







Languages
Pages
Legal

1
Stakeholder and Expert Perspectives on Dietary Sodium Reductions
in Thailand, 2017 Jahn Jaramillo, WHO Intern, M.P.H. Candidate, University of Washington
Summary Background As part of the global and national strategy for prevention and control of noncommunicable diseases
(NCDs), Thailand has set targets to reduce the prevalence of raised blood pressure by 25% and decrease population intake
of sodium by 30% by 2025. Passage of a resolution on sodium reduction by the National Health Assembly in 2015, and
development of a national strategy of reduction of Salt and Sodium Consumption (SALTS Strategy 2016-2025),
demonstrate Thailand’s commitment to reducing the risk of heart disease and other related chronic illnesses. The
perspectives of stakeholders and champions in the field of NCDs and salt reduction are imperative for ensuring optimal
operationalization of the current salt strategy. The aim of this report is to provide an up-to-date scan of the landscape and
ongoing research in the field, to identify barriers to policy implementation, and to obtain key recommendations from
national stakeholders and experts. The report intends to expand available information on salt reduction in Thailand to
showcase ongoing efforts and offer ways to strengthen national initiatives.
Methods Available literature on salt reduction in Thailand were accessed in order to assess the current situation. In-depth
interviews with national stakeholders and experts were also conducted. Interviewees were asked about perceived
challenges to effective policy implementation, recommendations to overcoming barriers identified, and ongoing research
in their field. Barriers and recommendations obtained were reviewed.
Findings A total of 8 studies were found from 2009-2016 that measured sodium intake and dietary sources in Thailand to
date. In total, 15 salt experts and stakeholders were interviewed representing academia, government, and the industry
sectors. National stakeholders and experts identified barriers to implementation of the SALTS Strategy in the areas of:
prioritization of interventions and leadership, inter and intra agency collaboration, marketing and health promotion,
industry approach and timing, and research priorities. Stakeholder recommendations were categorized in monitoring and
evaluation, policy and strategy, consumer education and behavior modification, and research. There was clear consensus
that the strategy was relatively new and gaining momentum.
Value This report identifies current existing literature on sodium research and describes barriers to – and
recommendations for – advancing sodium reduction policy implementation in Thailand from the perspectives of experts
and stakeholders.
Interpretation Effective implementation of the action plan under the sodium and salt reduction policy will require
continuous surveillance, monitoring and evaluation activities, bridging the strategy with other national initiatives,
increased coordination amongst diverse stakeholders, prioritization of interventions focused on street food/food shops, and
additional investment in food science, nutrition research, and consumer education.
Introduction Non-communicable diseases account for 70% of all
deaths worldwide1, with a similar pattern occurring in
Southeast Asia2. In Thailand, hypertension is a major
cause of cardiovascular disease (CVD)3,4,5
, which kills
17 million6 people each year. In particular, higher levels
of sodium intake as part of an unhealthy diet are
associated with elevated blood pressure, a leading risk
factor for CVD and premature death. The World Health
Organization (WHO) has set a global target of less than
5 grams7 of salt per person in order to improve
population health. However, overconsumption of salt is
prevalent worldwide8 as evidenced by global estimates
placing Thailand at 13.5g/salt per day9.
Between 2010-14, over 70 countries10
reported national
salt reduction mechanisms in a concerted effort to meet
global targets, including Thailand. Thailand’s
multipronged SALTS strategy11,12
is focused on
developing the stakeholder network, mass awareness
campaigns, legislation, technology, and surveillance.
The goal of the strategy is a 30% relative reduction of
population sodium intake by 2025 in accordance with
WHO guidelines.

2
Latest initiatives have included mandatory nutrition
labeling and Guideline Daily Amounts (GDA) on
specific food products13
and the launching of the
Healthier Choice Logo14
– a voluntary approach
encouraging companies to reformulate their food
products. The development of a Thai food database15
comprising of an inclusive list of food products and their
corresponding nutritional value; the technological
development of a salt meter measurement tool16
;
consumer phone scanning applications17
; and the
implementation of Healthy Food Menus18
in food shops
have been new innovations.
The evolution19
of salt reduction developments in
Thailand position the country as a regional leader in
preventing unnecessary lives lost due to CVDs20
. As
Thailand joins other global champions in managing high
salt intake and its deleterious implications, current expert
and stakeholder input can help guide implementation of
the comprehensive national-level Salt and Sodium
Reduction Strategy.
Rationale and Study Aims Thailand continues to develop rigorous research in the
field of salt and sodium reduction to influence policy
formulation. A compilation of recent and ongoing
research can offer those interested in Thailand’s efforts
access to current developments. As the action plan’s
initiatives begin to roll out, expert recommendations are
vital to ensuring the effective operationalization of the
national salt reduction framework. The aim of the study
is to assemble literature on sodium intake and sodium
sources in Thailand, and to identify barriers to
implementation of the SALTS strategy. It seeks to
provide recommendations, particularly with respect to
achieving national and global goals, from the
perspectives of stakeholders.
Methods Data Sources Most information collected was publically available.
National policy documents and surveys were retrieved
from official government websites and WHO.
PowerPoint presentations were obtained from experts.
Research studies were accessed through PubMed. Other
information was accessed through websites of national
stakeholders and internet searches.
Review of Literature Online searches of government, stakeholder, and WHO-
related websites were conducted on salt and sodium
reduction in Thailand. Efforts were followed up with
thorough scanning via PubMed. Search terms included:
sodium, salt, consumption, Thailand, Southeast Asia,
public health, survey, intake, sources. Researches were
chosen based on three criteria: relating to sodium
intake/sources, year, and whether they were previously
included in global reviews of sodium reduction
initiatives in Southeast Asia.
Interviews Semi-structured, in-depth interviews were conducted
during October-November 2017. National stakeholders
and experts were identified by a prominent Thai salt
champion. Requests for interviews were sent via email
and those who responded were interviewed. The
literature review informed open-ended questions on the
following topics: government response, attitudes towards
current sodium reduction legislation, perceived
obstacles, challenges and barriers, perceived strengths,
best practices and ways forward, and ongoing research.
Interviews were conducted in the offices of experts.
Notes were taken in the place of a recording device due
to cultural expectations. Attempts were made to reach
out to a diverse pool of stakeholders and experts in order
to ensure an array of opinions.
Results Literature Review
A. SODIUM INTAKE
A total of 8 studies were identified from 2009-2016 that
measured dietary intake of sodium through urine
analyses21,22,23,25
and dietary recalls9,26,27,29
(Table 1).
Several small scale studies measured sodium intake in
high-risk groups through 24-hour-urine (24hUNa) or 12-
hour overnight measurements. The strongest study21
comprised of 200 24hUNa samples selected from 8
districts in 4 regions of Thailand to assess population
sodium intake. 2 comprehensive studies26,27
utilizing
nationally representative samples were also conducted
(Figure 1).
A review30
of salt intakes in Southeast Asia estimated
sodium intake levels at 4.9g (12.3g) and 3.3g (8.3g) for
younger and older adults in Thailand, respectively. The
study concluded higher than recommended sodium
intakes across all population segments studied based on
research assessed from 1960-2009. The review contained
limited information on Thailand and was used as a
reference point to locate publications to date from 2009
onward to further complement previous efforts of
collection.
I. Based on Urinary Na Measurement
A 2012 study21
assessing the situation of sodium intake
in the Thai population measured 24hUna in a subset of
participants at 128.50 mmol/day (2,955mg) with 87.5%
of participants estimated at over 100 mmol/day

3
(2,300mg). Samples were obtained from a nationally
representative pool of 2,226 Thais aged 15-59 across
Northern, Northeastern, Central, and Southern regions.
Smaller-scale studies estimated sodium excretion among
various Thai participants22,23,25
ranging from 6 – 10g of
salt intake per day, with those at-risk for CVD23
and
hypertensive patients22,25
on the upper limits.
II. Based on Dietary Recalls
Thailand’s 2009 Study of Sodium Chloride (NaCI)
Consumption Among Thai People26
– the largest national
sodium survey thus far31
– indicated that Thais
consumed an average of 10.8 grams of salt (4,320 mg
sodium) per day. At more than double the WHO
recommended level, the main sources of salt derived
from salt added during cooking, packaged food, and
street food. The analysis indicated that salt intake in the
population came directly from condiments (8g), natural
food (2g), and ready to eat meals (0.8g) through the way
of sodium glutamate and sodium chloride32
.
An analysis of sodium chloride content in food
products33
identified the top 5 household condiments as
fish sauce (11.59g), soy sauce (3.15g), salt (3.05g),
shrimp paste (2.9g), and oyster sauce (2.17g) per person
per day. It also categorized instant noodles with
condiments, canned fish, mackerel, steamed chili, and
parsley as the most consumed household foods.
Samples obtained from the 4th National Health
Examination in 201127
measured sodium chloride
consumption in a subset of the Thai population,
reporting slightly lower levels. This difference was
attributed to dissimilar methods and the number of
provinces used to collect data. However, researchers
similarly concluded population intake over suggested
levels. Other studies29
found salt consumption over
5gs/day.
B. FOOD DATABASE
The 2016 Thai Food Composition Tables (FCTs)15
comprised of newly analyzed data with over 1,700 food
items distributed across 16 food categories, each with a
maximum of 27 nutrients including sodium. Published
by Mahidol University’s Institute of Nutrition, the
database is the first English edition of food composition
tables in Thailand. As a tool to determine the potential
contributions of foods to diet, the archive has been
leveraged to engage industry on practical reductions of
certain foods. Instant noodles, fermented fish, seasoned
snacks, fish sauce, soy sauce, and food pastes (chili, fish,
shrimp, curry) are among the frequently consumed foods
with the highest sodium content (Figure 2). Significant
variation in sodium content within the same food
categories were observed – e.g. foods within the Spices,
herbs, condiments, and seasonings category fall within
1,438 – 16,000mg – indicating scope for reductions
(Figures 3, 4).
C. GOVERNMENT RESPONSE: POLICY
INTERVENTIONS
In December 2015, the 8th National Health Assembly
endorsed a resolution entitled "Policy on reduction of
salt and sodium consumption to reduce NCDs”. Seven
recommendations from the assembly specified the main
directions for the current national salt reduction policy
passed the following year. The recommendations
directed the establishment of a national coordinating
mechanism, food standards and regulations, food
labeling, measurement tools, learning packages,
improvement of recipes, and research and development.
Thailand is currently in the final stages of finalizing the
SALTS action plan under the 2016 sodium reduction
policy11
. In response to increasing evidence on sodium
consumption exceeding recommended levels35
and
trends in consumption of frozen and ready-to-eat-
meals36,37
, the policy has set targets to reduce salt
consumption by 30% over the next 8 years in line with
WHO global targets for 2025. A 3% yearly reduction in
urine sample measurements to ensure progress with set
targets will be incorporated within the next Thai
National Health Examination Survey38
.
A national Low-Salt Network38
, established to support
current policy initiatives, has brought together over 40
experts and concerned agencies across government,
academic, and civil society sectors. The stakeholder
group is instrumental for initiating activities around
promotion of policies, public health awareness, and
knowledge creation for the purpose of encouraging
gradual and measurable reductions in packaged and
restaurant/street food.
The 2016 government Notification of Mandatory
Nutrition Labeling and GDA amounts13
– including
sodium content – in snacks, chocolate, bakery products,
semi-processed foods, and chilled/frozen read-to-eat
meals, paved the way for the development of an official
health logo14
for consumers. Since the launch of the
front-of-pack Healthier Choice Logo, new standards are
available for 6 food groups, including instant noodles5,34
and porridge39
– rated among the highest products in salt
content on the market. 51 food companies have joined. A
total of 232 products have been reformulated, including
182 beverages, 8 seasoning sauces, 36 dairy products, 3
instant noodles, and 3 snacks40
. Other plans and
considerations are underway concerning expanded food
labeling relating to nutrient function claims, maximum

4
levels, enforcement of new nutritional labeling
expectations, and official lowering of Thai RDI upper
limits from 2,400mg to 2,000mg41
.
Other food sources, particularly those in institutions and
street food, have remained largely unregulated42
. These
sources contribute significant amounts towards total
energy intake43
. Future initiatives to develop a shop
rating score are included within the strategy. Pilot
projects are also ongoing in environments such as
hospitals that have developed Healthy Menu options18
.
The technology and innovation prong of the strategy
seeks to develop further research in order to support
implementation of programs. Limited number of studies
have been conducted on knowledge, attitudes, and
perspectives of Thais. Of the studies found, behavioral
assessments examined the dietary habits of hypertensive
patients22
and the habits of college students5.
All studies found indicated that Thai adults consumed
over tolerable intake level amounts24,28,50
. Thai children,
apart from consuming foods high in sugar content, also
consumed foods high in sodium28,44
. Thailand aims to cut
national sodium intake by 30% by addressing the main
drivers responsible for high consumption rates in the
population.
I. Ongoing Research Ongoing research studies were also identified. Current
research studies ranged from assessments of sodium
content in 7/11 processed/packaged foods and other
market data, to investigations in usage trends of the
mobile Food Choice phone application, and
developments of potassium chloride based salt
substitutes utilizing umami ingredients. In addition,
recently concluded research pertaining to sodium
reduction through reading labels, sodium screening
devices in food and urine samples, and evaluations of
national trainings on GDA and salt education were also
found38
. Food science research conducted in leading
universities are exploring Thai herbs and spices as
potential salt enhancers, potassium chloride (KCI) salt
substitutes, and the use of umami (savory taste)
ingredients as taste improvers within potassium chloride-
based salt substitutes.
Interview Themes
A. BARRIERS
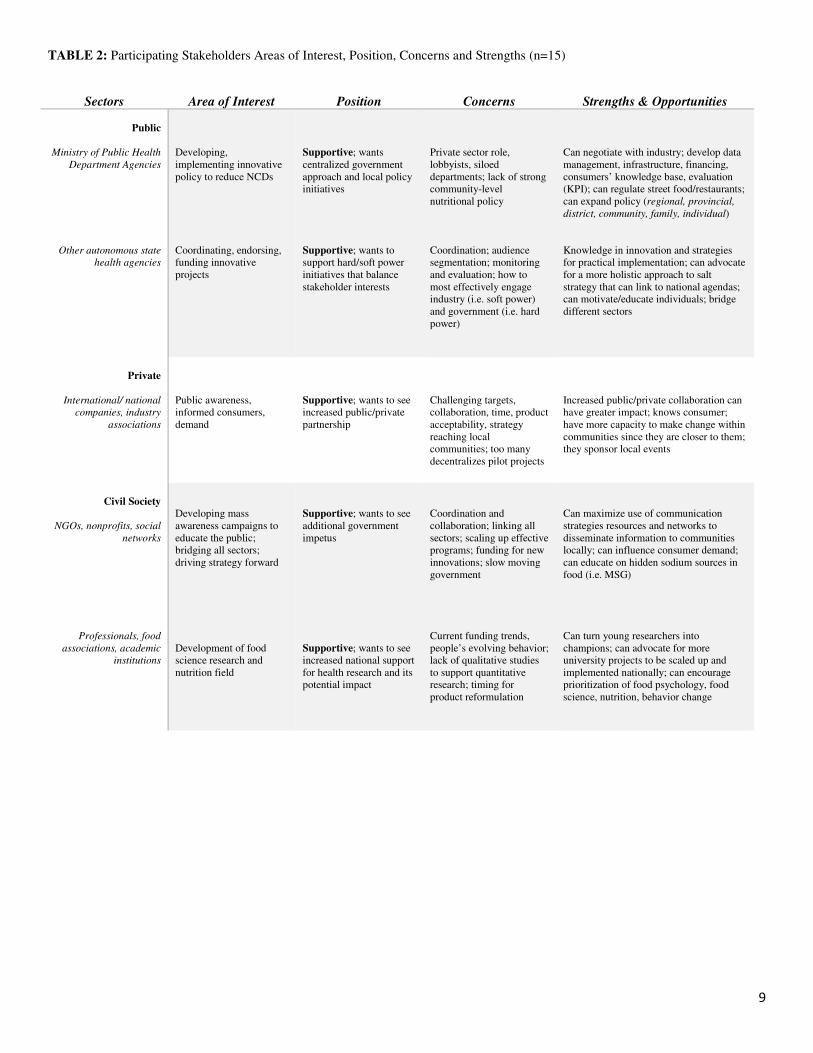
Perceived barriers obtained from participants were
diverse and associated with the sector that the
stakeholder was located within (Table 2). All
stakeholders interviewed were supportive of salt
reduction. Some barriers dominated stakeholder and
expert concerns in 5 main areas (Table 3).
I. Prioritization of Interventions and Leadership Monitoring and evaluation activities, according to
stakeholders and experts, were ambiguous, which
limited the scope of the strategy. It was unclear how the
actionable items under the strategy would be periodically
measured, and how data collection would help inform
future projects to strengthen the strategy. Lack of clarity
in the concrete ways to implement the strategy was a
chief reason why dispersed projects on sodium reduction
were disconnected, according to stakeholders. Pilot
projects across all sectors were perceived to each be
overseen by its own siloed department – a clear
coordinating mechanism linking each project to a central
overseeing agency, absent.
II. Inter and Intra Agency Collaboration
Although the government was acknowledged for
bringing together many key stakeholders involved in the
areas of salt and sodium reduction, it was observed that
stakeholders were disconnected and lacking synergy.
This played a major role as to why some stakeholders
could not clearly observe the national impact of the
strategy.
III. Marketing and Health Promotion Current capability to reach the population through
segmented messaging, especially higher-risk groups, was
identified as ineffective by the majority of stakeholders
and experts. Lack of cohesive community-based sodium
reduction and health promotion interventions were
identified. Conflicting or unclear messaging, particularly
with product labeling, hindered consumer ability to
make informed decisions.
IV. Industry Approach and Timing Stakeholders identified obstacles to developing
innovative strategies that engage industry through soft
power tactics for obtaining a higher degree of buy-in
from companies. In their perspective, legal mechanisms
and enforcement, identified as ‘hard power’ strategies
required complimentary approaches that considered
industry concerns regarding reformulation, technical
assistance, and timing for meeting targets gradually.
Other stakeholders perceived industry innovation and
consumer health as divergent, with a weak link among
the two.
V. Research Priorities
A general lack of research in the dimensions of sodium,
consumer acceptance, cost effectiveness, and long term
health impacts was also identified as a barrier for
evidence based decision making. Other stakeholders
indicated a low level of national support and priority for
projects investigating food behavior, food psychology,
and nutrition.

5
B. RECOMMENDATIONS
Recommendations emerged from discussions on the
ways to address perceived barriers in 4 main areas.
I. Monitoring and evaluation
Monitoring and evaluation, and promotion of a
continuous iterative process that evaluates the
effectiveness of current initiatives, was key for many
stakeholders. Stakeholders and experts conveyed the
importance of ensuring that resources and synergies
were maximized and interventions were well suited for
the population. Developing centralized mechanisms that
monitored progress for the country was suggested.
II. Policy and Strategy
Stakeholders recommended strengthening the
stakeholder network – particularly through public/private
cooperation and long-lasting partnerships with other
ministries – and connecting the strategy to other
initiatives such as the NCD strategy, and tobacco/alcohol
strategies. Many stakeholders recognized the importance
of legal policies and enforcement of mandatory
regulations. As a complement, many advised additional
focus on street food and food that was not yet nationally
regulated. Differing opinions on tax measures, maximum
levels of sodium in products, and other legal measures
for sodium reductions were designated as ongoing topics
in the field.
III. Consumer education and behavior modification
Most national stakeholders and experts highly rated
consumer education and environmental change as most
effective potential drivers for altering consumption
behaviors. They advised additional focus on programmes
and initiatives that targeted households, communities,
children, the open environment, and food shops. The
topic of creating healthier environments with access to
healthier food options across all populations and
geographical regions was a theme that dominated
discussions. Interventions that provided trainings to
provincial health personnel and educational resources for
teachers and children – as techniques to uplift
communities – were also suggested.
IV. Research
Continued research on the diverse facets of food and
nutrition including food psychology, assessments on
future gradual reductions and their impact on technical
requirements from industry, and investigations on
consumers’ taste and acceptance over time were
suggested. Research in tandem with long-term,
continuous mass awareness campaigns were implied.
Most stakeholders and experts agreed that standardized
measurement of current initiatives – in order to gauge
current successes of rolled out efforts – would be useful
knowledge to aid in developments of future innovative
interventions.
Summary and Conclusions This report scans available literature on the topic of salt
reduction in Thailand, assesses the perspectives of
national stakeholders and experts on barriers to salt
reduction policy implementation and provides
recommendations.
The data verify that current levels are around double that
of global recommended levels, and that the major
sources come from condiments used in the household,
packaged foods, and food bought from street vendors.
Perspectives from national stakeholders and experts
highlight a strong collective commitment to supporting
the SALTS strategy and curbing sodium consumption
rates in the Thai population. Stakeholder reports of the
perceived barriers in prioritization of interventions and
leadership, stakeholder collaboration, marketing and
health promotion, industry approach and timing, and
research priorities illustrated strategic areas for policy
improvements. Centralized monitoring and evaluation
efforts, focusing the policy and strategy, strengthening
consumer education and behavior modification
initiatives, and research development are specific
recommendations from national stakeholders that
promote optimal performance and impact of the salt
reduction policy.
Thailand is taking key steps to fulfill its commitment to
reducing sodium intake for improving population health.
This study pointed to institutionalizing sodium
surveillance – for purposes of monitoring and measuring
the national impact of the actionable items under the
strategy – and the role of a collective stakeholder
network in focusing the strategy and promoting gradual
and achievable results toward set targets.
Word Count: 2,820

6
References:
1. Non communicable diseases. (2017). World
Health Organization. Retrieved 11 December
2017, from
http://www.who.int/mediacentre/factsheets/fs35
5/en/
2. Noncommunicable diseases. South-East Asia
Regional Office. Retrieved 11 December 2017,
from
http://www.searo.who.int/entity/noncommunica
ble_diseases/en/
3. Aekplakorn, W. Thai National Health
Examination Survey, NHES V. Presentation.
4. Porapakkham Y, e. (2008). Prevalence,
awareness, treatment and control of
hypertension and diabetes mellitus among the
elderly: the 2004 National Health Examination
Survey III, Thailand. PubMed - NCBI.
Ncbi.nlm.nih.gov. Retrieved 11 December
2017, from
https://www.ncbi.nlm.nih.gov/pubmed/1903755
1
5. Prasutr Thawornchaisit, T. (2013). Health-
Risk Factors and the Prevalence of
Hypertension: Cross-Sectional Findings from a
National Cohort of 87 143 Thai Open
University Students. PubMed Central (PMC).
Retrieved 11 December 2017, from
https://www.ncbi.nlm.nih.gov/pmc/articles/PM
C4776825/
6. New initiative launched to tackle
cardiovascular disease, the world’s number one
killer. (2016). World Health Organization.
Retrieved 11 December 2017, from
http://www.who.int/cardiovascular_diseases/glo
bal-hearts/Global_hearts_initiative/en/
7. Salt reduction. (2016). World Health
Organization. Retrieved 11 December 2017,
from
http://www.who.int/mediacentre/factsheets/fs39
3/en/
8. Kontis, V., Mathers, C., Bonita, R., Stevens,
G., Rehm, J., & Shield, K. et al. (2015).
Regional contributions of six preventable risk
factors to achieving the 25 × 25 non-
communicable disease mortality reduction
target: a modelling study. The Lancet: Global
Health. Retrieved 11 December 2017, from
http://www.thelancet.com/journals/langlo/article
/PIIS2214-109X(15)00179-5/abstract
8. Salt reduction. (2016). World Health
Organization. Retrieved 11 December 2017,
from
http://www.who.int/mediacentre/factsheets/fs39
3/en/
9. Powles, J., Fahimi, S., Micha, R.,
Khatibzadeh, S., Shi, P., Ezzati, M., . . . Sichieri,
Rosely. (2013). Global, regional and national
sodium intakes in 1990 and 2010: A systematic
analysis of 24 h urinary sodium excretion and
dietary surveys worldwide. BMJ Open, 3(12),
BMJ Open, 23 December 2013, Vol.3(12).
10. Trieu, K., Neal, B., Hawkes, C., Dunford,
E., Campbell, N., & Rodriguez-Fernandez, R. et
al. (2015). Salt Reduction Initiatives around the
World – A Systematic Review of Progress
towards the Global Target. Retrieved 11
December 2017, from
https://www.ncbi.nlm.nih.gov/pubmed/2620103
1
11. Policy on reduction of salt and sodium
consumption to reduce NCDs. (2015).
en.nationalhealth.or.th. Retrieved 11 December
2017, from https://en.nationalhealth.or.th/wp-
content/uploads/2017/09/4_1salt-sodium-
main.pdf
12. ยทุธศาสตร์ลดการบริโภคเกลือและโซเดียมในประเทศไทย พ.ศ.
2559-2568. (2016). Thaincd.com. Retrieved 11
December 2017, from
http://www.thaincd.com/2016/media.php?tid=&
gid=1-015-005&searchText=&pn=2
13. The Notification of the Ministry of Public
Health (No.373) B.E. 2559 (2016): Display of
Nutrition Symbol on Food Label. (2017).
Retrieved from
http://food.fda.moph.go.th/law/data/announ_mo
ph/V.English/No.373_Notification_Nutrition_S
ymbol.pdf
14. ทางเลือกสุขภาพ | โครงการพฒันาและส่งเสริมการใชส้ญัลกัษณ์
โภชนาการ. Healthierlogo.com. Retrieved 11
December 2017, from http://healthierlogo.com/
15. Online Thai food composition Database
(THAI FCD). (2016). Inmu.mahidol.ac.th.
Retrieved 11 December 2017, from
http://www.inmu.mahidol.ac.th/thaifcd/home.ph
p
16. Wongsawat, Y. (2016). Development of Salt
Meter in Food and Urine for Thai Health
Promotion 2. Lowsaltthai.com. Retrieved 11
December 2017, from
https://www.lowsaltthai.com/download-งานวจิยั-
52587.page
17. "FoodChoice" บน App Store. (2015). iTunes
App Store. Retrieved 11 December 2017, from
https://itunes.apple.com/th/app/foodchoice/id11
18271150?l=th&mt=8
18. Kantachuvesiri, S. (2017). National strategy
to reduce salt and sodium intake in Thailand.
Presentation.
19. Supornsilaphachaii, C. (2013). Evolution of
salt reduction initiatives in Thailand: lessons for
other countries in the South-East Asia Region.
Pdfs.semanticscholar.org. Retrieved 11
December 2017, from
https://pdfs.semanticscholar.org/11a3/ce4d507ff
801b2029f3aa6280f865234a411.pdf
20. NOURISHING Framework. (2017).
Wcrf.org. Retrieved 11 December 2017, from
http://www.wcrf.org/sites/default/files/8_Inform
%20People_Feb%202017%20v2.pdf
21. ศรีเงินยวง, ล., วงษจิ์นดา, ธ., & อภิชนะกุลชยั, ฐ. (2012).
สถานการณการบริโภคเกลือโซเดียมในประชากรไทย : การศึกษาเชิงปริ
มาณ. Thaincd.com. Retrieved 12 December 2017,
from
http://thaincd.com/document/file/download/pap
er-manual/download1no167.pdf
22. Buranakitjaroen, P., &
Phoojaroenchanachai, M. (2013). The
prevalence of high sodium intake among
hypertensive patients at hypertension clinic,
Siriraj Hospital. Journal of the Medical
Association of Thailand = Chotmaihet
Thangphaet, 96 Suppl 2, S1-8.
23. Yokokawa, H., Yuasa, M., Nedsuwan, S.,
Moolphate, S., Fukuda, H., Kitajima, T., . . .
Marui, E. (2016). Daily salt intake estimated by
overnight urine collections indicates a high
cardiovascular disease risk in Thailand. Asia
Pacific Journal of Clinical Nutrition, 25(1), 39-
45.
24. Sornhiran, S., Ingsathit, A., &
Kantachuvesiri, S. (2016). Effect of intensive
education plus immediate feedback on sodium
intake in CKD patients at Bhumibol Adulyadej
hospital: A Randomized Controlled Trial.
Lowsaltthai.com. Retrieved 12 December 2017,
from http://Lowsaltthai.com
25. Kantachuvesiri, S. (2017). National strategy
to reduce salt and sodium intake in Thailand.
Presentation.
26. Maliwong, K., Saiwong, N., & Sannawat, S.
(2009). การสาํรวจการบริโภคโซเดียมคลอไรดข์องประชากรไทย.
Nutrition.anamai.moph.go.th. Retrieved 11
December 2017, from
http://nutrition.anamai.moph.go.th/download/art
icle/article_20160323133823.pdf
27. Satheannoppakao, W., Kasemsup, R.,
Inthawong, R., Chariyalertsak, S., Sangthong,
R., Taneepanichskul, S., . . . Aekplakorn, W.
(2013). Sodium intake and socio-demographic
determinants of the non-compliance with daily
sodium intake recommendations: Thai NHES
IV. Journal of the Medical Association of
Thailand, 96, S161-170.
28. Executive Summary: The 2013 Survey on
Food Consumption Behavior. (2013).
http://web.nso.go.th/. Retrieved 12 December
2017, from
http://web.nso.go.th/en/survey/data_survey/570
718_The%202013%20Survey%20on%20Food
%20Consumption%20Behavior.pdf
29. Ivanovitch, K., Klaewkla, J., Chongsuwat,
R., Viwatwongkasem, C., & Kitvorapat, W.
(2014). The Intake of Energy and Selected
Nutrients by Thai Urban Sedentary Workers: An
Evaluation of Adherence to Dietary
Recommendations. Journal of Nutrition and
Metabolism, 2014(2014), 17.
30. Batcagan-Abueg, A., Lee, J., Chan, P.,
Rebello, S., & Amarra, M. (2013). Salt intakes
and salt reduction initiatives in Southeast Asia:
a review. Asia Pac J Clin Nutr 2013, 22(4), 683-
697.
http://apjcn.nhri.org.tw/server/APJCN/22/4/490.
31. Expert Meeting on Population Sodium
Reduction Strategies for Prevention and Control
of Noncommunicable Diseases in the South-
East Asia Region. (2012).
http://www.searo.who.int/. Retrieved 11
December 2017, from
http://www.searo.who.int/entity/noncommunica
ble_diseases/documents/salt_meeting_report201
2.pdf?ua=1

7
32. Saiwongse, N. (2010). Thailand Salt
Reduction Policy. Presentation.
33. ป้องกนัการเกิดโรคไม่ติดต่อในวิถีชีวิตดว้ยการลดการบริโภคเกลือ.
(2013). E-lib.ddc.moph.go.th. Retrieved 20
December 2017, from http://e-
lib.ddc.moph.go.th/pdf/eb237/eb237.pdf
34. Chavasit, V. (2015). Labeling and Nutrition
Research in ASEAN and Research in Food
Products including Instant Noodles.
Presentation.
35. Thiamwong, L., & Suwanno, J. (2017). The
Process of Reducing Sodium Intake among
Older Adults: A Participatory Action Research
Study. Juniperpublishers.com. Retrieved 12
December 2017, from
https://juniperpublishers.com/oajggm/pdf/OAJG
GM.MS.ID.555556.pdf
36. Pavadhgul P, Sunthonwaraluk S,
Srisorachatr S, Temcharoen P. Dietary sodium
intake by semi-quantitative food frequency
questionnaire among undergraduate students of
Mahidol University. J Med Assoc Thai.
2009;92(Suppl 7):S75-82.
http://www2.ph.mahidol.ac.th/research/thai/jme
dassocthai/Vol92_Suppl7/S75-
82_mahidol%2025.pdf
37. วนัทนีย ์เกรียงสินยศ (2015). ลดโซเดียม ยดืชีวิต. Ministry
of Public Health. Retrieved from
http://tnfc.fda.moph.go.th/file/fileDoc/2015-04-
29_6645.pdf
38. ความเป็นมา. Lowsaltthai.com. Retrieved 20
December 2017, from http://Lowsaltthai.com
39. Sriwattana, S., Pongsirikul, I., Siriwoharn,
T., & Chokumnoyporn, N. (2016). Strategies for
Reducing Sodium in Instant Rice Porridge and
its Influence on Sensory Acceptability. Chiang
Mai University Journal of Natural Sciences,
5(3), 203-502.
40. Kriengsinyos, W., Chavasit, V.,
Mukdasakunphiban, B., Maksongrite, C.,
Termpornlert, N., & Parinyasiri, T. et al. (2017).
40th Anniversary of Institute of Nutrition,
Mahidol University (p. 57). Institute of
Nutrition, Mahidol University, Food and Drug
Administration; Ministry of Public Health.
Retrieved from
http://www.inmu.mahidol.ac.th/4decades_INM
U/pdf/Full_pdf%204decades.pdf
41. Rimpeekool, W., Seubsman, S., Banwell, C.,
Kirk, M., Yiengprugsawan, V., & Sleigh, A.
(2015). Food and nutrition labelling in Thailand:
A long march from subsistence producers to
international traders. Food Policy, 56, 59.
42. Draper, Alizon. (2017). STREET FOODS
IN DEVELOPING COUNTRIES: THE
POTENTIAL FOR MICRONUTRIENT
FORTIFICATION.
43. Wanjek, C. (2005). Food at work:
Workplace solutions for malnutrition, obesity
and chronic diseases. Geneva: ILO.
44. Klunklin S, Channoonmuang K. Snack
consumption in normal and undernourished
preschool children in Northeastern Thailand. J
Med Assoc Thai. 2006;89:706-13.

8
TABLE 1: Recent research studies that measure sodium intake and/or dietary sources of sodium in Thailand (n=8)
*Research not yet published.
Study Name Author(s) Date Group/Age Sampling Measurement Results URINARY SODIUM
EXCRETION METHOD
Situation of Sodium/salt Intake
in Thai Population21
Dr. Luechai S.; Maj.
Thanita W.; Thanida A.;
….
2012
2,226
aged 15-59
200 subsample
National;
Convenience; Cross-sectional
24hUNa; 24-hour-
dietary-recall;
response rate: 67.8%
Median 2,955.5 mg/day ; 87.5% level of >
2,300 mg/ day; 4 persons have level exceeding 4,600 mg/day; 22.6% ate instant noodles >
3x/week
Prevalence of High Sodium
Intake among Hypertensive
Patients at Hypertension
Clinic, Siriraj Hospital22
P, Buranakitjaroen;
M.Phoojaroenchanachai
2013
320
hypertensive
patients
Cross-sectional
24hUNa
Mean total daily Na intake 3,404 mg/day i.e.
3.4 g of Na/day; prevalence of high salt intake
at 73.4%; 76.3% patients who knew effects of
salt on BP consumed high salt diet
Daily salt intake estimated by
overnight urine collections
indicates a high cardiovascular
disease risk in Thailand23
Hirohide Yokokawa,
Motoyuki Yuasa,
Supalert Nedsuwan
2016
793
participants at
high risk of
CVD
Cross-sectional;
cluster
randomized
trial
24-hour salt intake
estimated from 3 days
overnight UNa
Mean salt intake 3,960 mg/day; higher salt
group patients with family history of HTN,
antihypertensive drug use, less ideal BMI,
higher exercise frequency, lower intake
awareness
Study on the effect of low
sodium condiments on blood
pressure and sodium intake in
hypertensive patients in the
community*25
Dr. Surasak
Kantachuvetsiri
....
2016
100
hypertensive
patients
Community-based
participatory
research; cross
over RCT
12h overnight UNa;
Blood pressure (BP)
Mean 4,000mg/day; use of low sodium condiment in household cannot reduce daily
BP/sodium intake per day; intensive education
can reduce salt intake/BP
DIET RECALL MEHOD
Study of Sodium Chloride
(NaCI) Consumption Among
Thai People26
Ministry of Public
Health, Bureau of
Nutrition
2009
2,733
households
National ;
Multistage
random
7-day -dietary-recall
Mean 4,320 mg/day (10.8g/salt/day)
Sodium Intake and Socio-
Demographic Determinants of
the Non-Compliance with
Daily Sodium Intake
Recommendations: Thai
NHES IV27
Warapone S. Rachada
K.; Surasak T.
2011
8,462 (aged 2-
14); 20,470
(aged 15+)
2,969 subgroup
Data sampled
from National
Health Exam
Survey
(NHES IV)
Food frequency
questionnaire;
24-hour-dietary-recall
Daily consumption of snack foods increased to
42.9%; 10% eat instant noodles daily
2,472.7 mg/day for those 1-15 years; 3,264.5
mg/day for those 16 years and older
Global, regional and national
sodium intakes in 1990 and
2010 …9
John Powles, Saman
Fahimi, Renata Micha,
Shahab Khatibzadeh …
2013
-
-
Age-standardized
estimated sodium
intakes
Average sodium 5,400 mg/day (13.5g/salt)
The Intake of Energy and
Selected Nutrients by Thai
Urban Sedentary Workers:
Evaluation of Adherence to
Dietary Recommendations29
Katiya I, Jeeranun K.,
Rewadee C., Chukiat V., Wanicha K.
2014
215 adults 20–
50 years in sedentary
occupations
Convenience
24-hour dietary recall;
2-day food record;
response rate: 78%
male; 73% female
Male median intake 1,967 mg/day; female
intake 2,021 mg/day
9
TABLE 2: Participating Stakeholders Areas of Interest, Position, Concerns and Strengths (n=15)
Sectors Area of Interest Position Concerns Strengths & Opportunities
Public
Ministry of Public Health
Department Agencies
Other autonomous state
health agencies
Developing,
implementing innovative
policy to reduce NCDs
Coordinating, endorsing,
funding innovative
projects
Supportive; wants
centralized government
approach and local policy
initiatives
Supportive; wants to
support hard/soft power
initiatives that balance
stakeholder interests
Private sector role,
lobbyists, siloed
departments; lack of strong
community-level
nutritional policy
Coordination; audience
segmentation; monitoring
and evaluation; how to
most effectively engage
industry (i.e. soft power)
and government (i.e. hard
power)
Can negotiate with industry; develop data
management, infrastructure, financing,
consumers’ knowledge base, evaluation
(KPI); can regulate street food/restaurants;
can expand policy (regional, provincial,
district, community, family, individual)
Knowledge in innovation and strategies
for practical implementation; can advocate
for a more holistic approach to salt
strategy that can link to national agendas;
can motivate/educate individuals; bridge
different sectors
Private
International/ national
companies, industry
associations
Public awareness,
informed consumers,
demand
Supportive; wants to see
increased public/private
partnership
Challenging targets,
collaboration, time, product
acceptability, strategy
reaching local
communities; too many
decentralizes pilot projects
Increased public/private collaboration can
have greater impact; knows consumer;
have more capacity to make change within
communities since they are closer to them;
they sponsor local events
Civil Society
NGOs, nonprofits, social
networks
Professionals, food
associations, academic
institutions
Developing mass
awareness campaigns to
educate the public;
bridging all sectors;
driving strategy forward
Development of food
science research and
nutrition field
Supportive; wants to see
additional government
impetus
Supportive; wants to see
increased national support
for health research and its
potential impact
Coordination and
collaboration; linking all
sectors; scaling up effective
programs; funding for new
innovations; slow moving
government
Current funding trends,
people’s evolving behavior;
lack of qualitative studies
to support quantitative
research; timing for
product reformulation
Can maximize use of communication
strategies resources and networks to
disseminate information to communities
locally; can influence consumer demand;
can educate on hidden sodium sources in
food (i.e. MSG)
Can turn young researchers into
champions; can advocate for more
university projects to be scaled up and
implemented nationally; can encourage
prioritization of food psychology, food
science, nutrition, behavior change

10
TABLE 3: Barriers to and Recommendations for Successful Implementation of the SALTS Strategy Thailand, 2017
Themes Identified
Barriers
Prioritization of Interventions and Leadership � Not enough emphasis on consumer education and behavior change
� The action plan is relatively new– though roles are defined, it is not unclear who will lead & coordinate implementation
� Ambiguity with the M&E Framework; population surveillance inconsistent and no follow up NaCl survey since 2009
� Fragmentation of actions and pilot projects divided among different sectors; lack of overseeing body
� Too much emphasis on reformulation and regulatory mechanisms despite 80% of food consumed at home/street/market
� Rigidity of government which usually depends on internal leader within govt. sector to champion a project
� Weaknesses in labeling and marketing: Healthier Choice Logo, monochrome labeling
� Difficulty of WHO sodium consumption guidelines to be practically implemented despite political will
� Lack of low-salt products available broadly
� Top-down approach is not effective especially for poorer, rural communities
Inter and Intra Agency Collaboration
� Perceived disconnect among the stakeholder network – disparate and lack of synergy – cannot clearly see impact on national level
� MoPH departments are understaffed and underfunded, and at times working in isolation without clear connecting mechanism with
other stakeholders and ministries, especially those relating to the food chain
� Weak integration of salt policy within larger systems (NCD, veggie, fruit consumption, tobacco)
� Lack of effective inter-ministerial partnerships
� Lack of government leadership willing to implement proven interventions and/or scale up pilot programs
Marketing and Health Promotion
� Ineffective at reaching target segment populations (children, elderly, NCD patients, adolescents)
� Unclear and confusing for the consumer
� Not strong enough to work against misinformed social media information and/or industry
Industry Approach and Timing
� There is a weak link between Industry innovation/technology and consumer health
� Lack of inventive strategies for obtaining higher degree of industry buy-in through soft power methods
� Industry cannot adapt to 30% reduction immediately and requires time for gradual adjustment
Research Priorities
� Lack of research on salt, sodium, reformulation, and food science for informing policy and interventions
� Insufficient research on consumer acceptance, value, cost effectiveness, and long term health impacts
Recommendations
Monitoring and Evaluation
� More investment in M&E related to evaluating current interventions & integration with other NCD risk factors and data systems
� Establishment of a consumer database to measure consumption behavior trends of products with healthier choice logo
Policy and Strategy
� Strengthen stakeholder network; additional assistance to meet targets set out by MoPH/FDA
� Expand strategy to link with national agenda beyond MoPH
� Clear designation of a centralized implementation body and systematic evaluation framework
� More rigorous and consistent population surveillance
� More emphasis on other initiatives: tax (similar to sugar tax), warning labels (similar to tobacco), upper limits of sodium in food,
traffic light approach (in order to expand number of products), a more practical approach that accommodates sodium reduction levels
with the product type/category; expansion of labeling to all packaged foods; additional focus on national street food initiatives
� Harmonization of national guidelines and data collection methods/management
� Ongoing/continuing collaboration with industry and private sector, public/private partnerships
� Development of long-term, sustainable approach for collaborating with other ministries/extending beyond health-related agencies
Consumer Education and Behavior Modification
� Prioritization of consumer education across all population segments especially children, elderly and other high risk groups
� Prioritization on educating street vendors
� Utilize nutritional teachers and/or train teachers in nutritional education
� Develop creative, culturally relevant inexpensive tactics that focus on behavior modification
� Emphasis on educating consumer on using informed choice (GDA) as a tool rather than providing consumer with an interpretive
symbol (Healthy Choice logo)
Research
� More investment in food science research, nutrition, behavior modification, food psychology, consumer behavior
� More investment in sodium molecular research, monosodium glutamine, sodium chloride

11
FIGURE 1:
FIGURE 2:

12
FIGURE 3:
FIGURE 4:
Top Related