45
5.2.5 Perceived privacy . . . . . . . . . . . . . . . . . . . . . . . . 46
5.2.6 HI Sharing preferences . . . . . . . . . . . . . . . . . . . . . 51
5.2.7 Results summary . . . . . . . . . . . . . . . . . . . . . . . . . 53
6 Confirmatory Study: Online Survey . . . . . . . . . . . . . . . . . . . 54
6.1 Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
6.1.1 Why Facebook? . . . . . . . . . . . . . . . . . . . . . . . . . . 54
6.1.2 Participants recruitment . . . . . . . . . . . . . . . . . . . . 55
6.1.3 Data collection . . . . . . . . . . . . . . . . . . . . . . . . . . 55
6.1.4 Data analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
6.1.5 Survey items . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
6.2 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
6.2.1 Demographics . . . . . . . . . . . . . . . . . . . . . . . . . . 59
vii

6.2.2 Perceived health status . . . . . . . . . . . . . . . . . . . . . 61
6.2.3 Attitudes toward privacy . . . . . . . . . . . . . . . . . . . . 65
6.2.4 HI sharing experiences . . . . . . . . . . . . . . . . . . . . . 66
6.2.5 Motivation to share HI on Facebook . . . . . . . . . . . . . 68
6.2.6 Preferred recipients of the shared HI . . . . . . . . . . . . 71
6.2.7 Willingness to search for specific users . . . . . . . . . . . 73
6.2.8 Anonymous identity . . . . . . . . . . . . . . . . . . . . . . . 74
6.2.9 Willingness to trust SNSs with HI . . . . . . . . . . . . . . 80
7 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
7.1 Motivating factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
7.2 Implications for design . . . . . . . . . . . . . . . . . . . . . . . . . . 85
7.2.1 Search features . . . . . . . . . . . . . . . . . . . . . . . . . . 85
7.2.2 Anonymous online identity . . . . . . . . . . . . . . . . . . 85
7.2.3 Trusted SNS providers . . . . . . . . . . . . . . . . . . . . . 86
8 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
9 Future Work . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
Bibliography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
A Supplementary Materials for the Preliminary User Study . . . . . 98
A.1 Survey Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101
A.1.1 Questions About Participants’ Demographics . . . . . . . . 101
viii

A.1.2 Questions About SNS Usage . . . . . . . . . . . . . . . . . . 102
A.1.3 Questions About HI Sharing Behaviours in SNSs . . . . . 103
A.1.4 Questions About Privacy Risk Perceptions and Behavioural
Responses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
A.2 Categorization of HI examples . . . . . . . . . . . . . . . . . . . . . 107
B Supplementary Materials for the Exploratory Study (Interviews) 109
B.1 Interview guide and questions . . . . . . . . . . . . . . . . . . . . . 114
B.1.1 Health condition background . . . . . . . . . . . . . . . . . 114
B.1.2 Health management . . . . . . . . . . . . . . . . . . . . . . . 115
B.1.3 SNS usage and background . . . . . . . . . . . . . . . . . . 115
B.1.4 HI sharing on SNSs . . . . . . . . . . . . . . . . . . . . . . . 115
B.1.5 A specialized SNSs for managing health conditions . . . 116
B.1.6 Study related feedback . . . . . . . . . . . . . . . . . . . . . 116
B.2 Supplementary results . . . . . . . . . . . . . . . . . . . . . . . . . . 116
C Supplementary Materials for the Confirmatory Study (Online Sur-
vey) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119
C.1 Survey questionnaire . . . . . . . . . . . . . . . . . . . . . . . . . . . 123
C.2 Supplementary results: Online survey . . . . . . . . . . . . . . . . 136
ix

List of Tables
Table 4.1 Participants demographics (N = 166). . . . . . . . . . . . . . . 23
Table 4.2 Reasons for sharing HI online. . . . . . . . . . . . . . . . . . . . 25
Table 4.3 Reasons against sharing HI online. . . . . . . . . . . . . . . . . . 26
Table 5.1 Participants demographics. . . . . . . . . . . . . . . . . . . . . . 39
Table 6.1 Participants demographics (N = 492). . . . . . . . . . . . . . . 61
Table 6.2 PCA results for different personal information items. The
last column represents the percentage of participants who
were likely to hide each information item. . . . . . . . . . . . . 79
Table A.1 HI categories and examples. . . . . . . . . . . . . . . . . . . . . 108
Table B.1 Participants demographics and health conditions. The first
column represents participants’ ID. . . . . . . . . . . . . . . . . 118
Table C.1 Health-related sites used by participants that are not consid-
ered as SNSs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139
x
Table C.2 Positive HI sharing experience. The first two columns repre-
sent the coded category and related sub-categories. The last
two columns represent the total number/percentage of pos-
itive coded events under each category (272 total references).141
Table C.3 Negative HI sharing experience. The first two columns rep-
resent the coded category and related sub-categories. The
last two columns represent the total number/percentage of
negative coded events under each category (86 total refer-
ences). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142
xi
List of Figures
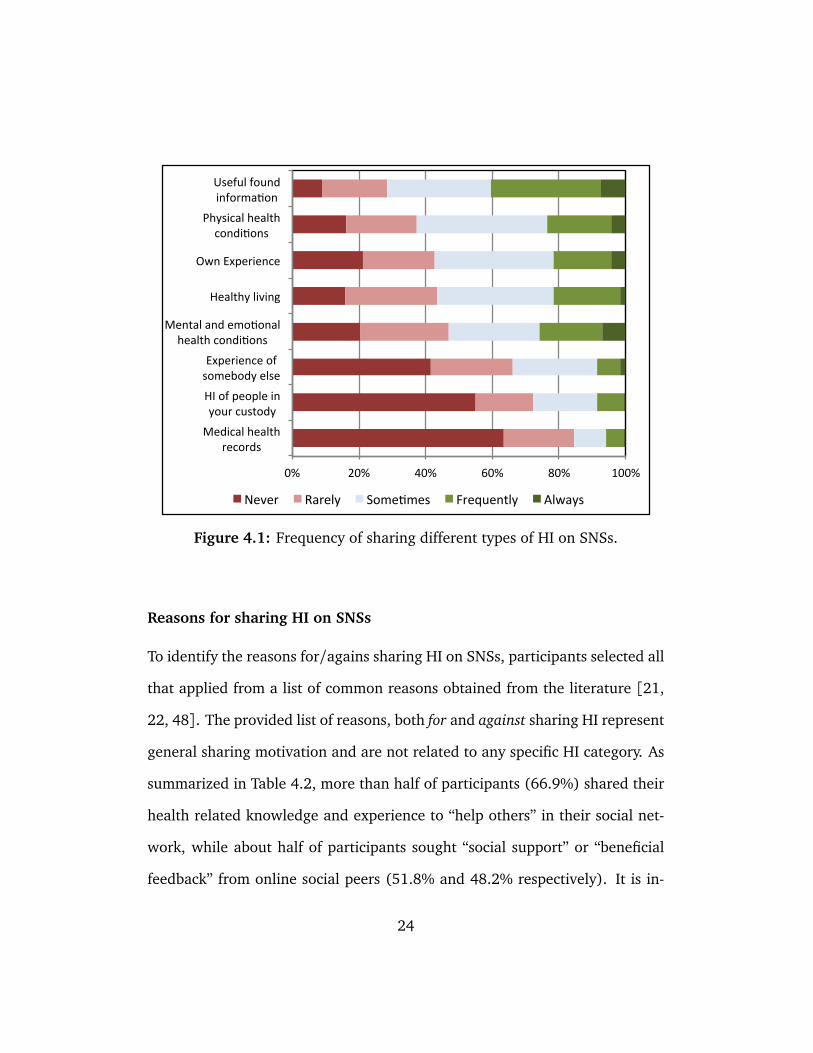
Figure 4.1 Frequency of sharing different types of HI on SNSs. . . . . . 24
Figure 4.2 Factors that might influence participants’ perceived privacy
risks when sharing HI on SNSs. . . . . . . . . . . . . . . . . . . 28
Figure 4.3 Perceived privacy risks when sharing HI with select individuals. 29
Figure 4.4 Perceived privacy risks when sharing HI with select groups. . 30
Figure 4.5 Perceived privacy risks when sharing HI with entire contact
list. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Figure 4.6 Perceived privacy risks when sharing HI with all SNS users. . 31
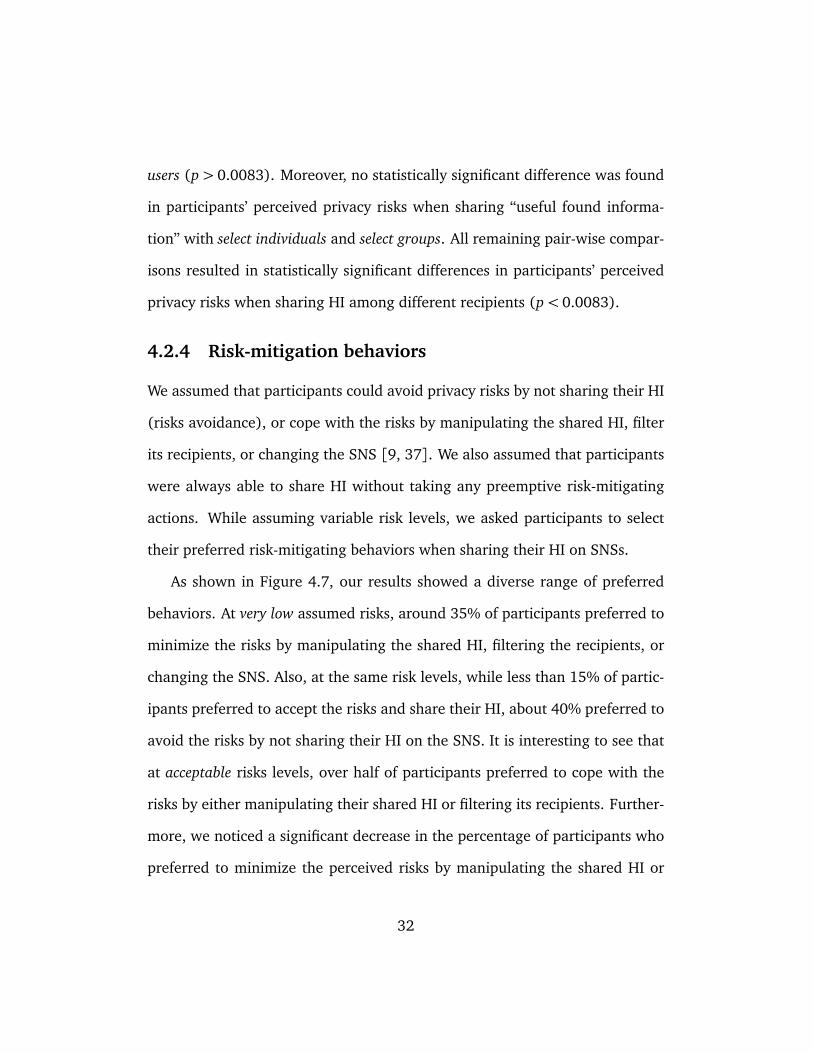
Figure 4.7 Participants’ preferred risk-mitigating behaviors at different
risk levels. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Figure 5.1 Data analysis and theoretical saturation (21 interviews and
123 unique codes). . . . . . . . . . . . . . . . . . . . . . . . . . 40
Figure 6.1 Health conditions cumulative percentage frequency (95%). 63
Figure 6.2 Perceived health status and the number of reported health
conditions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
xii
Figure 6.3 Categorizing participants according to their perceived health
status and the number of health conditions. . . . . . . . . . . 64
Figure 6.4 Attitudes toward privacy (Westin Privacy Index). . . . . . . . 66
Figure 6.5 Percentage of participants who shared details of their HI
with other user groups on Facebook (n= 253). . . . . . . . . 67
Figure 6.6 HI sharing experience evaluation (n= 250). . . . . . . . . . . 68
Figure 6.7 Willingness to disclose HI to different recipients on Facebook. 72
Figure 6.8 Willingness to “search” for specific recipients on Facebook. . 74
Figure 6.9 Willingness to use an “anonymous” identity for sharing HI
on Facebook. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Figure 6.10 Willingness to hide different information pieces when cre-
ating an “anonymous” identity for the purpose of sharing
HI on Facebook. . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
Figure 6.11 Willingness to trust different SNS providers. . . . . . . . . . . 81
Figure C.1 Participants’ age distribution. . . . . . . . . . . . . . . . . . . . 137
Figure C.2 Participants’ employment categories distribution. . . . . . . . 138
xiii

Acknowledgments
First, I would like to thank my kind advisor, Konstantin Beznosov, for patiently
guiding me through this journey. Second, I would like to thank all members
of LERSSE for their feedback and constructive discussions. I am greatly thank-
ful to Yazan Boshmaf, Ildar Muslukhov, Pooya Jaferian, San-Tsai Sun, Hootan
Rashtian, Primal Wijesekera, Ivan Cherapau, and Ahmad Mahfouz. Also, I
would like to thank Hyoungshick Kim and Primal Asanka for their guidance
and feedback during different stages of the research. Third, I would like to
thank NSERC Internetworked Systems Security Network (ISSNet), for their
partial funding and support of the research. Last but not least, I would like to
thank my beloved family, especially my parents, my wife, and all those who
showed endless support and compassion through my journey.
xiv

Dedication
To my beloved parents, my dearwife, and all my family memberswho never stopped supporting me.
xv

Chapter 1
Introduction
Patients with chronic health condition(s) can benefit from sharing their health
information (HI)1 on SNSs in different ways: seeking or providing social
support, learning from the shared experiences, and self-management educa-
tion [43, 48, 56]. Furthermore, sharing HI on SNSs was shown to be ben-
eficial not only to the individuals themselves, but also to their online social
peers. Motivated by the two-way benefits, a variety of web-based services
have been used by patients to share their HI with other people (e.g., Blogs,
emails). Among these services, Facebook, which have attracted the largest
number of active online users, have emerged as a common place for sharing
different types of personal information, including HI [22, 46].
A variety of methodological approaches were used to understand patients’
HI sharing practices and the benefits of sharing HI among different patient
1Any type of information related to the health of an individual including personal healthinformation (PHI), electronic health records (EHRs), and personal health records (PHRs)
1

groups (e.g., breast cancer patients) [43, 48]. Despite the benefits, revealing
HI to other people was always associated with privacy concerns. In addition,
an implicit consensus among people was noted toward the idea that their HI
should be considered as “personal” and “private” information [42, 48]. Be-
sides that, Facebook was shown to be vulnerable toward different attacks,
resulting in unintended information disclosure, privacy invasion, and medical
data misuse [10, 25, 55]. One can argue that the general attitude toward
disclosing HI on Facebook might be influenced by the perceived privacy risks
and the gained benefits (privacy calculus) [40]. Moreover, while a number
of studies brought attention to the benefits and the privacy concerns related
to HI sharing on Facebook, there has been little done to understand the main
factors that influence patients’ motivation to engage in effective HI sharing
on Facebook [39, 43, 44]. In addition, given that existing SNSs’ security and
privacy features were not designed to support patients’ privacy requirements
while sharing HI on SNSs, it is important to design new features that enable
patients to communicate their HI effectively and without any concerns. This,
however, demands building a better understanding of patients’ practices and
preferences when sharing HI on SNSs.
In this study, we bridge the knowledge gap by answering the general re-
search questions: Why, how, and with whom patients share their HI on Face-
book? Following a series of qualitative and quantitative studies, we explored
Facebook users’ HI sharing practices and risk perceptions. We started by con-
ducting a preliminary online survey to collect quantitative data from a broad
2

number of active Facebook users. The survey aimed at corroborating prior
findings while removing the uncertainties that were caused by the limited
related work. After that, we adopted a grounded theory approach to inter-
view individuals with chronic health conditions [12]. We focused on exploring
users’ practices, preferences, and risk perceptions when sharing HI on SNSs.
The interviews helped us in developing a better understanding of the reason-
ing behind patients’ behaviors and privacy perceptions, while identifying the
key factors that influenced patients’ motivation to share HI on SNSs. We con-
ducted an online survey in order to confirm and extend upon our findings. The
online survey provided the opportunity to recruit a more representative sam-
ple of Facebook users. Moreover, analyzing the quantitative data resulted gen-
eralizable findings that characterized the main factors that influenced users’
motivation to share HI.
The results showed that participants who previously shared their HI on
Facebook, especially those who gained some benefits, were more willing to
share their HI. On the other hand, despite the perceived benefits, participants
who had strong privacy concerns (privacy Fundamentalists) were always un-
likely to share their HI, as compared to others who showed more flexibility in
the presence of different motivating factors (privacy Pragmatists and Uncon-
cerned). Along with the aforementioned factors, we also showed how partici-
pants’ perceived health status could influence their motivation toward sharing
HI with other social peers, especially strangers. Furthermore, we showed that
the recipients of the shared HI, and the type of the shared HI, could also play
3
a major role in motivating participants toward sharing their HI. Other than
the factors that influenced HI sharing motivation, our results highlighted a
number of features that could motivate users toward engaging in effective HI
sharing on Favebook (e.g., anonymous identity, search and recommendation
features). Armed with such an understanding, new privacy-preserving fea-
tures could be developed that might be more effective in practice. Ultimately,
while optimizing the gained benefits, these features would improve Facebook’s
privacy and make it less vulnerable toward privacy threats.
The rest of the thesis is structured as following: we summarized back-
ground and related work in Chapter 2. We presented the overall methodology
in Chapter 3. Details of the conducted user studies are presented in Chap-
ters 4, 5, and 6 respectively. The main findings of the research were discussed
in Chapter 7. Finally, we concluded the thesis by presenting conclusions and
future work (Chapters 8 and 9).
4

Chapter 2
Background and Related Work
2.1 Social networking sites (SNSs)
Social networking sites (SNSs) are web-based services that allow their users
to create visible profiles within the site, maintain connections with a list of
online users (including strangers), and interact with other users through the
created connections [8]. SNSs are classified as Web 2.0 sites that incorporate
strong social components (e.g., maintaining friends lists), and encourage shar-
ing user-generated contents (e.g., photos, comments) [15]. While a variety of
additional services are provided by different SNSs (e.g., online gaming), they
are mainly used to facilitate maintaining social relationships. Also, SNSs pro-
vide their users with the opportunity to establish new relationships with others
who share common interests or background [39]. It is important to recognize
that a number of web-based services might also incorporate properties similar
5
to SNSs, where they allow limited profile creation and collaborative communi-
cations among members of the site (e.g., blogs, discussion forums). However,
despite the similarities in terms of the implementation of social components,
there has been uncertainty about classifying these online services as SNSs due
to the adopted user interface technology and architecture [8, 15].
2.2 Sharing HI on SNSs
SNSs have been developed and used for a variety of purposes, including but
not limited to: socializing and content sharing (e.g., Facebook, Twitter), net-
working and maintaining professional profiles (e.g., LinkedIn), and peer-to-
peer communication (e.g., Skype). The highly inter-connected nature of ex-
isting SNSs, and the increasing number of users have encouraged people to
actively engage in sharing different types of information on SNSs. Several
studies have indicated that HI sharing is becoming a leading habit among a
considerable number of SNSs users [22, 41, 49]. The results of the Pew In-
ternet survey [21] indicate that a considerable number internet users in the
US went online to follow their friends’ personal health experience, with a no-
ticeable increase when compared to the previous reports. Meanwhile, 16% of
the surveyed participants reported going online to find others who had sim-
ilar health concerns [22]. Moreover, people with health concerns have been
shown to visit their SNSs to seek support from other online peers [46].
Despite their practices, users’ motivation to share HI on SNSs was shown
to be influenced by a number of factors:
6

2.2.1 Perceived benefits
The benefits of using SNSs for HI sharing has been discussed in a number of
studies [42, 43, 56]. Lederman et al. [38] discussed the benefits of addressing
socio-technical needs by utilizing SNSs and developing engaging therapeutic
solutions for mentally ill patients. Following a user-centered design approach,
Skeels [48] captured breast cancer patients’ HI sharing requirements and de-
signed an online interactive technology to facilitate HI sharing and manage-
ment. Kamal [30] also used a similar approach to design a SNS prototype
for promoting healthy behavior changes. Despite the reported benefits for
patients, literature reviews showed that only a small number of studies have
focused on the effects of using SNSs on patients’ health management. For in-
stance, Merolli et al. [43] reviewed the literature and found that among all the
identified studies (N=19), only five studies focused on SNSs (classified as web
2.0 sites). For them, this was a clear indication that research on SNSs usage in
chronic disease management was still in its early stage. Moreover, Moorhead
et al. [44] surveyed primary research and identified the lack of information
about the uses, benefits, and limitations of social media for health communi-
cation among the general public, patients, and health professionals. Similar
conclusions were also drawn by Lefebvre and Bornkessel [39]. Furthermore,
they suggested addressing a number of general research questions in order to
better understand how SNSs can be effectively and efficiently used to improve
health across the population.
7

2.2.2 Perceived health status
Patients’ motivation to engage in protective health behaviors was shown to be
influenced by the severity and the likelihood of their health conditions [52]. In
the context of HI sharing on SNSs, a number of studies have shown that people
who suffered from chronic health conditions were likely to visit SNSs to seek
or share their HI with other social peers [21, 46]. There are different ways
to asses one’s overall health status and the severity of the health conditions.
The self-reported perceived health status was used as a reliable measurement
of patients’ overall health status in a number of studies [28, 54]. Also, they
found a correlation between the perceived health status and the number of
health conditions, with patients who had “poor” health to have more health
conditions. Nevertheless, the subjective assessment of the health conditions
might not always accurately describe the overall health status. For instance,
one might suffer from a number of severe health conditions and yet consider
his health to be stable or good, while another person might have a minor
health issue and feels completely devastated by his health issues.
2.2.3 Perceived privacy
The nature of SNSs can lead to the diffusion of personal information beyond
its intended targets, while resulting in the lack of subsequent control over
its exposure [10, 27, 44]. In general, information revelation in SNSs was
shown to be influenced by the raised privacy concerns due to both the per-
sonal experiences and the negative reports in the media [55]. In the context
8
of SNSs, privacy concerns have been always associated with sharing HI among
users [16, 51]. A survey of 1060 US adults found that 63% raised concerns
related to publicly sharing their HI on SNSs, while 57% were concerned that
their HI might be hacked or leaked from the SNSs [3]. Morris et al. [45]
surveyed different types of questions that SNSs users asked their social peers
about and found that “health” was a type of topic that people tend to consider
too personal. Moreover, SNSs were considered as inappropriate places for dis-
cussing overly personal information such as information related to individual’s
health [16, 45].
It has been shown that internet users’ privacy concerns and their attitudes
toward privacy could highly influence their motivation to disclose personal
information to online sites [11, 16, 49]. The Westin privacy index was intro-
duced as a way to meaningfully classify internet users based on their attitudes
toward privacy and their motivations to disclose personal information on the
internet [33]. According to the Westin privacy index, internet users could be
divided into three groups: (1) Privacy Fundamentalists, who highly value pri-
vacy and feel very strongly about it; (2) Privacy Pragmatists, who have strong
feelings about privacy but can also see the benefits from surrendering some
privacy in situations where they believe they can prevent the misuse of their
information; and (3) Privacy Unconcerned, who have no real concerns about
privacy or about how other people and organizations use their information.
A number of studies showed that the Westin privacy index could be used as a
reasonable indicator of internet users’ attitudes toward privacy and their moti-
9

vation to disclose personal information online [11, 14, 33, 34]. Nevertheless,
Woodruff et al. [53] argued that the prescribed classification of internet users
using the Westin privacy index might not always correlate with their motiva-
tion to disclosure information online. Despite their argument, we found that
the literature provides sufficient evidence to reflect on the overall correlations
between internet users’ privacy attitudes and their motivation to disclose per-
sonal information online.
10

Chapter 3
Methodology
The research was conducted following a three steps methodology: (1) a broad
survey of active SNS users HI sharing practices and risk perceptions in order to
corroborate prior findings and identify important research directions; (2) in-
depth interviews to explore patients’ motivation to share HI on SNSs; and (3)
a confirmatory survey in order to test our previous findings and identify the
main factors that influenced HI sharing motivations on SNSs. In what follows,
we provide more details about the methodology used for each conducted user
study:
3.1 Preliminary study: privacy perceptions andrisk-mitigating behaviors
The goal of the initial study was to address the uncertainties with respect to
findings from literature (Chapter 4). In early stages of this research, we ex-
11

plored SNS users’ privacy perceptions and risk-mitigating behaviors. To the
best of our knowledge, previous studies were either limited to niche demo-
graphics (e.g., teenage patients, elderly patients, mothers with children in
custody) [26, 47, 48, 51], or focused on non-SNS users [19, 22, 42, 56]. In
addition, while the literature on “information sharing security and privacy”
was quite rich in content, it lacked the quantitative data on active SNS users’
practices and privacy perceptions when sharing HI on SNSs. Therefore, build-
ing upon the partial knowledge gained from literature, we employed an online
survey as the first step toward exploring HI sharing practices and risk percep-
tions. We used the online survey to quantify HI sharing practices and risk
perceptions. Furthermore, the online survey was used to corroborate prior
findings by reaching a broad number of active SNS users, while highlighting
important research directions.
3.2 Exploratory study: interviews
In an effort to develop a better understanding of users’ motivation to share
HI on SNSs, 21 chronically ill patients were interviewed about their moti-
vation to share HI on SNSs (Chapter 5). Following a qualitative approach,
we explored participants’ HI sharing practices, perceptions, and preferences.
Our main objective was to understand how patients, who were also active
SNSs users, shared instances of their HI with other peers on SNSs. We used
a grounded theory approach to guide our sampling, data collection, and data
analysis [12]. The grounded theory approach was adopted in order to avoid
12

any prejudices, presuppositions or previous knowledge of the subject area, that
is, we concentrate on finding new information, ideas and themes in the data
we collect. Our investigation started with semi-structured interviews, with the
flexibility to add new questions during the interviews when new and interest-
ing inputs were captured. The iterative data collection and analysis procedure
helped us in developing a deep understanding of patients’ perceived privacy
risks while identifying the main factors that influenced their motivation to
share HI on SNSs.
3.3 Confirmatory study: online survey
Following our exploratory interviews, we conducted a confirmatory study in
a form of online survey. The online survey consisted of a mixture of close-
and open-ended questions, where the questionnaire was designed to collect
data for the purpose of testing prior findings along with investigating new
insights on HI sharing motivation on SNSs. The goal of the online survey
was to provide quantitative data from a representative sample of SNS users
in order to confirm and extend our findings from the exploratory study. The
quantitative data was used to describe SNS users’ practices, perceptions and
motivations. The data was also used to perform inferential statistical analysis
that helped in identifying the main factors that influenced users’ motivation to
share HI on SNSs. Further details on sampling, data collection, and analysis is
presented in Chapter 6.
13

3.4 Limitations
While individual interviews can lead to better understanding of user behav-
ior, they have few limitations. First, the interview results are limited by par-
ticipants’ prior experiences. Second, participants might indicate behavioral
preferences that they may not necessarily practice in real life [6]. Third, inter-
views are hard to scale in terms of the number of participants, and therefore,
their findings are not generalizable. Finally, the interview results might be
influenced by the interviewer biases [29]. To overcome the limitations, we
restricted the participation to patients who were also active SNSs users, with
at least one SNS account that they used regularly. To minimize the second
limitation, we tried to infer privacy preferences from participants’ previous HI
sharing practices. To address generalizability, we conducted a followup survey
to confirm our findings from the interview study. Finally, to avoid imposing
biases on the responses of participants, we asked open-ended questions and
tried to probe the participants to tell their story from their own perspectives.
The main limitation of the online survey was in the self-reported nature
of the data, which was hard to validate without violating participants’ pri-
vacy. For instance, participants reported a number of health conditions that
were difficult to confirm in real life. Therefore, we used the self-reported data
as our ground truth throughout the study. Nevertheless, to minimize threats
to validity, the survey questionnaire and responses were reviewed and tested
prior to conducting the study. Whenever necessary, the survey questionnaire
14

was modified by incorporating participants’ comments and feedback in order
to ensure unique understanding and avoid confusion. Finally, a crowdsourc-
ing tool (MTurk) was used to reach a broad range of participants and recruit
a representative sample of SNS users.
3.5 Ethical considerations
This work consisted of two online surveys and an interview study. All stud-
ies were reviewed by the University of British Columbia’s Behavioural Re-
search Ethic Board (BREB). The study related materials are available in Ap-
pendices A–C. We minimized risk to participants by excluding any personally
identifiable information from the collected data, generated results, and pub-
lished reports. Participation in all studies were completely voluntarily, and
participants were able to withdraw from the study at anytime.
For the online surveys, we used Amazon Mechanical Turk (MTurk) to re-
cruit participants. For each survey, we posted a task on MTurk that contained
a link to the survey website, where participants reviewed the study descrip-
tion and policies before consenting to participate in the study (Appendix A
and C). To guarantee compensation by MTurk, participants were required to
prove survey submission by entering a unique 7-digit alpha-numeric code that
was assigned to them upon survey completion.
For the interview study, participants were recruited through media ad-
vertisements. An informed consent was obtained prior to interviewing each
participant in order to ensure complete awareness about the nature of the
15
study and the collected data (Appendix B). All recorded media, transcripts,
and consent forms were identified by codes. To ensure complete anonymity,
pseudonyms (false names) were substituted for participants’ real names and
the names of anyone else mentioned during the interviews. Furthermore, the
investigators and the transcriptionists were the only people that were allowed
to hear the recorded interviews and/or see the transcripts.
16

Chapter 4
Preliminary Study: Privacy
Perceptions and Risk-Mitigating
Behaviors
By employing an online survey on a broad number of active SNS users, we
aimed at confirming our partial knowledge on HI sharing practices and risk
perceptions. We also aimed at identifying important research directions by
exploring several broad aspects of HI sharing on SNSs.
4.1 Methodology
We surveyed active SNS users’ HI sharing practices and privacy perceptions.
The online survey gave us the opportunity to reach a broad range of active
SNS users. By answering the following research questions (RQs), we aimed at
17

providing descriptive statistics that quantify HI sharing practices while high-
lighting users’ privacy concerns and risk-mitigating behaviors:
RQ1. What types of HI is being shared on existing SNSs?
RQ2. What are the main reasons for/against sharing HI on SNSs?
RQ3. How does SNS user’s risk perceptions changes when sharing different
types of HI with various SNS users?
RQ4. What are the preferred risk-mitigating behaviors that SNS users
would adopt when sharing HI on SNSs?
4.1.1 Participant recruitment
We recruited Amazon MTurk [2] workers through CrowdFlower [1], a crowd-
sourcing website that provides different labour channels. MTurk workers, who
were shown to be more educated and younger than the general population,
can be considered as a reliable source of high-quality data for research involv-
ing human-subjects [50]. We recruited “trusted” MTurk workers, who were
identified by CrowdFlower according to different factors (e.g., their prior com-
pleted jobs and reported activities). The posted recruitment ad title did not
mention privacy, while in the instructions, participants were requested to com-
plete an online survey about their HI sharing practices, perceived privacy risks,
and corresponding behavioral responses (Apppendix A). The survey was de-
signed to take less than 30 minutes to be completed. Participants were also
compensated with $1 (US) through CrowdFlower for successfully completing
the job.
18

4.1.2 Data collection
On April 4th, 2013, 191 participants successfully completed the survey. The
constructed online survey was administered on Enterprise Feedback Manage-
ment (EFM), which is a Canadian-hosted survey solution complying with the
Freedom of Information and Protection of Privacy Act of British Columbia.1
Out of the all participants, two did not consent to the study, and therefore
were removed from further analysis. The majority of participants were from
the US (87.8%), followed by India (9.5%). We also received a single submis-
sion from participants residing in each of the following countries: Australia,
Philippines, Romania, Canada, and UK. We decided to minimize the effect of
cultural differences in our analysis by discarding submissions made by partic-
ipants residing outside of the US [5]. The remaining 166 submissions were
included in further analysis throughout the study.
4.1.3 Survey items
The survey questionnaire consisted of the following sections (Appendix A.1):
SNS usage
We asked participants about the total number of active SNS accounts they
maintained, and, for each active SNS account, we asked the following: (i)
name of the SNS; (2) how often the SNS account was used; and (3) the pre-
ferred device for connecting to that SNS account (e.g., smartphone, laptop,
1This enterprise-level survey tool represents a comparable alternative to the US-based Sur-vey Monkey.
19

tablet).
HI sharing practices
As shown in Appendix A.2, we grouped different HI examples found in the
literature into eight HI categories [21, 22, 48]. For each category, we asked
participants to rate the likelihood of sharing information from never to always
on a 5-point Likert scale. We also asked participants to specify all reasons
for/against sharing HI by selecting all that applied from a list of given reasons.
Perceived privacy risks
We identified several factors that influenced the perceived privacy risks (HI
recipients, HI category, used SNSs, and current health conditions). We asked
participants to identify how much each factor contributed to their perceived
privacy risks by rating their responses on a 5-point Likert scale from does not
affect at all to strongly affects. We also asked participants to rate their per-
ceived privacy risks when sharing different HI with the following users: select
individuals, select groups, entire contacts, and all other SNS users (responses
varied on a 5-point Likert scale from very low or no risks to extreme risks).
Risk-mitigating behaviors
In a hypothetical situation, we asked participants to indicate their preferred
risk-mitigating behavior(s) when sharing HI on SNSs at different assumed pri-
vacy risk levels (very low or no risks–extreme risks). Participants selected their
preferred risk-mitigating behaviors from a given list of options (Appendix A.1).
20

4.2 Results
4.2.1 Participant demographics and SNS usage
A total of 166 participants successfully completed the survey. Participants rep-
resented SNS users from 39 different states. Submissions were made by an
equal number of male (49.4%) and female (50.6%) participants, with an age
range of 19–70 years old (mean= 30.4, σ= 10). A summary of participants
age ranges, completed education, and employment categories is presented in
Table 4.1. About 39% of all participants indicated having only one active SNS
account, while 35.5% indicated using two SNSs. The remaining participants
indicated using 3 or more SNSs on regular basis. A total of 140 participants
indicated using their SNS account(s) on daily basis, among which the majority
(96.4%) were active Facebook users.
4.2.2 HI sharing practices
To investigate HI sharing practices, we categorized different examples of HI
that people often shared online into eight HI categories (refer to Appendix A.2
for further details). We asked participants to indicate on a 5-point Likert
scale how regularly they shared information from each HI category. As shown
in Figure 4.1, about 85% of participants never or rarely shared information
about their medical health records on SNSs (e.g., x-rays, treatments, name
and address, insurance policy number). Slightly above 70% of participants
never/rarely shared HI of people in their custody (e.g., children and elderly
21

parents), while about 65% of participants never/rarely shared other people’s
health related experience. Among all participants, only 7 participants never
shared any types of HI on SNSs, while the vast majority of participants (about
96%) indicated sharing different types of HI on their SNSs. On the other
hand, about 40% of participants frequently or always shared useful found in-
formation on SNSs (Figure 4.1). Furthermore, while about 25% of partici-
pants frequently/always shared information related to their mental and emo-
tional health conditions, slightly less than 25% of participants frequently/al-
ways shared information related to their physical health conditions. About
22% of participants frequently/always shared information related to their “own
experiences” and “health living” categories. Finally, less than 10% of partici-
pants reported frequently/always sharing information related to “experience of
somebody else”, “HI of people in their custody”, or “medical health records”.
22

Table 4.1: Participants demographics (N = 166).
Demographic Category Count (%)
Gender Female 84 50.6
Male 82 49.4
Age range 19–29 90 59.0
(19–70) 30–39 41 24.7
40–49 14 8.4
50+ 13 7.8
Completed Undergraduate University (Bachelor’s) 66 39.8
Education Some college/university courses 11 6.6
Graduate University (Masters’s/PhD) 17 10.2
High School 42 25.3
Diploma (post-secondary courses) 21 12.7
Other 9 5.4
Employment Education/Academic 17 10.2
Categories IT/Computer 16 9.6
(Top 5) Medical/Health 14 8.4
Sales (e.g., retail, wholesale) 13 7.8
Banking/Financial 11 6.6
23
0% 20% 40% 60% 80% 100%
Medical health records
HI of people in your custody
Experience of somebody else
Mental and emo@onal health condi@ons
Healthy living
Own Experience
Physical health condi@ons
Useful found informa@on
Never Rarely Some@mes Frequently Always
Figure 4.1: Frequency of sharing different types of HI on SNSs.
Reasons for sharing HI on SNSs
To identify the reasons for/agains sharing HI on SNSs, participants selected all
that applied from a list of common reasons obtained from the literature [21,
22, 48]. The provided list of reasons, both for and against sharing HI represent
general sharing motivation and are not related to any specific HI category. As
summarized in Table 4.2, more than half of participants (66.9%) shared their
health related knowledge and experience to “help others” in their social net-
work, while about half of participants sought “social support” or “beneficial
feedback” from online social peers (51.8% and 48.2% respectively). It is in-
24

teresting to see that about 44% of participants shared their HI on SNSs in
order to initiate online interactions and discussions, while about 38% of par-
ticipants used it as a way to alleviate their anxiety or promote healthy living
(Tables 4.2).
Table 4.2: Reasons for sharing HI online.
Reasons for sharing HI Participants (%)
Help others by sharing personal experience and knowl-
edge66.9
Seek help or social support 51.8
Get benefits by receiving useful feedback from online
contacts48.2
Seek online interactions and make discussions 44.0
Alleviate anxiety 38.6
Promote healthy living 37.3
Other reasons 6.6
Reasons against sharing HI on SNSs
On the other hand, for the HI that participants did not share on their SNSs, ap-
proximately half of them (49.4%) indicated not sharing HI due to the existence
of different people among their SNS contacts (Table 4.3). In addition, 43.4%
of all participants considered their HI to be “personal” and did not want to
share it with anyone on their SNSs. About 40% of participants avoided shar-
ing their HI on SNSs because they did not want to be treated as “the sick”
person by their online peers. Moreover, about 35% of participants did not
25
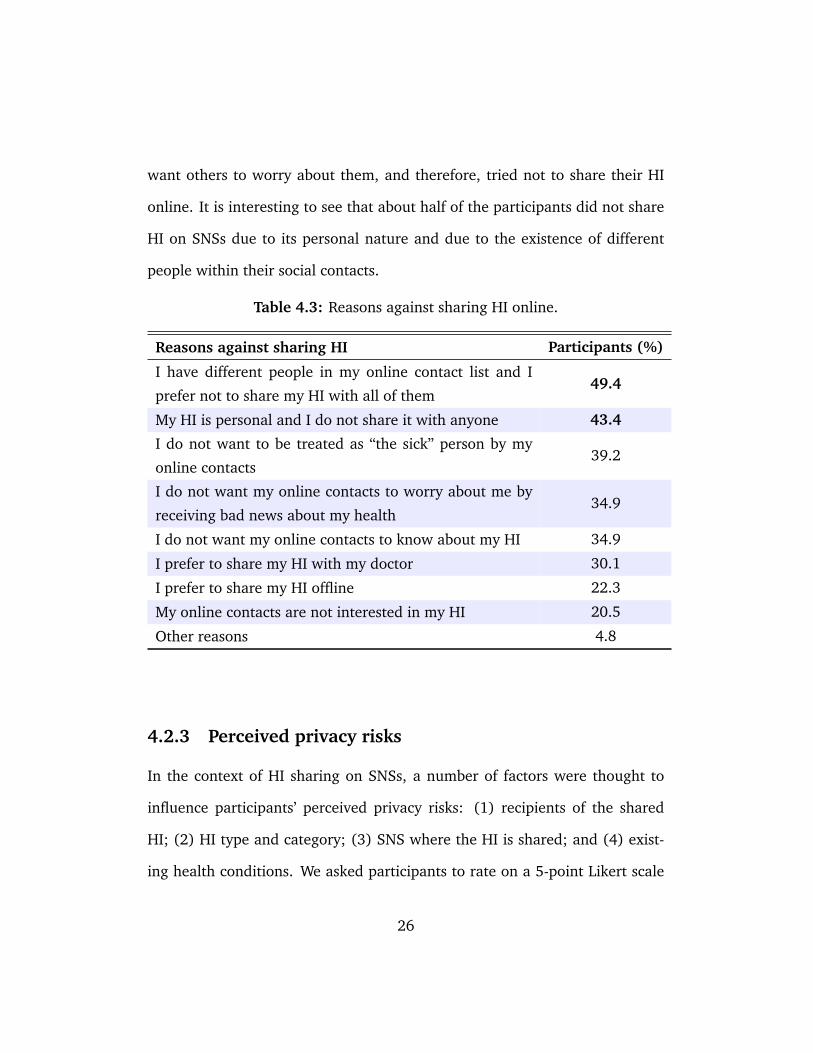
want others to worry about them, and therefore, tried not to share their HI
online. It is interesting to see that about half of the participants did not share
HI on SNSs due to its personal nature and due to the existence of different
people within their social contacts.
Table 4.3: Reasons against sharing HI online.
Reasons against sharing HI Participants (%)
I have different people in my online contact list and I
prefer not to share my HI with all of them49.4
My HI is personal and I do not share it with anyone 43.4
I do not want to be treated as “the sick” person by my
online contacts39.2
I do not want my online contacts to worry about me by
receiving bad news about my health34.9
I do not want my online contacts to know about my HI 34.9
I prefer to share my HI with my doctor 30.1
I prefer to share my HI offline 22.3
My online contacts are not interested in my HI 20.5
Other reasons 4.8
4.2.3 Perceived privacy risks
In the context of HI sharing on SNSs, a number of factors were thought to
influence participants’ perceived privacy risks: (1) recipients of the shared
HI; (2) HI type and category; (3) SNS where the HI is shared; and (4) exist-
ing health conditions. We asked participants to rate on a 5-point Likert scale
26

how much each of the above four factors would affect their perceived privacy
risks (responses varied between does not affect to strongly affect). As shown in
Figure 4.2, only a small number of participants indicated that the “recipients
of the shared HI” and the “HI type/category” does not affect their perceived
privacy risks (< 7%). Relatively more number of participants (about 13%)
indicated that their “existing health conditions” and/or the “SNS where the
HI is shared” do not affect their perceived privacy risks. On the other hand,
about 60% of participants indicated that the shared “HI type/category” would
somewhat or strongly affect their perceived privacy risks (Figure 4.2). Approx-
imately 55% of participants considered the “recipients of the shared HI” to
be somewhat or strongly affecting their perceived privacy risks. Furthermore,
about 43% of all participants indicated that their “existing health conditions”
and/or the “SNS where they share their HI on” would somewhat or strongly
affect their perceived privacy risks.
27

0% 20% 40% 60% 80% 100%
The recipients of the shared HI
HI type and category
The SNS where the HI is shared
Exis@ng health condi@ons
Does not affect Might affect Slightly affect Somewhat affect Strongly affect
Figure 4.2: Factors that might influence participants’ perceived privacyrisks when sharing HI on SNSs.
We also asked participants to rate their perceived privacy risks on a 5-point
Likert scale (with responses varying from very low or no risk to extreme risk),
when sharing different types of HI with the following user groups on SNSs:
select individual(s); select group(s); entire contact list; and all SNS users. As
shown in Figure 4.3, the majority of participants (about 95%) reported having
very low or acceptable privacy concerns when sharing information related to
“healthy living” or “useful found information” with select individuals. About
85% reported very low or acceptable concerns when sharing information re-
lated to their “physical health conditions” and/or their “own experiences” with
select individuals. Furthermore, while between 65% to 75% of participants
had no concerns with sharing “experience of somebody else” or their “men-
tal/emotional health conditions” with select individuals, slightly over half of
28
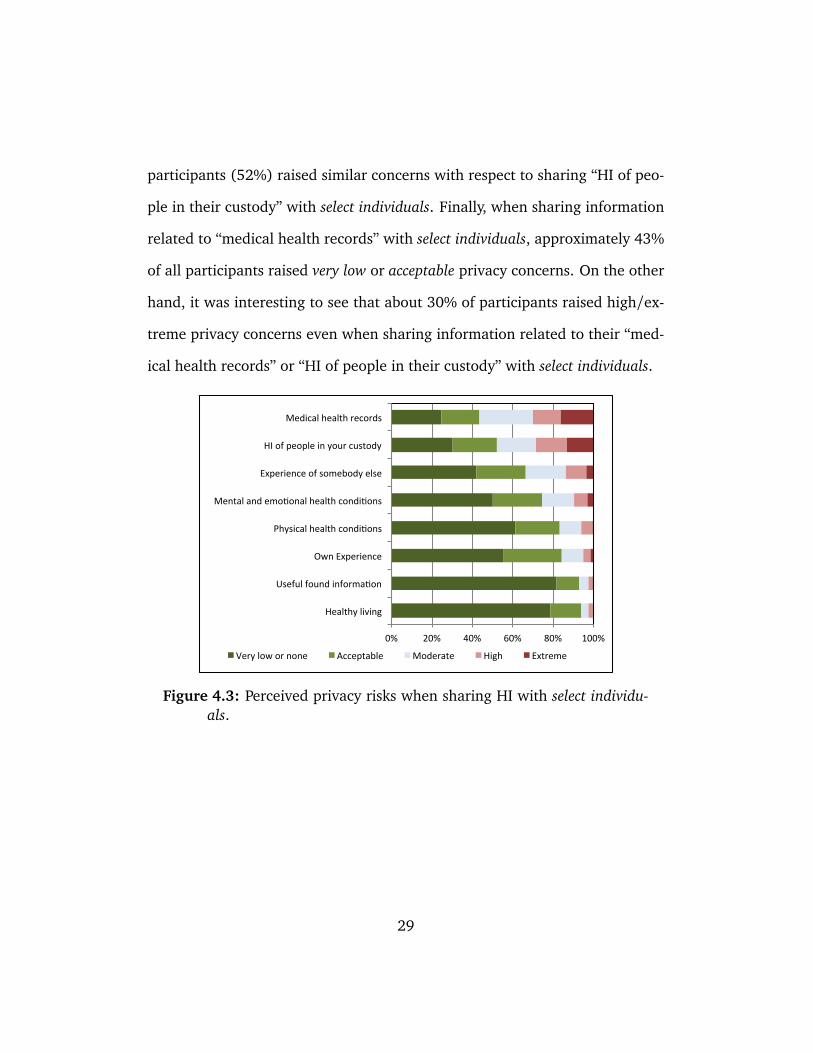
participants (52%) raised similar concerns with respect to sharing “HI of peo-
ple in their custody” with select individuals. Finally, when sharing information
related to “medical health records” with select individuals, approximately 43%
of all participants raised very low or acceptable privacy concerns. On the other
hand, it was interesting to see that about 30% of participants raised high/ex-
treme privacy concerns even when sharing information related to their “med-
ical health records” or “HI of people in their custody” with select individuals.
0% 20% 40% 60% 80% 100%
Healthy living
Useful found informa<on
Own Experience
Physical health condi<ons
Mental and emo<onal health condi<ons
Experience of somebody else
HI of people in your custody
Medical health records
Very low or none Acceptable Moderate High Extreme
Figure 4.3: Perceived privacy risks when sharing HI with select individu-als.
29

0% 20% 40% 60% 80% 100%
Healthy living
Useful found informa<on
Own Experience
Physical health condi<ons
Mental and emo<onal health condi<ons
Experience of somebody else
HI of people in your custody
Medical health records
Very low or none Acceptable Moderate High Extreme
Figure 4.4: Perceived privacy risks when sharing HI with select groups.
0% 20% 40% 60% 80% 100%
Useful found informa6on
Healthy living
Physical health condi6ons
Own Experience
Mental and emo6onal health condi6ons
Experience of somebody else
HI of people in your custody
Medical health records
Very low or none Acceptable Moderate High Extreme
Figure 4.5: Perceived privacy risks when sharing HI with entire contactlist.
30

0% 20% 40% 60% 80% 100%
Useful found informa6on
Healthy living
Physical health condi6ons
Own Experience
Mental and emo6onal health condi6ons
Experience of somebody else
HI of people in your custody
Medical health records
Very low or none Acceptable Moderate High Extreme
Figure 4.6: Perceived privacy risks when sharing HI with all SNS users.
As shown in Figures 4.3 to 4.6, the percentage of participants who raised
high/extreme privacy concerns when sharing different types of HI increased
while expanding the number of recipients from select individuals to all SNS
users. Furthermore, when sharing HI with different user groups, “medical
health records” and “HI of people in custody”, resulted the highest privacy
concerns as compared to other HI categories. To find out if there was sig-
nificant differences in participants’ perceived privacy risks when sharing HI
with different user groups, we performed Friedman rank sum tests followed
by a series of post-hoc Wilcoxon tests over all participants’ responses (with
Bonferroni adjustment). For “healthy living” and “useful found information”
categories, we did not find statistically significant differences in participants’
perceived privacy risks when sharing HI among entire contact list and all SNS
31
users (p> 0.0083). Moreover, no statistically significant difference was found
in participants’ perceived privacy risks when sharing “useful found informa-
tion” with select individuals and select groups. All remaining pair-wise compar-
isons resulted in statistically significant differences in participants’ perceived
privacy risks when sharing HI among different recipients (p< 0.0083).
4.2.4 Risk-mitigation behaviors
We assumed that participants could avoid privacy risks by not sharing their HI
(risks avoidance), or cope with the risks by manipulating the shared HI, filter
its recipients, or changing the SNS [9, 37]. We also assumed that participants
were always able to share HI without taking any preemptive risk-mitigating
actions. While assuming variable risk levels, we asked participants to select
their preferred risk-mitigating behaviors when sharing their HI on SNSs.
As shown in Figure 4.7, our results showed a diverse range of preferred
behaviors. At very low assumed risks, around 35% of participants preferred to
minimize the risks by manipulating the shared HI, filtering the recipients, or
changing the SNS. Also, at the same risk levels, while less than 15% of partic-
ipants preferred to accept the risks and share their HI, about 40% preferred to
avoid the risks by not sharing their HI on the SNS. It is interesting to see that
at acceptable risks levels, over half of participants preferred to cope with the
risks by either manipulating their shared HI or filtering its recipients. Further-
more, we noticed a significant decrease in the percentage of participants who
preferred to minimize the perceived risks by manipulating the shared HI or
32

filtering its recipients at higher risk levels. On the other hand, while the per-
ceived risk levels increased, we noticed a significant increase in the number of
participants who preferred not to share their HI on SNS, with about 58% of
participants choosing not to share HI at extreme risk levels (Figure 4.7).
0%
10%
20%
30%
40%
50%
60%
Minimize risks by manipula9ng the shared HI
Minimize risks by filtering the recipients
Minimize risks by changing the
SNS
Accept risks and share HI
Avoid risks by not sharing HI
Percen
tage of p
ar9cipants
Very low or none Acceptable Moderate High Extreme
Figure 4.7: Participants’ preferred risk-mitigating behaviors at differentrisk levels.
4.2.5 Results summary
We constructed an online survey to investigate existing practices of sharing HI
on SNSs. We recruited 166 active SNS users through Amazon Mechanical Turk
(MTurk) [2]. We explored users’ privacy risks perceptions and risk-mitigating
behaviors. Our results indicated that the majority of participants (95.8%)
33

shared some HI on SNSs. Reasons for sharing varied with “helping others”
and “seeking help and social support” identified as the top reasons (66.9%
and 51.8% respectively). On the other hand, about half of the participants
(49%) preferred not to share their HI because of they had different people
among their SNS contacts, whom they did not want to share their HI with.
In addition, the majority of participants (about 93%) considered the HI type
and its recipients to be the most significant factors influencing their perceived
privacy risks. Finally, our results indicated that participants perceived lower
privacy risks when sharing HI with select individuals or select groups, while
their risk perceptions increased with the expansion of the receiver base to
include entire contacts and all SNS users respectively.
4.3 Discussion
Our results contribute to better understanding of HI practices in SNS, per-
ceived privacy risks, and preferred risk-mitigating behavior. We found that
most active SNS users (about 96%), who indicated using their SNS account(s)
on a daily basis, had shared some HI in the past. The influence of “infor-
mation recipient” and “HI type and category” factors were clearly observed
in increasing participants’ perceived privacy risks when sharing HI on SNSs
(Section 4.2.3). As shown in Figures 4.3–4.6, for almost all HI categories, the
perceived privacy risks of sharing HI on SNSs increased toward higher risk
levels, with respect to the expansion of the recipient base. In addition, when
sharing “healthy living” and “useful found information” categories with differ-
34

ent user groups, the results showed less granularity in participants’ perceived
privacy risks. Therefore, while different recipient groups influenced partici-
pants’ perceived privacy risks, the type of the shared HI was also shown to be
influential in determining participants’ perceived privacy risks.
Medical health records may include personally identifiable information
along with information that is directly related to an individual’s health, and
therefore, participants’ concerns regarding sharing such information was justi-
fiable. However, “HI of people in custody” had received considerable attention
from participants as well. We believe that people handle HI of other individu-
als in their custody with extra care and with a sense of responsibility toward
protecting them against privacy threats. Moreover, the category “HI of peo-
ple in custody” represents an abstract view of all HI related to a person in
custody, including their medical health records. Therefore, participants might
have considered an overall risk perception with respect to the most sensitive
HI categories, such as medical records of people in their custody, and as a
result, indicated high privacy concerns when sharing such HI.
We explored participants’ preferred risk-mitigating behaviors at different
risk levels. We found that even at extreme risk levels, about 41% of the partic-
ipants shared HI, while minimizing risks using different techniques (manipu-
late shared HI, filter recipients, and change the SNS). Furthermore, at accept-
able risk levels, more than half of participants preferred to mitigate privacy
risks by manipulating and filtering shared HI and its recipients respectively.
Meanwhile, about 19% of participants were extra cautious and preferred to
35

avoid risks by not sharing their HI, even at acceptable risk levels. A study of
Europeans’ perception, behavior, and attitude toward sharing HI on the inter-
net identified three sharing profiles: self-revealing (aware of risks but reveals
information to gain benefits), indifferent, and cautious [42]. We believe that
our participants’ behavior could be profiled similarly, classifying participants
who shared HI regardless of the perceived risk levels as “indifferent,” whereas
“self-revealing” participants to be those who were motivated to share their HI
but preferred to minimize risks by adopting available methods, and finally,
“cautious” participants, who refused to share HI under any circumstances.
36

Chapter 5
Exploratory Study: Interviews
In an effort to develop a better understanding of users’ motivation to share
HI on SNSs, we explored participants’ HI sharing practices, perceptions, and
preferences.
5.1 Methodology and research questions
Following a grounded theory approach [12], we interviewed 21 chronically
ill patients to explore their HI sharing experiences on SNSs. We aimed at
identifying the main factors that influenced participants’ motivation to share
HI on SNSs by answering the following research questions (RQs):
RQ1. Why patients share their HI on SNSs?
RQ2. How patients share their HI on SNSs?
RQ3. With whom do patients share their HI on SNSs?
37

5.1.1 Sampling and participants recruitment
Following a theoretical sampling approach [12], individuals with chronic health
condition(s) were recruited through media advertisements. Potential partici-
pants were invited to visit the study webpage, where they viewed details of the
study, along with the consent form. To be eligible for the study, participants
were required to be: 19 years of age or older, living in greater Vancouver area,
maintaining at least one active account on an SNS that they visited regularly,
and having at least one chronic health condition. Participants were compen-
sated with the amount of $25 (CAD) for taking part in the study.
A total of 21 patients were interviewed throughout the study. The purpo-
sive sampling of patients who had chronic health condition(s) assured partici-
pants’ involvement in HI sharing practices. The sample included 7 women and
14 men, ranging in age between 21 and 68 years old. Participants came from
diverse ethnic backgrounds but all were speaking English fluently. A summary
of participant demographics is given in Table 5.1. Participants also came with
different health issues, including physical, mental, or both physical and men-
tal health issues. Details about participants’ health conditions are presented in
Appendix B.2.
38
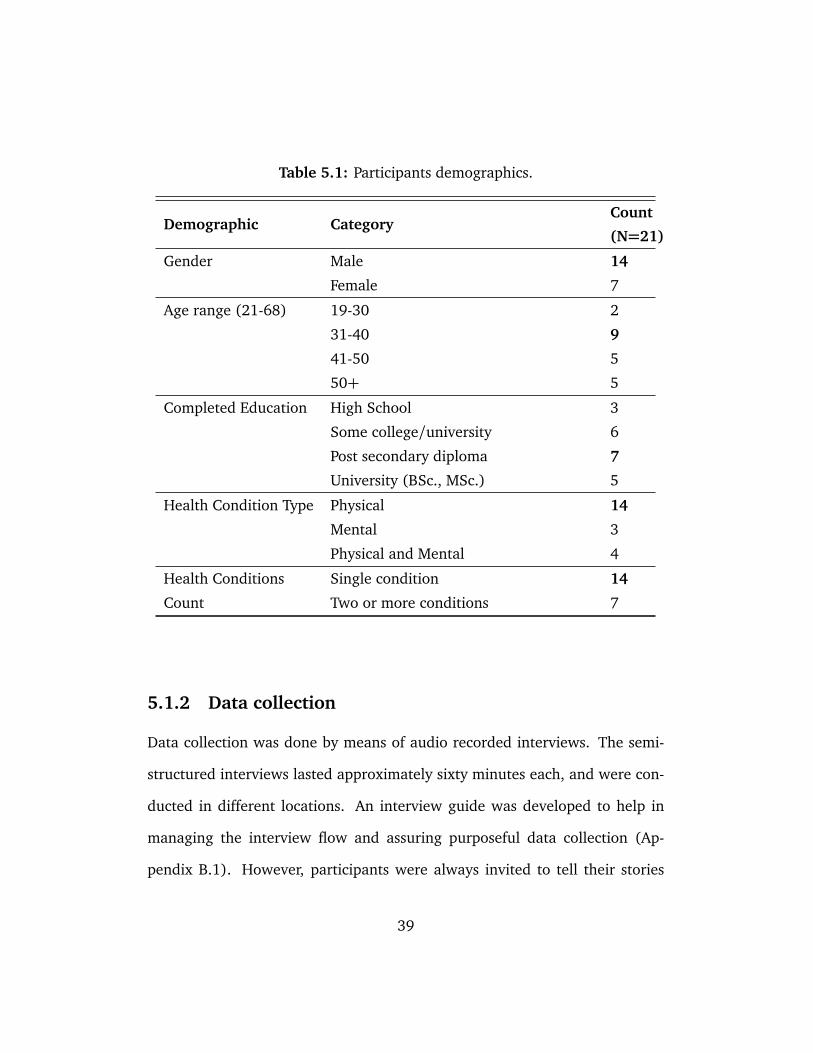
Table 5.1: Participants demographics.
Demographic CategoryCount
(N=21)
Gender Male 14
Female 7
Age range (21-68) 19-30 2
31-40 9
41-50 5
50+ 5
Completed Education High School 3
Some college/university 6
Post secondary diploma 7
University (BSc., MSc.) 5
Health Condition Type Physical 14
Mental 3
Physical and Mental 4
Health Conditions Single condition 14
Count Two or more conditions 7
5.1.2 Data collection
Data collection was done by means of audio recorded interviews. The semi-
structured interviews lasted approximately sixty minutes each, and were con-
ducted in different locations. An interview guide was developed to help in
managing the interview flow and assuring purposeful data collection (Ap-
pendix B.1). However, participants were always invited to tell their stories
39
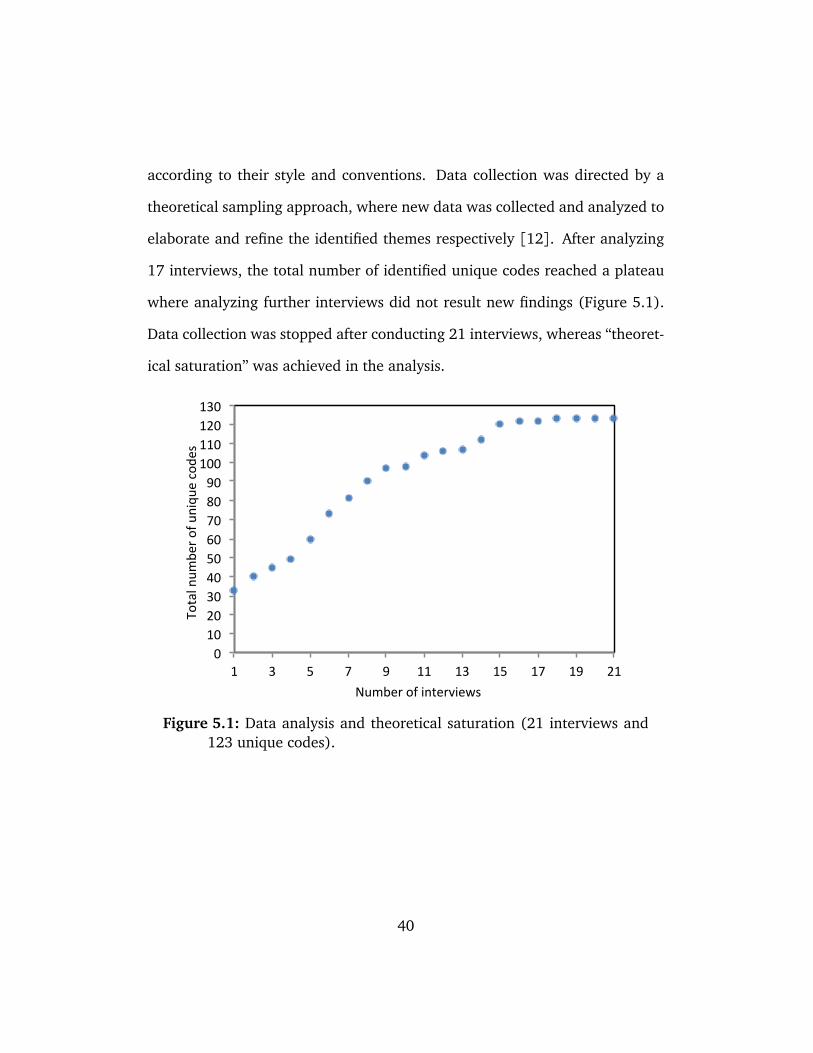
according to their style and conventions. Data collection was directed by a
theoretical sampling approach, where new data was collected and analyzed to
elaborate and refine the identified themes respectively [12]. After analyzing
17 interviews, the total number of identified unique codes reached a plateau
where analyzing further interviews did not result new findings (Figure 5.1).
Data collection was stopped after conducting 21 interviews, whereas “theoret-
ical saturation” was achieved in the analysis.
0 10 20 30 40 50 60 70 80 90 100 110 120 130
1 3 5 7 9 11 13 15 17 19 21
Total num
ber o
f uniqu
e code
s
Number of interviews
Figure 5.1: Data analysis and theoretical saturation (21 interviews and123 unique codes).
40

5.1.3 Analysis
The analysis process started immediately after transcribing the first interview
and continued concurrently with the data collection process. The recorded
interviews were transcribed verbatim by professional transcriptionists. Inter-
view transcripts were anonymized by removing identifiable information (e.g.,
names). NVivo (Version 10.1) was used as the main qualitative data analysis
tool for coding and analyzing the transcripts.
Constant comparison of coding and analyzing data through several itera-
tive stages of open, axial, and selective coding were applied [12]. Open coding
was initially used to identify, describe, and categorize interesting phenomena
that were found in the data. The first set of transcripts were read line by line
and coded accordingly, resulting in 90 unique codes after analyzing 8 inter-
views. At that point, we also started to look at interrelated codes that formed
meaningful categories (axial coding). The identified categories were as fol-
lowing: perceived privacy, perceived benefits, the recipients of the shared HI,
used technologies, prior HI sharing experiences, HI sharing motivation, trusted
entities, anonymous communication, HI sharing preferences, and health status.
We identified participants’ Motivation to share HI on SNSs as the core category
(selective coding). We also identified the following sub-categories: perceived
privacy, perceived health status, the recipients of the shared HI, prior HI sharing
experiences, and health status. The transcripts were further analyzed by selec-
tively coding new data that was related to the core category until theoretical
saturation was reached.
41

The analysis resulted in a total of 2,521 coded excerpts, with an average of
120 coded excerpts per interview. The quality and consistency of the analysis
was checked by a second researcher, who reviewed and coded a total of 100
randomly selected excerpts using our generated codes. Finally, memoing was
used frequently to describe coded events, explain observed concepts and their
relations.
5.2 Results
5.2.1 HI sharing practices on SNSs
While participants used a variety of SNSs, all participants were active users
on Facebook. Considering the fact that more than 71% of North American
internet users are on Facebook,1 it is not an anomaly to have the majority of
participants to be Facebook users. Participants indicated going on their SNSs
on regular basis. Moreover, participants indicated using a variety of sites to
share or seek HI online (e.g., SNSs, blogs). Despite the fact that the identified
sites were not designed to support HI among social peers, the majority of par-
ticipants recalled sharing HI instances on them in the past:
“I’ve got a lot of pictures on Facebook of when I was in hospital. I had pictures
of myself, my scar, and everything else. All of those are on my Facebook.”–P2 (M,
59, fractured back and defective knee)
1http://www.pewinternet.org/fact-sheets/social-networking-fact-sheet/
42

5.2.2 Perceived benefits
From simply sharing how a person feels at a specific moment, to detailed in-
formation about treatments, participants experienced sharing HI with select
individuals or groups in the past. Participants shared their HI with others
for the sake of getting benefits. The benefits of sharing HI include but not
limited to: learning from the shared experience; initiating conversations with
online peers; justifying specific behaviors; reaching out to others who had sim-
ilar health conditions; and engaging in social support. Moreover, participants
showed interest in helping other people by providing social support, empa-
thy, and experience-related feedback. It was also interesting to see how some
participants felt relieved simply by talking about their problems with others,
regardless of the expected reactions and responses:
“I feel better letting them know. Whether they understand or not, I feel re-
lieved telling them.”–P15 (M, 37, bipolar depression/anxiety)
5.2.3 The recipients of the shared HI
A number of participants (5/21) shared detailed HI with select family mem-
bers and/or close friends via online services (e.g., email, SNSs). For instance,
P21 (F, 35, herniated disks at L4-L5) used Facebook occasionally to communi-
43

cate her health issues with a friend, who was an experienced therapists, and
tried to ask for her opinion and advice. Generally speaking, while partici-
pants preferred to have in-person discussions of their health issues with other
friends and family members, the online services have provided them with a
convenient way of communication, especially when physically distanced from
friends and/or family members:
“I do [talk about health on Facebook], and especially with my wife [she lives
in a different province]. Because my wife is a nurse so, rather than going to a
doctor, she would be somebody that I would talk to first.”–P12 (M, 59, degener-
ative disc disease and brain injury)
In addition to close friends and family members, participants shared their
HI with other people who had been through similar health experiences. In
fact, they believed that their mutual experiences helped them in understand-
ing each other and communicate with less effort:
“I talk about all kinds of things I’d never talk to my able-bodied friends about,
because these people know what our lives are like. Our lives are all different but
they have a commonality that doesn’t exist with able-bodied people.”–P4 (F, 68,
C4-C5 quadriplegic)
44

5.2.4 Perceived health status
Participants developed an overall perception of their health status based on
their knowledge and perceived control over their health conditions. For in-
stance, P19, who suffered from HIV, considered his health condition as yet
another manageable disease that required only few tweaks to his life style.
This was mainly because he was completely aware of his condition, its compli-
cations, and the necessary ways to control it. Interestingly, participants who
perceived their health status to be “manageable” were found to be less mo-
tivated to engage in sharing their HI on SNSs. Moreover, participants who
suffered from chronic pain due to physical injuries and/or arthritis (9/21),
considered their health status to be stable and “manageable.” Therefore, they
showed less interest in using SNSs for sharing their HI with other people. On
the other hand, P9, who suffered from a rare disease called Neuromyelitis Op-
tica (NMO), was heavily engaged in sharing her HI on blogs and SNSs (e.g.,
MS society of Canada, Twitter, Facebook). She described a number of reasons
for her enthusiasm toward sharing her HI online, including but not limited to:
helping newly diagnosed patients; finding new information about the disease;
and participating in research. Overall, the insufficient scientific knowledge
about her condition, and the relatively small population of diagnosed patients
with similar condition were also among the reasons that motivated her to ac-
tively engage in sharing her HI on SNSs.
45

5.2.5 Perceived privacy
Despite their perceived benefits, users’ attitude toward disclosing HI on SNSs
was also affected by their need to protect their privacy [32, 40]. By explor-
ing users’ HI sharing practices and preferences, we tried to develop a better
understanding of the factors that shaped users’ perceived privacy risks when
sharing HI on SNSs.
The shared HI
To minimize the privacy concerns when sharing HI on SNSs, the majority of
participants tried to keep their shared information very general, with the least
included details about their personal health. Moreover, participants altered
their HI sharing behaviors with respect to the audience in different SNSs.
For instance, while P11 (M, 40, L3-L4 fusion) shared information about his
back injury/pain with a group of people who suffered from similar injuries on
LinkedIn, he tried to maintain his professional image by not posting irrelevant
and unprofessional details (e.g., feelings and emotions, certain drug usage).
Some participants on the other hand, avoided talking about their health issues
on their SNSs because their social peers had not experienced similar health
issues. They felt that their social peers might misread their situation and call
judgments:
“I’m not the kind of guy that is just going to throw it out there [Facebook]
and get responses from anyone on a medical issue. I think it’s just common sense
46

like, people judge. People rumour. You don’t want to throw out a bunch of stuff
that’s going to be misconstrued.”–P1 (M, 38, chronic sciatica).
It was interesting to see that some participants considered the shared HI
instances to be mostly of abstract nature. Participants believed that the shared
HI contained no important details about them, and therefore, they did not
mind sharing it with their social peers. For instance, P2 (M, 59, chronic back-
/knee pain) did not mind sharing pictures of himself and his scar on Facebook
while staying at the hospital after his surgery.
Health conditions and associated stigma
Participants shared general aspects of their health on different SNSs. More
specifically, information related to physical health conditions (e.g., injuries,
chronic pain, arthritis) were considered to be less sensitive than other types
of HI. Participants showed more discomfort when sharing information related
to their mental health. In fact, the stigma associated with such health issues
stopped them from sharing their HI with specific audiences, especially with
people whom they knew. Furthermore, we noticed that some male partici-
pants were less motivated to talk about their health issues with friends and
family members on SNSs. They believed that there was a stigma of men talk-
ing about their health, especially mental health issues:
“It’s just a stigma of men not talking about stuff like that. With you, you’re
47

a complete stranger and I’ll never see you again probably. So, it’s not that hard
for me to be candid and open about. But with friends, I’m always worried about
bumping into people I’ve known.”–P20 (M, 50, depression/chronic neck pain)
Few female participants were also concerns about sharing information re-
lated to their mental health issues on their SNSs. For instance, P5 preferred to
use an online website (reddit)2 to anonymously ask questions related to her
depression. She also tried to maintain her privacy by hiding her reddit name
from her friends. Another way of avoiding the stigma associated with shar-
ing information regarding mental health conditions was to engage in online
discussions and express feelings and health issues in an indirect manner. For
instance, P15, who suffered from chronic depression, talked about his men-
tal health issues by posting philosophical questions on his blog and Facebook
page. He used these questions as an indirect way to indicate his willingness to
talk about his feelings and mental health issues.
Anonymity and online identity
Despite the concerns and stigma of sharing HI with known people, few partici-
pants indicated that the physical distance between them and the people whom
they share their HI with through the SNS would provide them with some level
of privacy. P20 (M, 50, depression/chronic neck pain) for instance did not
mind using Facebook to share his health issues with a couple of friends who
2http://www.reddit.com/
48

were not living in the same city where he lived in. For him, there was very
little chance of running into those friends on a typical day. Similarly, P16 felt
more comfortable to communicate his health issues with physically distanced
people through Facebook:
“Even if I’m using my real name, it still feels kind of anonymous because
they’re not right there beside me. I’m not looking at them while I’m talking to
them. They could be in Sydney, Australia.”–P16 (M, 48, post-traumatic stress
disorder)
As described by P16, his anonymity was maintained by keeping himself
physically unreachable. The importance of the physical proximity in defin-
ing privacy in the online space was clearly present in participants’ responses
during the interviews. Participants also raised huge concerns with regards to
revealing their physical location in online environments. Regardless of their
healths status, participants wanted their current and/or future location to be
kept strictly confidential.
SNSs vulnerabilities and HI misuse
A number of participants perceived existing SNSs to be vulnerable to privacy
and security exploits and therefore, risking the confidentiality of their infor-
mation and increasing the chances of undesirable information disclosure. On
top of that, few participants were also concerned about the probability of hav-
49

ing their HI being misused by insurance companies and some governmental
agencies. Participants recited several stories about themselves and other indi-
viduals in their social networks that were victims of shared information mis-
use. For instance, P7 (M, 54, quadriplegic) was overwhelmed by the attempts
made by insurance companies towards cutting disability benefits from patients
by misusing their shared information on SNSs.
Moreover, both P1 (M, 38, chronic sciatica) and P5 (F, 30, chronic de-
pression) raised concerns with respect to sharing specific “risky” information
regarding their health on SNSs, especially if these behaviors were classified as
illegal behaviors in different jurisdictions (e.g., licensed drug consumptions).
Furthermore, P5 was worried about being denied access to the U.S. if she
shared information about being hospitalized for depression or bi-polar disor-
ders. She mentioned knowing over a dozen of stories about people who were
turned away from the U.S. boarders just because they shared similar HI on
Facebook.
50

5.2.6 HI Sharing preferences
Preferred user groups
Participants identified three main user groups, with whom they were willing
to share their HI on SNSs:
1. Doctors and health professionals. Almost all participants did not mind
sharing their HI with their doctors through SNSs. Doctors are the source of
information, advice and medical care. Also, they have the knowledge, ex-
perience, and the authority to initiate health management decisions [7]. As
a result, having them in any SNS that will be used for HI sharing might be
essential for patients.
2. Select friends and family members. Participants preferred to keep their
family members and friends updated about their overall health status. More
importantly, participants indicated their interest in sharing further details of
their HI with select friends and family members. However, the nature and the
level of details of the shared HI was totally dependent on the mutual health
related experiences and the closeness of their relationships. Participants were
also more open to discuss details of their health issues with those friends and
family members who had expertise n the medical field.
3. Others with similar health conditions and experiences. All partic-
ipants valued the importance of having access to a pool of people who had
gone through similar health issues. Due to the mutual experiences, the per-
ceived benefits were higher when communicating HI with others who had
51

gone through similar health experiences. It was also important for partici-
pants to consider other mutual factors when deciding to share their HI with
other people (e.g., age range, ethnicity, undergone treatments).
The SNS environment
Other than the preferred involved user groups, participants also identified a
number of important features for any SNS that would be used for HI sharing.
For the majority of participants, it was important to know who owns/operates
the SNS. Most of the participants (20/21) considered the government and/or
their doctors’ offices to be the most reliable and trusted entities with their
HI. Moreover, participants did not necessarily trust SNSs that were provided
by private companies with their health records, unless recommended by their
doctors. The ability to maintain an online version of their health records in
the SNS was essential to all participants as well. Nevertheless, participants
required to have their health records fully contained in the SNS environment.
Participants preferred to keep their health records private and hidden from
other users. In addition, participants required adequate security measures for
protecting their stored data (e.g., using encryption).
Communication and HI presentation
To maintain their boundaries while communicating HI with strangers, par-
ticipants required having anonymous communication capabilities in the SNS.
Anonymity does not necessarily mean hiding all personal information. In fact,
the majority of participants did not mind revealing their first name and their
52

city of residence. However, the anonymity was necessary to maintain privacy
by managing the identity and hiding some HI from other social peers. In gen-
eral, participants preferred to perform one-to-one communications whenever
they wanted to discuss details about their health with other social peers. Par-
ticipants also indicated their need to maintain the way their HI was viewed
by others. For instance, while participants did not want their social peers to
view every detail of their HI, they did not mind sharing an aggregate view of
their HI with those who had similar health conditions (e.g., viewing progress
updates during a course of treatment).
5.2.7 Results summary
In this study, we explored HI sharing practices and privacy preferences on
SNSs. We asked chronically ill SNS users about their prior experiences with
sharing HI on SNSs. We highlighted the perceived benefits, perceived privacy
risks, and perceived health status as the main factors that influenced users’
motivation to share HI on SNSs. In addition, our results indicated that users’
perceived benefits and perceived privacy risks were highly related to the recip-
ients of the shared HI on SNSs. Moreover, we identified key characteristics of
the preferred recipients of the shared HI on SNSs (medical expertise level, mu-
tual health experiences, strength of social ties). Finally, we discussed general
requirements for developing a trusted SNS environment that would facilitate
HI sharing among social peers (e.g., anonymity, trusted owner/operator, HI
communication/presentation).
53

Chapter 6
Confirmatory Study: Online Survey
6.1 Methodology
In this user study, we conducted an online survey to confirm our findings from
the exploratory study. The online survey consisted of a mixture of close- and
open-ended questions. The survey gave us the opportunity to reach a more
representative sample of SNSs users, which in return helped in achieving more
generalizable findings.
6.1.1 Why Facebook?
Results of our exploratory study indicated that the majority of participants
were active Facebook users (Section 5.2). Facebook is the largest SNS today,
consisting of more than a billion active users, with a huge active user popu-
lation that goes on Facebook on daily basis.1 As of August 2015, Facebook
1http://newsroom.fb.com/company-info/
54

remains by far the most popular SNS in the US, with 72% of online adults
to use Facebook (62% of all adults in the US) [17]. Furthermore, Facebook is
one of the few SNSs that have been extensively studied by social and computer
scientists, resulting in a good understanding of how it is generally used and
for what purposes [18, 35, 36].
6.1.2 Participants recruitment
Participants were recruited via Amazon Mechanical Turk (MTurk),2 which is a
crowdsourcing website that provides a reliable source of high-quality data for
research involving human-subjects [50]. A respondent was expected to finish
the survey in less than 30 minutes. To ensure quality data collection and anal-
ysis, we used MTurk’s features to recruit highly qualified participants who had
successfully completed 100 tasks or more on MTurk with a minimum approval
rate of 95%. Participants were limited to a single submission only. They were
compensated with $1 (US) through MTurk for successfully completing the sur-
vey. To ensure successful compensation on MTurk, participants were required
to submit a unique code, which was assigned to them after completing the
survey.
6.1.3 Data collection
A total of 537 participants accessed the online survey between October 16–23,
2015. A single participant declined to take the survey while 18 other par-
2www.mturk.com
55

ticipants submitted incomplete responses. The average completion time was
approximately 10 minutes with an overall survey completion rate of 96.5%.
Submissions were closely examined considering completion time. All submis-
sions that lasted less than 4 minutes were fully examined to ensure quality and
validity of the provided answers. Finally, to insure consistency of the sample
and avoid the effects of cultural differences, we excluded submissions made
from people residing outside of the US. The remaining 492 submissions were
included in further analysis through the study.
6.1.4 Data analysis
The survey was employed on UBC’s online survey tool.3 We used MS Excel
and SPSS (Version 23.0) to perform statistical analysis on the data. We also
used NVivo (Version 10.1) for coding and analyzing qualitative text responses
whenever required. Descriptive statistics were used to explain the underlying
properties of the collected data (e.g., mean, SD), while a number of inferential
statistic analysis were used to highlight correlations and significant differences
among groups (e.g., person’s correlation). A series of between-subjects anal-
ysis were used to explore participants’ motivations and perceptions. We used
Kruskal-Wallis test for comparing k−independent samples, with post-hoc pair-
wise comparisons using Mann-Whitney U tests. We also employed Friedman’s
test and/or Wilcoxon signed-rank tests to check for significant differences in
participants’ responses when repeated measurements were collected from the
3www.survey.ubc.ca
56

same participants (within-subjects).
6.1.5 Survey items
The survey questionnaire, which is presented in Appendix C.1, consists of the
following parts:
Demographics and background
We collected general demographic information that were used to characterize
different groups of participants (Q.1–Q.5). We also asked participants to iden-
tify their IT background and computer experiences (Q.6). Finally, we collected
information about participants’ Facebook usage Facebook friends (Q.7–Q.11).
Perceived health status and previous HI sharing experiences
We asked participants’ about their health conditions (Q.12–Q.13). We also
asked participants to indicate their health status from their point of view
(Q.14). Furthermore, we asked participants to indicate their experiences with
health-related SNSs (Q.15–Q.18). We also surveyed participants’ previous HI
sharing experiences on Facebook (Q.19–Q.20). Furthermore, we asked partic-
ipants to evaluate their previous HI sharing experiences on Facebook (Q.21–
Q.22).
Motivation to share HI on Facebook
Participants were asked to indicate their overall willingness to share their HI
on Facebook by rating their choice on a 5-points Likert scale (Q.23). We also
57

asked participants to identify the factors that might motivate or stop them
from sharing their HI on Facebook (Q.24–Q.25).
Preferred recipients of the shared HI
Participants were asked to indicate their motivation to share their HI with
different user groups by rating their level of agreement on a 5-points Likert
scale (Q.26). We also asked participants to indicate their willingness to use a
search feature to find certain users through Facebook (Q.27).
Anonymous online identity
We asked participants to consider an option for creating anonymous online
identities and indicate their willingness to use it whenever sharing their HI
with other Facebook users (Q.28–Q.29). Participants were also asked to iden-
tify the information items that they were likely to hide if they were to create
an anonymous online identity for the purpose of sharing HI on SNSs (Q.30).
Trusted SNSs providers
We identified possible SNS providers and asked participants to identify their
level of trust in each SNS provider (Q.31). We also ask participants to indicate
their level of trust in an SNS if it was recommended to them by either a close
friends/family member, friends who had medical expertise, friends who had
mutual health experiences, or their doctors (Q.32).
58

Attitudes toward privacy
We used the Westin Privacy Index to categorize our participants into three
groups: privacy Fundamentalists, privacy Pragmatists, or privacy Unconcerned.
We asked participants to rate their level of agreement on a 4-points Likert
scale for the given statements in Q.33 (Appendix C.1). Privacy Fundamental-
ists were participants who agreed (strongly or somewhat) with the first state-
ment and disagreed (strongly or somewhat) with the second and third state-
ments. Privacy Unconcerned were those who disagreed with the first statement
and agreed with the second and third statements. The remaining participants
were categorized as privacy Pragmatists [33]. Furthermore, we asked partici-
pants to indicate the number of performed privacy-related actions on Facebook
(Q.34).
6.2 Results
6.2.1 Demographics
We analyzed responses from 492 participants residing in the US with ages
ranging between 19 and 74 years old (mean=34.7 and σ=10.8). A summary
of participant demographics is presented in Table 6.1. The sample consisted
of almost equal number of male and female participants, with a wide range
of employment categories including Students (32/492) and Unemployed par-
ticipants (72/492). While about 75% of our participants were younger than
40 years old, almost half of all participants were between 19 and 30 years of
59

age (46.1%). About 60% of participants completed a post-secondary degree
(e.g., Diploma, Bachelor’s, Master’s, or PhD). Approximately 20% of partici-
pants indicated having a degree and/or work experience in fields related to
Computer/IT. Furthermore, the vast majority of participants (91.1%) spent
more than 2 hours on the Internet on daily basis (mean= 6.5 and σ= 3.4).
These demographics reflect the nature of MTurk workers, who were shown to
be highly active internet users with higher education levels and younger ages
than the general population [50].
We also asked participants to indicate their Facebook usage and back-
ground. About 97% of participants have been on Facebook for at least 4
years (mean= 7.7 and σ= 2.3). On average, participants had approximately
289 Facebook friends (min= 0,max = 3165).4 The majority of participants
(98.8%) were checking their Facebook accounts at least once a week, while
84.6% of all participants checked their Facebook on daily basis. Participants
were asked to describe their Facebook friends by selecting all that applies from
a list of categories. Family members and relatives, offline friends, colleagues/co-
workers, and friends’ friends represented the top four categories as specified
by participants. A comparison of participants’ Facebook usage frequency and
friends’ demographics with Pew research centre’s recent report shows that our
sample is in fact representative of US Facebook users with slightly more active
participants, which is typical for MTurk worker [17].
4A participant used Facebook only to view certain pages (no added friends).
60

Table 6.1: Participants demographics (N = 492).
Demographic Category Count (%)
Gender Male 246 50.0
Female 245 49.8
Unspecified 1 0.20
Age range 19–30 227 46.1
(19–74) 31–40 145 29.5
41–50 62 12.6
51+ 58 11.8
Completed Undergraduate University 208 42.3
Education Some college/university courses 136 27.6
Graduate University 58 11.8
High School 51 10.4
Post-secondary diploma 33 6.70
Less than High School 3 0.60
Other 3 0.60
Employment Business, management, or financial 65 13.2
Categories Services 62 12.6
(Top 5) Computer engineer, IT professional 41 8.30
Administrative support 34 6.90
Education 33 6.70
6.2.2 Perceived health status
We asked participants about their overall health status and existing health
conditions. Only 73 participants (14.8%) did not have any chronic health
conditions while the remaining 419 participants (85.2%) reported 55 different
61

health conditions. Allergies, anxiety, depression, stress, arthritis and chronic
pain, asthma, obesity, diabetes, heart disease, and cancer represented the most
frequent health conditions reported by participants (Figure 6.1). About one
third of all participants (33.9%) suffered from one chronic health condition,
while slightly over half of participants (51.2%) reported two or more chronic
health conditions. Among participants who reported having chronic health
conditions (n=419), the majority (96.9%) reported having the chronic health
condition(s) for at least two years.
Participants were asked to identify their perceived health status on a 4-
point Likert scale (“poor”, “fair”, “good”, and “excellent”). A number of studies
showed that the self-reported health status could be considered as a reason-
able indicators of one’s overall health [28, 54]. Despite that, in Section 5.2.1
of the exploratory study, we discussed that patients’ perceived health status
could be influenced by their perceived control over their health conditions. In
line with our previous findings, we noticed that 253 of the online survey par-
ticipants (about 51%) had one or more health conditions and yet perceived
their health status to be “good” or “excellent” (Figure 6.2). Furthermore, 13
participants reported “fair” health status without having any health conditions.
By combining the self-reported health status with the reported health con-
ditions, we grouped participants into three groups: (1) Healthy (14.8%), indi-
viduals who had no chronic health conditions; (2) Manageable (51.4%), indi-
viduals who had at least one chronic health condition and perceived “good/ex-
cellent” health status; and (3) Unhealthy (33.7%), individuals who had at
62

least one chronic health condition and perceived “fair/poor” health status (Fig-
ure 6.3). We believe that these categories provide a better representation of
participants’ overall health, and therefore, we used them for further compari-
son of participants’ behaviors according to their health status.
36.8% 34.8%
28.0% 18.1%
14.6% 13.8%
11.8% 4.1% 3.0% 2.6%
1.4% 1.4% 1.0% 0.8% 0.8% 0.8% 0.6% 0.6% 0.6% 0.6%
0% 10% 20% 30% 40% 50%
Allergies Anxiety
Depression Stress
Arthri<s and chronic pain Asthma Obesity Diabetes
Heart disease Cancer
Ea<ng disorder Hypertension
Irritable bowel syndrome Migraine
Mul<ple Sclerosis Crohn's
Autoimmune disorder COPD
Chronic Fa<gue Sjogren's Syndrome
% of par<cipants
Figure 6.1: Health conditions cumulative percentage frequency (95%).
63

0 13
37 23 22
144
226
27
0
40
80
120
160
200
240
280
Poor Fair Good Excellent
Num
ber o
f par?cipants
No health condi?ons 1 or more condi?ons
Figure 6.2: Perceived health status and the number of reported healthconditions.
Healthy, 14.8%
Manageable, 51.4%
Unhealthy, 33.7%
Figure 6.3: Categorizing participants according to their perceived healthstatus and the number of health conditions.
64

6.2.3 Attitudes toward privacy
We used the Westin Privacy Index to categorize participants based on their
privacy attitudes [11, 14, 33]. As shown in Figure 6.4, about 54.3% of our
participants were Privacy Fundamentalists, 33.5% were Privacy Pragmatists,
and 12.2% were Privacy Unconcerned. Our sampling resulted more Privacy
Fundamentalists participants. This might be a result of sampling MTurk work-
ers, who were shown to be more privacy-aware and tech-savvy as compared
to the general population [31].
To verify the results of the Westin privacy index, we asked participants to
report the number privacy-preserving actions that they performed on Face-
book. About 26% of participants performed 10 privacy-preserving actions on
Facebook (mean=7.16 and σ=2.63). It was assumed that the privacy Funda-
mentalists perform more privacy-preserving actions in the online environment
when compared to Pragmatists and Unconcerned. A Spearman’s rank-order
correlation showed a negative correlation between the number of performed
privacy-preserving actions and participants’ privacy attitudes, which was sta-
tistically significant (r(490) =−0.176, p < 0.001). This however verifies the
results of the Westin privacy index, which identified relatively more number
of privacy fundamentalists in the sample.
65

Fundamentalists, 54.3% Pragma6cs,
33.5%
Unconcerned, 12.2%
Figure 6.4: Attitudes toward privacy (Westin Privacy Index).
6.2.4 HI sharing experiences
We asked participants to indicate if they ever shared details of their health
information with other people on Facebook. As shown in Figure 6.5, about
half of participants (48.6%) never shared their HI with anyone on Facebook.
Among the remaining participants, 71.1% indicated sharing their HI details
with “some close friends or family members”, while 37.9% shared their HI
details with “select friends who had medical expertise and/or mutual health
experiences.”
66

71.1%
37.9% 32.8%
11.5%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Some close friends or family members
Select friends who had medical experBse and/
or mutual health experiences
Everyone on my Facebook friends list
Other Facebook users (Non-‐friends) who had medical experBse and/
or mutual health experiences
% of p
arBcipants
Figure 6.5: Percentage of participants who shared details of their HI withother user groups on Facebook (n= 253).
Furthermore, we asked participants to evaluate their prior HI sharing expe-
riences on Facebook (Positive, Negative, Both positive and negative, or Neither
positive nor negative). Three participants did not provide an evaluation for
their prior HI sharing experiences on Facebook. Among the remaining 250
participants, more than half of them (57.7%) evaluated their prior HI sharing
experience to be Positive, while about 18.2% had Both positive and negative
experiences. It is interesting to see that only eight participants (3.2%) in-
dicated having only Negative experiences, while the remaining participants
(19.8%) indicated Neither positive nor negative experiences. We also asked
participants to explain in their own words why they thought that their experi-
67
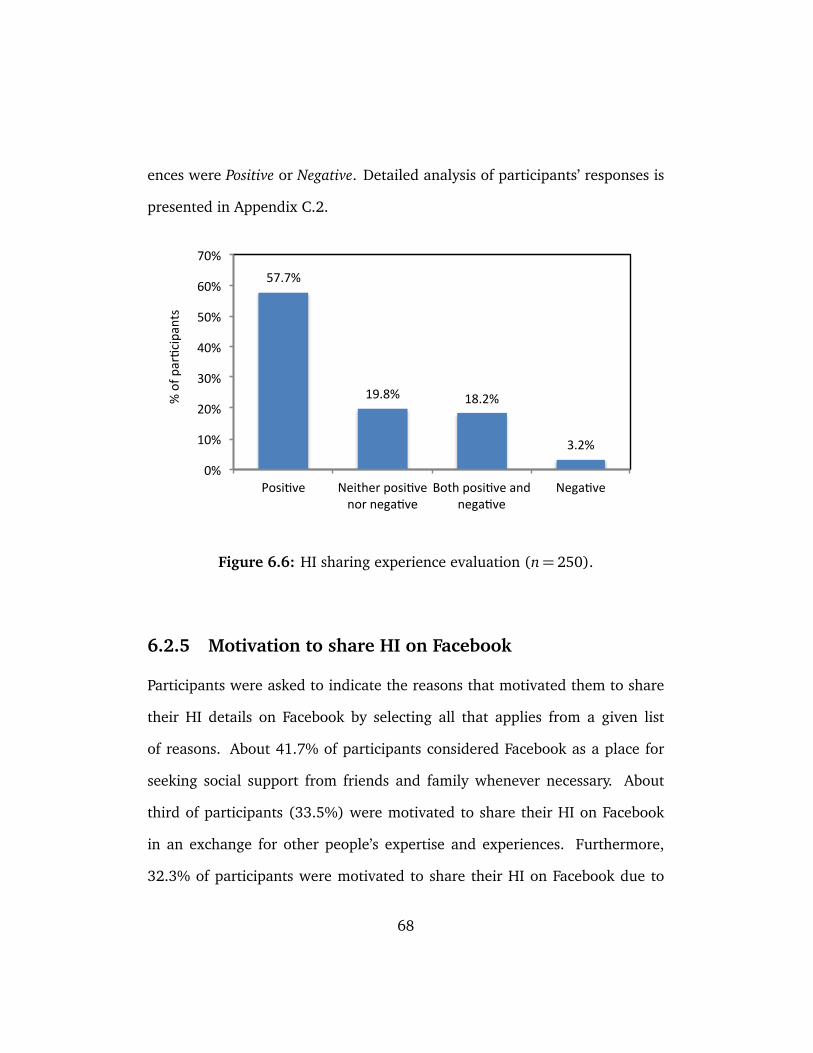
ences were Positive or Negative. Detailed analysis of participants’ responses is
presented in Appendix C.2.
57.7%
19.8% 18.2%
3.2%
0%
10%
20%
30%
40%
50%
60%
70%
Posi2ve Neither posi2ve nor nega2ve
Both posi2ve and nega2ve
Nega2ve
% of p
ar2cipants
Figure 6.6: HI sharing experience evaluation (n= 250).
6.2.5 Motivation to share HI on Facebook
Participants were asked to indicate the reasons that motivated them to share
their HI details on Facebook by selecting all that applies from a given list
of reasons. About 41.7% of participants considered Facebook as a place for
seeking social support from friends and family whenever necessary. About
third of participants (33.5%) were motivated to share their HI on Facebook
in an exchange for other people’s expertise and experiences. Furthermore,
32.3% of participants were motivated to share their HI on Facebook due to
68

their previous positive experiences. It was also interesting to see that 28.9%
of participants were passionate to help others by sharing their own health-
related experiences on Facebook. This however conformed with the two-way
nature of information sharing on SNSs where some people tend to generate
and disseminate content for the rest of the population. Finally, the lack of
knowledge about the health conditions, and the fact that Facebook helped
participants in connecting to other people who had similar health issues, were
also among the motivating factors for about 20% of participants.
Prior HI sharing experiences on Facebook
The results of the Mann-Whitney U tests showed a statistically significant
difference in participants’ willingness to share HI on Facebook when com-
pared based on their prior HI sharing experiences, with mean ranks of 328.3
and 160.0 for the two groups respectively (p < 0.001 and large effect size
r = 0.61). This indicates that those who had previously shared their HI on
Facebook were more willing to share their HI on Facebook in the future. To in-
vestigate further, we used participants’ evaluation of their prior HI sharing ex-
periences to group them into the following categories: (1) Positive, those with
only positive experiences; (2) Negative, those with only negative experiences;
(3) Both, those with both positive and negative experiences; and (4) Neither,
those with neither positive nor negative. A Kruskal-Wallis test followed by a se-
ries of pair-wise comparisons using Mann-Whitney U tests showed statistically
significant differences for all pair-wise comparisons except when comparing
69
Both and Neither groups. The results showed that having only positive experi-
ences in the past would highly motivate participants to share HI in the future.
In addition, participants who had only negative experiences were shown to
be less motivated to share their HI details on Facebook as compared to other
groups.
Privacy attitudes and motivation to share HI on Facebook
Participants were grouped based on their privacy attitudes (Fundamentalists,
Pragmatists, and Unconcerned). A Kruskal-Wallis test showed a statistically
significant difference in willingness to share HI details on Facebook between
all groups (χ2(2) = 33.42, p < 0.001), with mean ranks of 218.4 for Funda-
mentalists, 263.5 for Pragmatists, and 325.1 for Unconcernedparticipants. The
pair-wise comparisons using Mann-Whitney U tests showed significant differ-
ences between all three groups, with p≤ 0.001 for all pair-wise comparisons
(r1−2 = 0.168, r1−3 = 0.287, and r2−3 = 0.226). Conforming with prior find-
ings, privacy Fundamentalists were shown to be less willing to share their HI
details on Facebook as compared to privacy Pragmatists and privacy Uncon-
cerned respectively.
Health status and motivation to share HI on Facebook
We conducted a of Kruskal-Wallis test to investigate the effects of health status
(Healthy, Manageable, and Unhealthy) on the motivation to share HI on Face-
book. The test showed a statistically significant difference in the motivation
to share HI details on Facebook among the three groups (χ2(2) = 8.11, p <
70
0.017), with mean ranks of 241.4, 242, and 267.4 respectively. Furthermore,
the pair-wise comparisons using Mann-Whitney U tests showed significant dif-
ferences in motivation to share HI details on Facebook between Healthy and
Unhealthy groups only (p=0.007 and r1−3=0.176). This conforms with prior
findings that associated online HI seeking/sharing activities with the overall
health status and the number of health conditions [17, 23, 54]. Moreover, a
closer look at the participants who were motivated to share their HI on Face-
book showed that the majority of them (about 91%) were classified as either
Unhealthy or Manageable, which was another good indication of the under-
lying correlations between participants’ health status and their motivation to
share HI on Facebook.
6.2.6 Preferred recipients of the shared HI
We asked participants to indicate their willingness to share their HI with differ-
ent recipients on Facebook. As shown in Figure 6.7, about 67% of participants
considered sharing their HI with “some close friends and/or family members,”
while about 65% considered sharing their HI with “friends and/or family
members who had medical expertise and/or mutual health experiences.” On
the other hand, about 73% of all participants did not consider sharing their HI
with “all their Facebook friends.” Furthermore, about 53% of participants did
not consider sharing their HI with strangers through Facebook, even if those
strangers had “expertise in the medical field or mutual health experiences.”
Within-subjects comparison of the repeated measures showed that partici-
71

pants were significantly more willing to share their HI with friends and family
members who had strong social ties. Moreover, while the “closeness” and the
strength of the relationships among friends and family members were shown
to influence their motivation to share HI with each other, the presence of “med-
ical expertise and/or mutual health experiences” were also considered as im-
portant motivating factors that encouraged them toward exchanging their HI
on SNSs.
0% 20% 40% 60% 80% 100%
All my Facebook friends
Other Facebook users (Non-‐friends) who might have medical experGse and/or
mutual health experiences
Friends and/or family members who might have medical experGse and/or mutual
health experiences
Some close friends and/or family members
Strongly Disagree Disagree Neutral Agree Strongly Agree
Figure 6.7: Willingness to disclose HI to different recipients on Facebook.
To extend our investigation, we compared participants’ willingness to share
HI with different recipients on Facebook.5 For every recipient group, we found
5The “All Facebook friends” group was excluded from the pair-wise comparisons since itwas not representing specific recipients.
72

statistically significant differences in participants’ willingness to share HI when
compared based on their prior HI sharing experiences and privacy attitudes.
Our results conformed to participants’ overall motivation to share HI on Face-
book. In addition, our test results indicated that Unhealthy participants were
significantly more willing to share their HI with “non-friends” Facebook users
as compared to Healthy participants (p= 0.007 and r = 0.18). In other words,
while participants’ health status was not a determining factor when sharing
HI with friends and family members, it significantly influenced participants’
motivation to share HI with non-friends Facebook users.
6.2.7 Willingness to search for specific users
In a hypothetical situation, participants were asked to indicate their willing-
ness to use customized search features that could help them in finding other
Facebook users who had “mutual health experiences” or “expertise in the med-
ical field.” Between 32-29% of all participants were “(Very) Likely” to search
for Facebook users who had “mutual health experiences” or “medical exper-
tise” respectively. On the other hand, about half of all participants were “(Very)
Unlikely” to use the search feature for finding other Facebook users.
Within-subjects comparison of participants’ willingness to use the search
features for finding different users showed that participants were significantly
more willing to search for other Facebook users who had “mutual health ex-
periences” as compared to users who had “expertise in the medical field”
(p < 0.001 and r = 0.2). Moreover, the between-subjects tests showed that
73
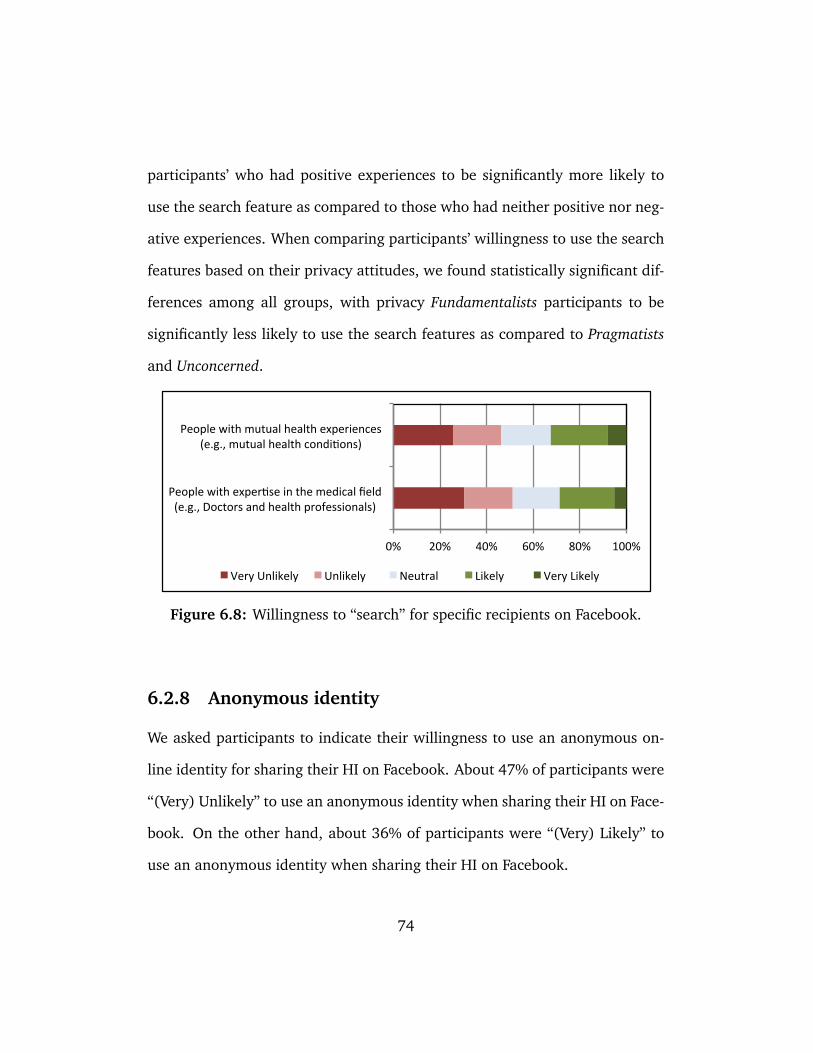
participants’ who had positive experiences to be significantly more likely to
use the search feature as compared to those who had neither positive nor neg-
ative experiences. When comparing participants’ willingness to use the search
features based on their privacy attitudes, we found statistically significant dif-
ferences among all groups, with privacy Fundamentalists participants to be
significantly less likely to use the search features as compared to Pragmatists
and Unconcerned.
0% 20% 40% 60% 80% 100%
People with exper4se in the medical field (e.g., Doctors and health professionals)
People with mutual health experiences (e.g., mutual health condi4ons)
Very Unlikely Unlikely Neutral Likely Very Likely
Figure 6.8: Willingness to “search” for specific recipients on Facebook.
6.2.8 Anonymous identity
We asked participants to indicate their willingness to use an anonymous on-
line identity for sharing their HI on Facebook. About 47% of participants were
“(Very) Unlikely” to use an anonymous identity when sharing their HI on Face-
book. On the other hand, about 36% of participants were “(Very) Likely” to
use an anonymous identity when sharing their HI on Facebook.
74

24.8% 22.6%
16.9%
25.4%
10.4%
0%
5%
10%
15%
20%
25%
30%
Very Unlikely Unlikely Neutral Likely Very Likely
% of p
ar>cipants
Figure 6.9: Willingness to use an “anonymous” identity for sharing HI onFacebook.
A between-subjects comparison of participants’ willingness to use anony-
mous identities for sharing HI on Facebook showed that participants who had
IT/Computer knowledge were significantly more willing to use anonymous
identities on Facebook as compared to those who had no IT/Computer knowl-
edge (p = 0.036 and small effect size r = 0.1). Furthermore, our results in-
dicated that privacy Pragmatists were significantly more willing to use anony-
mous identities for sharing their HI on Facebook as compared to Fundamental-
ists and Unconcerned participants (p= 0.016 and p= 0.015). Finally, we were
unable to find statistically significant difference in participants’ willingness to
use an anonymous identity for sharing HI on Facebook when compared based
on their health status. This means that regardless of participants health status,
75

their motivation to use an anonymous online identity for sharing HI on Face-
book was mainly influenced by their privacy attitudes and their IT/Computer
knowledge and experience.
Participants were also asked about their willingness to “hide” different in-
formation items when creating their anonymous identity that would be used
for sharing HI with strangers. As shown in Figure 6.10, about 95% of partici-
pants were “(Very) Likely” to hide their residential address and phone number.
Approximately 90% preferred to hide their current/future location informa-
tion, identifiable profile picture, email address, and last name. On the other
hand, slightly over 60% of participants were “(Very) Unlikely” to hide their
gender. It was also interesting to see that about 50% of all participants were
“(Very) Unlikely” to hide their health conditions when creating their anony-
mous identities.
In an effort to reduce the correlated information items presented in Fig-
ure 6.10 into fewer meaningful items, we performed principle component
analysis (PCA). The results of the component analysis indicated that about
66% of the cumulative variance was described by selecting three components.
We considered an information item to be a part of a component if it had a
factor loading of at least 0.6 for the particular component and a factor load-
ing under 0.4 for the other components. Moreover, the appropriateness of
the component analysis was tested using KMO and Bartlett’s tests, which re-
sulted statistically significant correlations that were appropriate for using PCA
(KMO= 0.87, p< 0.001, d f = 91).
76

0% 20% 40% 60% 80% 100%
Residen/al address
Phone number
Last name
Future loca/on informa/on
Email address
Iden/fiable profile picture
Current loca/on informa/on
Occupa/on and employment
City where I live
First name
Age and date of birth
Hobbies and interests
My health condi/on(s)
Gender
Very Likely Likely Neutral Unlikely Very Unlikely
Figure 6.10: Willingness to hide different information pieces when cre-ating an “anonymous” identity for the purpose of sharing HI onFacebook.
As shown in Table 6.2, twelve information items were grouped into three
components, while the remaining two items did not conform to any particular
component (occupation and employment, and city of residence). We named
the identified components as following: (1) Contact and location information,
which consisted of information that could be used to directly reach an individ-
77

ual (e.g., phone number, residential address); (2) Demographic information,
which consisted of information that were not identifiable by themselves but
could be used to describe properties of an individual in real life (e.g., age,
gender, hobbies); and (3) Identity information, which represented informa-
tion that could lead to revealing one’s real identity (e.g., picture, first/last
name). We also created an index variable for each component by averaging
participants’ rating for every information item within that component.
The results in Table 6.2 indicates that considerably more participants were
“(Very) Likely” to hide information related to their Contact and location and
Identity, with an average score of 91% and 81% respectively. Demographic
information on the other hand resulted the least score among all components
(average score of 38%), with statistically significantly less number of partici-
pants who were likely to hide their demographic information on Facebook as
compared to identity, contact, or location information. It was also interesting
to see that “health conditions” were categorized as Demographic information,
with about 30% of participants who were likely to hide information related to
their health conditions on Facebook.
78

Table 6.2: PCA results for different personal information items. The lastcolumn represents the percentage of participants who were likely tohide each information item.
ComponentFactor
loading
Agreement
(%)
Contact and location information — 91
Phone number 0.87 94
Residential address 0.80 95
Email address 0.74 89
Future location information 0.73 89
Current location information 0.72 86
Demographic information — 38
Gender 0.83 21
My health condition(s) 0.80 30
Hobbies and interests 0.69 38
Age and date of birth 0.62 64
Identity information — 81
Identifiable profile picture 0.79 87
Last name 0.75 89
First name 0.72 66
Information items that did not
conform to any component — —
Occupation and employment NA 76
City where I live NA 72
79

Comparing participants based on their privacy attitudes, we found statisti-
cally significant differences in participants motivation to hide different infor-
mation items with the exception of the following two cases: (1) Pragmatists
and Unconcerned participants’ motivation to hide Contact and location infor-
mation, which confirms the relatively higher level of concerns raised by all
participants toward revealing their Contact and location information; and (2)
Fundamentalists and Pragmatists participants’ motivation to hide Demographic
information, which indicates less concerns toward revealing information re-
lated to participants’ demographics. In addition, we found a statistically sig-
nificant difference in participants’ motivation to hide Demographic information
when compared based on their prior HI sharing experiences (p= 0.003). The
tests results also indicated that participants with Positive experiences in the
past were more willing to reveal their Demographic information as compared
to participants with other experiences (e.g., Negative).
6.2.9 Willingness to trust SNSs with HI
We asked participants to indicate their willingness to trust different SNS providers
with their submitted HI. About 27% of all participants trusted an SNS with
their HI if it was provided by a governmental health authority, while slightly
less than 20% of participants trusted a governmental agency (non-health re-
lated) and a recognized private company (Figure 6.11). On the other hand,
about 58% of participants did not trust an SNS that was provided by a govern-
mental agency (non-health related), which was relatively more than the per-
80

centage of participants who did not trust other SNS providers. Within-subjects
comparisons showed that significantly more number of participants were will-
ing to trust an SNS with their HI if it was provided by a governmental health
agency as compared to other providers.
0% 20% 40% 60% 80% 100%
A governmental agency (non-‐health related)
A recognized private company
A governmental health authority (e.g., city, state/province, federal/naDonal)
Strongly Disagree Disagree Neutral Agree Strongly Agree
Figure 6.11: Willingness to trust different SNS providers.
We also asked participants to indicate their willingness to trust an SNS
with their HI if it was recommended by different people (doctors, friends with
mutual health experiences, friends with medical expertise, and close friends/-
family members). The results of a Friedman’s test and the post-hoc comparison
using Wilcoxon signed-rank test showed statistically significant differences in
participants willingness to trust an SNS with their HI if it was recommended
by their doctors as compared to other people. This however might indicate
the overriding influence of doctors’ recommendations on their patients’ over-
all willingness to trust different SNS providers with their shared HI.
81

Chapter 7
Discussion
7.1 Motivating factors
Our results indicated that participants’ willingness to disclose HI on Facebook
was mainly influenced by the following factors: (1) prior HI sharing experi-
ences; (2) privacy attitudes; (3) perceived health status; and (4) the preferred
recipients of the shared HI.
We found that participants’ prior HI sharing experiences had a significant
impact on their willingness to share HI on Facebook, with participants who
previously shared their HI on Facebook to be more willing to share their HI
on Facebook in the future. Furthermore, participants who described their
prior HI sharing experiences to be Positive were significantly more likely to
disclose their HI on Facebook as compared to participants who had Negative
experiences. In addition, we found that Positive HI sharing experiences were
82

described as online communications with other social peers that resulted some
form of benefits (e.g., positive support). Moreover, discussing HI on SNSs cre-
ated an opportunity for some users to find other SNS users who had similar
health experiences. On the other hand, Negative experiences were mainly ex-
pressed due to the lack of gained benefits as a result of sharing HI on SNSs.
However, participants were also intimidated by the loose control over their
shared HI in the semi-public SNS environments, which in times lead to un-
foreseen consequences such as gossips, rumours, and judgments.
We used participants’ attitudes toward privacy to classify them into privacy
Fundamentalists, privacy Pragmatists, and privacy Unconcerned groups [14,
33]. Our results showed that privacy Fundamentalists participants performed
relatively more privacy-preserving actions on Facebook as compared to privacy
Pragmatists and Unconcerned participants. In addition, privacy Fundamental-
ists participants were found to be significantly less likely to disclose their HI
on Facebook as compared to participants who were classified as privacy Prag-
matists or Unconcerned. Our results came in line with findings from previous
studies that discussed the influence of privacy attitudes on users’ overall will-
ingness to disclose sensitive personal information to online websites [11, 40].
The number of health conditions and the self-reported health status were
used to categorize participants into Healthy, Manageable, and Unhealthy groups.
Conforming with previous findings [23, 28, 54], we showed that Unhealthy
participants, who had one or more health conditions and perceived their health
to be poor/fair, were significantly more likely to disclose their HI on Face-
83

book as compared to Healthy participants (people with no health conditions).
Furthermore, participants with Manageable health status, who had at least
one chronic health condition and perceived their health to be good/excellent,
were shown to fall somewhere between Healthy and Manageable participants
in terms of their motivation to share HI on SNSs. In other words, patients’
motivation to share HI on SNSs could highly depend on their confidence in
the level of control over their health conditions, with those who had higher
control to be less motivated to discuss their HI issues with other social peers
and vice versa.
Our results indicated that despite participants’ health status, they were
more willing to disclose their HI to “friends and/or family members” as com-
pared to other Facebook users (e.g., non-friends). Moreover, while the strength
of the relationship among friends and family members increased their willing-
ness to share HI with each other, the presence of “medical expertise” or “mu-
tual health experiences” were also considered as important motivating factors
that encouraged them toward exchanging their HI on SNSs. Moreover, while
participants were generally less motivated to share their HI with non-friend
Facebook users, Unhealthy participants were found to be significantly more
willing to share their HI with non-friend Facebook users who had “medical ex-
pertise” or “mutual health experiences” as compared to Healthy participants.
This however indicates that having poor health might encourage SNS users
to discuss their health issues with strangers, especially if those strangers had
expertise in the medical field or if they had mutual health experiences.
84

7.2 Implications for design
7.2.1 Search features
By exploring participants’ motivation to use a hypothetical search feature for
finding different Facebook users, we found that participants were more willing
to search for Facebook users who had mutual health experiences as compared
to users who had expertise in the medical field. Furthermore, while our results
showed that users with poor health status (Unhealthy) to be more willing to
share their HI with different user groups, we did not find statistically signifi-
cant difference in their willingness to use the search features when compared
to other user groups (Healthy or Manageable). Despite the reasons behind
participants’ motivation to use the search features, we believe that SNSs can
utilize users’ shared HI in order to provide automatic recommendations that
could facilitate finding the preferred user groups on behalf of users. In fact, our
results indicated that users were less sensitive toward revealing their health
conditions when creating their online anonymous identity. Therefore, it would
be possible for SNSs to utilize such information to perform automatic searches
for the purpose of recommending Facebook users who had mutual health ex-
periences or medical expertise.
7.2.2 Anonymous online identity
Using an anonymous online identity to share HI with strangers was considered
to be a preferable option for overcoming privacy concerns [4, 43]. Similarly
85

in our exploratory study (Section 5), patients considered using anonymous
identities to protect their privacy when talking about their health issues with
online users, especially strangers. We believe that providing the ability to
anonymously communicate HI on SNS can encourage SNS users, especially
privacy Pragmatists users, to engage in active HI sharing by regaining some
of the privacy that was surrendered when users disclosed their HI online. In
order to maintain anonymity, it is important for users to be able to hide their
contact, location, and identity information from other users. Furthermore,
we believe that SNSs can also benefit from patients’ low sensitivity towards
revealing their health conditions in order to facilitate HI sharing among users
and increase their interactions by offering them an option to use anonymous
online identities whenever needed.
7.2.3 Trusted SNS providers
Internet users’ trust in web-based service was shown to influence their moti-
vation to provide personal information to these online services [13, 24, 54].
In the context of sharing HI on SNSs, we identified a number of trusted SNS
providers, among which a “governmental health authority” was identified as
the most trusted SNS provider by participants. Furthermore, we found that
regardless of the SNS provider, participants’ were more likely to trust an SNS
with their HI if it was recommended by their doctors. Keeping that in mind,
we believe that SNSs providers, especially those specialized in HI sharing and
management, may benefit from doctors as intermediate channels for attract-
86

ing new users or increasing online interactions of existing users on their sites.
This however will require incentivizing, educating, and motivating doctors,
which might be a challenging but worthwhile process by itself.
87
Chapter 8
Conclusions
In this thesis, we quantified HI sharing practices on Facebook and showed that
despite the raised concerns, a considerable number of users were in fact shar-
ing their HI on SNSs. Furthermore, we employed qualitative and quantitative
instruments to investigate users’ motivation to share HI on Facebook. Our
results indicate that users’ prior HI sharing experiences, attitudes toward pri-
vacy, and perceived health status, are linked to their motivation to share HI.
In addition, we identified the key characteristics of the recipients that users
preferred to share their HI with. Armed with such an understanding, we dis-
cussed the opportunities of utilizing existing features in order to optimize the
gained benefits, while improving users’ privacy when sharing HI. Also, our re-
sults indicate that users’ health conditions could be used to facilitate HI shar-
ing on Facebook without compromising their online privacy. Finally, by hiding
Contact and location information, Facebook users’ can maintain some level of
88

anonymity and privacy when sharing HI with strangers.
In summary, this work makes the following main contributions:
• provide a better understanding of Facebook users’ HI sharing practices,
preferences, and risk perceptions,
• identify factors linked to users’ perceived privacy and motivation to share
HI on Facebook, and
• suggest design features that could facilitate effective HI sharing among
Facebook users.
89

Chapter 9
Future Work
As part of future work, we believe that it would be necessary to capture users’
actual HI sharing practices on Facebook while examining the influence of the
identified factors on users’ motivation to share HI. Furthermore, by imple-
menting and testing the user preferred features (e.g., anonymous identity),
we would like to enrich our understanding of the different factors that moti-
vate Facebook users’ toward sharing their HI with their social peers. Finally, it
is important to examine Facebook users’ HI sharing practices over a reasonable
period of time in order to capture the influence of their HI sharing experiences
on their privacy perceptions and motivation to share HI.
90

Bibliography
[1] CrowdFlower. URL www.crowdflower.com. Accessed: April 5, 2016. →pages 18
[2] Amazon Mechanical Turk. URL https://www.mturk.com/. Accessed: April5, 2016. → pages 18, 33
[3] Social media “likes” healthcare: From marketing to social business.PwC HRI Social Media Consumer Survey, 2012. URLhttp://download.pwc.com/ie/pubs/2012_social_media_likes_healthcare.pdf.→ pages 9
[4] S. A. Adams. Revisiting the online health information reliability debatein the wake of “web 2.0”: an inter-disciplinary literature and websitereview. International journal of medical informatics, 79(6):391–400,2010. → pages 85
[5] I. Altman. Privacy regulation: culturally universal or culturally specific?Journal of Social Issues, 33(3):66–84, 1977. → pages 19
[6] S. B. Barnes. A privacy paradox: Social networking in the united states.First Monday, 11(9), 2006. → pages 14
[7] T. Bodenheimer, K. Lorig, H. Holman, and K. Grumbach. Patientself-management of chronic disease in primary care. Jama, 288(19):2469–2475, 2002. → pages 51
[8] D. Boyd and N. Ellison. Social network sites: Definition, history, andscholarship. Journal of Computer-Mediated Communication, 13(1):210–230, October 2008. ISSN 10836101.doi:10.1111/j.1083-6101.2007.00393.x. URLhttp://dx.doi.org/10.1111/j.1083-6101.2007.00393.x. → pages 5, 6
91

[9] B. Bulgurcu. Understanding the Information Privacy-Related Perceptionsand Behaviors of an Online Social Network User. PhD thesis, The Facultyof Graduate Studies, Business Administration, University of BritishColumbia, August 2012. → pages 32
[10] J. A. Calandrino, A. Kilzer, A. Narayanan, E. W. Felten, andV. Shmatikov. ’you might also like:’ privacy risks of collaborativefiltering. In Proceedings of the 2011 IEEE Symposium on Security andPrivacy, SP ’11, pages 231–246, Washington, DC, USA, 2011. IEEEComputer Society. ISBN 978-0-7695-4402-1. doi:10.1109/SP.2011.40.URL http://dx.doi.org/10.1109/SP.2011.40. → pages 2, 8
[11] F. Chanchary and S. Chiasson. User Perceptions of Sharing, Advertising,and Tracking. In Eleventh Symposium On Usable Privacy and Security(SOUPS 2015). USENIX Association, 2015. → pages 9, 10, 65, 83
[12] K. Charmaz. Constructing Grounded Theory. SAGE publications, 2006.→ pages 3, 12, 37, 38, 40, 41
[13] V. Choudhury and E. Karahanna. The relative advantage of electronicchannels: a multidimensional view. Mis Quarterly, pages 179–200,2008. → pages 86
[14] S. Consolvo, I. E. Smith, T. Matthews, A. LaMarca, J. Tabert, andP. Powledge. Location disclosure to social relations: why, when, & whatpeople want to share. In Proceedings of the SIGCHI conference on Humanfactors in computing systems, pages 81–90. ACM, 2005. → pages 10, 65,83
[15] G. Cormode and B. Krishnamurthy. Key differences between web 1.0and web 2.0. First Monday, 13(6), 2008. → pages 5, 6
[16] M. De Choudhury, M. R. Morris, and R. W. White. Seeking and sharinghealth information online: Comparing search engines and social media.In Proceedings of the SIGCHI Conference on Human Factors in ComputingSystems, CHI ’14, pages 1365–1376, New York, NY, USA, 2014. ACM.ISBN 978-1-4503-2473-1. doi:10.1145/2556288.2557214. URLhttp://doi.acm.org/10.1145/2556288.2557214. → pages 9
92

[17] M. Duggan, N. B. Ellison, C. Lampe, A. Lenhart, M. Madden, L. Rainie,and S. Aaron. Social Media Update 2014. Pew Research Center,January 2015. → pages 55, 60, 71
[18] N. B. Ellison, C. Steinfield, and C. Lampe. The benefits of Facebook“friends:” social capital and college students’ use of online socialnetwork sites. Journal of Computer-Mediated Communication, 12(4):1143–1168, July 2007. ISSN 10836101.doi:10.1111/j.1083-6101.2007.00367.x. URLhttp://dx.doi.org/10.1111/j.1083-6101.2007.00367.x. → pages 55
[19] T. W. Feeley and K. I. Shine. Access to the medical record for patientsand involved providers: Transparency through electronic tools. Annalsof Internal Medicine, 155(12):853–854, 2011.doi:10.1059/0003-4819-155-12-201112200-00010. URL+http://dx.doi.org/10.1059/0003-4819-155-12-201112200-00010. → pages12
[20] S. Fox. Health topics. Pew Research Center Report, February 2011. →pages 107
[21] S. Fox. The social life of health information. Pew Research CenterReport, May 2011. → pages 6, 8, 20, 24
[22] S. Fox and M. Duggan. Health online 2013. Pew Research Center’sInternet and American Life Project, January 2013. → pages 1, 6, 12,20, 24
[23] S. Fox and M. Duggan. The Diagnosis Difference. Pew Research Center,November 2013. → pages 71, 83
[24] D. Gefen, E. Karahanna, and D. W. Straub. Trust and TAM in OnlineShopping: An Integrated Model. MIS Q., 27(1):51–90, Mar. 2003. ISSN0276-7783. URL http://dl.acm.org/citation.cfm?id=2017181.2017185. →pages 86
[25] R. Gross and A. Acquisti. Information revelation and privacy in onlinesocial networks. In Proceedings of the 2005 ACM Workshop on Privacy inthe Electronic Society, WPES ’05, pages 71–80, New York, NY, USA,2005. ACM. ISBN 1-59593-228-3. doi:10.1145/1102199.1102214. URLhttp://doi.acm.org/10.1145/1102199.1102214. → pages 2
93

[26] A. Hartzler, M. Skeels, M. Mukai, C. Powell, P. Klasnja, and W. Pratt.Sharing is caring, but not error free: Transparency of granular controlsfor sharing personal health information in social networks. In AMIAAnnual Symposium, volume 2011, pages 559–568, 2011. → pages 12
[27] C. Hawn. Take two aspirin and tweet me in the morning: how twitter,facebook, and other social media are reshaping health care. Healthaffairs, 28(2):361–368, 2009. → pages 8
[28] T. K. Houston and J. J. Allison. Users of internet health information:differences by health status. Journal of Medical Internet Research, 4(2),2002. → pages 8, 62, 83
[29] G. Iachello and J. Hong. End-user privacy in human-computerinteraction. Found. Trends Hum.-Comput. Interact., 1(1):1–137, 2007.ISSN 1551-3955. doi:http://dx.doi.org/10.1561/1100000004. → pages 14
[30] N. Kamal. Designing online social networks to motivate health behaviourchange. PhD thesis, University of British Columbia, 2013. → pages 7
[31] R. Kang, S. Brown, L. Dabbish, and S. Kiesler. Privacy attitudes ofmechanical turk workers and the us public. In Symposium on UsablePrivacy and Security (SOUPS), 2014. → pages 65
[32] H. Krasnova, S. Spiekermann, K. Koroleva, and T. Hildebrand. Onlinesocial networks: why we disclose. Journal of Information Technology, 25(2):109–125, 2010. → pages 46
[33] P. Kumaraguru and L. F. Cranor. Privacy indexes: a survey of Westin’sstudies. Technical report, Carnegie Mellon University, 2005. → pages 9,10, 59, 65, 83
[34] M. Kwasny, K. Caine, W. A. Rogers, and A. D. Fisk. Privacy andTechnology: Folk Definitions and Perspectives. In CHI’08 ExtendedAbstracts on Human Factors in Computing Systems, pages 3291–3296.ACM, 2008. → pages 10
[35] C. Lampe, N. Ellison, and C. Steinfield. A face(book) in the crowd:social searching vs. social browsing. In Proceedings of the 2006 20thanniversary conference on Computer supported cooperative work, CSCW’06, pages 167–170, New York, NY, USA, 2006. ACM. ISBN
94

1-59593-249-6. doi:http://doi.acm.org/10.1145/1180875.1180901. URLhttp://doi.acm.org/10.1145/1180875.1180901. → pages 55
[36] C. Lampe, N. B. Ellison, and C. Steinfield. Changes in use andperception of facebook. In Proceedings of the 2008 ACM conference onComputer supported cooperative work, CSCW ’08, pages 721–730, NewYork, NY, USA, 2008. ACM. ISBN 978-1-60558-007-4.doi:http://doi.acm.org/10.1145/1460563.1460675. URLhttp://doi.acm.org/10.1145/1460563.1460675. → pages 55
[37] R. Lazarus. Coping theory and research: Past, present, and future. FiftyYears of the Research and Theory of RS Lazarus: An Analysis of Historicaland Perennial Issues, pages 366–388, 1993. → pages 32
[38] R. Lederman, G. Wadley, J. Gleeson, S. Bendall, and M. ÁlvarezJiménez. Moderated online social therapy: Designing and evaluatingtechnology for mental health. ACM Trans. Comput.-Hum. Interact., 21(1):5:1–5:26, Feb. 2014. ISSN 1073-0516. doi:10.1145/2513179. URLhttp://doi.acm.org/10.1145/2513179. → pages 7
[39] R. C. Lefebvre and A. S. Bornkessel. Digital social networks and health.Circulation, 127(17):1829–1836, 2013. → pages 2, 5, 7
[40] Y. Li. Theories in online information privacy research: A critical reviewand an integrated framework. Decision Support Systems, 54(1):471–481, 2012. → pages 2, 46, 83
[41] Social Media Survey Report. Liquid Grids, May 2014. → pages 6
[42] F. Lupiáñez-villanueva, W. Lusoli, M. Bacigalupo, I. Maghiros,N. Andrade, and C. Codagnone. Health-related information as personaldata in Europe: Results from a representative survey in Eu27. Medicine2.0: Ethical and legal issues, confidentiality and privacy, 2011. → pages2, 7, 12, 36
[43] M. Merolli, K. Gray, and F. Martin-Sanchez. Methodological review:Health outcomes and related effects of using social media in chronicdisease management: A literature review and analysis of affordances.Journal of Biomedical Informatics, 46(6):957–969, 2013. → pages 1, 2,7, 85
95
[44] A. S. Moorhead, E. D. Hazlett, L. Harrison, K. J. Carroll, A. Irwin, andC. Hoving. A new dimension of health care: Systematic review of theuses, benefits, and limitations of social media for healthcommunication. J Med Internet Res, 15(4):e85, Apr 2013.doi:10.2196/jmir.1933. URL http://www.ncbi.nlm.nih.gov/pubmed/23615206.→ pages 2, 7, 8
[45] M. R. Morris, J. Teevan, and K. Panovich. What do people ask theirsocial networks, and why?: a survey study of status message q&abehavior. In Proceedings of the SIGCHI conference on Human factors incomputing systems, pages 1739–1748. ACM, 2010. → pages 9
[46] H. J. Oh, C. Lauckner, J. Boehmer, R. Fewins-Bliss, and K. Li.Facebooking for health: an examination into the solicitation and effectsof health-related social support on social networking sites. Computers inHuman Behavior, 29(5):2072–2080, 2013. → pages 1, 6, 8
[47] P. Ressler, Y. Bradshaw, L. Gualtieri, and K. Chui. Communicating theexperience of chronic pain and illness through blogging. Journal ofMedical Internet Research, 14(5):e143, 2012. → pages 12
[48] M. M. Skeels. Sharing By Design: Understanding and supporting personalhealth information sharing and collaboration within social networks. PhDthesis, University of Washington, 2010. → pages 1, 2, 7, 12, 20, 24, 107
[49] S. Torabi and K. Beznosov. Privacy Aspects of Health RelatedInformation Sharing in Online Social Networks. In USENIX Workshopon Health Information Technologies (HealthTech ’13). USENIXAssociation, August 2013. URLhttp://0b4af6cdc2f0c5998459-c0245c5c937c5dedcca3f1764ecc9b2f.r43.cf2.rackcdn.com/12452-healthtech13-torabi.pdf. → pages 6, 9
[50] B. Ur, P. G. Kelley, S. Komanduri, J. Lee, M. Maass, M. L. Mazurek,T. Passaro, R. Shay, T. Vidas, L. Bauer, et al. How does your passwordmeasure up? the effect of strength meters on password creation. InProc. USENIX Security, 2012. → pages 18, 55, 60
[51] M. Velden and K. El Emam. “not all my friends need to know”: aqualitative study of teenage patients, privacy, and social media. Journal
96

of the American Medical Informatics Association, 20(1):16–24, July2012. → pages 9, 12
[52] N. D. Weinstein. Perceived probability, perceived severity, andhealth-protective behavior. Health Psychology, 19(1):65, 2000. → pages8
[53] A. Woodruff, V. Pihur, S. Consolvo, L. Schmidt, L. Brandimarte, andA. Acquisti. Would a privacy fundamentalist sell their DNA for $1000...if nothing bad happened as a result? the westin categories, behavioralintentions, and consequences. In Symposium on Usable Privacy andSecurity (SOUPS), 2014. → pages 10
[54] N. Xiao, R. Sharman, H. Rao, and S. Upadhyaya. Factors influencingonline health information search: An empirical analysis of a nationalcancer-related survey. Decision Support Systems, 57:417–427, 2014. →pages 8, 62, 71, 83, 86
[55] A. L. Young and A. Quan-Haase. Information revelation and internetprivacy concerns on social network sites: a case study of facebook. InProceedings of the fourth international conference on Communities andtechnologies, pages 265–274. ACM, 2009. → pages 2, 8
[56] D. M. Zulman, K. M. Nazi, C. L. Turvey, T. H. Wagner, S. S. Woods, andL. C. An. Patient interest in sharing personal health record information:A web-based survey. Annals of Internal Medicine, 155(12):805–810,2011. doi:10.1059/0003-4819-155-12-201112200-00002. URL+http://dx.doi.org/10.1059/0003-4819-155-12-201112200-00002. → pages1, 7, 12
97

Appendix A
Supplementary Materials for the
Preliminary User Study
The study was reviewed and approved by UBC’s BREB. Participants also re-
viewed the recruitment ad before answering the questionnaire on the study
webpage. After reviewing the study related information, participants had to
submit their information and consent to participate in the study. Note that
while the terms “health information” (HI) and “social networking sites” (SNSs)
were used throughout the research, the terms “health related information”
(HRI) and “online social networks” (OSNs) were used interchangeably to re-
fer to the same terms in the first study only (as reflected in the supplementary
materials in Appendix A).
98

!
Sharing!Health!Related!Information!on!Online!Social!Networks:!Risk!
Perceptions!and!Behavioural!Responses!
!
Introduction:!
This!is!an!exploratory!study!to!understand!users’!privacy!risks!perceptions!when!sharing!health!related!information!(HRI)!on!online!social!networks!(OSNs).!
Principal!Investigator:!
The!principal!investigator!of!this!research!is!Dr.!Konstantin!Beznosov!from!the!Department!of!Electrical!
and!Computer!Engineering!at!the!University!of!British!Columbia.!You!can!contact!him!at!beznosov@ece.ubc.ca!or!(604)!822!9181.!
Co5Investigator(s):!
Sadegh!Torabi,!Ph.D.!Student!! ([email protected])!
The!coXinvestigator!is!from!the!Department!of!Electrical!and!Computer!Engineering!at!UBC.!You!can!contact!him!at!604!827!3410.!
Terms!and!definitions:!
In!this!study,!you!will!encounter!a!number!of!terms!that!you!should!be!familiar!with!before!answering!the!questions:!
• Health'related'information'(HRI):!It!is!a!general!term!that!refers!to!any!information!that!is!
directly!or!indirectly!related!to!one’s!health.!This!information!includes!but!is!not!limited!to!the!
following:!diet!related!information,!prescriptions,!exercise!routines,!symptoms,!healthier!life!
choice/practices,!mental!or!physical!health!status,!and!chronic!disease!information.!
!
• Online'social'network'(OSN):!Online!social!networks!are!defined!as!webXbased!services!that!are!used!by!individuals!to!get!in!touch!with!other!online!peers.!The!common!features!of!every!OSN!
are!the!ability!for!users!to:!(1)!create!and!maintain!a!profile,!(2)!add/delete!online!peers!and!
finally,!(3)!interact!with!online!peers!through!existing!services.!Examples!of!wellXknown!OSNs!are:!
Facebook,!Twitter,!LinkedIn,!PatientsLikeMe,!Yahoo!messenger,!Skype,!Instagram,!and!Google+.!!
!
• Active'OSN'user:!an!active!OSN!user!is!a!person!who!maintains!at!least!one!OSN!profile!and!uses!
the!service!to!share/seek!information!with/from!online!peers!on!regular!basis.!
!
!
!
! ! T H E ! U N I V E R S I T Y ! O F ! B R I T I S H ! C O L U M B I A !
!
99

!
Purpose:!
The!purpose!of!the!study!is!to!investigate!OSN!users’!HRI!sharing!behaviour,!along!with!their!perceived!privacy!risks!and!triggered!behavioural!responses!in!the!presence!of!privacy!risks.!!
Study!Procedures:!
You!will!take!part!in!an!online!survey!about!your!OSN!information!sharing!behaviour,!perceived!privacy!
risks!and!corresponding!behavioural!responses.!The!online!survey!will!take!approximately!30!minutes.!During!this!survey,!you!will!be!asked!questions!regarding!your!information!sharing!activities!on!OSNs.!
Confidentiality:! !
Your!identifiable!information!will!not!be!collected!and!therefore,!your!identity!will!remain!anonymous!
throughout!the!study.!All!data!will!be!kept!confidential,!and!your!anonymity!will!be!protected!in!any!
reports,!research!papers,!and!presentations!that!result!from!this!study.!
Remuneration/Compensation:!
We!would!like!to!thank!you!and!inform!you!that!as!a!result!of!participating!in!this!online!survey!study,!you!will!be!compensated!with!the!amount!of!$1!(USD)!through!Amazon!Mechanical!Turk.!
Contact!for!information!about!the!study:!
If!you!have!any!questions!or!require!further!information!about!the!project!you!may!contact!Sadegh!Torabi!at!+1!604!827!3410.!
Contact!for!concerns!about!the!rights!of!research!subjects:!
If!you!have!any!concerns!about!your!treatment!or!right!as!a!research!subject,!you!may!contact!the!
Research!Subject!Information!Line!in!the!UBC!Office!of!Research!Services!at!604!822!8598!or!eXmail!rsil@ors.ubc.ca.!
Consent:!
Your!participation!in!this!study!is!entirely!voluntary!and!you!may!refuse!to!participate!or!withdraw!from!the!study!at!any!time.!By!selecting!the!“Agree”!option!below!you!indicate!the!following:!
i) You!are!19!years!and!older,!!
ii) You!are!an!Active!OSN!user!who!maintains!at!least!one!OSN!profile!and!uses!the!service!to!
share/seek!information!and!connect!to!other!online!peers!regularly,!and!
iii) You!have!read!and!understood!the!provided!information,!and!that!you!consent!to!participate!in!this!study![you!can!print!or!save!a!copy!of!this!consent!form!for!your!records].!
!
!
!
!
Agree! Decline!
100

A.1 Survey Questions
A.1.1 Questions About Participants’ Demographics
1. Gender:
• Male
• Female
2. How old are you?
(19 to 99) years old
3. What is your highest level of completed education?
• Less than high school
• High school (secondary school)
• Diploma (post-secondary courses)
• Undergraduate university degree (Bachelor’s)
• Graduate university degree (Masters’s or PhD)
• Community college or professional school (College degree)
• Other (please specify)
4. Employment category: [Select a category that best fits your current job]
• A range of employment categories (e.g., Education, Business, Engi-
neering, ...), or
101

• Other (please specify)
5. Current country of residence?
• Select from list, or
• Other (please specify)
A.1.2 Questions About SNS Usage
1. How many active SNS profiles do you maintain? [Active accounts are
those which you regularly use to connect to people, share information,
and perform online activities]
• 1
• 2
• 3
• 4
• 5 or more
2. For your most frequently used SNS account(s), provide the name of the
SNS and specify how regularly do you log into your account. [Informa-
tion for at least one SNS is required, you may skip the rest if does not
apply]
The following questions will be repeated for each specified active SNS
account:
102

• SNS name [Select from list, or specify other SNS names]
• How regularly do you log into your above SNS account?
– Daily
– Weekly
– Monthly
– Every few months
– Other
• Select the device that you use the most to connect to the specified
SNS account.
– Personal Computer/Laptop/Desktop
– Tablet (e.g., iPad)
– Smartphone (e.g., iPhone)
– Other (please specify)
A.1.3 Questions About HI Sharing Behaviours in SNSs
1. For each HI category, how often do you share information in SNSs? [The
survey presented 8 HI categories with corresponding responses in the
form of a 5-point Likert scale with anchor points specified as: never,
sometimes, and always]
• Refer to Table A.1 for HI categories.
103

2. Specify other types of HI that you share and do not appear in the above
list.
3. Why do you share your HI in SNSs? [Select all that apply]
• Help others by sharing personal experience and knowledge
• Get benefits by receiving useful feedback from online contacts
• Seek help or social support
• Alleviate anxiety (Sharing HI makes me feel better and less stressed)
• Seek online interactions and make discussions
• Promote healthy living
• Other (please specify)
4. For HI that you do not share in SNSs, describe your choice by selecting
all reasons that apply from below.
• I do not want to be treated as “the sick” person by my online con-
tacts
• I do not want my online contacts to worry about me by receiving
bad news about my health
• I have different people in my online contact list and I prefer not to
share my HI with all of them
• My HI is personal and I do not share it with anyone
• I prefer to share my HI with my doctor
104

• I do not want my online contacts to know about my HI
• My online contacts are not interested in my HI
• I prefer to share my HI offline
• Other (please specify)
A.1.4 Questions About Privacy Risk Perceptions andBehavioural Responses
1. When sharing HI in SNSs, how much each of the following factors con-
tribute to the increase of your perceived privacy risks: [Responses vary
on a 5-point Likert scale with anchor points specified as: does not affect,
slightly affects, and strongly affects]
• The receiver(s) of the HI
• HI type and category
• The SNS platform where the HI is shared
• Your current physical or mental health condition (e.g., depressed,
healthy, suffer from chronic pain, etc.)
2. For every HI category (Table A.1), how do you evaluate your perceived
privacy risk level when sharing HI with the given four user categories:
• Select individual(s)
• Select group(s)
• Your entire contact list
105

• All other SNS users
[Select the perceived privacy risk level from a 5-point Likert scale with
anchor points: very low (or none), moderate, and extreme]
3. “Behavioural responses” refer to different actions undertaken by an in-
dividual to mitigate the perceived privacy risks.
Assume you want to share some HI in SNS: For each assumed privacy
risk level (very low, acceptable, moderate, high, extreme), what would
be your preferred behavioural response(s)? [select all that apply for
each risk level]
• Avoid risks by not sharing HI
• Minimize risks by manipulating shared HI (e.g., change or remove
personal and identifiable information)
• Minimize risks by filtering recipients (e.g., share with specific indi-
vidual(s) or group(s))
• Minimize risks by changing the used SNS (e.g., share HI in other
trusted SNS)
• Accept risks and share HI without any preemptive actions
106

A.2 Categorization of HI examples
Prior to conducting our survey, we reviewed the literature and found more
than 30 different examples of HI that people often shared online [20, 48].
They include but not limited to the following: mental or physical conditions,
healthy eating and dietary information, daily exercise routines, experience
with a specific doctor, previous surgeries, symptoms and side effects, insur-
ance company information, useful online articles, information about children
and elderly family members. We categorized the identified examples of HI
sharing according to their similarities and characteristics. To triangulate the
categorization, we used an online card sorting tool (OptimalSort)1 to run a
closed card sorting exercise, where we asked 11 participants, mostly friends
and colleagues, to group different HI examples into the predefined 8 cate-
gories. Seven participants grouped over 75% of the HI examples into cate-
gories similar to our predefined ones. Participants’ feedback was also incorpo-
rated toward refining/rephrasing the HI categories and the given HI examples
in order to avoid further ambiguity in the survey questionnaire and study ma-
terials. The finalized HI categories are presented in Table A.1.
1www.optimalworkshop.com
107

Table A.1: HI categories and examples.
Category HI Examples
Healthy livingdietary and healthy eating, physical exercise,
mental exercise
Own experienceexperience with: previous surgeries, treat-
ments, and symptoms
Useful found information books, articles, websites
Mental and emotional
health conditionsstressed, excited, depressed
Physical health conditions sick, injured, in good shape
Medical health recordspersonal information and address, physician
information, insurance policy, x-rays, reports
Experience of somebody
else
experience with: previous surgeries, treat-
ments, and symptoms
HI of people in your custody parents, children, and others
108

Appendix B
Supplementary Materials for the
Exploratory Study (Interviews)
The study was reviewed and approved by UBC’s BREB. Participants also re-
viewed the recruitment ad before sending their participation request through
the study webpage. After reviewing the study related information, participants
had to submit their information and consent to participate in the study.
109

! Recruitment!page,!v1.2!!!!!29/11/2013!1!
Sharing Health Related Information In Online Social Networks The purpose of this exploratory research is to investigate different aspects of sharing health related information (HRI) in online social networks (OSNs). While most people consider HRI to be private and personal in nature, recent studies showed increasing number of users who shared information about their health in OSNs (e.g., Facebook). In fact, sharing HRI is becoming a new application of OSNs. Whether if it is for the gained benefits of sharing HRI, or simply to help others and provide social support, there is a lack of understanding about different aspects of sharing HRI in OSNs.
How to participate? Your participation is important for our research. You will be interviewed about your opinions, thoughts, and experiences when using OSNs (e.g., Facebook). If you have one or more chronic health condition(s) (e.g., spinal cord injury), or you are a caregiver who provides healthcare support to an individual with chronic health condition(s), then you can participate in this study by clicking on the “Participate” button below:
Compensation: $25 per interview (approximately 1 hour)
* For further inquiries, email us at: [email protected]
110

! Study!Participation!Request!page,!v1.3!!!!!10/01/2014!1"
!!
Study Participation Request
Please review the following information carefully and provide your consent by clicking on "Submit" button at the end of the page
Principal Investigator The principal investigator of this research is Dr. Konstantin Beznosov from the Department of Electrical and Computer Engineering at the University of British Columbia. You can contact him at [email protected] or (604) 822 9181. Co-Investigator Sadegh Torabi ([email protected]) The co-investigator is a PhD student from the Department of Electrical and Computer Engineering at UBC. You can contact him at 604 827 3410. Purpose The purpose of this exploratory user study is to address the lack of understanding about different aspects of health related information (HRI) in online social networks (OSNs). While most people consider HRI to be private and personal in nature, recent studies showed increasing number of users who shared information about their health in OSNs. In fact, sharing HRI is becoming a new application of OSNs. Whether if it is for the gained benefits of sharing HRI, or simply to help others and provide social support, there is a lack of understanding about the privacy aspects of sharing HRI in OSNs. We will interview individuals with similar health conditions (e.g., spinal cord injury patients) to identify privacy and usability requirements. We will eventually suggest a set of privacy-preserving guidelines that could be used by OSN designers and application developers to enhance HRI sharing experience in OSNs. Study Procedures In this study, we will collect qualitative data by means of individual interviews. As a person with chronic health condition(s) (e.g., spinal cord injury), or a caregiver who is providing healthcare support for an individual with chronic health condition(s), you will take part in an individual interview about your OSN usage, online information sharing behaviours, health condition and health management activities, perceived privacy risks, and corresponding behavioural responses. The interview will be conducted in a mutually convenient time and location. It will last approximately 60 minutes, and with your permission, it will be audio-recorded and transcribed. The interview will also include the collection of some demographic 111

! Study!Participation!Request!page,!v1.3!!!!!10/01/2014!2"
information (e.g., age, gender, education, etc.) through a designated online form, or by completing a printed version of the form upon request. A follow-up telephone call or email communication may be necessary to clarify issues arising from the discussion. Confidentiality All information will be kept strictly confidential. To ensure complete anonymity, pseudonyms (false names) will be substituted for your real name and the names of anyone else mentioned in the interview discussion. All stored media, transcripts and consent forms will be identified by code and kept in a locked filing cabinet in the project office. The only people that will hear the recorded interviews and/or see the transcripts will be the Principal investigator (Dr. Konstantin Beznosov), the Co-Investigator (Sadegh Torabi), and the transcriptionist. The information gained from this research will be anonymized and written up in publications and/or reports and will be shared with interested parties. You may request copies of these publications or reports about the findings of the study. The recorded interviews will be destroyed 5 years after publication of the original analysis and findings. Compensation, Benefits, and Potential Risks Your participation is important for our research. As a result of participating in this research, you will be compensated with the amount of $25 (CAD). Also, there might be some other benefits to you as a result of participating in this research, as discussion with others about your thoughts and experiences may help you to clarify your own thinking. Moreover, the outcomes of the study may help increase the awareness and gained knowledge about the studied topic. There might be some potential risks related to involvement in this research. It is possible that some topics discussed in the interview may raise new and/or previous emotional issues but you need only answer questions or express your views when you wish to do so. The investigator(s) will be respectful of your preferences. However, the investigator(s) are not equipped to provide counseling or professional advice. Contact for information If you have any questions or require further information about the project, you may contact the co-investigator (Sadegh Torabi at +1 604 827 3410). If you have any concerns about your treatment or right as a research subject, you may contact the Research Subject Information Line in the UBC Office of Research Services at 604 822 8598 or e-mail [email protected].
112
! Study!Participation!Request!page,!v1.3!!!!!10/01/2014!3"
Consent
It is very important that your participation in this study is entirely voluntary and based on clear understanding. Furthermore, you may refuse to participate or withdraw from the study at any time. By clicking on the “Submit” button below you accept to participate in this study and indicate the following:
1. You are 19 years and older, 2. You are living in the Greater Vancouver region, 3. You maintain at least one active OSN account that you use
regularly, 4. You have one or more chronic health conditions (e.g., spinal cord
injury), or you are a caregiver who provides healthcare support to an individual with chronic health condition(s),
5. Your participation in this study is entirely voluntary and you may refuse to participate or withdraw from the study at any time without giving a reason and without any negative impact on received benefits and compensation, and
6. You have read and understood the provided information, and you consent to participate in this study [you can print or save a copy of this consent form for your records].
Provide your Name and Contact information and submit your request [Required fields are marked with * ] By clicking on "Submit" button below, you consent to participate in this study. Your contact information will be recorded and you will be contacted shortly. *"Name: " *"Email: " Phone: "
!
113

B.1 Interview guide and questions
Will collect qualitative data by means of semi-structured interviews. The inter-
view lasted between 60-90 minutes, and were audio-recorded and transcribed.
The interviews started by reviewing the consent form and the collection of
demographic information (age, gender, education, etc.). Then, a number of
research-related questions were asked, as shown in the following subsections.
A follow-up telephone call or email communication was made when neces-
sary to clarify issues arising from the discussion. The interview questions are
presented as following:
B.1.1 Health condition background
• What is the health condition you have?
• How/When did the health condition appeared or started the first time?
• How does the health condition affect your daily life?
• What are the challenges that you face due to the health condition you
have?
• How does the health condition you have affect your social life?
• Is there anything specific about your health condition that is of your
concern?
114

B.1.2 Health management
• How do you manage your health condition?
• How others (if any) are involved in your health management process?
• What is your relationship with doctors, physicians, and nurses?
• Do you have any concerns regarding your health management?
B.1.3 SNS usage and background
• How many SNS accounts do you maintain?
• How often do you log into your SNS accounts and what do you usually
do there?
• Who do you connect to using the SNSs? Who are your online friends?
• What do the SNS environments mean to you (e.g., Facebook)?
B.1.4 HI sharing on SNSs
• Have you ever shared HI in your SNSs? Why?
• Whom do you usually share your HI with?
• How do you think sharing HI could be helpful/beneficial to you or others
in your social network?
• When it comes to sharing HI, do you have specific preferences about the
type of the SNS where you share your HI in? Why?
115

• How do you think about existing privacy settings in SNSs?
B.1.5 A specialized SNSs for managing health conditions
• Have you ever considered using an SNS to manage, share, and seek HI?
• What do you expect from a specialized SNS that is used to help you
manage your health conditions and get connected to others?
• How do you define your privacy?
B.1.6 Study related feedback
Do you have any comments, suggestions or concerns related to this study? We
appreciate your constructive feedback?
B.2 Supplementary results
Participants came with different health issues. Nine participants suffered from
chronic pain and arthritis in different parts of their body. We interviewed two
quadriplegic participants with limited physical mobility, among whom one had
also suffered from chronic lung and heart diseases. We also interviewed an
HIV positive patient, who was infected as a results of an accidental needle
poke while doing his job as a paramedic. Finally, one participant had Neu-
romyelitis Optica (NMO), which is a rare disease that attacks the central nerve
system and causes blindness, paralysis, and other health issues. The remaining
participants suffered from a combination of mental and/or physical illnesses
116

(e.g., eating disorder and depression, arthritis and lung disease). More details
about participants’ health conditions are presented in Table B.1.
117

Table B.1: Participants demographics and health conditions. The firstcolumn represents participants’ ID.
ID Gender Age Health condition(s)
P1 M 38 chronic sciatica due to an accident
P2 M 59 back fracture and defective left knee
P3 M 31 severe arthritis in right hand due to a car accident
P4 F 68C4-C5 incomplete quadriplegic due to damaged
neck in a sport accident
P5 F 30 chronic depression
P6 F 21 curved spine and chronic back pain
P7 M 54C5-C6 quadriplegic due to a motor accident, and
chronic heart/lung disease
P8 M 38 chronic back pain
P9 F 42Neuromyelitis optica (NMO), episodes of blindness,
headaches, and fatigue
P10 M 37 osteoarthritis (deformed leg) and defective knee
P11 M 40L3-L4 fusion due to a work-related accident and
COPD (lung problem)
P12 M 59degenerative disk and brain injury (lost senses of
balance, taste, and smell)
P13 M 51 osteoarthritis in all joints
P14 F 39 eating disorder and post-traumatic stress disorder
P15 M 37 bipolar depression and anxiety
P16 M 48 post-traumatic stress disorder
P17 M 48 arthritis in hands and knees
P18 F 38degenerative arthritis in foot and ankle, anemia,
and depression
P19 M 50 HIV due to an accidental needle poke
P20 M 50 depression and chronic pain from broken neck
P21 F 35 herniated disks (L4-L5) with chronic pain
118

Appendix C
Supplementary Materials for the
Confirmatory Study (Online
Survey)
The study was reviewed by UBC’s BREB and a certificate of approval was
issued. To take part in the study, participants reviewed the recruitment ad
through MTurk and reviewed the study related information. Participants were
required to consent to participate in the online survey before answering survey
questions.
119

Online&recruitment&flyer&&Version&1&&&204Sept42015&&1&
Sharing Health Information on Social Networking Sites
The Department of Electrical and Computer Engineering at University of British Columbia invites participants for a study on health information sharing behaviours on Facebook.
We require volunteers to participate in our online survey that takes no more than 30 minutes. All participants will receive the amount of 1 US dollar through Amazon Mechanical Turk.
The study requires the participant to satisfy the following conditions: (1) you must be 19 years and older; and (2) you must be an active Facebook user, that is a person who maintains a Facebook profile and uses the service to share/seek information with/from online contacts regularly.
If you would like to participate in this study, please follow the link below:
https://survey.ubc.ca/surveys/sadeq/phealth-v1-pilot/ For further information, please contact us at [email protected]
&
!!The!University!of!British!Columbia! !
120

! Consent!Form!v2!!!!!!02.Oct.2015!1!
Sharing(Health(Information(on(Social(Networking(Sites((University(of(British(Columbia(>(Department(of(Electrical(and(Computer(Engineering)(
(Introduction:(This( is( a( study( to( understand( users’( perceptions( when( sharing( health(information((HI)(in(social(networking(sites((SNSs).((Principal( Investigator:(The(principal( investigator(of( this( research( is(Dr.(Konstantin(Beznosov(from( the( Department( of( Electrical( and( Computer( Engineering( at( the( University( of( British(Columbia.(You(can(contact(him(at([email protected](or((604)(822(9181.((Co>Investigator(s):( Sadegh( Torabi,( MSc.( Student( ([email protected])( The( co>investigator( is(from(the(Department(of(Electrical(and(Computer(Engineering(at(UBC.(You(can(contact(him(at(604(827(3410.((Terms(and(definitions:(In(this(study,(you(will(encounter(a(number(of(terms(that(you(should(be(familiar(with(before(answering(the(questions:((((((Health(information((HI):(It(is(a(general(term(that(refers(to(any(information(that(is(directly(or(indirectly( related( to( one’s( health.( This( information( includes( but( is( not( limited( to( the(following:(diet(related(information,(prescriptions,(exercise(routines,(symptoms,(healthier(life(choice/practices,(mental(or(physical(health(status,(and(chronic(disease(information.((((((((Social(networking(sites((SNSs):(Social(networking(sites(are(defined(as(web>based(services(that(are(used(by(individuals(to(get(in(touch(with(other(online(peers.(The(common(features(of(every(SNSs(are(the(ability(for(users(to:((1)(create(and(maintain(a(profile,((2)(add/delete(online(peers(and(finally,((3)(interact(with(online(peers(through(existing(services.(Examples(of(well>known(SNSs(are:(Facebook,(Twitter,(LinkedIn,(PatientsLikeMe,(and(Google+.((((((((Active(SNS(user:(an(active(SNS(user( is(a(person(who(maintains(at( least(one(SNS(profile(and(uses(the(service(to(share/seek(information(with/from(online(peers(on(regular(basis.(((((Study(Purpose:(The(purpose(of( the(study( is( to( investigate(SNSs(users’(HI( sharing(behaviors,(perceived(benefits,(and(risk(perceptions.((Study( Procedures:( You(will( take( part( in( an( online( survey( about( health( information( sharing(behaviors(in(SNSs.(The(online(survey(will(take(approximately(30(minutes.(During(this(survey,(you( will( be( asked( questions( regarding( your( health( information( sharing( practices( and(preferences( in(SNSs.(You(will(be(also(asked(questions(about(your(health(status(while( listing(any(health(conditions(that(you(currently(have.((Confidentiality:( Your( identifiable( information( will( not( be( collected( and( therefore,( your(identity(will(remain(anonymous(throughout(the(study.(All(data(will(be(kept(confidential,(and(your( anonymity( will( be( protected( in( any( reports,( research( papers,( and( presentations( that(result( from( this( study.( Finally,( this( study( is( a( part( of( a( graduate( study( project( for( Sadegh(Torabi(and(the(results(might(be(used(in(his(final(graduate(thesis.(
( ( T H E ( U N I V E R S I T Y ( O F ( B R I T I S H ( C O L U M B I A (
(
121
! Consent!Form!v2!!!!!!02.Oct.2015!2!
(Remuneration/Compensation:(We(would(like(to(thank(you(and(inform(you(that(as(a(result(of(participating( in( this( online( survey( study,( you(will( be( compensated(with( the( amount( of( $1((USD)(through(Amazon(Mechanical(Turk.((Contact( for( information( about( the( study:( If( you( have( any( questions( or( require( further(information(about(the(project(you(may(contact(Sadegh(Torabi(at(+1(604(827(3410.((Contact( for( concerns( about( the( rights( of( research( subjects:( If( you( have( any( concerns( or(complaints( about( your( rights( as( a( research( participant( and/or( your( experiences( while(participating(in(this(study,(contact(the(Research(Participant(Complaint(Line(in(the(UBC(Office(of(Research(Ethics(at(604>822>8598(or(if(long(distance(e>mail([email protected](or(call(toll(free(1>877>822>8598.(!
CONSENT(Your( participation( in( this( study( is( entirely( voluntary( and( you(may( refuse( to( participate( or(withdraw(from(the(study(at(any(time.(By(selecting(the(“Agree”(option(below(you(indicate(the(following:((((((
• You(are(at(least(19(years(old,((((((• You(maintain(a(Facebook(account(that(you(use(regularly,(and((((• You(have(read(and(understood(the( information(provided(on(previous(page,(and(that(
you(consent(to(participate(in(this(study([you(can(print(or(save(a(copy(of(this(consent(form(for(your(records].(
!
! Agree!
! Decline!(Exit!survey)!!
122

C.1 Survey questionnaire
By volunteering to take part in this study, participants declare that they are at
least 19 years old and that they maintain an active Facebook profile that they
visit regularly. To complete the survey, participants were required to answer
the following questions:
1. What is your gender?
• Male
• Female
• Decline to answer
2. How old are you: [Select from list between 19 and 99]
3. What is your highest level of completed education?
• Less than High School
• High school (secondary school)
• Some college/university courses
• Diploma (post secondary courses)
• Undergraduate University degree (Bachelor’s)
• Graduate University degree (Masters’s or PhD)
• Other (Please specify)
123

4. What is your employment category?
• Administrative support (e.g., secretary, assistant)
• Art, writing, or journalism (e.g., author, reporter)
• Business, management, or financial (e.g., manager, accountant,
banker)
• Computer engineer or IT professional (e.g., systems administrator,
programmer, IT consultant)
• Education (e.g., teacher)
• Engineer in other fields (e.g., civil engineer, bio-engineer)
• Legal (e.g., lawyer, law clerk)
• Medical (e.g., doctor, nurse, dentist)
• Scientist (e.g., researcher, professor)
• Service (e.g., retail clerks, server)
• Skilled labor (e.g., electrician, plumber, carpenter)
• Student
• Unemployed
• Other (Please specify)
5. What is your current country of residence? [Select from the list]
• United States of America
124

• Canada
• Afghanistan
• ... Additional choices hidden ...
• Zimbabwe
• Other
6. Do you have a college degree or work experience in computer science,
software development, web development or similar computer/IT related
fields?
• Yes
• No
• I don’t know
7. Approximately how many hours do you spend on the Internet each day?
[Select between 0 and 24 hours]
8. When did you start using Facebook? [Select between 2004 and 2016]
9. How often do you check your Facebook?
• At least once a day
• At least once a week
• Every month
• Less often than every month
125

• Don’t use it at all
10. Please check your Facebook profile and tell us how many friends you
have on Facebook?
11. How do you describe your Facebook friends? [Select all that applies]
• Family members and relatives
• Offline friends (e.g., childhood friends, school friends)
• My friends’ friends (online and offline)
• Colleagues and co-workers
• People whom I met online for the first time (e.g., people with com-
mon interests)
• Celebrities and public figures
• People with specific expertise/profession (e.g., lawyers, doctors,
engineers)
• Others (please specify)
12. Do you currently suffer from any chronic health conditions? [Please
select all that applies]
• Allergies
• AIDS/ HIV
• Asthma
126

• Heart disease
• Stroke
• Cancer
• Diabetes
• Arthritis and chronic pain
• Eating disorder
• Obesity
• Stress
• Depression
• Anxiety
• None
• Others (please specify)
13. How long have you had the above mentioned health conditions (if any)?
• I don’t have any chronic health conditions
• Less than a year
• About two years
• About three years
• About four years
• More than four years
127

14. In general, would you say your health is:
• Poor
• Fair
• Good
• Excellent
15. Have you ever joined health-related social networking sites?
• Yes
• No
• I don’t know
16. Why did you join the health-related social networking sites?
17. Are you still using the health-related social networking sites?
• Yes
• No
• I don’t know
18. If you are not using the health-related social networking site anymore,
then why did you decide to do so? [Type "NA" if you are still using the
health-related social networking sites]
128

19. Have you ever shared details of your health information with anyone of
the following people on Facebook? [Select all that applies]
• Everyone on my Facebook friends list
• Some close friends or family members
• Select friends who had medical expertise and/or mutual health ex-
periences
• Other Facebook users (Non-friends) who had medical expertise and/or
mutual health experiences
• No one (Never shared my health information with others on Face-
book)
• Other people (Please specify)
20. Why did you share (or didn’t share) your health information on Face-
book?
21. How do you evaluate your prior experience with sharing your health
information on Facebook?
• Positive
• Negative
• Both positive and negative
• Neither positive nor negative
129
• I don’t know or does not apply to me
22. What was positive and/or negative about your prior experience of shar-
ing your health information on Facebook? [Leave blank if does not apply
to you]
23. How likely would you share details of your health information with other
people on Facebook? [Participants are asked to rate their response on a
5-points likert scale with responses varying from “Very Unlikely” to “Very
Likely”]
24. What might motivate you to use Facebook for sharing your health infor-
mation details with other people? [Please select all that applies]
• My previous positive experiences
• Lack of knowledge about my health issues (if any)
• My passion to help others by sharing my health-related experiences
with them
• The need to learn from other people’s expertise and experiences
• Facebook provides me with the ability to hide my personal infor-
mation and real identity from others
• Seeking social support
• Facebook can help me find other people with similar health issues
130

• Facebook helps me to communicate with other people without hav-
ing to meet them in real life
• Nothing motivates me to share my health information on Facebook
• Other (Please specify)
25. What might stop you from using Facebook to share your health informa-
tion details with other people? [Please select all that applies]
• My previous negative experiences
• I don’t see any benefits of sharing my health information with oth-
ers
• I am a healthy person and I do not have anything to say about my
health
• My health issues are personal and I do not want to share them with
other people on Facebook
• Others don’t understand my health conditions
• I don’t have any Facebook friends that have expertise and/or expe-
riences in the medical field
• I don’t want others to worry about my health
• I have different people on my Facebook and I prefer not to talk
about my health to all of them
• My health condition(s) are completely manageable
131

• I don’t like to cry for help or feel week, my friends might misunder-
stand me
• I don’t feel protected online, my shared information might be mis-
used against me
• Other (Please specify)
26. I would consider sharing my health information details with the follow-
ing Facebook users: [For each user group, participants must rate their
response on a 5-points likert scale with responses varying from “Strongly
disagree” to “Strongly agree”]
• All my Facebook friends
• Some close friends and/or family members
• Friends and/or family members who might have medical expertise
and/or mutual health experiences
• Other Facebook users (Non-friends) who might have medical ex-
pertise and/or mutual health experiences
27. Facebook provides a “search” feature that can help you in finding people
with specific interests, expertise, and/or experiences. Suppose that you
have a chronic health condition, how likely would you use the “search”
feature to find people with: [For each user group, participants must rate
their response on a 5-points likert scale with responses varying from
“Very Unlikely” to “Very Likely”]
132

• Expertise in the medical field (e.g., Doctors, nurses, health profes-
sionals)
• Mutual health experiences (e.g., people with similar health condi-
tions)
28. Suppose that Facebook allows you to create an anonymous online iden-
tity. How likely would you use an anonymous online identity if you want
to share your health information with other people on Facebook? [Par-
ticipants are asked to rate their response on a 5-points likert scale with
responses varying from “Very Unlikely” to “Very Likely”]
29. Why would you use (or not use) an anonymous online identity when
sharing your health information on Facebook?
30. Suppose you want to create an anonymous identity in order to share
your health information with strangers on Facebook. How likely would
you “hide” each of the following personal information? [For each item,
participants must rate their response on a 5-points likert scale with re-
sponses varying from “Very Unlikely” to “Very Likely”]
• First name
• Last name
• Identifiable profile picture
• Residential address
133
• City where I live
• Occupation and employment information
• Hobbies and interests
• Current location information (e.g., I am in "restaurant name" now)
• Future location information (e.g., I will be in "restaurant name" at
6 PM)
• My health condition(s)
• Email address
• Phone number
• Age and date of birth
• Gender
31. In general, I would trust a social networking site with my health infor-
mation if it is operated/owned by: [For each provider, participants must
rate their response on a 5-points likert scale with responses varying from
“Strongly disagree” to “Strongly agree”]
• A governmental agency (non-health related)
• A governmental health authority (e.g., city, state/province, feder-
al/national)
• A recognized private company
134

32. In general, I would trust a social networking site with my health in-
formation if it is recommended by: [For each group, participants must
rate their response on a 5-points likert scale with responses varying from
“Strongly disagree” to “Strongly agree”]
• My close friends and/or family members
• Friends who might have medical expertise
• Friends who might have mutual health experiences
• My doctor(s)
33. Please rate your level of agreement with each given statement below [4-
points likert scale with the given responses: “Strongly disagree”, “Some-
what disagree”, “Somewhat agree”, and “Strongly agree”]
• Internet users have lost all control over how personal information
is collected and used by social networking sites
• Most social networking sites handle the personal information they
collect about consumers in a proper and confidential way
• Existing laws and organizational practices provide a reasonable
level of protection for internet users’ privacy today
34. Have you ever performed any of the following actions on Facebook?
[For each action, participants must answer with “Yes”, “No”, or “I don’t
know”]
135

• Modified the privacy settings to specify the people who can see your
photos, likes, comments, and other posts
• Deleted some shared photos, comments, and/or other posts
• Changed profile visibility (profile information that others can see)
• Hid your friends’ list from other Facebook friends
• Modified the privacy settings to specify the people who can post on
your Timeline
• Deleted and/or blocked friends
• Refused to provide some profile information or used fake informa-
tion because it was too personal or unnecessary
• Modified the way people can search your information on Facebook
• Hid a specific post from others and shared it only with select friends
• Modified the privacy settings to specify the people who can com-
ment on and/or like your posts
C.2 Supplementary results: Online survey
Participants’ age distribution and employment categories are presented in Fig-
ures C.1 and C.2. Also, Table C.1 presents a list of health-related sites that
were used by participants (note that these sites were not considered to be
SNSs).
136

0%
1%
2%
3%
4%
5%
6%
7%
19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73
% of p
ar1cipants
Age (19-‐74)
Figure C.1: Participants’ age distribution.
137

13.2%
12.6%
8.3%
6.9%
6.7%
6.5%
5.3%
5.1%
3.9%
2.6%
2.2%
1.2%
0% 5% 10% 15%
Business, management, or financial (e.g., manager, accountant, banker)
Service (e.g., retail clerks, server)
Computer engineer or IT professional (e.g., systems administrator, programmer, IT consultant)
AdministraKve support (e.g., secretary, assistant)
EducaKon (e.g., teacher)
Student
Medical (e.g., doctor, nurse, denKst)
Art, wriKng, or journalism (e.g., author, reporter)
Skilled labor (e.g., electrician, plumber, carpenter)
Engineer in other fields (e.g., civil engineer, bio-‐engineer)
ScienKst (e.g., researcher, professor)
Legal (e.g., lawyer, law clerk)
% of par(cipants
Figure C.2: Participants’ employment categories distribution.
138

Table C.1: Health-related sites used by participants that are not consid-ered as SNSs.
Name/Description Name/Description
Insulin Pump forum
(www.insulinpumpforums.com)PBC Group
Lymphomation.org Hypothyroid Mom
www.community.breastcancer.orgPost traumatic stress self help
group
JDRF (T1 Diabetes) Understood.org (Kids learning)
Wrongplanet Inspire (www.inspirehealth.ca)
Achalasia support group Reddit communities
Weight Watchers Healthy Brain Network
IBS Groups (ibsgroup.org) MS Society (beta.mssociety.ca)
MS World (www.msworld.org/)mdjunction
(www.mdjunction.com/)
Mitoaction
(www.mitoaction.org/)Myelomabeacon
(www.myelomabeacon.com/)
fibromyalgia of Ireland lupus and
me (Facebook group)enotalone (www.enotalone.com/)
Parenting/Breastfeeding MedHelp (www.medhelp.org/)
Positive and negative experiences
We asked participants to explain in their words why they think their experi-
ences were Positive. As presented in Table C.2, a total of 272 text responses
were analyzed and coded to represent participants’ positive experiences. Pos-
itive emotional and social support in the form of sympathy, empathy, and
139

prayers, were identified as the most common positive experiences among par-
ticipants. Useful recommendations and advice came second in the list, with
participants receiving feedback that positively helped them toward managing
their health conditions. Participants also described their positive experiences
by indicating that Facebook was used as an effective communication channel
for broadcasting information related to their health, while receiving timely
feedback from other social peers. Furthermore, participants benefitted from
their conversations with others in order to bring awareness to their health is-
sues and justify their behaviors whenever necessary. By sharing their HI on
Facebook, participants were able to find other social peers who had mutual
health experiences. Communicating with these social peers provided partici-
pants with valuable information/experiences while making them feel that they
belong to a group of understandable and easy to communicate people. Finally,
the two-way benefits of sharing HI on SNSs was easy to identify by going
through participants’ positive experiences in trying to help other people when-
ever possible.
140

Table C.2: Positive HI sharing experience. The first two columns repre-sent the coded category and related sub-categories. The last twocolumns represent the total number/percentage of positive codedevents under each category (272 total references).
Category Sub-categoriesCoded
events(%)
Positive supportsympathy, empathy, prayers, emotional
and social support107 39
Useful recom-
mendation and
advice
new medication, alternative medicine,
health condition management tips,
shared experiences and information re-
sources
74 27
Communication
with other peers
start conversations, quick/practical way
to broadcast health information, bring
attention to health conditions, receive
quick feedback, justify behaviors
49 18
Mutual experi-
ences
finding others with similar health is-
sues, easy communication, mutual un-
derstanding, useful feedback and ad-
vice, sense of belonging
27 10
Two-way bene-
fitsothers helped me, I tried helping others 15 6
As shown in Table C.3, participants identified a number of reasons for de-
scribing their prior HI sharing experiences to be Negative. Participants were
frustrated by the responses they received from their social peers who over-
reacted to their health problems and showed overwhelming and unnecessary
concerns. Participants were also agitated by the social peers who used their
shared HI in order to make judgments, spread rumours, gossip, or partici-
141

pated in insulting discussions. Furthermore, participants raised some privacy
concerns with respect to discussing their health issues in a semi-public en-
vironment lie Facebook, which occasionally led to oversharing their health
information without their permissions. Finally, while participants did not ap-
preciate the impractical recommendations and advice given to them by some
social peers, they felt lonely and unimportant when they received no support-
/replies from other social peers.
Table C.3: Negative HI sharing experience. The first two columns rep-resent the coded category and related sub-categories. The last twocolumns represent the total number/percentage of negative codedevents under each category (86 total references).
Category Sub-categoriesCoded
events(%)
People don’t un-
derstand
people overreact on health issues, feel
pity, create unnecessary worry, provide
responses that may increase anxiety
27 31
Negative social
impact
gossips, rumours, insulting discussions
and trolls, judgements, condescending
responses
22 26
Privacy concerns
public/open environment, people get
too involved/nosy, over sharing one’s
health information, receive spam/junk
17 20
Impractical
advice
impractical recommendations, advice,
and information12 14
Ignored postno replies to posts, no social support/in-
teractions, feel lonely/unimportant8 9
142
Top Related