







Languages
Pages
Legal


Steno Diabetes Center Peter Rossing Head of Research Professor MD DMSc
20. September 2016
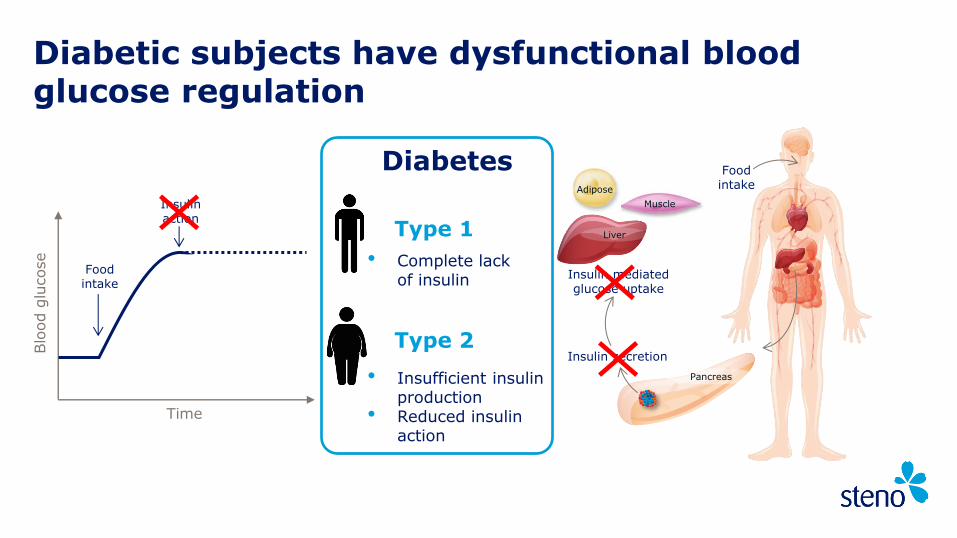
Diabetic subjects have dysfunctional blood glucose regulation
Insulin secretion
Food intake
Blo
od g
lucose
Time
Food intake
Insulin action
Muscle
Adipose
Liver
Pancreas
Insulin mediated glucose uptake
Type 1
• Complete lack of insulin
Type 2
• Insufficient insulin production
• Reduced insulin action
Diabetes

Diabetes pandemic is primarily driven by an increase in number of T2D patients…
Adapted from Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J et al., editors. Harrison’s principles of internal medicine. 18th ed. New York, McGraw Hill; 2011. International Diabetes Federation. IDF Diabetes Atlas, 6th edn. Brussels, Belgium, 2013. http://www.idf.org/diabetesatlas.
T2D risk factors
Family history Lack of exercise Overweight
Unhealthy eating Advancing age High blood glucose during pregnancy
T1D risk factors
Diet early in life Early events in the womb
Environmental risk factors Viral infections
The number of T1D patients is also increasing
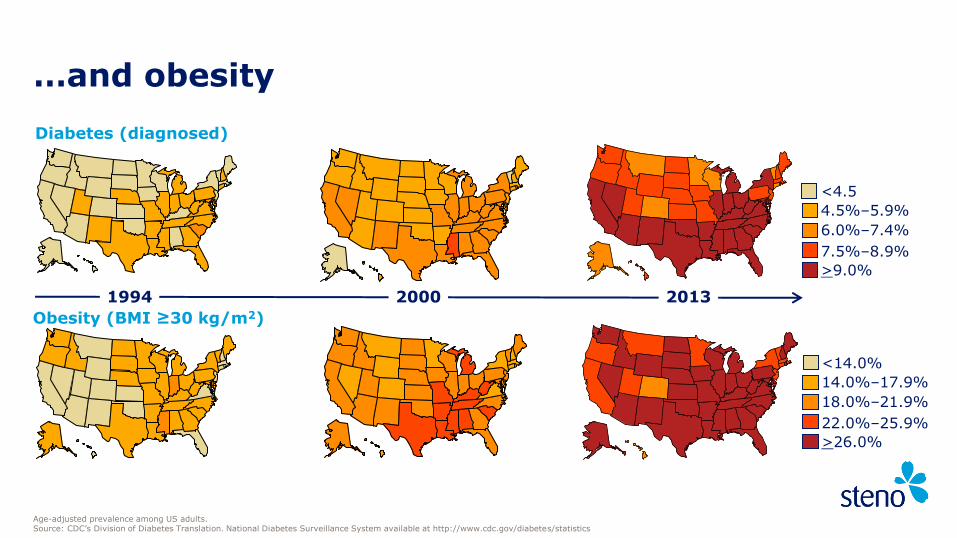
…and obesity
Age-adjusted prevalence among US adults. Source: CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
<4.5
4.5%–5.9%
6.0%–7.4%
>9.0%
7.5%–8.9%
Diabetes (diagnosed)
1994 2013 2000
<14.0%
14.0%–17.9%
18.0%–21.9%
>26.0%
22.0%–25.9%
Obesity (BMI ≥30 kg/m2)
Founded in 1932 to improve clinical care of patients and to understand diabetes

More than 80 years experience with diabetes care

100% specialised in diabetes
Treats 5,700 patients
230 employees
Research in all stages of DM from prevention to late complications
Vision to be leading in diabetes care and translational research
Steno Diabetes Center 2016

Four major areas at Steno
Research Health Promotion
Research
Patient Care Education

Our vision is to become leaders in diabetes care and translational research with focus on early disease and prevention

Public Private Partnership

Capital Region of
Copenhagen and other
regions
Novo Nordisk Foundation
Novo Nordisk A/S
External research
grants
Other revenue
Steno Diabetes Center Funding

Strategic Alliances
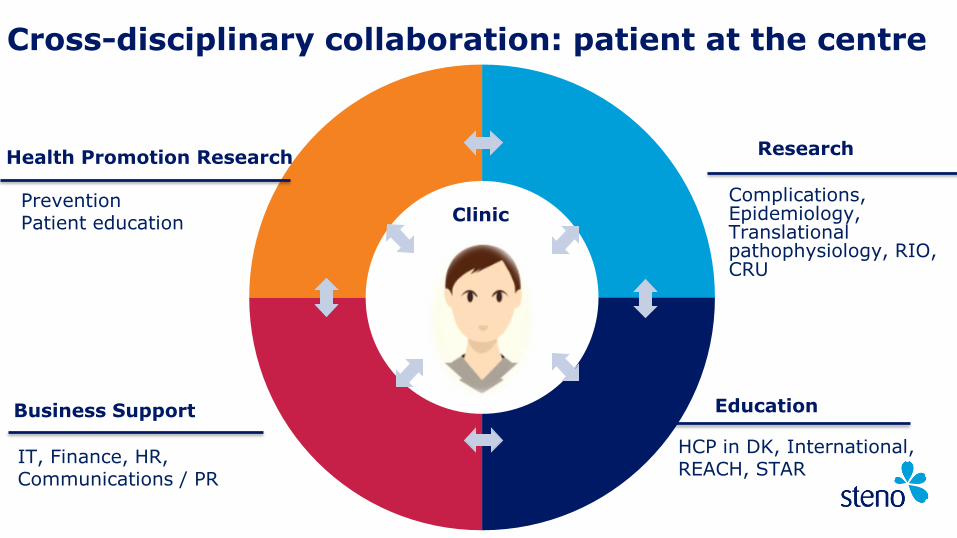
Research
Business Support
Clinic
IT, Finance, HR, Communications / PR
Complications, Epidemiology, Translational pathophysiology, RIO, CRU
HCP in DK, International, REACH, STAR
Prevention Patient education
Education
Cross-disciplinary collaboration: patient at the centre
Health Promotion Research
Steno Diabetes Center
Gentofte Hospital
Herlev Hospital
Nordsjællands Hospital
Hvidovre Hospital
Glostrup Hospital
… and others
Steno Diabetes Center Copenhagen

Future vision for national DM network
SDCJ
SDCF
SDCC
15
A world-class diabetes center is created - Steno Diabetes Center Copenhagen
… FOCUSED ON THE PATIENT
Vision of Region H as internationally leading within diabetes treatment and
research, and of developing tomorrows patient-focused treatment methods
– to benefit all diabetes patients
A LEADING CENTER OF EXCELLENCE…
• SDCC to lead the way and ensure world-class patient-focused treatment options
• Diabetes patients and citizens in the capital region to be the natural focus point
• SDCC to drive a joint improvement of diabetes activities with all partners in the capital region
16
SDCC’s ambition is built on a large patient-base and new joint facilities in 2020
• The ambition to create a world-class center is achieved by consolidating all diabetes activities in a single unified center with a larger patient-base
• A new center is build next to Herlev Hospital, where surroundings and infrastructure is designed to optimize functionality and to benefit patients
• In 2020 the center gathers 11-13,000 patients from region Midt, including newly-diagnosed type 1 patients, children and diabetes-pump patients from the entire region
REALIZING THE AMBITION

17
Pathophysiology
Systems Medicine
Complications
Epidemiology
Steno Research

First class clinical care and outcomes
Translational research
Incubation hub & access to patients
Deep phenotyping & Biobank
Talent attraction and career development
Prognostics and prevention of complications
Steno’s role as research centre
Research with focus on translation
Close link with clinic
Results implemented in our clinic to improve patient care
Collaboration national and international

Epid
em
iolo
gy
Syste
ms m
edic
ine
Clin
ical R
esearc
h
Genetic
s
People at risk
Type 2 Diabetes
Type 1 Diabetes
Diabetes Complications
Health
Pro
motio
n

Metabolite profile, clinical and lifestyle data
Predictive patient profile
Arrival Follow-up 1
Arrival
Treatment A
Follow-up 2
Treatment B
Follow-up 1
Treatment C
Evidence-based medicine (treatment-failure approach in clinical practice)
Personalised medicine (prediction of real life EBM-benefit in clinical practice)
A?
B? C?
Personalised Treatment
Our vision translate comprehensive patient phenotyping/profiling into the clinic

Diabetes is a leading risk factor for renal impairment
2,3%
2,0%
17,5% Diabetes
High blood pressure
Glomerulonephritis
Cystic diseases
Urologic diseases
Other
US Renal Data System 2007 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD.

Costs of complications in patients with diabetes: the Helsinki Study
395 637
9625
7418
0
2000
4000
6000
8000
10000
Excess cost of T2D Excess costs of T1D
Without complications
With complications
24
12x
Hospital days/1
00 p
atient
years
Mean excess costs of healthcare of people with diabetes (and without complications) by type of diabetes
Finnish Diabetes Association. DEHKO 2000–2010. Finnish Diabetes Association 2001

Wash-outRun-in
Allopurinol 100-400 mg(to keep serum uric acid between 2.5 and 4.5 mg/dl)
RandomizationEnd of
intervention
Screening visit
iGFR iGFR
Placebo
iGFRiGFRiGFR
RASB Standardization & BP control
Wash-outRun-in
Allopurinol 100-400 mg(to keep serum uric acid between 2.5 and 4.5 mg/dl)
RandomizationEnd of
interventionEnd of
intervention
Screening visit
iGFRiGFR iGFRiGFR
Placebo
iGFRiGFRiGFRiGFRiGFRiGFR
RASB Standardization & BP control 3 years
Study design

Urine
Sample
Capillary Electrophoresis
Mass Spectrometry
Ionization
Report
Data Storage
and
Evaluation
Diagnostic Disease specific
Biomarker pattern
Standard tests for diabetic nephropathy: - moderate specificity and sensitivity at early stages of disease
Urinary proteome analysis: - offers the prospect of detecting diabetic nephropathy earlier in the preclinical phase, enabling targeted treatment at an earlier stage
New marker Early and robust
Existing markers
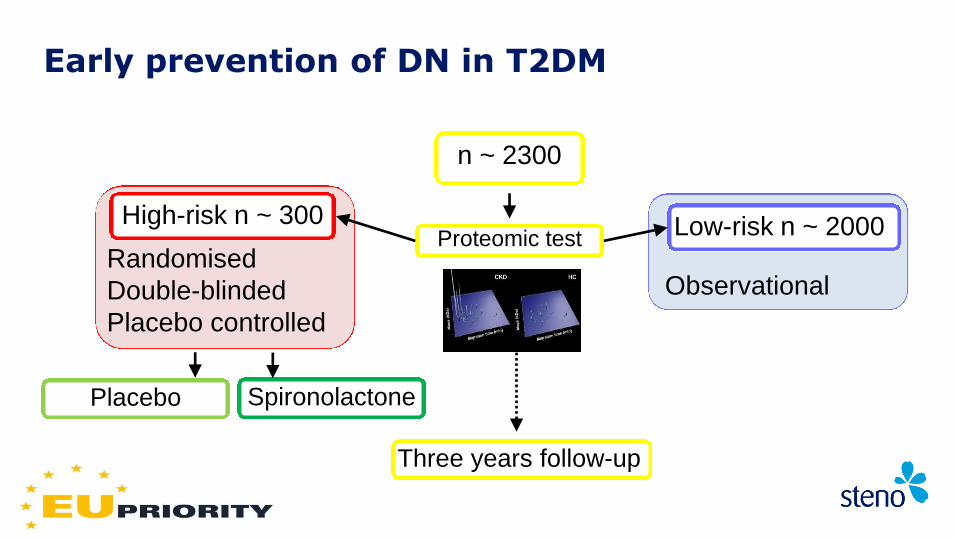
Early prevention of DN in T2DM
n ~ 2300
Proteomic test Randomised
Double-blinded
Placebo controlled
High-risk n ~ 300
Observational
Low-risk n ~ 2000
Three years follow-up
Placebo Spironolactone

PROTON PeRsOnalising Treatment Of diabetic Nephropathy Moving from albuminuria to multidimensional characterisation and intervention
Professor Peter Rossing
Professor Per-Henrik Groop
Professor Andrzej Krolewski
Professor Dick de Zeeuw
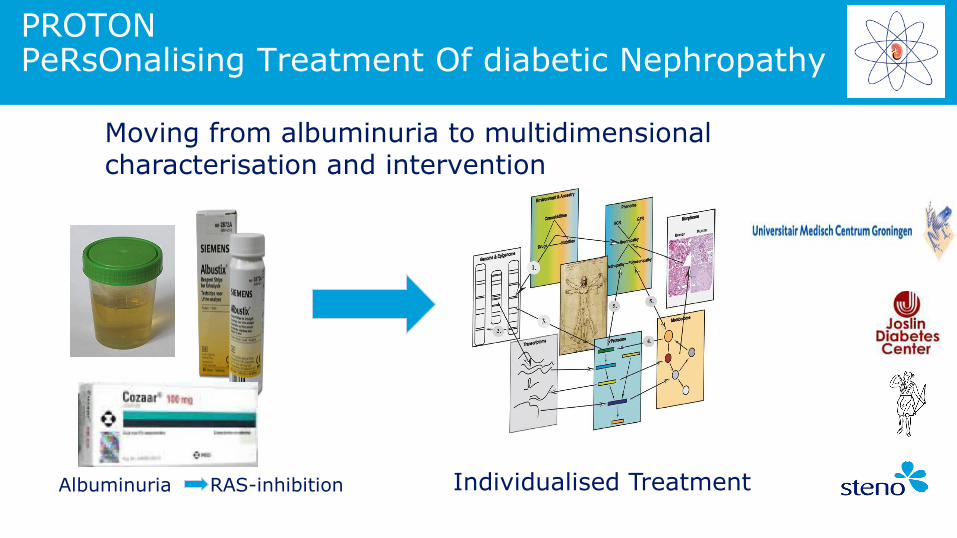
Albuminuria RAS-inhibition Individualised Treatment
PROTON PeRsOnalising Treatment Of diabetic Nephropathy
Moving from albuminuria to multidimensional characterisation and intervention

Population-based cohort-studies
The Addition-Pro study: progression to diabetes
Whitehall II study:
Latent class trajectory analysis
Vistisen et al. PLOS Medicine 2014
Greenland studies: genetic risk Moltke et al. Nature 2014
Screening status 2001-2006
ADDITION-PRO Follow-up 2009-1011
Non-classifiable
NGT iIFG iIGT IFG+IGT SDM KDM Total
n % N % N % N % N % N % N % N
Low risk 11 5.7 149 76.8 18 9.3 5 2.6 3 1.6 5 2.6 3 1.6 194
Normoglycaemia 21 1.9 741 67.4 109 9.9 77 7.0 52 4.7 60 5.5 40 3.6 1100
iIFG 0 0 101 28.0 84 23.3 13 3.6 29 8.0 29 8.0 105 29.1 361
iIGT 3 1.2 60 23.5 13 5.1 39 13.3 36 14.1 37 14.5 67 26.2 255
IFG+IGT 3 1.6 20 10.9 8 4.3 11 6.0 22 12.0 25 13.7 94 51.4 183
38 1071 232 145 142 156 309 2093

Novel options with systems biology approach

Growing teams of researchers
Major focus on the biology and clinical progression to complications
Closely linked with daily clinical practice
New laboratory methodologies: lipid and metabolomics
Prognostics and prevention of complications
Summary: Steno Diabetes Center Research

Steno Clinic

Steno Clinic - A unique Public Private Partnership -
Center-based health care
Collaborative Clinical Care for 5700 patients
Screening for and treating Complications
Team-based care delivery
Education of patients
One-stop shop
Quality Management

24 hr Phone Service
Foot Clinic
Type 2 Clinic
Day Hospital
Adolescent Clinic
Insulin Pump Clinic
Pregnancy Clinic
Eye Clinic
Steno Clinic - Creating an even flow -
Outpatient Clinic
Ambulatory
Day Hospital/ Type 2 Clinic
Specialist Ambulatory
Steno Clinic - Creating an even flow -
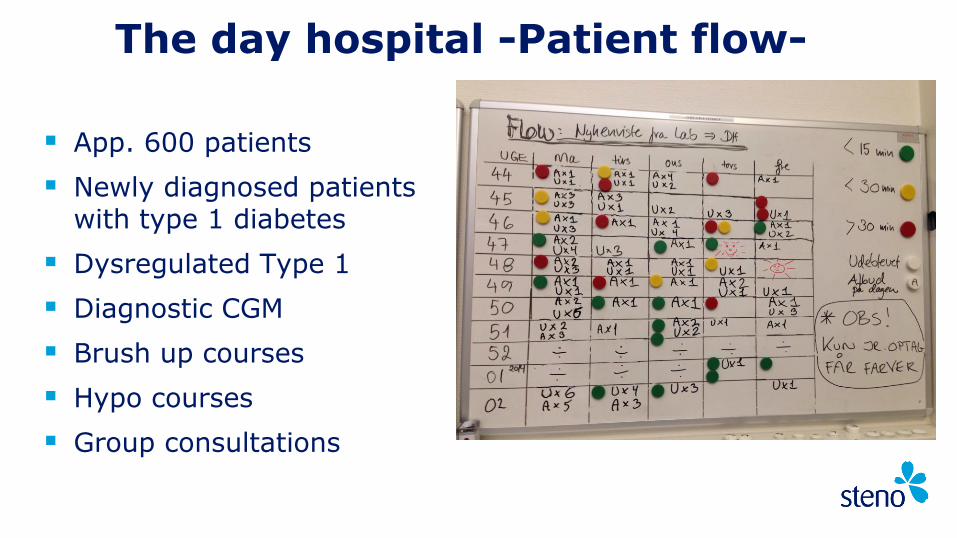
App. 600 patients
Newly diagnosed patients with type 1 diabetes
Dysregulated Type 1
Diagnostic CGM
Brush up courses
Hypo courses
Group consultations
The day hospital -Patient flow-

400 referrals annually
The type 2 team: 3 diabetes nurses, 1
endocrinologist, 1 dietician, 1 trainee doctor
8-12 month educational course (approx. 6 visits)
Type 2 clinic
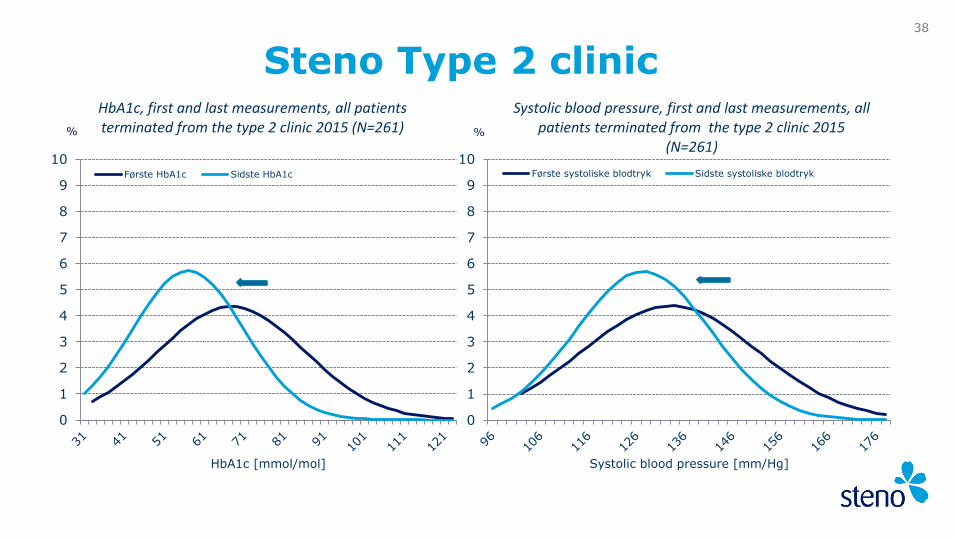
Steno Type 2 clinic 38
0
1
2
3
4
5
6
7
8
9
10
HbA1c [mmol/mol]
HbA1c, first and last measurements, all patients terminated from the type 2 clinic 2015 (N=261)
Første HbA1c Sidste HbA1c
%
0
1
2
3
4
5
6
7
8
9
10
Systolic blood pressure [mm/Hg]
Systolic blood pressure, first and last measurements, all patients terminated from the type 2 clinic 2015
(N=261)
Første systoliske blodtryk Sidste systoliske blodtryk
%
The Steno Pump Clinic
830 pump patients
Scandinavias largest pump clinic
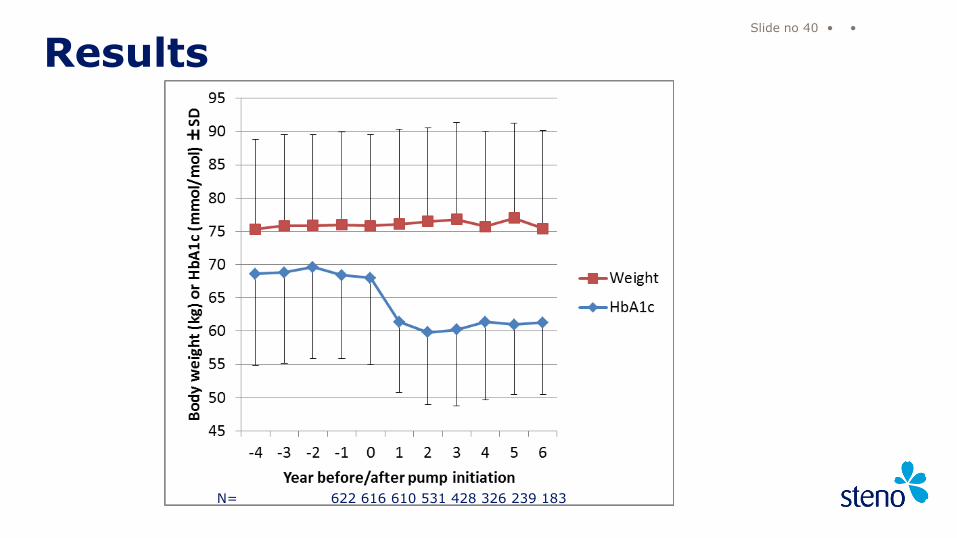
Results
Slide no 40 • •
N= 622 616 610 531 428 326 239 183
Steno Diabetes Center
“My Steno” – web-based diabetes care

Screening for diabetic retinopathy - nurse driven
Organised and run in collaboration with Dept. of Ophthalmology Glostrup Hospital
Nurses screen and assess retinal photos
Reading center for screening clinics in other hospitals
App. 4600 photo screenings pr year
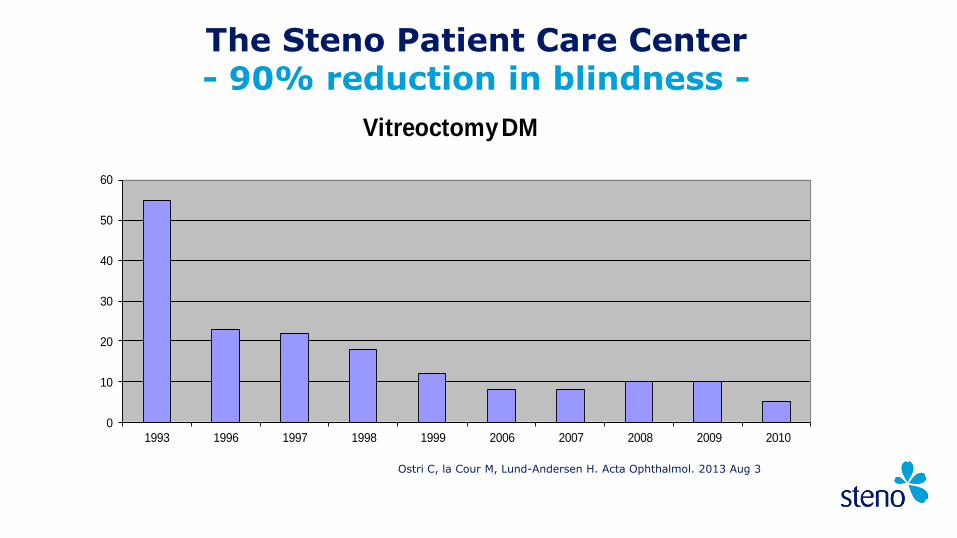
The Steno Patient Care Center - special attention to special needs -
0
10
20
30
40
50
60
1993 1996 1997 1998 1999 2006 2007 2008 2009 2010
Vitreoctomy DM
The Steno Patient Care Center - 90% reduction in blindness -
Ostri C, la Cour M, Lund-Andersen H. Acta Ophthalmol. 2013 Aug 3

Steno Clinic
52
56
60
64
68
72
76
All
Type 1
Type 2
0
10
20
30
40
50
60
70
80
90
100
Per
cen
t
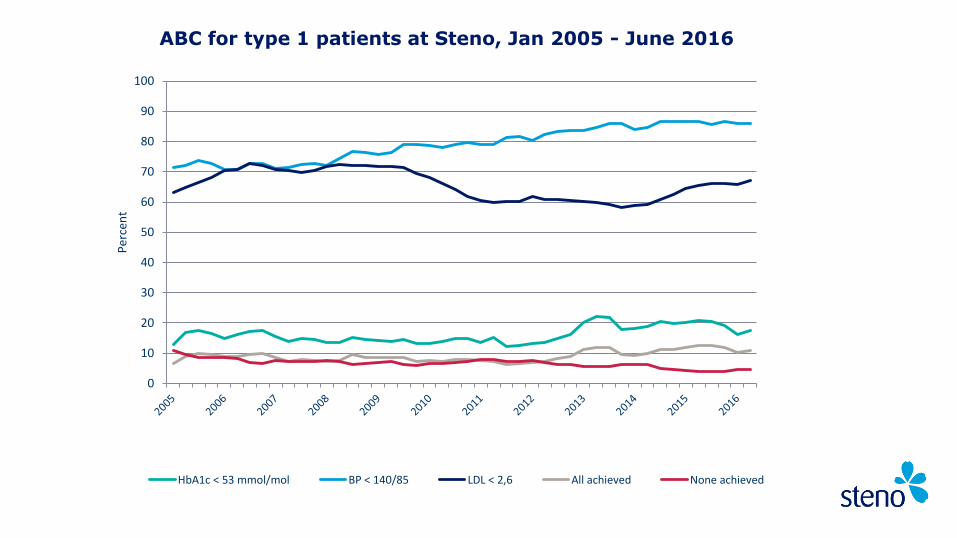
HbA1c < 53 mmol/mol BP < 140/85 LDL < 2,6 All achieved None achieved
ABC for type 1 patients at Steno, Jan 2005 - June 2016

G Andrésdóttir et al Diabetes Care, 2014;37(6):1660-7
2000-2010
1983-2002
P<0.05
T2D
Steno Clinic - Reduction in Mortality -

Diabetes nurse Orthopaedic Surgeon
Diabetologist External Departments
Podiatrist Coordinator
The Steno Foot-care Team
The podiatrist is a key member of the multidisciplinary team, with an important role, both in prevention and treatment of the diabetic foot
Outpatient Clinic: App. 3500 T1D and 2000 T2D patient
Staff in the foot-clinic
4 podiatrists
1 full-time (teamleader) and 3 part-time
1 orthopaedic surgeon (6 hours per week)
1 diabetologist associated to the foot-clinic
Diabetes nurse and doctor if needed
Multidisciplinary foot-clinic
App. 3000 consultations per year
Open 5 days a week (Mon-Fri)
Daily visits, either according to plan, or with an acute issue
Daily telephone service
Education of patients and staff
Research and development projects
Organisation of foot-care at Steno Diabetes Center
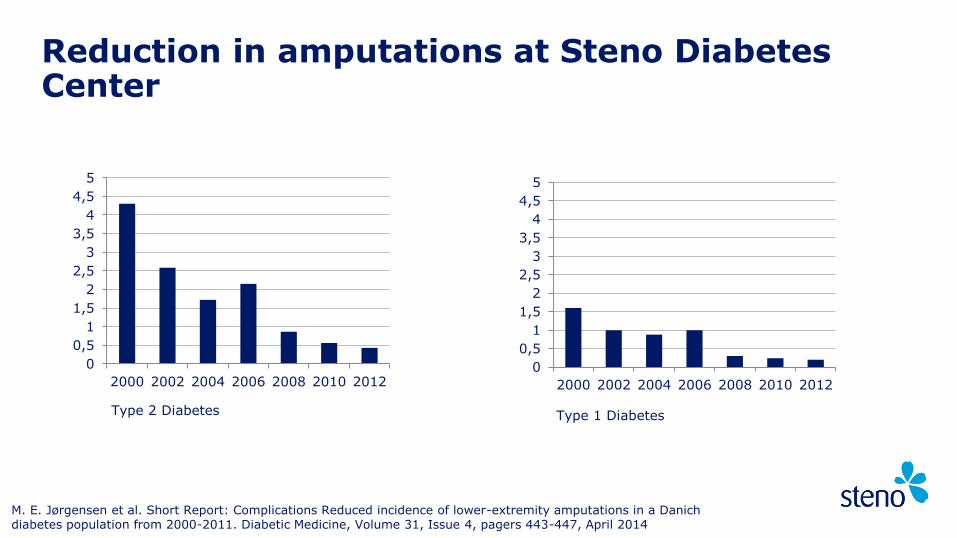
Reduction in amputations at Steno Diabetes Center
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
2000 2002 2004 2006 2008 2010 20120
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
2000 2002 2004 2006 2008 2010 2012
Type 2 Diabetes Type 1 Diabetes
M. E. Jørgensen et al. Short Report: Complications Reduced incidence of lower-extremity amputations in a Danich diabetes population from 2000-2011. Diabetic Medicine, Volume 31, Issue 4, pagers 443-447, April 2014

The yearly costs for running
our foot-clinic incl.orthopaedic expertice =
The costs of
3 major amputations
Steno foot-clinic
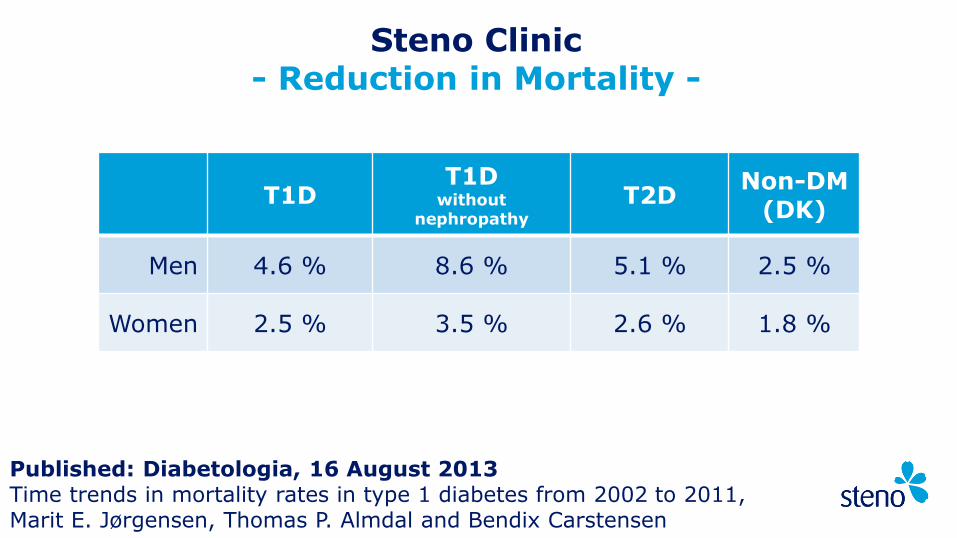
T1D T1D
without nephropathy
T2D Non-DM
(DK)
Men 4.6 % 8.6 % 5.1 % 2.5 %
Women 2.5 % 3.5 % 2.6 % 1.8 %
Published: Diabetologia, 16 August 2013 Time trends in mortality rates in type 1 diabetes from 2002 to 2011, Marit E. Jørgensen, Thomas P. Almdal and Bendix Carstensen
Steno Clinic - Reduction in Mortality -

Steno Clinic - The Annual Survey of Patient Satisfaction -
LUP overview dimensions: • Patient engagement (AA) • Information (AA) • Service level (AA) • Overall satisfaction (AA) • Personnel (OA) • Waiting times (OA)
Questions ?
Top Related