







Languages
Pages
Legal


Technology Adoption and
Change Acceleration
Karsten Russell-Wood, MBA, MPH (2015)Remedi SeniorCare

Why Adopt an EHR
Source: MHCC Adoption of Electronic Health Records amongLong Term Care Facilities in Maryland; 2013 Information Brief
Increasing Adoption
• Primary use is financial
• Despite cost (~$350k 5 yr)
Recognized Value
• Quality Assurance and Performance
Improvement (QAPI) initiatives
Further Exploration
• Common integration initiatives (Pharmacy / Lab / RAD / HIE)

Why Adopt an EHR
EHR Value to the 5 Rights:
• Medication documentation compliance
improvement
• Nursing hours to complete Month End
Changeover reduced
• Medication error reductions
• Increased clinical “leverage”
= Cost Recovery & QualityImprovement

Best Practices for Change
• Ensuring successful implementation
• Organizational leadership and vision communication
• Cultural readiness / changemanagement
• Communication and engagement
• Lasting success
• Importance of Goals: Strongaccountability and ownership ofadoption
• Monitoring
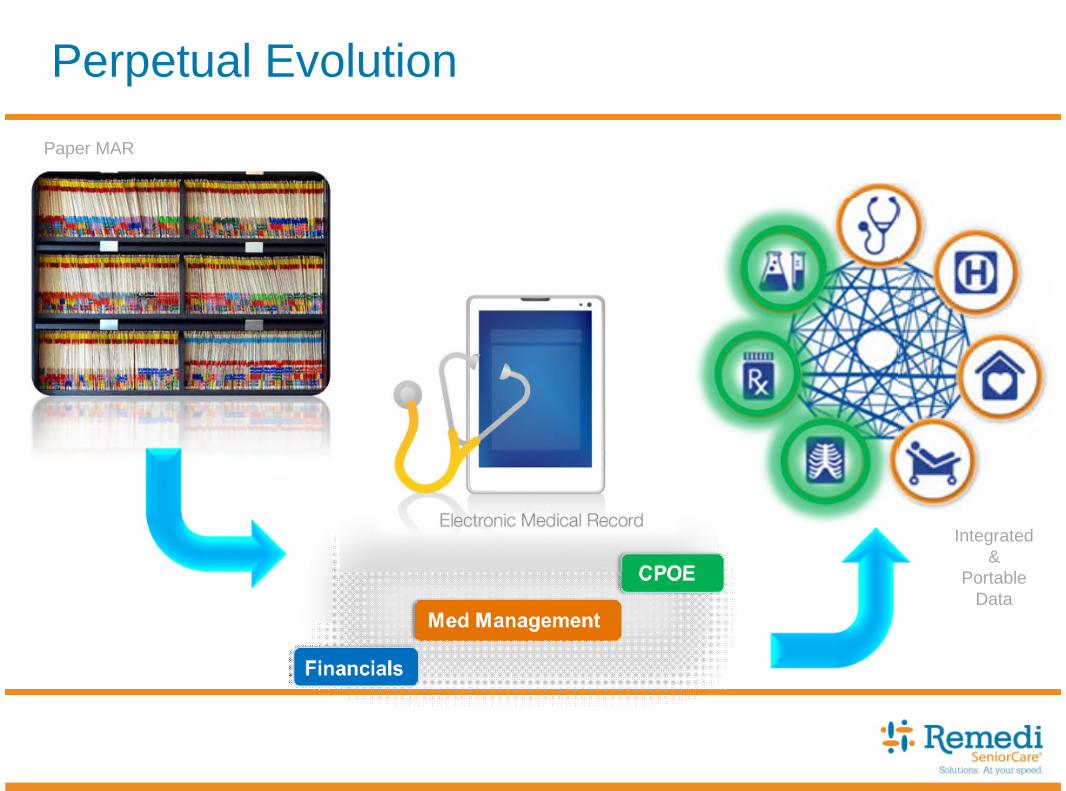
Perpetual Evolution
Paper MAR
Integrated&
PortableData

Interoperability – Objectives
Efficiency
• Single integrated system
• Longitudinal resident care
Safety & Security
• PHI / HIPAA
• State (NY I-Stop) Mandate
Accuracy
• Eliminated double entry
• Trace-ability of data

Interoperability – Setup for Success
Potential pre-requisites
• Technical readiness
• EHR & Pharmacy Interface
Certification (Regulatory Approval
per state)
• Costs / Feature requirements
• Additional quotation process
• Scheduling
• Technology acquisition
• Organizational support
• Executive sponsorship
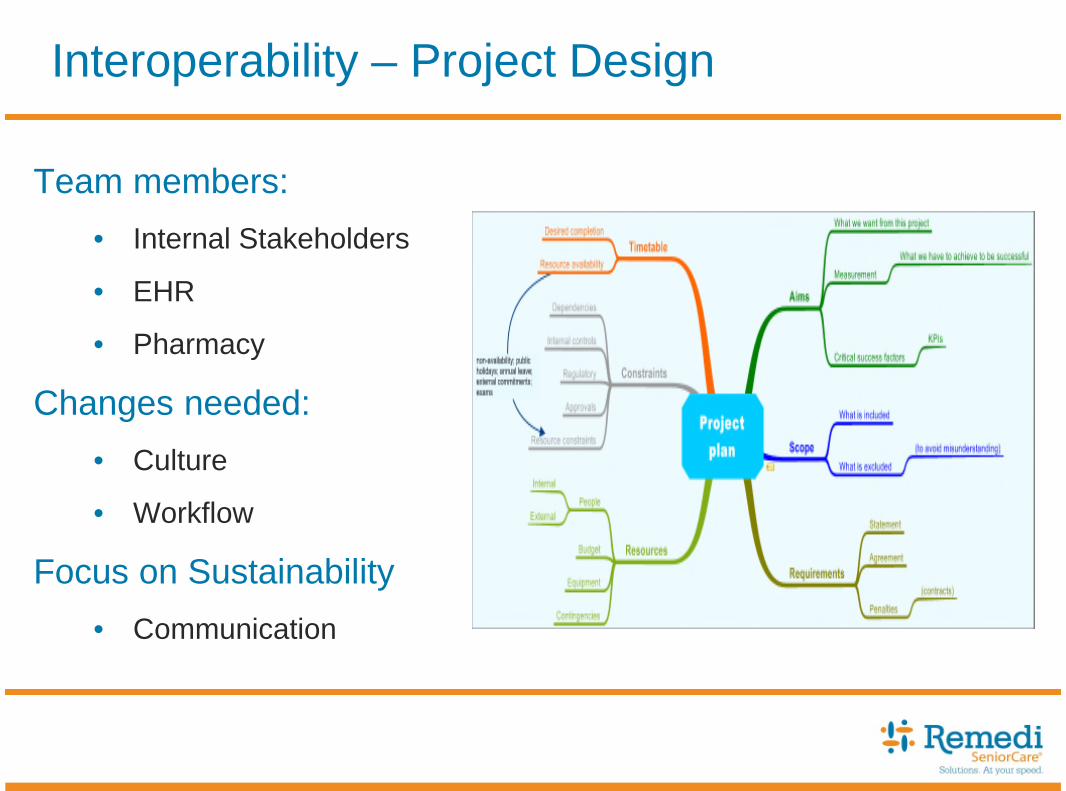
Interoperability – Project Design
Team members:
• Internal Stakeholders
• EHR
• Pharmacy
Changes needed:
• Culture
• Workflow
Focus on Sustainability
• Communication

Interoperability – Project in Practice

Feedback
• Multiple Vendors
• Multiple States
• AL and SNF Facilities
• EHR to Pharmacy
• EHR to Pharmacy to HIE

Feedback – Pre Interface
Accuracy
• Duplicate entry risks
• Clarification requirements / calls
Timeliness
• Multi-step order process
Communication
• Technical disconnected
• People silo mentality

Feedback – Post Interface
Continuity of data• Single record minimizes data errors
• Improved processes (refills)
Bi-directional flow• Feedback on order acknowledgement
• Therapeutic interchange
• Synchronized eMAR
Collaboration• Aligned team across partners (Facility/Pharmacy/EHR)
Improved pharmacy relationship
Increased opportunities• Referral and ACO alignment

Conclusions
Preparedness
• Clear plan and frequent communication
• Check-points to calibrate progress
• Change acceptance
Support
• A vision to “fall back on”
• Facility champions /
Executive Sponsorship
• Counter-measure plan

Top Related