





Languages
Pages
Legal


Stress (Takotsubo) cardiomyopathy and
heart failure: clinical predictors.
I. Nuñez-Gil1, JC. Garcia Rubira1, M. Luaces2, D. Vivas1, B. Ibanez1, B. Ruiz Mateos1,
A. De Agustin1, N. Gonzalo1, C. Macaya1, A. Fernandez Ortiz1
(1) Hospital Clínico San Carlos, Madrid, Spain
(2) Hospital de Fuenlabrada, Fuenlabrada, Spain.

No conflicts of interest.
Partially supported by a grant:
Mutua Madrileña
DISCLOSURES

Takotsubo syndrome (TS) presents features mimicking
acute coronary syndromes.
It is characterized by transient regional systolic
dysfunction of the LV, in the absence of obstructive
coronary artery disease.
Systolic heart failure (HF) is the most common
complication.
INTRODUCTION
Our aim was to examine:
Frequency of HF
Risk factors for HF
Prognosis of HF
Risk Score for..
patients with acute in stay HF complicating TS
(Killip≥2).
OBJETIVES

Retrospective analysis was conducted among 100 patients
prospectively registered between 2002 and 2010.
Inclusion criteria were (Mayo Clinic Crit. , mod. 2008):
Presentation mimicking acute coronary syndrome;
Transient dys/akinesis of LV segments, without significant coronary artery
narrowing;
ECG abnormalities and elevated cardiac troponin/CK;
Absence of: intracranial disease, pheochromocytoma …
… and no previous obstructive coronary artery disease.
METHODS

HF was assesed by means of the Killip classification (I-IV).
K2- dyspnea, pulmonary rales, elevated CVP, S3
K3- pulmonary edema depicted in chest X ray.
K4- SHOCK trial criteria+.
Cardiac cath and complete echocardiogram (<24hrs of admission)
were performed in 100%.
LV recovery was probed by echocardiogram (± CMRI), 100%.
METHODS II
+Hochman, NEJM, 1999.

LV DISFUNCTION

LV RECOVERY

Variables are presented as mean±standard deviation, counts (%),
or median with interquartile range (IQR).
Independent predictors for the development of HF were
estimated by means of a multivariate regression model.
The variables included in the multivariate analysis were chosen
because of the univariate results.
Goodness of fit: Hosmer Lemeshow.
Scores: ROC.
Follow up Events : Kaplan Meier (Breslow).
All analysis were performed using the software package SPPS, v15
(SPPS 2006, Ill, USA)
For all, a p-value<0.05 (two sided), was considered significant.
STATISTICAL ANALYSIS

RESULTS
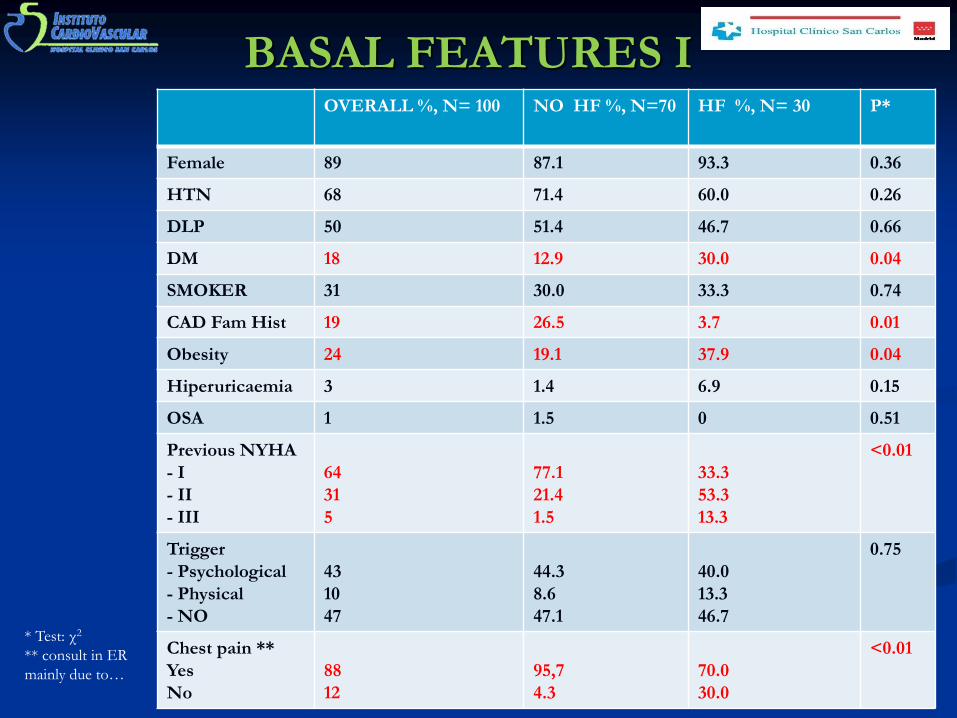
BASAL FEATURES I OVERALL %, N= 100 NO HF %, N=70 HF %, N= 30 P*
Female 89 87.1 93.3 0.36
HTN 68 71.4 60.0 0.26
DLP 50 51.4 46.7 0.66
DM 18 12.9 30.0 0.04
SMOKER 31 30.0 33.3 0.74
CAD Fam Hist 19 26.5 3.7 0.01
Obesity 24 19.1 37.9 0.04
Hiperuricaemia 3 1.4 6.9 0.15
OSA 1 1.5 0 0.51
Previous NYHA
- I
- II
- III
64
31
5
77.1
21.4
1.5
33.3
53.3
13.3
<0.01
Trigger
- Psychological
- Physical
- NO
43
10
47
44.3
8.6
47.1
40.0
13.3
46.7
0.75
Chest pain **
Yes
No
88
12
95,7
4.3
70.0
30.0
<0.01 * Test: χ2
** consult in ER
mainly due to…

BASAL FEATURES II
OVERALL*
N= 100
NO HF *
N= 70
HF *
N= 30
P **
Age (yrs) 68.0±13.2 66.0±13.2 72.9±12.0 0.01
SBP (mmHg) 143.0±35.8 150.1±32.6 127.0±38.0 0.04
HR (bpm) 86.0±21.0 81.4±16.5 96.8±27.3 0.02
Temp (Celsius) 36.2±0.4 36.2±0.4 36.4±0.5 0.43
Creatinine 0.95±0.4 .90±0.2 1.00±0.3 0.10
Leucocyte 9.8±3.3 9.5±2.9 10.6±3.9 0.15
Hb 13.5±1.4 13.5±13.0 13.5±15.0 0.89
Platelets 250.0±70.0 249.1±67.8 251.3±77.3 0.80
Max .Tn I *** 4.2 (2.0-8.9) 3.9 (2.1-7.8) 6.6 (1.8-11.9) 0.27
Max. CK *** 200.5 (123.5-329.8) 196 (121-325) 234 (140-462) 0.23
* Mean ± SD
** Test: Student’s-t.
*** Expressed as median (IQR). Test: Mann Whitney’s -U.

TEST FINDINGS
OVERALL
N= 100
NO HF
N= 70
HF
N= 30
P*
Sinus Rhythm 96 % 95.7 % 96.7 % 0.82
Onset ST elevation 58 % 59.7 % 62.1 % 0.82
ST Elevation 60 % 62.1 % 65.5 % 0.75
ST depression 5 % 3.2 % 10.7 % 0.13
Neg. T waves 87 % 86.4 % 89.3 % 0.69
Max. QTc (V3) 512.8±72.0 499.5±67.8 543.3±73.6 0.01
Onset LVEF (Echo, %)** 48.1±11.0 50.9±10.1 41.8±11.8 <0.01
Valve disease (>mild) 25 % 18.6 % 40.0 % 0.02
LVOT gradient (> 25mmHg) 9 % 7.1 % 13.3 % 0.32
LVEF after F-up (Echo, %)** 63.9±7.2 65.3±7.3 60.4±5.9 <0.01
Emergent cath 33 % 32.3 % 34.5 % 0.83
Right dominance 79 % 81.5 % 75.9 % 0.02
LVEF (Cath, %)** 53.5±11.0 55.3±11.5 48.8±10.1 0.01
* Test: χ2
** Test: Student’s-t.
EKG
TT
Echo
Cardiac
Cath
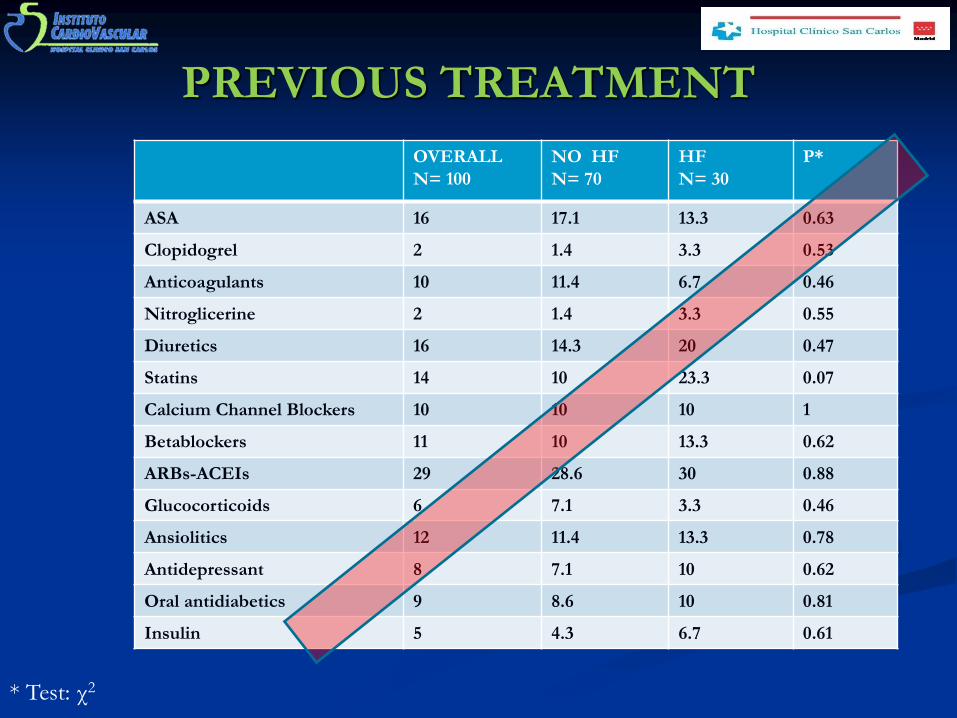
PREVIOUS TREATMENT
OVERALL
N= 100
NO HF
N= 70
HF
N= 30
P*
ASA 16 17.1 13.3 0.63
Clopidogrel 2 1.4 3.3 0.53
Anticoagulants 10 11.4 6.7 0.46
Nitroglicerine 2 1.4 3.3 0.55
Diuretics 16 14.3 20 0.47
Statins 14 10 23.3 0.07
Calcium Channel Blockers 10 10 10 1
Betablockers 11 10 13.3 0.62
ARBs-ACEIs 29 28.6 30 0.88
Glucocorticoids 6 7.1 3.3 0.46
Ansiolitics 12 11.4 13.3 0.78
Antidepressant 8 7.1 10 0.62
Oral antidiabetics 9 8.6 10 0.81
Insulin 5 4.3 6.7 0.61
* Test: χ2

CCU -TREATMENT
OVERALL , %
N= 100
NO HF, %
N= 70
HF , %
N= 30
P*
Inotropic drugs 11 1.4 * * 33.3 <0.001
IABP 2 0 6.7 0.02
Non invasive
Mechanical Ventilation.
3 0 10 0.007
Mechanical Ventilation. 6 1.4 16.7 0.003
Gp IIb/IIIa inhibitors 31 35.7 20.0 0.11
Fibrinolisis 3 4.3 0.0 0.25
* Test: χ2
* * Diuretic Dopamine.

DISCHARGE-TREATMENT
OVERALL
N= 100
NO HF
N= 70
HF
N= 30
P*
ASA 95 95.7 93.3 0.61
Clopidogrel 44 41.4 50.0 0.42
Anticoagulants 90 90.0 90.0 1
Nitroglicerine 64 64.4 63.3 0.92
Diuretics 36 15.7 83.3 <0.001
Statins 71 72.9 66.7 0.53
Calcium Channel Blockers 21 17.1 30.0 0.14
Betablockers 69 70.0 66.7 0.74
ARBs-ACEIs 70 68.6 73.3 0.63
Glucocorticoids 9 8.6 10.0 0.81
Ansiolitics 76 78.6 70.0 0.35
Antidepressant 10 10.0 10.0 1
Oral antidiabetics 9 8.6 10.0 0.73
Insulin 18 17.1 20.0 0.73
* Test: χ2

MAX. KILLIP

IN STAY EVENTS
OVERALL
N= 100
NO HF
N= 70
HF
N= 30
P*
LV Thrombus 5 2.9 10.0 0.14
Arrhythmias 32 27.1 44.3 0.27
New episode 11 10.0 14.8 0.53
Others (infection,
vascular, …)
20 13.6 35.7 0.01
Death 0 0.0 0.0 1
* Test: χ2

TIMES
OVERALL
N= 100
NO HF
N= 70
HF
N= 30
P*
FOLLOW UP 1380 (755-1941) 1534 (822-2109) 1075 (633-1622) 0.04
IN STAY 7 (5-10) 6 (4-9) 9.5 (7-14) <0.001
TIME TO 1ST ECHO 0 (0-1) 0 (0-1) 0 (0-1) 1
TIME TO CATH 1 (0-2) 1 (0-2) 1 (0-2) 0.72
TIME TO F-UP ECHO
(Full LV recovery)
74 (9-174) 74 (6-160) 73 (11-186) 0.15
* Expressed as median (IQR). Test: Mann Whitney’s -U.
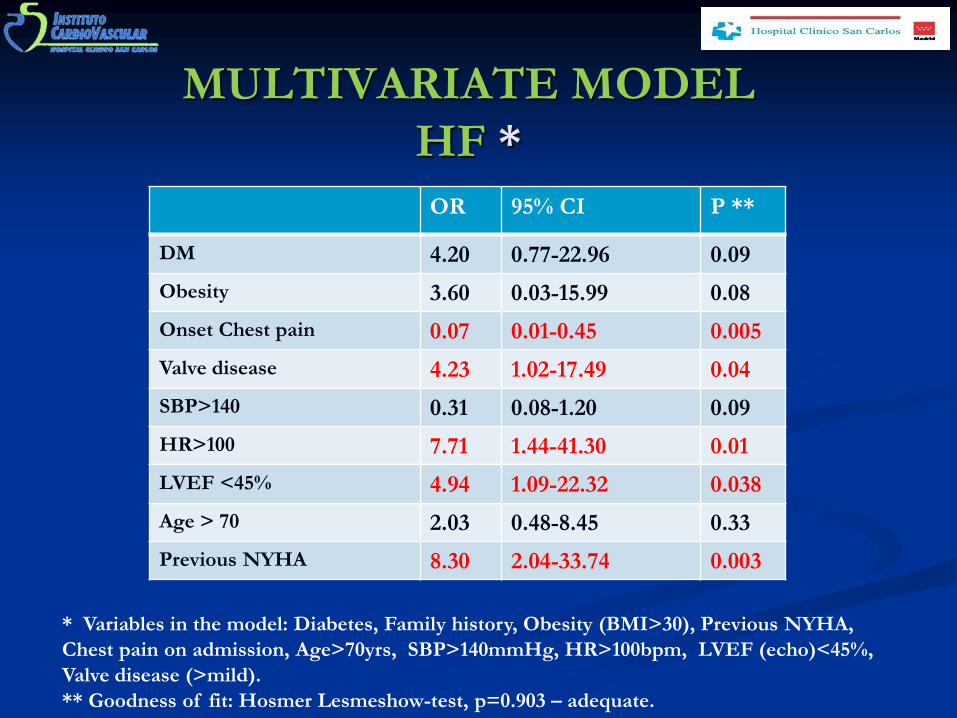
MULTIVARIATE MODEL
HF *
OR 95% CI P **
DM 4.20 0.77-22.96 0.09
Obesity 3.60 0.03-15.99 0.08
Onset Chest pain 0.07 0.01-0.45 0.005
Valve disease 4.23 1.02-17.49 0.04
SBP>140 0.31 0.08-1.20 0.09
HR>100 7.71 1.44-41.30 0.01
LVEF <45% 4.94 1.09-22.32 0.038
Age > 70 2.03 0.48-8.45 0.33
Previous NYHA 8.30 2.04-33.74 0.003
* Variables in the model: Diabetes, Family history, Obesity (BMI>30), Previous NYHA,
Chest pain on admission, Age>70yrs, SBP>140mmHg, HR>100bpm, LVEF (echo)<45%,
Valve disease (>mild).
** Goodness of fit: Hosmer Lesmeshow-test, p=0.903 – adequate.

HF predictors
DM
Obesity
Onset Chest pain
Valve disease
SBP>140
HR>100
LVEF <45%
Previous NYHA

FOLLOW UP
OVERALL
N= 100
NO HF
N= 70
HF
N= 30
P*
MACE 20 15.7 30.0 0.10
READMISSION 16 14.3 20.0 0.47
RECURRENCE 4 1.4 10.3 0.04
DEATH 6 1.4 16.7 0.03
CV DEATH 3 1.4 6.7 0.15
* Test: χ2

FOLLOW UP
Time (days)
MA
CE
F
ree S
urv
ival
No
Yes
Censored
Censored
HF (Killip≥2)
p * =0.034
* Test: Breslow

Time (days)
Su
rviv
al
No
Yes
Censored
Censored
HF (Killip≥2)
FOLLOW UP
p * =0.01
* Test: Breslow
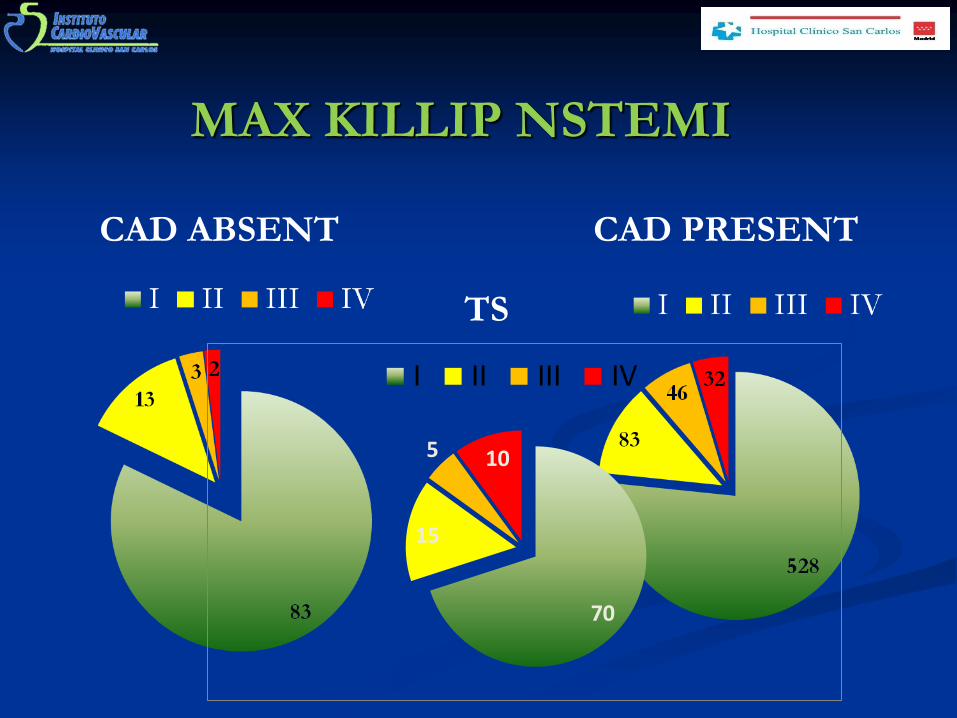
MAX KILLIP NSTEMI
CAD ABSENT CAD PRESENT
70
15
5 10
I II III IV
TS

SCORE MAYO*
Simple.
C-statistic=0. 77, p<0.001
1Point each.
Physical trigger (present).
Age > 70yrs.
LVEF< 40%.
*Madhavan et al. JACC, 2011.
S
1-E
C= 0.741
p< 0.001

SCORE TAKO-SCO I
Simple.
1Point each.
Previous NYHA class.
Onset Chest pain (absent).
HR> 100 bpm.
Valve disease (>mild).
LVEF< 45%.
S
1-E
C= 0.866
p< 0.001
Tako-Sco
Mayo

SCORE TAKO-SCO II
2 Points each.
Previous NYHA class.
Onset Chest pain (absent).
HR > 100 bpm.
Valve disease (>mild).
LVEF< 45%.
1 Point each
DM
Obesity
S-BP<140
S
1-E
C= 0.908
p< 0.001

CONCLUSIONS
In spite of coronary arteries without significant
obstructions, TakoTsubo cardiomyopathy is not lacking
of in-hospital complications.
The most frequent is HF.
HF could be related with future CV events during F-up
and merits early detection and treatment.
Patients with lower previous NYHA class, absent chest
pain at admission, HR> 100 bpm, valve disease
(>mild), LVEF< 45% have an increased probability to
present HF.
We developed a simple score to predict HF.

THANK
YOU
Top Related