- 1.Sleep Disordered Breathing
2. Objectives
- Understand CO2, O2 relationships in the lungs
- Describe types of Sleep Disordered Breathing
- Treatment options for OSA
3. Spontaneous Breathing
- Thoracic cage increases in volume, intrathoracic pressure
decreases
- Negative pressure causes intake of air
4. Lung Unit
- Alveoli and blood capillaries intertwine
5. Gas Exchange
- Occurs at at alveolar-capillary membrane
6. O2 TransportCO2 Transport
7. Diffusion affected by:
8. V/Q ratio relationship between blood flow to an individual
alveoli and airflow to that alveoli
-
- Perfusion with no ventilation
-
- Alveoli receives blood supply, airflow blocked by mucous no gas
exchange
-
- Ventilation with lack of perfusion
-
- Blockage in bloodflow, wasted ventilation no gas exchange
occurs
9. Dissociation Curve
- The curve represents the relationship between oxygen and Hb,
and the factors that affect the uptake and release of oxygen and
the degree of saturation.
10. Dissociation curve 11.
- Basic Principles of the Curve:
-
- Increasing O2 tensions result inSat%
-
- Flat portion of the curve (60 mmHg - 100 mmHg), large changes
in PO2 result in very small changes in Sat%.
-
- Steep portion of the curve (10 mmHg - 60 mmHg), small changes
in PO2 result in large drops in O2 Sat%.
12.
- Factors Altering HB Affinity for O2:
13.
- Shifts of the Curve to the Right:
-
- Results in a decreased affinity
-
- Results in a decreased O2 transport capability (O2
content)
-
- Aids in unloading of oxygen to the tissues
-
- Extreme shifts are a disadvantage, because O2 content is so
depleted the tissue oxygenation is severely impaired
14.
- Shifts of the Curve to the Left:
-
- Results in a increased affinity
-
- Results in a increased O2 transport capability (O2
content)
-
- Hinders unloading of oxygen to the tissues.
15. Capnography
- The measurement and graphical display of the concentration of
carbon dioxide in waveform format
16. EtCO2
- Refers to the measurment of carbon dioxide concentration at the
end of expiration
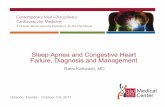
17. ETCO2 Assessment
- CO2 measurement with each breath
A-B:A near zero baselineExhalation of CO2-free gas contained in
dead space. B-C:Rapid, sharp riseExhalation of mixed dead space and
alveolar gas. C-D:Alveolar plateauExhalation of mostly alveolar
gas. D:End-tidal value Peak CO2 concentrationnormally at the end of
exhalation. D-E:Rapid, sharp downstrokeInhalation 18. Wave form
allows us to assess
- proper functioning of a mechanical ventilator or anesthesia
delivery system
19. EtCO2 waveform
- Earliest Detection of Hypoventilation and Apnea
- Shows cessation of breathing before pulse oximetry would alert
medical staff to a problem
- Helpful if the patient is on supplemental oxygen
20. Why are dissociation curve and EtCO2 important?
- Windows to ventilation and perfusion
21. Abnormal capnograms
- Sudden loss of EtCO2 to zero or near zero Possible causes:
Airway disconnection Dislodged ET tube/esophageal intubation
Totally obstructed/kinked ET tube Complete ventilator
malfunction
22. Abnormal capnograms
- SustainedlowEtCO2 with good alveolar plateau
- Possible causes: Hyperventilation Hypothermia Sedation,
anesthesia Dead space ventilation
23. Abnormal Capnography
- ElevatedEtCO2 with good alveolar plateau
- Possible causes:Hypoventilation Respiratory-depressant drugs
Hyperthermia, pain, shivering
24. ABG Values 28 88 50 60 7.38 COPD 22-26 94-99 35-45 80-100
7.40 Normal HCO3 SaO2 PCO2 PO2 pH 25.
- Cyanosis (bluish coloring) occurs with a PaO2 reduction of 5 gm
%
26. Hypoventilation
27. Hyperventilation
28. Hypoxic Drive
- Normal drive- CO2 build up
29. Characteristics of Respiratory Events Not required Usually
mild cyclic desats Crescendo-Decrescendo pattern Waz-wane May last
15-30 min or more Cheyne-Stoles Respiration Mandatory Not required
Slight increase, may crescendo to end of event Slight decrease from
baseline Respiratory Event Related Arousal Not required 4% required
Yes 30% from baseline 10-120 sec, Longer hypo-ventilation Hypopnea
Not required Common; not mandatory NO Absent Minimum 10 sec Central
Apnea Not required Not required Yes Absent Minimum 10 sec
Obstructive Apnea Arousal Desaturation Effort Airflow Duration 30.
Treatment of OSA
31. Goals of Treatment
- Eliminate associated arousals
32. Goals cont
- Eliminate associated desaturations
- Increase Sleep Efficiency
33. Titration Techniques
- Increase 1-2 cm increments
- Record each pressure for a minimum of 15 minutes
- Record REM sleep while in supine position
34. BiPAP
- Varying pressures; insp 4 cm > expiration
-
- Optimal CPAP pressure > 15
-
- Optimal CPAP pressure is associated with the occurrence of
central apneas
35. Lung Volumes 36.
- The use of CPAP / BiPAP increases FRC which in turn improves
oxygenation
37. Surgical Options
- Uvulopalatopharyngoplasty (UPPP)
- Laser assisted uvulopalatopharyngoplasty (LAUP)
- Maxillomandibular advancement
38. More surgical options
- Approximately 50% effective
39. Oral Appliances
- Mandibular repostitioners
40. 41. 42.
- Treatment of patients with:
43. Identified Risks
- Intraoral gingival, palatal, or dental soreness
- Obstruction of oral breathing
- Loosening or flaring of lower anterior teeth
44. Oral appliances, contraindications
- Severe respiratory disorders
- Loose teeth or advanced periodontal disease