







Languages
Pages
Legal

1
Slide 1JSOMTC, SWMG(A)
SOCMPhysical Exam of the Abdomen
PFN: SOMPYL0S
Hours: 1.5
Slide 2JSOMTC, SWMG(A)
Terminal Learning Objective Action: Communicate knowledge of “Physical Exam of the Abdomen”
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% IAW course standards on the formative quizzes and the Physical Exam Practical Test grade sheet
Slide 3JSOMTC, SWMG(A)
References
Bickley L, Szilagyi PG. Bates' Guide to Physical Examination and History‐Taking. Lippincott Williams & Wilkins; 2012.
Venes D, Taber CW. Taber's CyclopedicMedical Dictionary. F A Davis Company; 2013.
D'amico DT, Barbarito C. Clinical Pocket Guide for Health and Physical Assessment in Nursing. Prentice Hall; 2015.
2
Slide 4JSOMTC, SWMG(A)
Reason
Hands on physical exams are a “lost art” due to the many imaging procedures that can be done in a hospital. As a SOF medic you will not have that luxury. Learning how to perform a physical exam of the abdomen could save your teammates hours of pain and possibly even his life!
Slide 5JSOMTC, SWMG(A)
Agenda
Define key terms related to the physical exam of the abdomen
Communicate the inspection, auscultation, percussion, and palpation of the abdomen
Communicate the examination techniques when assessing the liver, spleen, abdominal aorta, and kidneys
Identify normal and possible abnormal findings on an abdominal radiograph
Slide 6JSOMTC, SWMG(A)
The Key Terms Related to Physical Exam of the Abdomen

3
Slide 7JSOMTC, SWMG(A)
Key Terms
Aerophagia: swallowing air
Anorexia: a loss of appetite
Bruits: an adventitious sound of venous or arterial origin heard on auscultation
Bloating: an abdominal discomfort related to disorders of intestinal motility and intestinal sensitivity to distention
Slide 8JSOMTC, SWMG(A)
Key Terms
Borborygmi: a gurgling, splashing sound normally heard over the abdominal region; caused by passage of gas through the liquid contents of the intestine
Cholecystitis: an inflammation of the gallbladder, usually caused by obstruction of the biliary ducts by gallstones
Constipation: a decrease or difficulty in the passage of stool or fecal matter
Slide 9JSOMTC, SWMG(A)
Key Terms
Diarrhea: the passage of fluid or unformed stool
Dyspepsia: nonspecific upper abdominal discomfort, pain, or nausea not attributed to structural abnormality or peptic ulcer disease
Dysphagia: an inability or difficulty to swallow
Dysuria: a painful or difficulty in urinating
4
Slide 10JSOMTC, SWMG(A)
Key Terms
Flatus: the passing of gas
Guarding: a voluntary contraction of the abdominal wall
Hematuria: blood in the urine
Hematochezia: bright red stool
Hematemesis: vomiting of blood
Incontinence: a loss of control, e.g. urine or feces
Slide 11JSOMTC, SWMG(A)
Key Terms
Icterus (jaundice): a yellowish discoloration of the skin and sclerae from increased levels of bilirubin
Melena: black tarry stools, caused by digested blood in the GI tract
Nocturia: excessive or frequent urination after going to bed
Slide 12JSOMTC, SWMG(A)
Key Terms
Obstipation: an absence of the passage of gas or feces
Odynophagia: painful (or pain) when swallowing
Polyuria: passage of a large volume of urine in a given period of time
Tenesmus: straining, especially ineffectual and painful straining at stool or urination
5
Slide 13JSOMTC, SWMG(A)
Key Terms & Health History
Common or Concerning Symptoms
Abdominal pain (acute & chronic)
Indigestion, nausea, vomiting including blood, loss of appetite, early satiety
Dysphagia and/or odynophagia
Changes in urinary frequency or habits
Changes in bowel function (Diarrhea and/or constipation)
Jaundice (icterus)
Slide 14JSOMTC, SWMG(A)
Key Terms & Health History
Associated symptoms
Nausea (feeling sick to my stomach)
Recurrent vomiting and/or retching
• Ask about the amount of vomit
• Ask about the type of vomit: food, green‐ or yellow‐colored bile, mucus, blood, coffee‐ground emesis*
Heartburn (often associated with regurgitation)
Dehydration or electrolyte imbalance
Anorexia and/or excessive weight loss
Slide 15JSOMTC, SWMG(A)
Key Terms & Health History
Other symptoms
Dysphagia (difficulty swallowing)
Odynophagia (pain on swallowing)
Change in bowel function
• Use open ended questions like
“How are your bowel movements?”
“Do you have any difficulties?”
• Excessive gas or flatus
Needing to belch or fart
Patients often state they feel bloated

6
Slide 16JSOMTC, SWMG(A)
Key Terms & Health History Quantify and qualify the patient’s pain
Visceral pain: felt when hollow organs forcefully contract or become distended
• Visceral pain is usually gnawing, cramping, or aching and is often difficult to localize
Visceral periumbilical pain may signify early acute appendicitis
• When severe, may be associated with sweating, pallor, N & V, and restlessness
• Solid organs (liver, spleen) may also generate this type of pain when they swell against their capsules (alcoholic hepatitis)
Slide 17JSOMTC, SWMG(A)
Types of Visceral Pain
Slide 18JSOMTC, SWMG(A)
Key Terms & Health History
Parietal pain: inflammation in the parietal peritoneum
Steady, aching and aggravated by coughing and/or movement (patients will prefer to lie still)
• More severe and usually easily localized (e.g., late appendicitis)
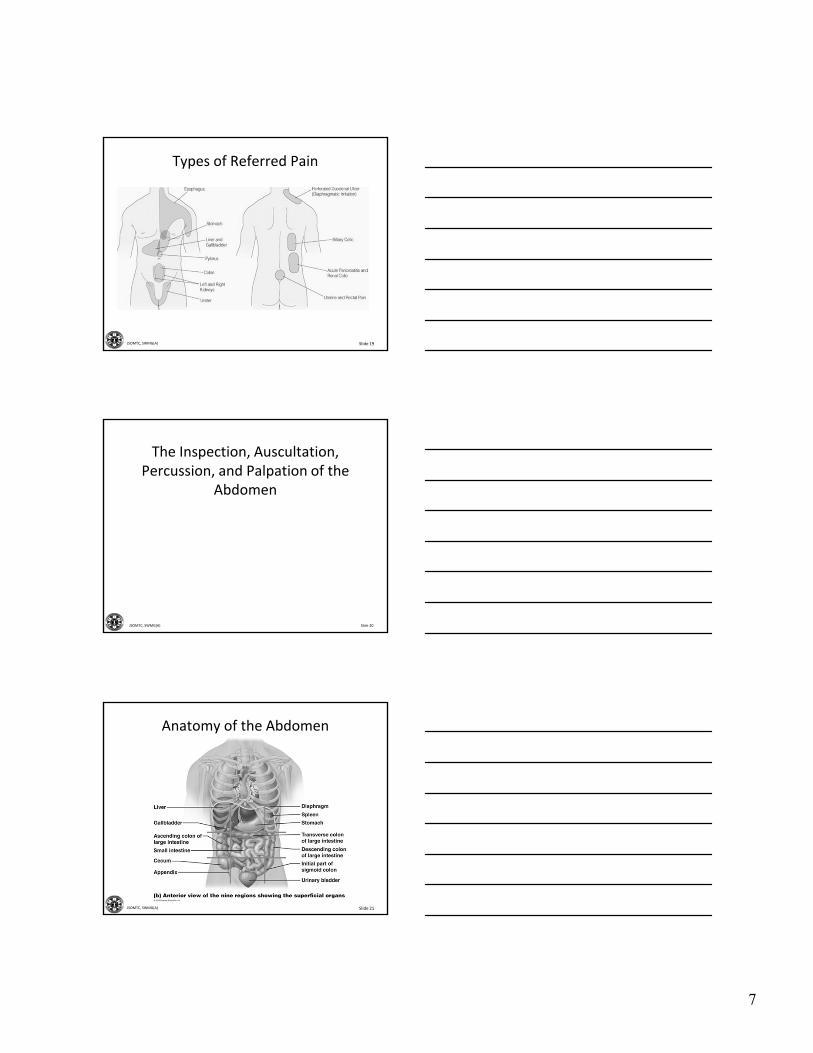
Referred pain: Pain felt at different location than disordered structure.
Multiple sensory fibers from different sources connecting at a single level of the spinal cord make it difficult for the brain to discern the actual origin of the pain (e.g., liver / gallbladder pain usually refers to the right shoulder)
7
Slide 19JSOMTC, SWMG(A)
Types of Referred Pain
Slide 20JSOMTC, SWMG(A)
The Inspection, Auscultation, Percussion, and Palpation of the
Abdomen
Slide 21JSOMTC, SWMG(A)
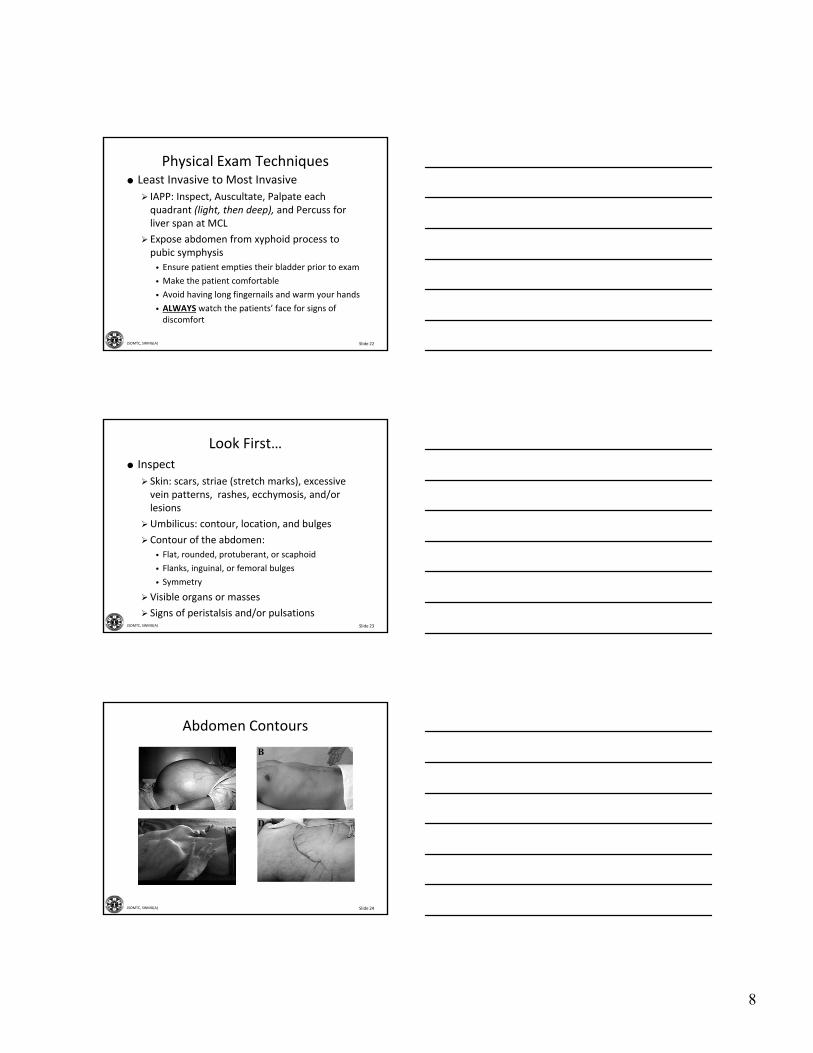
Anatomy of the Abdomen
8
Slide 22JSOMTC, SWMG(A)
Physical Exam Techniques Least Invasive to Most Invasive
IAPP: Inspect, Auscultate, Palpate each quadrant (light, then deep), and Percuss for liver span at MCL
Expose abdomen from xyphoid process to pubic symphysis
• Ensure patient empties their bladder prior to exam
• Make the patient comfortable
• Avoid having long fingernails and warm your hands
• ALWAYS watch the patients’ face for signs of discomfort
Slide 23JSOMTC, SWMG(A)
Look First…
Inspect
Skin: scars, striae (stretch marks), excessive vein patterns, rashes, ecchymosis, and/or lesions
Umbilicus: contour, location, and bulges
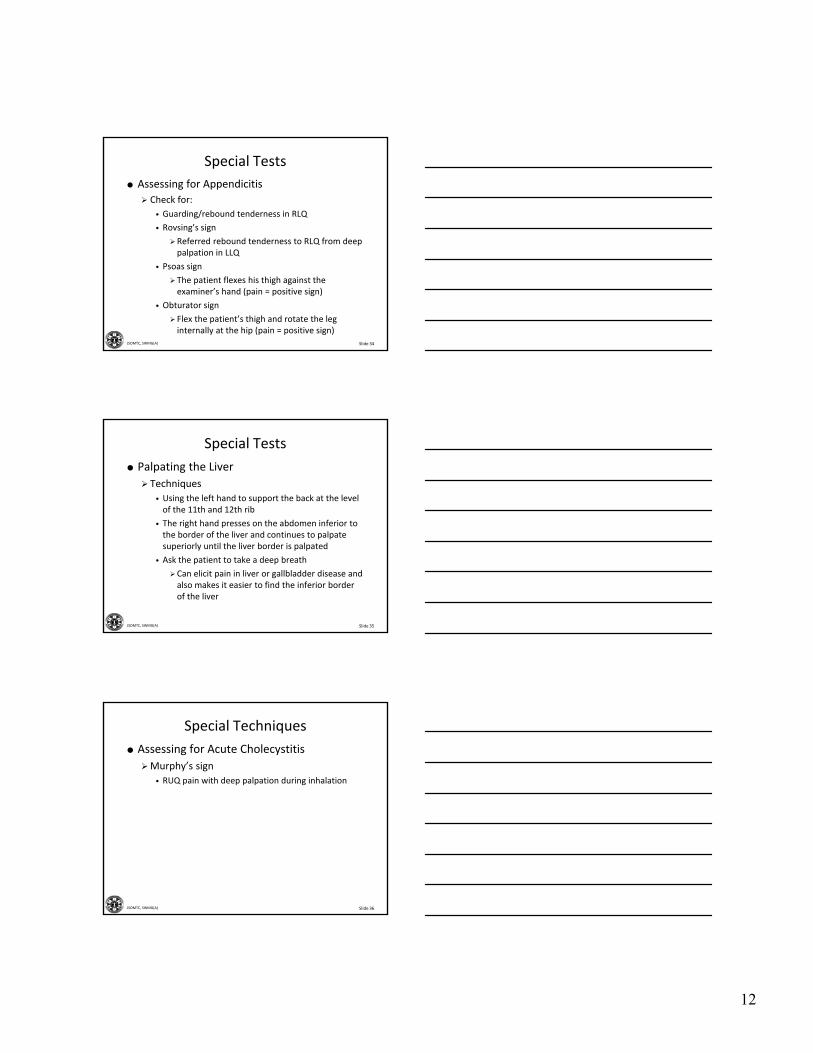
Contour of the abdomen:
• Flat, rounded, protuberant, or scaphoid
• Flanks, inguinal, or femoral bulges
• Symmetry
Visible organs or masses
Signs of peristalsis and/or pulsations
Slide 24JSOMTC, SWMG(A)
Abdomen Contours
A
C
B
D

9
Slide 25JSOMTC, SWMG(A)
Abnormal?
D
A B
C
Slide 26JSOMTC, SWMG(A)
Physical Exam Techniques
Assessing for ventral hernias
Ask patient to raise head and shoulders
• Bulge of a hernia will appear
Assessing for abdominal mass
Ask patient to tighten abdominal muscles
• A mass in abdominal wall remains palpable
• An intra‐abdominal mass is obscured with contraction
Slide 27JSOMTC, SWMG(A)
Ventral hernias

10
Slide 28JSOMTC, SWMG(A)
Physical Exam Techniques
Auscultation
Always auscultate before palpation and/or percussion
Listen for
• Bowel sounds
Active bowel sounds are ≈5‐34 sounds per min.
Prolonged gurgles of hyperparistalsis(borborygmi)
• Abdominal bruits over the aorta, iliac, renal, and femoral arteries
• Friction rubs over the liver or spleen
Slide 29JSOMTC, SWMG(A)
Auscultation Landmarks
Slide 30JSOMTC, SWMG(A)
Physical Exam Techniques
Light palpation
Start with gentle probing with the hands
• Identify any superficial organs or masses
• Assess for guarding
Voluntary (patient consciously flinches when you touch him)
Involuntary (muscles spasm when you touch the patient, but he cannot control the reaction)
• Palpate with a light, gentle, dipping motion
When moving your hand, raise it off the skin
Move smoothly and feel in all quadrants

11
Slide 31JSOMTC, SWMG(A)
Physical Exam Techniques
Light palpation (cont’d)
Use relaxation techniques to assess voluntary guarding
• Tell the patient to breathe out deeply
• Tell the patient to breathe through the mouth
Slide 32JSOMTC, SWMG(A)
Physical Exam Techniques
Deep palpation
Palpate deeply in all quadrants
• Identify any masses and note their location, size, shape, consistency, tenderness, pulsations, and any mobility
• Correlate palpable findings with percussion notes
Slide 33JSOMTC, SWMG(A)
Examination Techniques when Assessing the Liver, Spleen,
Abdominal Aorta, and Kidneys
12
Slide 34JSOMTC, SWMG(A)
Special Tests
Assessing for Appendicitis
Check for:
• Guarding/rebound tenderness in RLQ
• Rovsing’s sign
Referred rebound tenderness to RLQ from deep palpation in LLQ
• Psoas sign
The patient flexes his thigh against the examiner’s hand (pain = positive sign)
• Obturator sign
Flex the patient’s thigh and rotate the leg internally at the hip (pain = positive sign)
Slide 35JSOMTC, SWMG(A)
Special Tests
Palpating the Liver
Techniques
• Using the left hand to support the back at the level of the 11th and 12th rib
• The right hand presses on the abdomen inferior to the border of the liver and continues to palpate superiorly until the liver border is palpated
• Ask the patient to take a deep breath
Can elicit pain in liver or gallbladder disease and also makes it easier to find the inferior border of the liver
Slide 36JSOMTC, SWMG(A)
Special Techniques
Assessing for Acute Cholecystitis
Murphy’s sign
• RUQ pain with deep palpation during inhalation
13
Slide 37JSOMTC, SWMG(A)
Special Techniques
Palpating the Liver
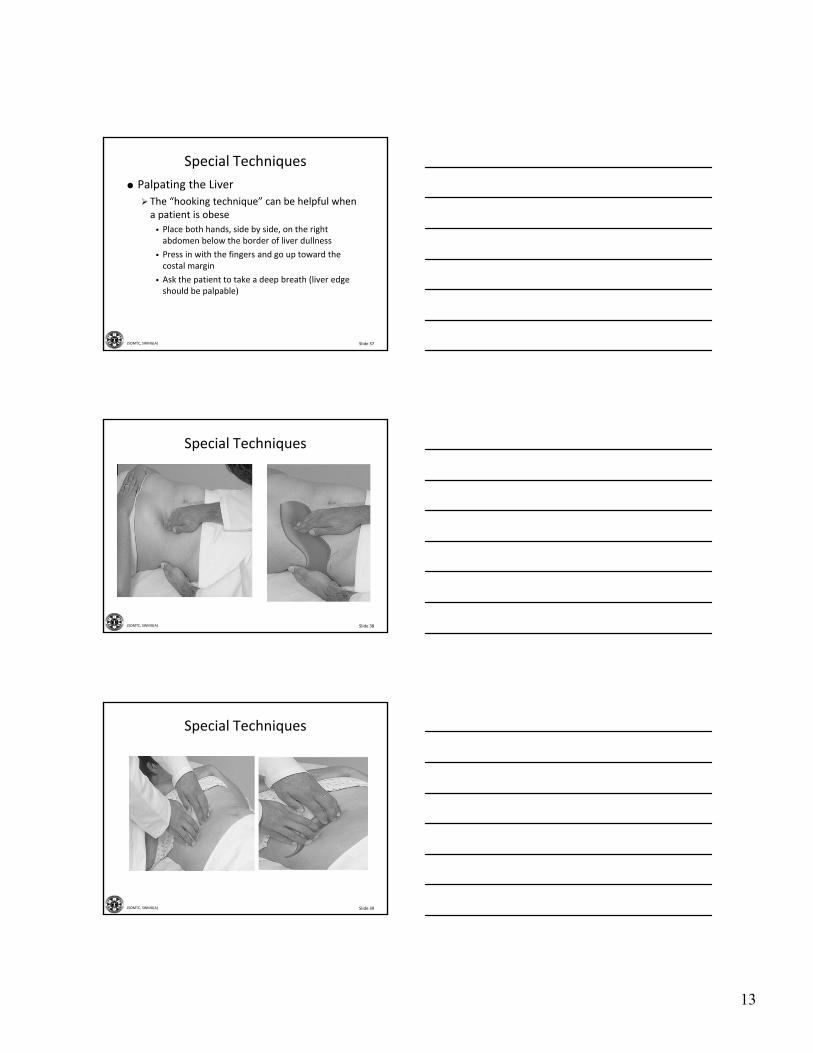
The “hooking technique” can be helpful when a patient is obese
• Place both hands, side by side, on the right abdomen below the border of liver dullness
• Press in with the fingers and go up toward the costal margin
• Ask the patient to take a deep breath (liver edge should be palpable)
Slide 38JSOMTC, SWMG(A)
Special Techniques
Slide 39JSOMTC, SWMG(A)
Special Techniques
14
Slide 40JSOMTC, SWMG(A)
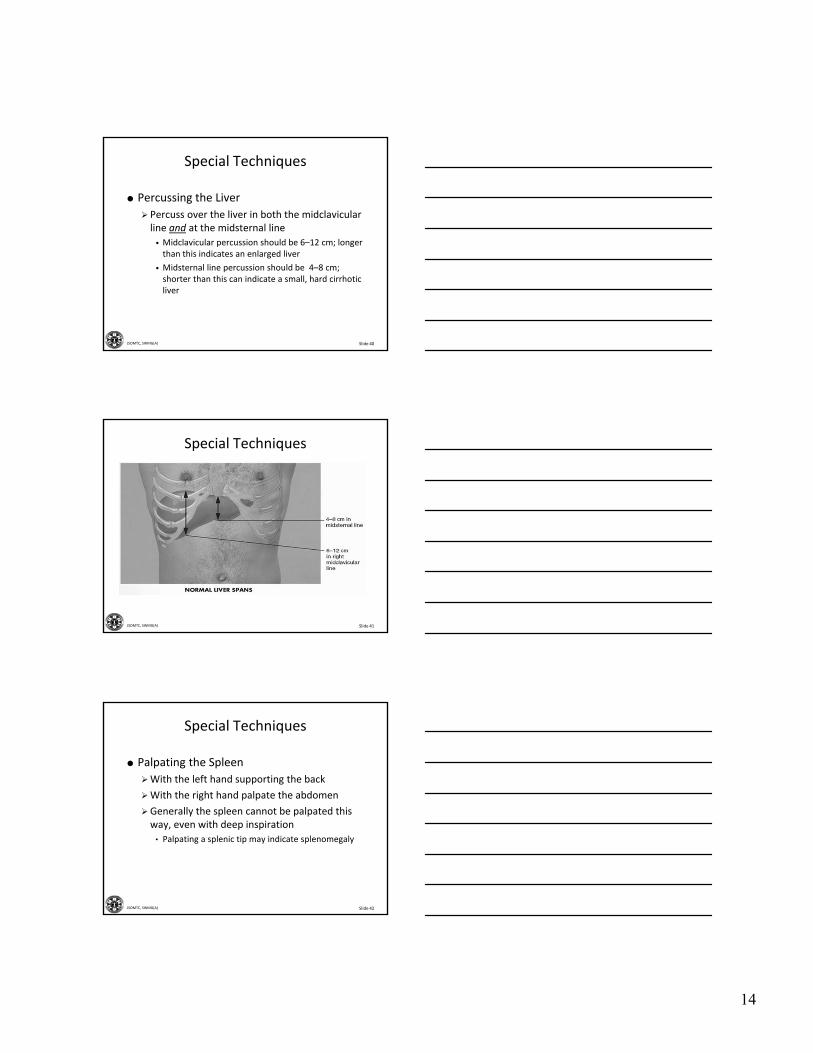
Special Techniques
Percussing the Liver
Percuss over the liver in both the midclavicularline and at the midsternal line
• Midclavicular percussion should be 6–12 cm; longer than this indicates an enlarged liver
• Midsternal line percussion should be 4–8 cm; shorter than this can indicate a small, hard cirrhotic liver
Slide 41JSOMTC, SWMG(A)
Special Techniques
Slide 42JSOMTC, SWMG(A)
Special Techniques
Palpating the Spleen
With the left hand supporting the back
With the right hand palpate the abdomen
Generally the spleen cannot be palpated this way, even with deep inspiration
• Palpating a splenic tip may indicate splenomegaly
15
Slide 43JSOMTC, SWMG(A)
Special Techniques
Slide 44JSOMTC, SWMG(A)
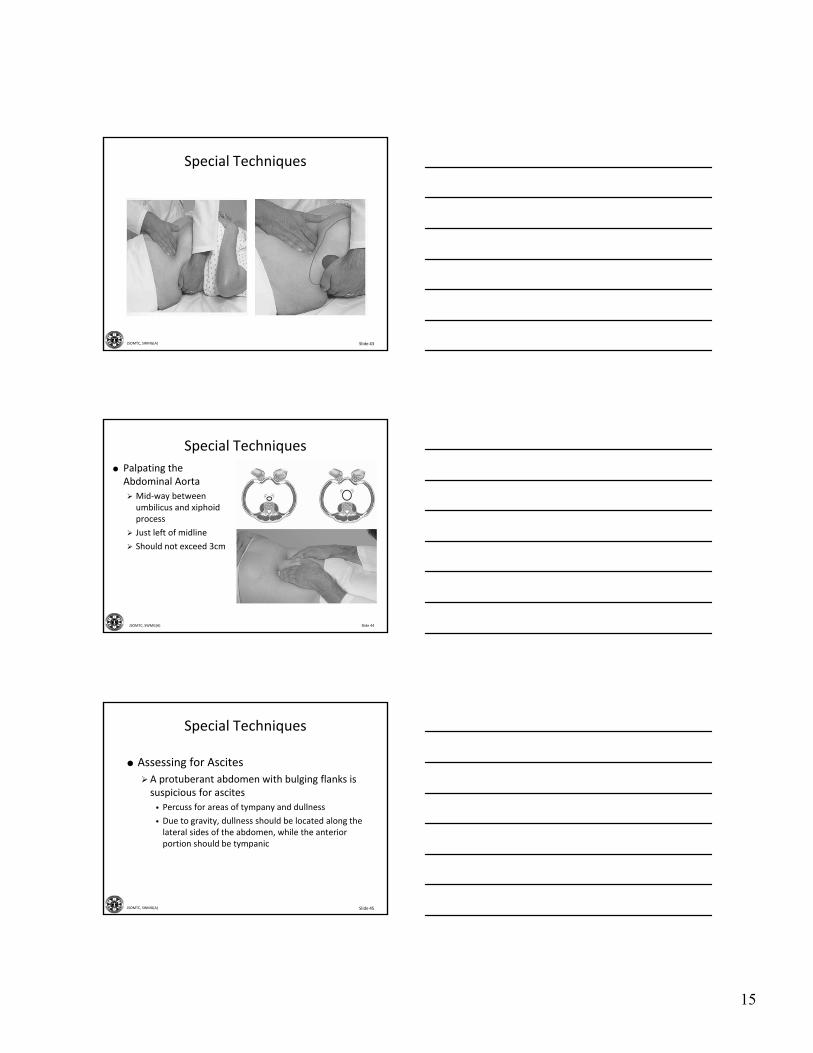
Special Techniques
Palpating the Abdominal Aorta
Mid‐way between umbilicus and xiphoid process
Just left of midline
Should not exceed 3cm
Slide 45JSOMTC, SWMG(A)
Special Techniques
Assessing for Ascites
A protuberant abdomen with bulging flanks is suspicious for ascites
• Percuss for areas of tympany and dullness
• Due to gravity, dullness should be located along the lateral sides of the abdomen, while the anterior portion should be tympanic
16
Slide 46JSOMTC, SWMG(A)
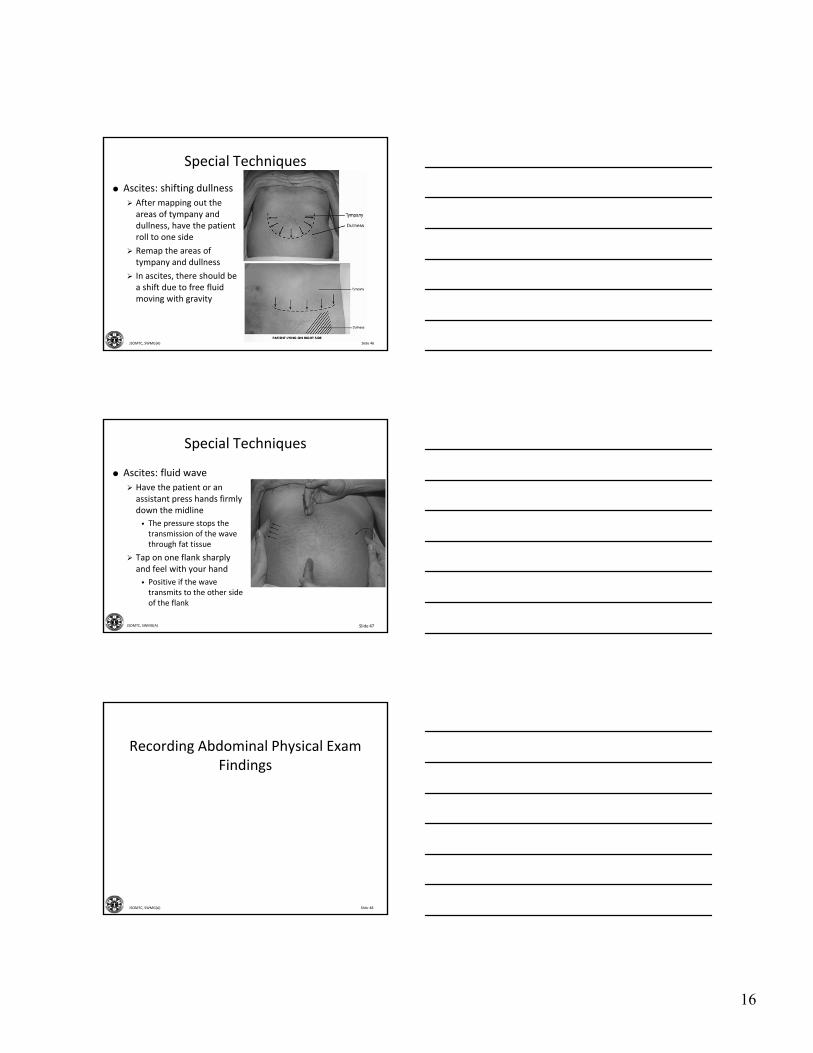
Special Techniques
Ascites: shifting dullness
After mapping out the areas of tympany and dullness, have the patient roll to one side
Remap the areas of tympany and dullness
In ascites, there should be a shift due to free fluid moving with gravity
Slide 47JSOMTC, SWMG(A)
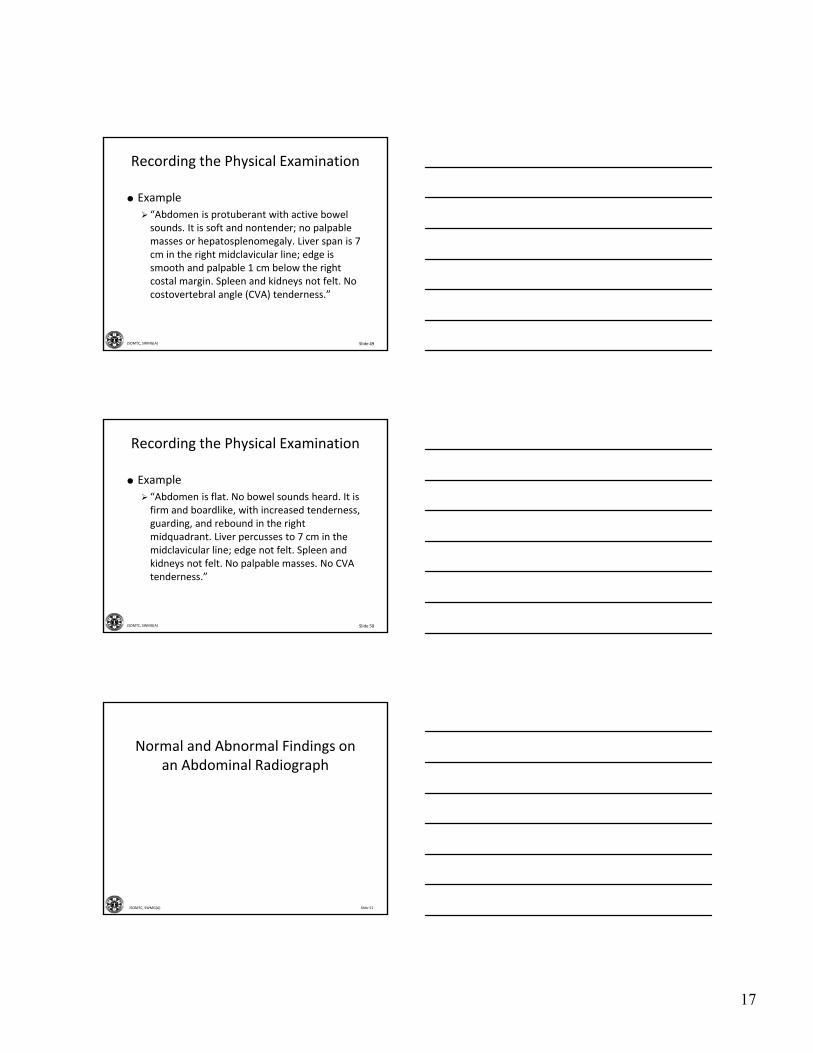
Special Techniques
Ascites: fluid wave
Have the patient or an assistant press hands firmly down the midline
• The pressure stops the transmission of the wave through fat tissue
Tap on one flank sharply and feel with your hand
• Positive if the wave transmits to the other side of the flank
Slide 48JSOMTC, SWMG(A)
Recording Abdominal Physical Exam Findings
17
Slide 49JSOMTC, SWMG(A)
Recording the Physical Examination
Example
“Abdomen is protuberant with active bowel sounds. It is soft and nontender; no palpable masses or hepatosplenomegaly. Liver span is 7 cm in the right midclavicular line; edge is smooth and palpable 1 cm below the right costal margin. Spleen and kidneys not felt. No costovertebral angle (CVA) tenderness.”
Slide 50JSOMTC, SWMG(A)
Recording the Physical Examination
Example
“Abdomen is flat. No bowel sounds heard. It is firm and boardlike, with increased tenderness, guarding, and rebound in the right midquadrant. Liver percusses to 7 cm in the midclavicular line; edge not felt. Spleen and kidneys not felt. No palpable masses. No CVA tenderness.”
Slide 51JSOMTC, SWMG(A)
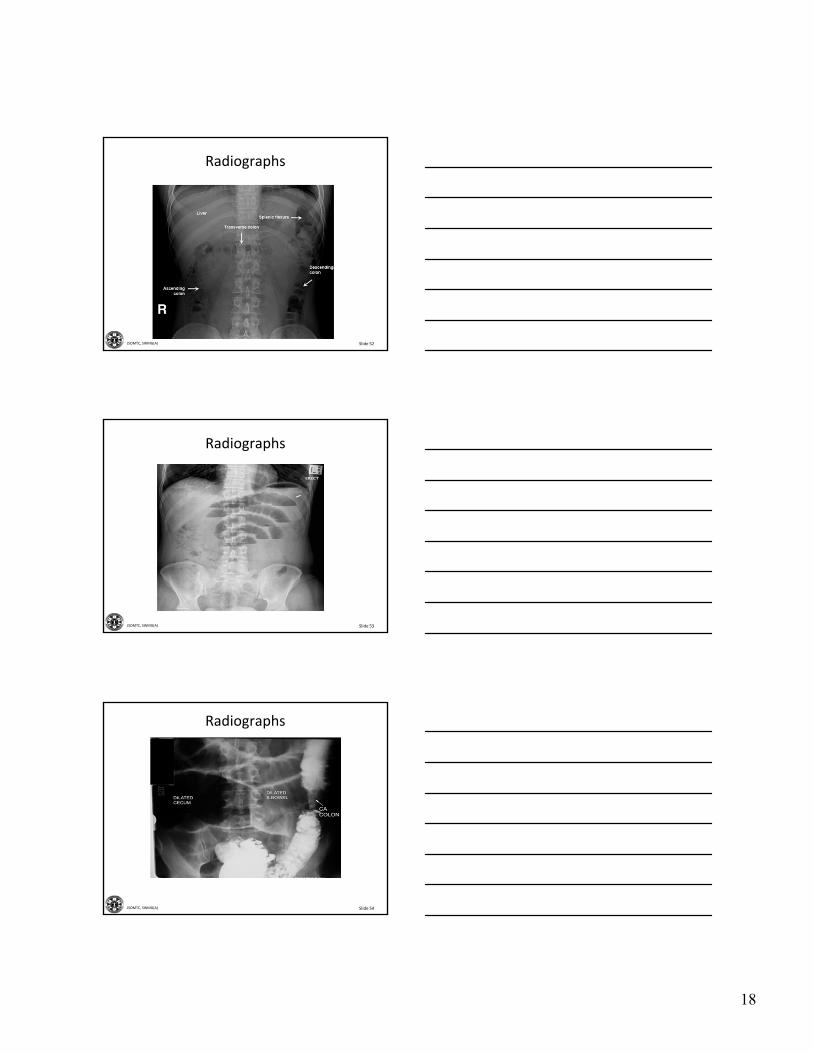
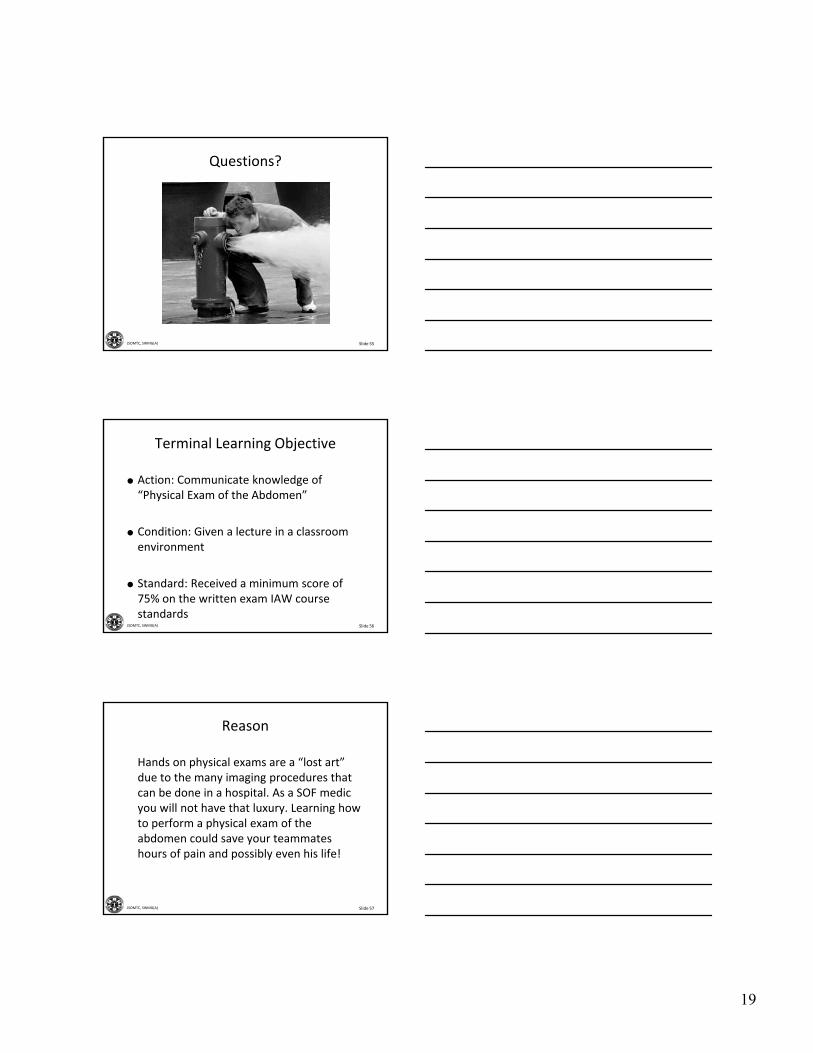
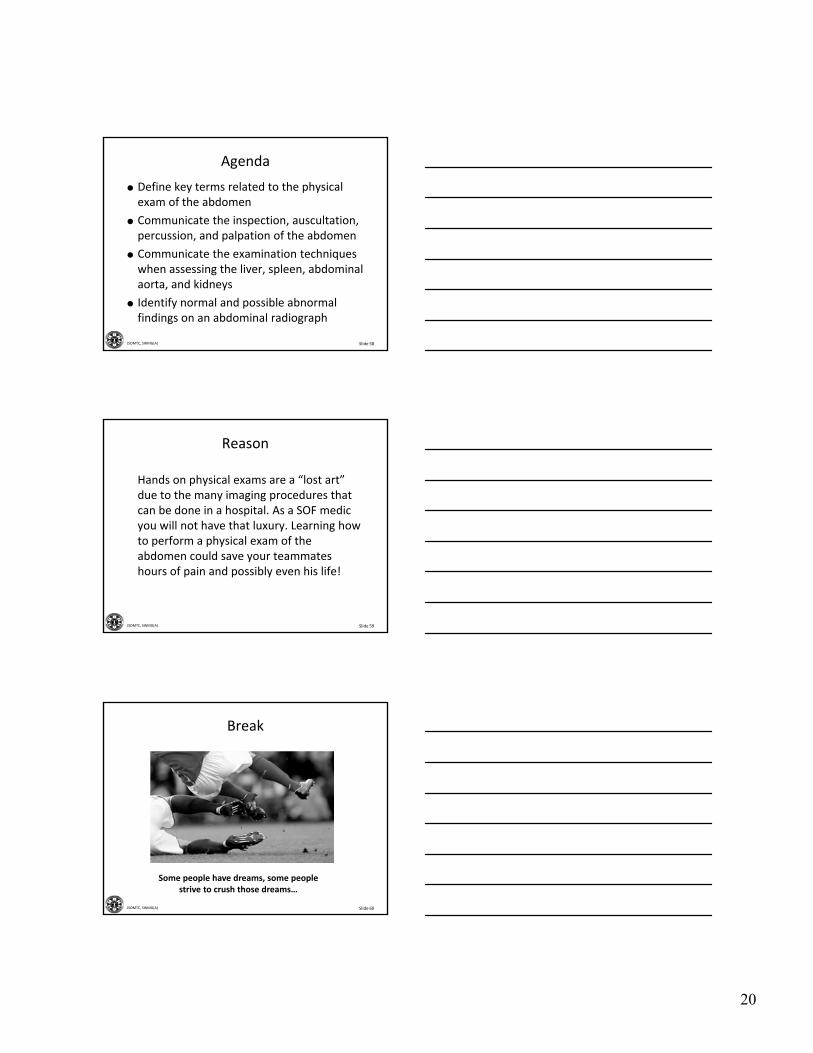
Normal and Abnormal Findings on an Abdominal Radiograph
18
Slide 52JSOMTC, SWMG(A)
Radiographs
Slide 53JSOMTC, SWMG(A)
Radiographs
Slide 54JSOMTC, SWMG(A)
Radiographs
19
Slide 55JSOMTC, SWMG(A)
Questions?
Slide 56JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of “Physical Exam of the Abdomen”
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
Slide 57JSOMTC, SWMG(A)
Reason
Hands on physical exams are a “lost art” due to the many imaging procedures that can be done in a hospital. As a SOF medic you will not have that luxury. Learning how to perform a physical exam of the abdomen could save your teammates hours of pain and possibly even his life!
20
Slide 58JSOMTC, SWMG(A)
Agenda
Define key terms related to the physical exam of the abdomen
Communicate the inspection, auscultation, percussion, and palpation of the abdomen
Communicate the examination techniques when assessing the liver, spleen, abdominal aorta, and kidneys
Identify normal and possible abnormal findings on an abdominal radiograph
Slide 59JSOMTC, SWMG(A)
Reason
Hands on physical exams are a “lost art” due to the many imaging procedures that can be done in a hospital. As a SOF medic you will not have that luxury. Learning how to perform a physical exam of the abdomen could save your teammates hours of pain and possibly even his life!
Slide 60JSOMTC, SWMG(A)
Break
Some people have dreams, some people strive to crush those dreams…
Top Related