





Languages
Pages
Legal


Professor Brenda Zimmerman,
Director of Health Industry Management Program
Schulich School of Business,
September 23, 2014
Engaging with Complexity
Thrive! A Plan for a Healthier Nova Scotia
22
Why do strategic plans tend to fall short of expectations?

3
There Are Several Types of Problems
pSimpleMaking Soup
Right “recipe” essential
Gives same results every time
pComplicatedSending a Rocket to the
Moon
“Formulae” needed
Experience built over time and can be repeated with success
pComplex
Raising a Child
No “right” recipes or protocols Outside factors influence Experience
helps, but doesn’t guarantees success
4
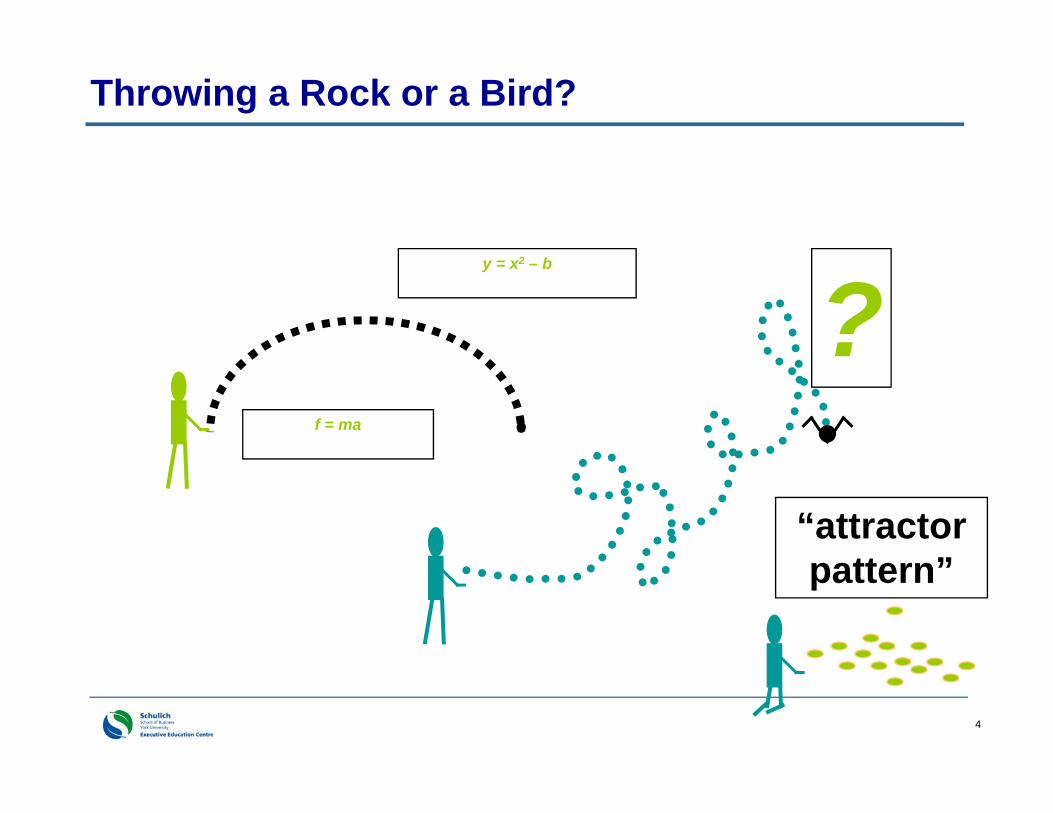
Throwing a Rock or a Bird?
4
y = x2 – b
f = ma
?“attractor pattern”
5
Complicated and Complex Systems
Complicated (machine-like)– Metaphor: Send a rocket to the moon– Reliance on installation and mechanical replication of technically
correct solutions designed by experts.
Complex (organic)– Metaphor: Raising a child– Keys: appreciation of uniqueness, interaction, being adaptable,
& staying tuned in to what is happening. Looking for the attractor patterns
5

6http://www.youtube.com/watch?v=Miwb92eZaJg

7
Dave Snowden – BD party lessons “We manage emergence of beneficial coherence
within attractors, within boundaries.”
How? We observe & stimulate the patterns of activity
called an attractor. When we see beneficial attractors – we attempt to
stabilize and amplify them When we see negative attractors – we attempt to
dampen or destroy them
7
8
Understanding Change in Complex Social Systems
Behavior of the system can be largely explained by understanding “attractors.”
Relationships and coordination among parts can be more important than the parts themselves.
9
Creating Attraction for Change
The concept of “resistance to change” is negative and emotionally draining
We need to stop speaking of “us” and “them”
Complex adaptive systems can be understood through attractor patterns
How can I make my change more naturally attractive to others?
When you encounter resistance, ask yourself… “What is it that *I* do not understand here?”
9
10
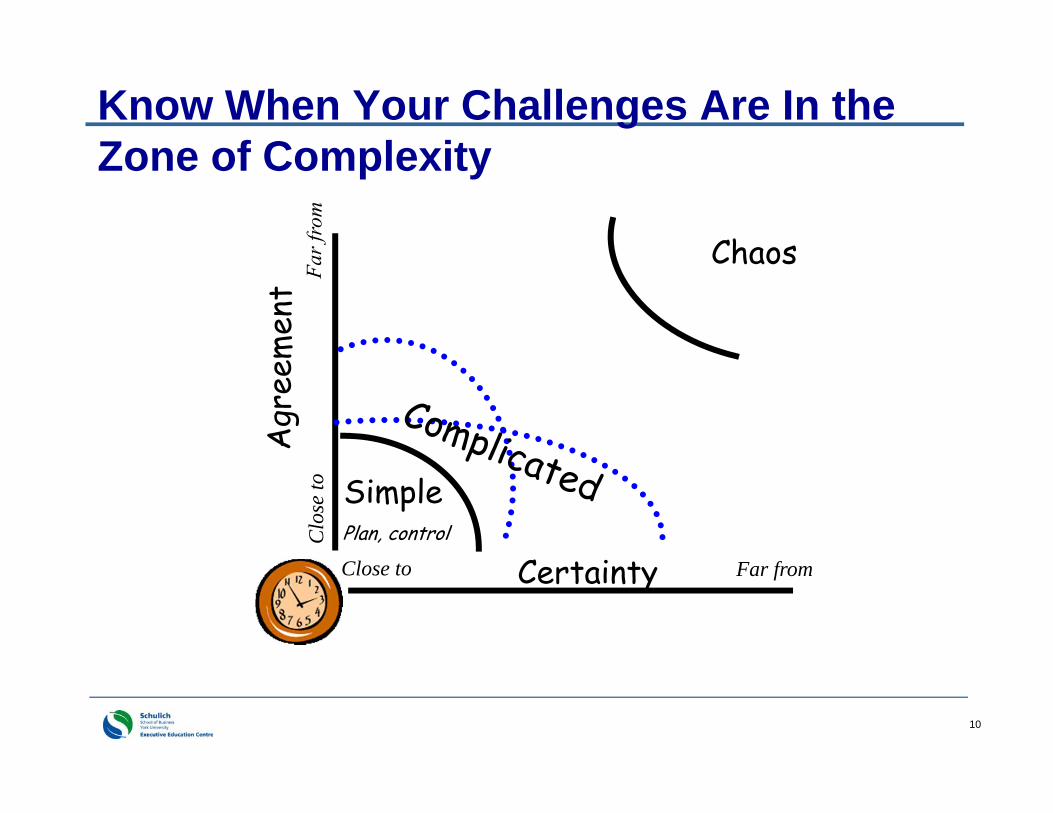
Know When Your Challenges Are In the Zone of Complexity
CertaintyClose to Far from
Clo
se to Simple
Plan, control
Chaos

11
Simple &
complicatedPlan, control CertaintyClose to Far from
Clo
se to
ChaoticSeek Patterns
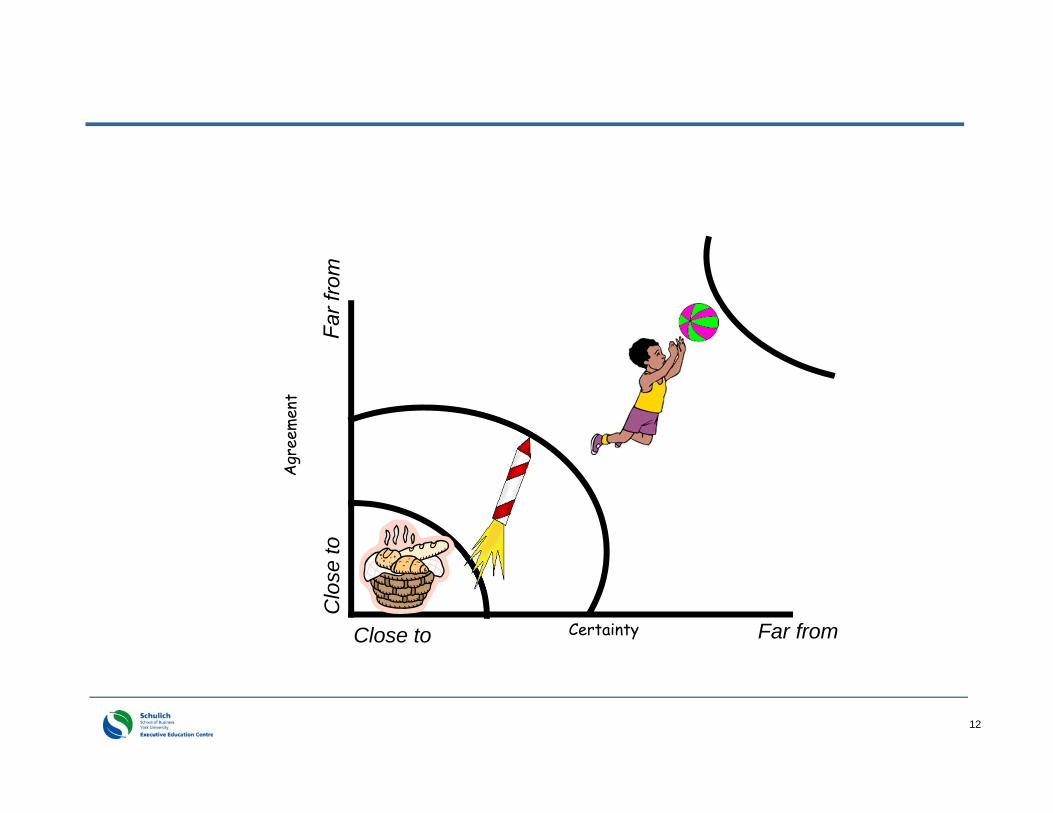
12
CertaintyClose to Far from
Clo
se to

13
Workout one on SCC Take a stuck problem you have. One that keeps
rearing its head.
Use two peers to interview you about this. Their job is to get the facts and probe deeper but NOT to advice or share their own experiences.
Where is the issue on the SCC grid? What strategies have you been trying to date? What
is working? What isn’t working?
13

14
“Things that never happened before, happen all the time”
Kathleen Sutcliffe, PhD
So what??We need to be skillful at expecting, seeing andresponding to surprise. This is both for individuals
and the collective.
Key to adaptability
15
Lessons From Biology Living systems - follow simple “rules” or minimum specifications that create complex adaptability
“Boids”, ants, democracy & chess
Champions for Change: Leading a Backbone Organization for Collective
Impact

16April 2013 Champions for Change: Leading a Backbone Organization for Collective
Impact
Insert flamingos….
17
Example: Reynolds’ Flocking Rules
Maintain a minimum distance from other boids and objects
Match speed of neighbouring boids Move toward the center of mass of flock-mates in
your area
Complex “flocking” emerges!
18
Exploring Min Specs/ Simple Rules
What are the rules that are currently affecting action? (inductive analysis)
What are the minimum set of rules to shape action in the future? (deductive analysis)

19
ALCOA – “prevent all injuries”
Safety is a precondition not a priority(if priority – can say “can’t afford to be better”)
Report all injuries within 24 hours(“capital offense” – failure has consequence)
Share lessons learned(financial incentive to learn and share)
20
Priority vs. Precondition
Paul O’Neill – ED of Pittsburg Health Authority (ex CEO of Alcoa and also ex Secretary of Commerce)
“When “safety” is a priority rather than a precondition, won’t have “0” accidents.”
Preconditions aren’t negotiable
“Capital offense” to not report accidents

21
Patient Safety – example Missouri Baptist hospital
Fix what you can Tell what you fixed Report what you cannot
ALL employees know this and it is reinforced through both compensation and evaluation
22
Checklist vs. Min Specs/Simple Rules
Min Specs/Simple Rules Need to adapt
quickly to changing circumstances Set boundaries of
acceptable behaviour Leave room for
flexibility or creativity Coherence Adaptability
Checklist Lay out clear task Optimal process
known apriori Steps to optimal
process known and articulated Consistency Efficiency
23
… Picking up on yesterday’s remarks
“Why is our health not a sacred value in Canada?”
… “should be a priority”…. Minister Glavine
Beyond priority to precondition
If it is a sacred value it will influence every decision.
It would be a “minimum specification”.
“Governance for Health” - Hancock

24
Imagine what it would mean if Nova Scotia adopted human development as a pre-condition. Then the economy could be a priority
as it would be filtered through the lens of human development. Priorities can change year by year
24
25
Min Specs/Simple Rules – allow for swarming
They give enough of a sense of direction without over-specifying
Local solutions can be discovered (at the “edge” rather than center)
Following same rules – can result in different solutions – Creates coherence rather than
consistency– Allows for constant adaptation &
innovation

26
“… Human systems grow toward
what they persistently
ask questions about”
(Cooperrider and Whitney 1999, 10).

27

28
The Brazil Complex Problem
How do you respond to an AIDS epidemic in a developing country? No money for expensive drugs
– problems of affordability of drugs A very iffy health care system
– problems of treatment High levels of illiteracy
– problems of compliance even if there were drugs High levels of poverty and hunger
– problems of nutritional needs for drugs And… it is a sexually transmitted disease
29
Questions Posed by World Bank “What will drug costs be for the infected
population?”
“What resources are needed to manage drug therapies for illiterate patients?”
“What resources are needed to assure compliance with drug associated nutrition in this population?”
“What are the resources needed for an effective prevention program?”
30
World Bank Responds to AIDS as Complicated
Meaningful solutions require sophisticated, integrated national health care systems We cannot provide treatment to all when
the drug costs are so high We cannot afford resources to manage
treatment compliance With our limited resources, we should
focus more on prevention than treatment It will therefore take a long time for the
problem to work itself through

31
Brazil Implicitly Recognized the Complexity
Were unwilling to accept the answers of the World Bank
Hence – had to change the questions…– Changing the questions changes the
focus, changes what is “analyzed”, changes what is seen as possible/impossible
32
The Brazil Questions Assume Complexity
“What will drug costs be for our infected population?”
“What resources are needed to manage drug therapies for illiterate patients?”
“How can we reduce costs so that we can provide treatment to all who need it?”
“What methods of communication will work to convey the drug therapy routine to a patient – even a homeless, illiterate patient?”
World Bank Questions Brazil Questions

33
The Brazil Questions
“What resources are needed to assure compliance with drug associated nutrition in this population?”
“What are the resources needed for an effective prevention program?”
“If food is an issue, how can we ensure greater compliance by linking up with charities/food banks/ churches etc.?”
“How can we achieve our prevention goals while treating all of those currently infected?”
World Bank Questions Brazil Questions
34
35
36
37
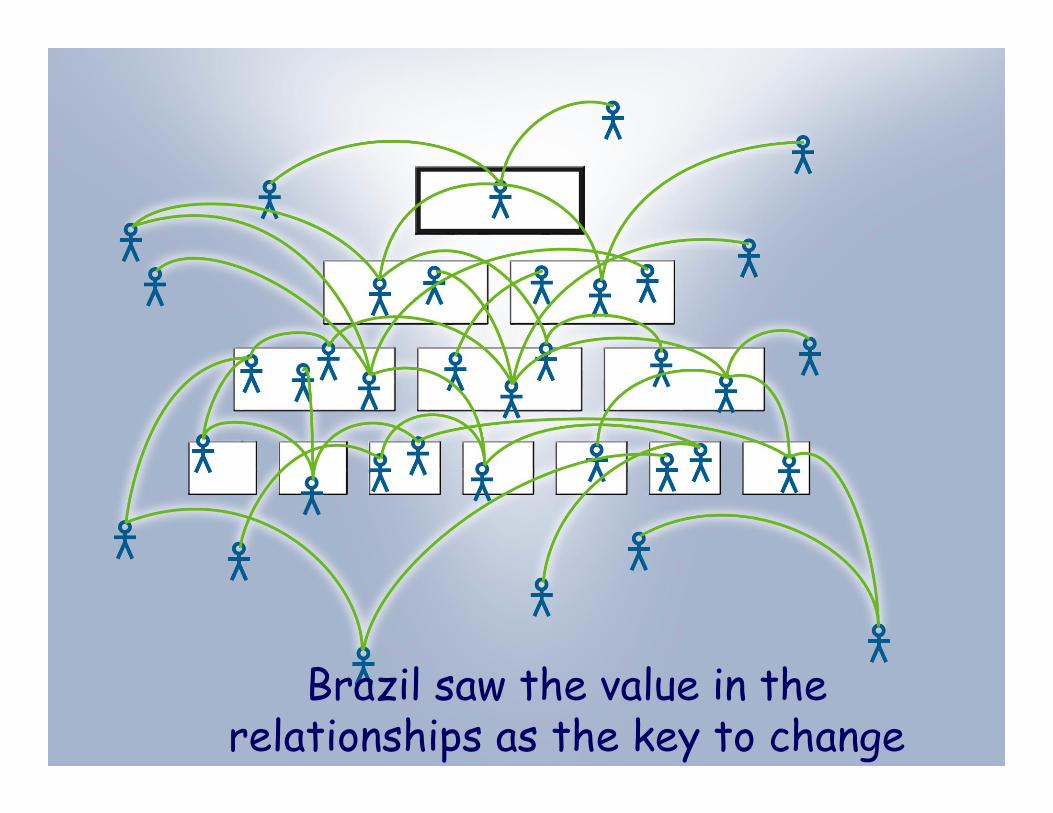
Brazil saw the value in the relationships as the key to change

38
The Brazil Conclusions
Meaningful solutions require sophisticated, integrated national health care systems
We cannot provide treatment to all when the drug costs are so high
We cannot afford resources to manage treatment compliance
With limited resources, focus more on prevention than treatment
It will therefore take a long time for the problem to work itself through
Find ways to use the resources we have to respond to the problem
Provide drugs to all by finding ways to reduce drug costs
Use our informal system to train people to care for themselves
Prevention will be part of the treatment
Seek short and long term results
World Bank Conclusions Brazil Conclusions

39
The Brazil Responses
A stable container: Brazil built on existing infrastructure (natural network existed)– A somewhat shaky health system of
hospitals and clinics– Added to by 600 NGOs, churches
(hubs)
Free drugs to all AIDS patients: faced down drug companies in pursuit of national interest
40
The Brazil Responses - cont’d
Patients managed their own drugs– Illiterate people were taught by local “trustworthy” folks (hubs were sought)
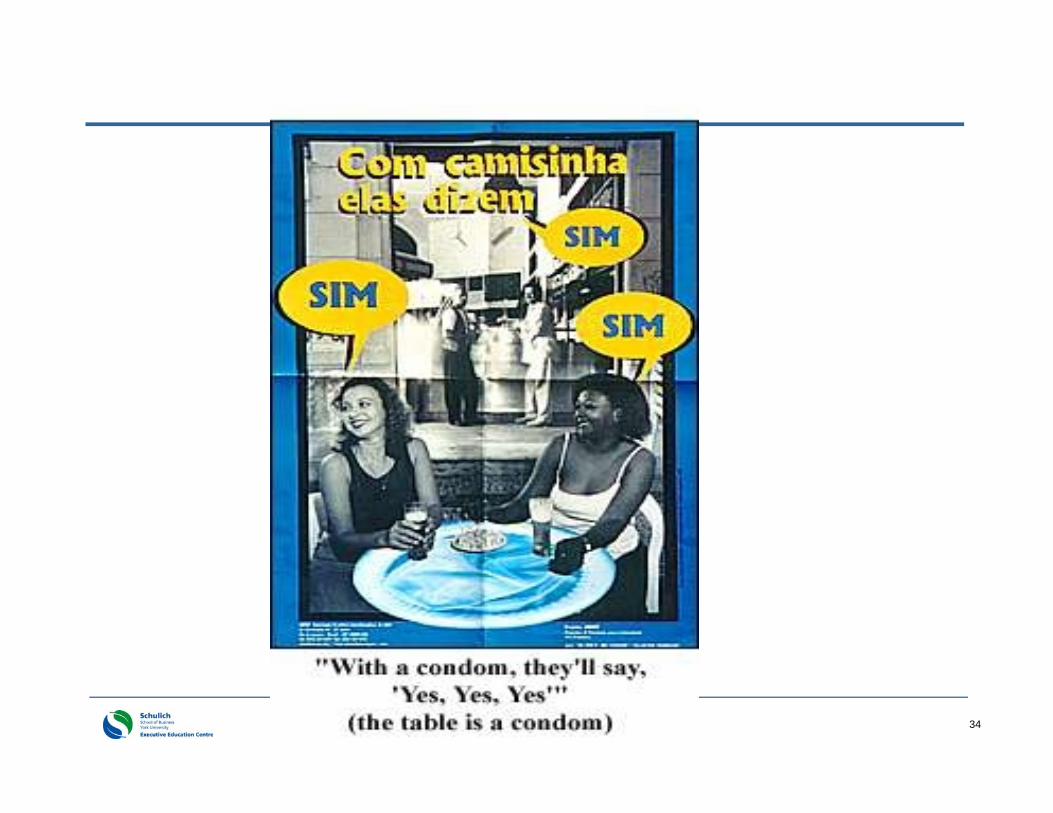
Free treatment spread prevention ideas– No labeling of those affected– Prevention information readily
available

41
Brazil --- epilogue to the case
For over 20 years maintained their HIV prevalence to 0.3% of the population
But with complexity, success is never a destination. Things change, contexts change and what worked at one time will not work at another time.
Today prevalence is climbing in youth (15-24 year olds) -- dramatic increase in number of cases
WHY?? What has changed?
42
Brazil in 2014
Christian following has changed – In 1970 5% of Christians in Brazil were Evangelical– In 2013 grew to 22% -- and trending up
-- And so??
With a low prevalence rate for HIV, young people were starting to feel immune – “It was a problem of the past”
Starting to ask new questions… -facing up to changed context
43
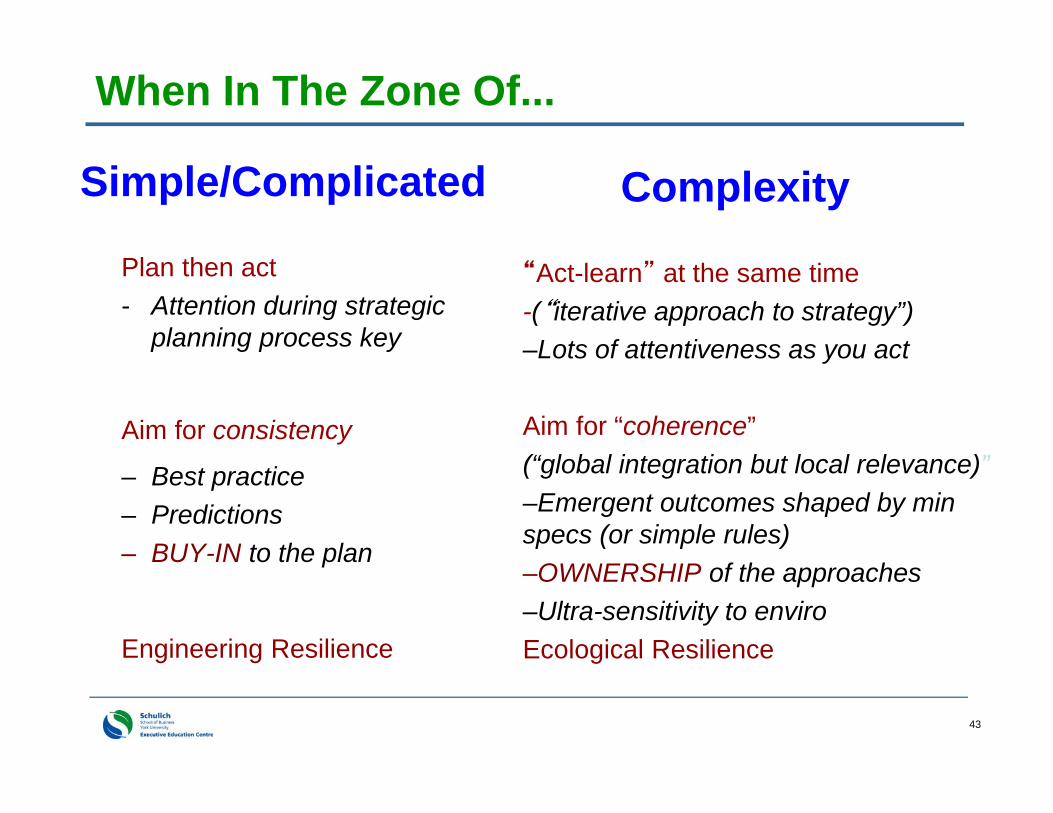
When In The Zone Of...
Simple/Complicated
Plan then act- Attention during strategic
planning process key
Aim for consistency
– Best practice– Predictions– BUY-IN to the plan
Engineering Resilience
Complexity
“Act-learn” at the same time -(“iterative approach to strategy”)–Lots of attentiveness as you act
Aim for “coherence”(“global integration but local relevance)”–Emergent outcomes shaped by min specs (or simple rules)–OWNERSHIP of the approaches–Ultra-sensitivity to enviroEcological Resilience
44
ENGINEERING RESILIENCE: Bouncing back to
the status quo
ECOLOGICAL RESILIENCE: Adaptation and deep
change throughcreative destruction which allows the system to continuallylearn from surprises

45
Buy–In vs Ownership*Buy-In: Someone else has developed the
idea, made the decision, designed an action plan and then asks and needs the staff to implement it.
Ownership: Front line staff develops the idea, makes the decisions, designs the action plan and acts on it.
* Buy-in is the opposite of ownership and a danger signal that tells you that your development and implementation process are missing the essential ingredient of involving everyone who needs to be.
4646
Workout 2 – go back to your stuck problem
Are you aiming for buy-in or ownership?
Are you looking for consistency or coherence?
47
When In The Zone Of...
Simple/Complicated– Plan then act
– Aim for consistency– Buy-In – Limit type of action (best
practice)– “Blueprints”– Project Management– Inquiry – problem
solving, convergent, data
Complexity– “Act-learn” at the same
time (tight feedback loops)– Aim for “coherence”– Ownership– Multiple actions– Min specs/simple rules– Generative thinking AND
Generative relationships– Inquiry – appreciative
inquiry, divergent, “wicked”

48
“Stop trying to change reality by attempting to eliminate complexity.”
David Whyte
49
Time is too short and
things are too bad
for pessimism.Dee Hock

50
REFERENCES for future reading www.plexusinstitute.com - Excellent resources (books,
articles, and cases).
For more articles, books from Brenda Zimmerman:
– www.change-ability.ca --- some articles from Brenda Zimmerman and colleagues
– Westley, Frances, Brenda Zimmerman and Michael Quinn Patton, “Getting to Maybe: How the World is Changed”, Random House Canada, 2006
– Zimmerman, Brenda, Lindberg, Curt and Plsek, Paul. (1998). Edgeware: Lessons From Complexity Science for Health Care Leaders. Dallas, TX: VHA Inc. (This book can also be found on the Plexus Institute website under Resources – Edgeware)
50
Top Related