







Languages
Pages
Legal


7/31/2012
1
Towards personalized medicine – integration of imaging into therapy
Robert JerajAssociate Professor of Medical Physics, Human Oncology,
Radiology and Biomedical Engineering
Translational Imaging Research (TIR) Program
University of Wisconsin Carbone Cancer Center, Madison, WI
Georges Chicotot treats a patient with X-Rays,1907
Imaging and therapy
Wilhelm Röntgen examines a patient with X-rays, 1896
100 years later… Image Guided Radiation Therapy

7/31/2012
2
100 years later… Image Guided Surgery
100 years later…What did medical physics contribute?
Imaging advances– New imaging modalities: MRI, PET, combined
modalities– Improved imaging technologies: contrast,
resolution, noise, speed, accuracy
Treatment advances– New RT technologies: Co-60, linacs, IMRT– Surgery: Minimally invasive procedures
We can be very PROUD of these achievements!
100 years later…Where is medical physics in Tx chain?
Shore et al 2012, Br J Urol Intl, 6: 22
Medical physics space
?
Dis
ease
pro
gre
ssio
n

7/31/2012
3
”4 P’s of medicine”: Individuals respond differently to environmental conditions, according to their genetic endowment and their own behavior. In the future, research will allow us to predict how, when, and in whom a disease will develop. We can envision a time when we will be able to precisely target treatment on a personalized basis to those who need it, avoiding treatment to those who do not. Ultimately, this individualized approach will allow us to preempt disease before it occurs, utilizing the participationof individuals, communities, and healthcare providers in a proactive fashion, as early as possible, and throughout the natural cycle of a disease process.
Elias A. Zerhouni, M.D.Director, National Institutes of Health (NIH), 2008
100 years later…Where is the medicine going?
”4 P’s of medicine”: Individuals respond differently to environmental conditions, according to their genetic endowment and their own behavior. In the future, research will allow us to predict how, when, and in whom a disease will develop. We can envision a time when we will be able to precisely target treatment on a personalized basis to those who need it, avoiding treatment to those who do not. Ultimately, this individualized approach will allow us to preempt disease before it occurs, utilizing the participationof individuals, communities, and healthcare providers in a proactive fashion, as early as possible, and throughout the natural cycle of a disease process.
Elias A. Zerhouni, M.D.Director, National Institutes of Health (NIH), 2008
100 years later…Where is the medicine going?
Imaging in treatment process
…. PRE Tx TREATMENT POST Tx
DIAGNOSISSTAGING
TREATMENTSELECTION
TREATMENT ASSESSMENT
TREATMENTSELECTION
…. TREATMENT

7/31/2012
4
TREATMENT SELECTION
…. PRE Tx TREATMENT POST Tx
DIAGNOSISSTAGING
TREATMENTSELECTION
TREATMENT ASSESSMENT
TREATMENTSELECTION
…. TREATMENT
FMISO PET in HN
Rischin et al 2006, J Clin Oncol, 24: 2098.
FMISO PET + (hypoxia) + chemo boost
FMISO PET + (hypoxia) + TPZ boost
FMISO PET – (no hypoxia)
FMISO PET focal uptake mildly larger than bgrd
0
2
4
6
8
10 HER2 NegHER2 Pos
LABC or Metastatic Br CA Primary Tamoxifen Rx
Recurrent or Metastatic Br CA Aromatase Inhibitor Rx
(P < 0.01 for both)
FE
S S
UV
FE
S S
UV
Responders Non-Responders
FES PET in Breast
Responders Non-Responders
FES PET SUV=1.5Linden et al 2006,
J Clin Oncol, 24: 2793Mortimer et al 2001, J Clin Oncol, 19: 2797

7/31/2012
5
DCE/DSc MRI in GBM
Yao et al. 2011, Sem Rad Oncol, 21:147
Radiation Therapy
FTV = 0.07
© The Author 2011. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: [email protected]
Can we image everything - lung?
Sequist et al. 2011, Ann Oncol, 22:2616
Riley et al. 2009, Proc Am Thorac Soc, 6:201
Maemondo et al 2010, N Engl J Med, 362:2380
MICAD: Molecular Imaging and Contrast Agent Database
1260 agents listed(July 2012)

7/31/2012
6
1
23
4
5
But can we really use them all?
1. Credentialing
2. Modality creation
3. Supporting tools
4. Development
5. Clinical trials
Regulatory approval (eIND, RDRC)
Regulatory approval (full IND)Multicenter trial infrastructure (NCI CIP, ACRIN)
100%
10%
1%
Highly interdisciplinary
Cell/molecular biology
Chemistry/radiochemistry
Radiology
Medical physics
Pharmacology
Medicine
Engineering
Mathematics
Material science
Computer science
Role for medical physics?
Courtesy of W. Cai, UW
Is imaging just an expensive tool?
…branched evolutionary tumor growth, with 63 to 69% of all somatic mutations
not detectable across every tumor region…
Gerlinger et al 2012, N Engl J Med 366: 883.
NO, this makes imaging essential,
and complementary
7/31/2012
7
TREATMENT ASSESSMENT
…. PRE Tx TREATMENT POST Tx
DIAGNOSISSTAGING
TREATMENTSELECTION
TREATMENT ASSESSMENT
TREATMENTSELECTION
…. TREATMENT
WHO (1979, 1981)1,2
– anatomic
RECIST (2000, 2009)3,4
– Response Evaluation Criteria In Solid Tumors
– anatomic, CT/MR based
– unidimensional
– 4 response categories (CR, PR, SD, PD)
1WHO 1979, 2Miller et al. 1981, 3Therasse et al. 2000, 4Eisenhauer et al. 2009
| | | | | | |-100% -60% -30% 0% +30% +60% +100%
partialresponse
completeresponse
progressive disease
stable disease
Treatment response assessment
Power of molecular imaging
Pre-treatment 1 month post treatment
Stroobants et al 2003, Eur J Cancer 39, 2012Van der Abbelle 2008, The Oncologist 13(suppl 2), 8
• FDG PET response correctly predicts response to Gleevec in majority of patients• FDG PET response correctly predicts SD and PD, while CT does not• FDG PET response precedes the CT response (shrinkage) by several weeks• FDG PET response is strongly associated with a longer progression free survival (92% vs. 12% after 1 year) and closely correlated with subjective symptom control

7/31/2012
8
Acute myeloid leukemia
Specificity = 43%NPV = 64%17.4 mo
6.9 mo
Day 28 BMBx
Day 14 BMBx
Hussein et al 2008, Am J Hemat, 83(6): 446
Pre-therapy
Completeremission
Resistantdisease
Chemo
Chemo
10
5
0
SUV
How early can imaging predict future?
FLT PET
CLINICAL OUTCOME
(6 mo)
Post-therapy(2 wks)
Vanderhoek et al 2011, Leuk Res 35: 310
Early treatment response assessment
Post-therapy Day 6 Day 4 Day 2Co
mp
lete
Re
mis
sio
n(6
mo
)
Post-therapy Day 2
Day 5
SUVmean SUVmaxCoefficientof Variation
CompleteRemission
0.81 ± 0.03 3.6 ± 0.4 0.33 ± 0.02
ResistantDisease
1.6 ± 0.1 11.4 ± 0.8 0.71 ± 0.04
10
5
0
SUV
t-test: p<0.001 for SUVmean, SUVmax, CV
Res
ista
nt
Dis
ease
(6 m
o)
6.5 σ6.1 σ 6.3 σ
Better than Higgs!!!
7/31/2012
9
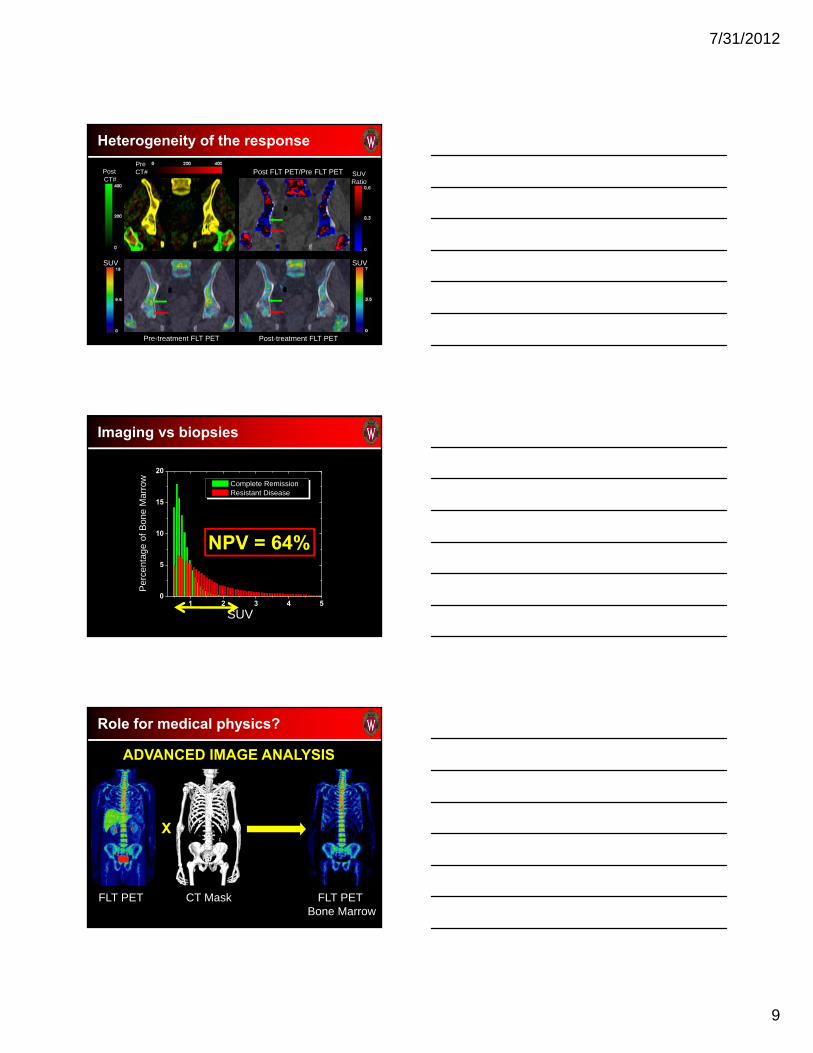
Post FLT PET/Pre FLT PETPre CT#Post
CT#
Pre-treatment FLT PET Post-treatment FLT PET
SUVRatio
SUV SUV
Heterogeneity of the response
Imaging vs biopsies
1 2 3 4 50
5
10
15
20
Per
cent
age
of B
one
Mar
row
SUV
Complete Remission Resistant Disease
NPV = 64%
FLT PET CT Mask
Role for medical physics?
X
FLT PET Bone Marrow
ADVANCED IMAGE ANALYSIS

7/31/2012
10
FDG PET in NSCLC
HR = 2.27(1.70-3.02 95% CI)
N=1474
SUVmax
SUVmean
Unspecified
Weight LBMUnspecified
Best cut-off MedianArbitrary
5-205-102.5
Berghmans et al 2008, J Thorac Oncol, 3: 6.
PET-based response assessment
EORTC, NCI Recommendations (1999, 2005) 1,2
– SUV-based approach– SUVmean and SUVmax
– Response categories with thresholds (CR, PR, SD, PD)
PET Response Criteria in Solid Tumors (PERCIST) (2009) 3
– SUV-based approach– SUVpeak
– Response categories with thresholds (CR, PR, SD, PD)
1Young et al 1999, 2Shankar et al 2006, 3Wahl et al 2009
Images are more than just one number!
Volume
SUVmean SUVtotal
Size measures
– Volume
– 1D size (axial)
Standardized Uptake Value (SUV) measures:
– SUVmean
– SUVtotal
– SUVmax
– SUVpeak
Uptake Non-uniformity measure:
– SUVsd
…
1D Size (axial)
SUVmaxSUVpeak
0 5 10 15 200
50
100
150
200
250
Num
ber
of
Vo
xels
Standardized Uptake Value
SUVsd

7/31/2012
11
SUVtotal VolumeSUVmean SUVmax
GOOD RESPONSE POOR RESPONSE NEW LESIONS
Different measures tell different stories
SCANNER HARMONIZATION
UW GE DVST S2N2 vs Dis/cc measured for different reconstruction settings NCI Gemini TF S2N2 vs Dis/cc measured for one reconstruction setting
Phantom measurements to characterize the scanners Comparative patient data from UW and NCI studied Patient S2N2 data presented using phantom data for reference
Role for medical physics?
NCI
TREATMENT SELECTION - AGAIN
…. PRE Tx TREATMENT POST Tx
DIAGNOSISSTAGING
TREATMENTSELECTION
TREATMENT ASSESSMENT
TREATMENTSELECTION
…. TREATMENT
7/31/2012
12
Published by AAAS
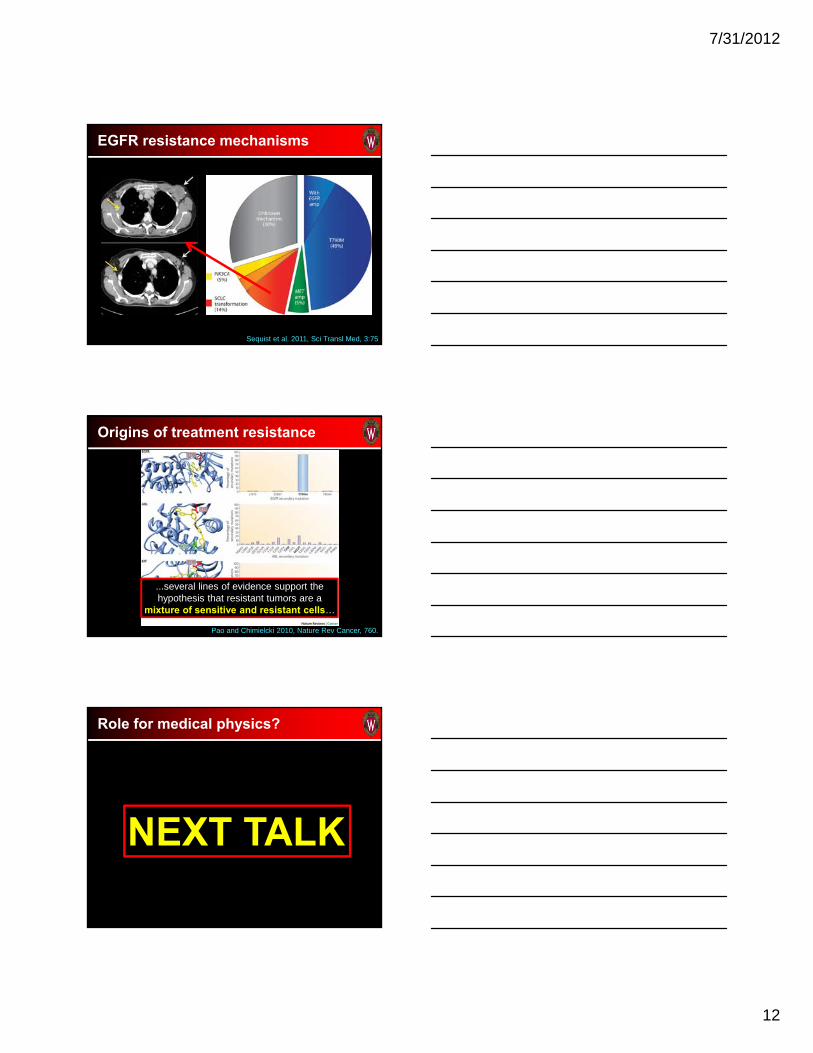
EGFR resistance mechanisms
Sequist et al. 2011, Sci Transl Med, 3:75
Origins of treatment resistance
...several lines of evidence support the hypothesis that resistant tumors are a
mixture of sensitive and resistant cells…
Pao and Chimielcki 2010, Nature Rev Cancer, 760.
Role for medical physics?
NEXT TALK

7/31/2012
13
Summary
Medical physics has been extremely successful, but it has “captured” only a small part of the interface between imaging and therapy – ENORMOUS POTENTIAL!!!
Future of medicine – personalized therapy - is complex, but extremely exciting, don’t wait - EXPAND HORIZONS!!!
MANY ESSENTIAL ROLES we should play beyond radiotherapy and diagnostic imaging:– Clinical trial design!– Molecular imaging chain – Advanced image analysis– Quantitative imaging– Modeling– …
CJ’s FUTURE
Pondering her future… ... Easy decision…
Courtesy of Stephanie Harmon and her niece CJ, March 2012
Thanks to:
Image-guided therapy group– Vikram Adhikarla– Tyler Bradshaw– Enrique Cuna– Ngoneh Jallow– Matt La Fontaine– Paulina Galavis– Stephanie Harmon– Courtney Morrison– Surendra Prajapati– Urban Simoncic– Peter Scully– Benny Titz– Natalie Weisse– Koala Yip– Stephen Yip– Former students…
Funding– NIH, PCF, UWCCC, Pfizer,
AstraZeneca, Amgen, EntreMed
Medical Oncology/Hematology– Glenn Liu– George Wilding– Mark Juckett– Brad Kahl– Anne Traynor
Human Oncology– Søren Bentzen– Paul Harari– Mark Ritter
Radiology– Scott Perlman– Chris Jaskowiak
Veterinary School– Lisa Forrest– David Vail
Medical Physics– Rock Mackie– Jerry Nickles– Onofre DeJesus
Phase I Office

7/31/2012
14
Medical physics and ART
Courtesy of Koala Yip and her mom, January 2012
Top Related