







Languages
Pages
Legal

Single Tooth Incisionless-Sutureless SurgeryTEETH IN A DAY™
(Continued on Page 2)
Glenn J. Wolfinger,DMD, FACP
Thomas J. Balshi,DDS, FACP
www.teeth-usa.com.
Introduction
Immediate loading of titanium implantsintended to become osseointegrated haspeaked the interest of many clinicians andresearchers. The evolution from thetraditional 2-stage protocol, originallydeveloped by Per Ingvar Brånemark, hasprovided exceptionally excellent resultsover the past two decades.
However, patients’ desires and needshave also traditionally encouragedclinicians and researchers alike to findnew solutions. Thus, acceleration of thetreatment process has occurred as a resultof perspective scientific studies. Muchof the immediate loading researchperformed over the past nine years hasfocused on extensive partial and full archrestorations. Researchers havedemonstrated the efficacy of immediateloading using the TEETH IN A DAY™protocol in the fully edentulous maxillaand fully edentulous mandible as well aspartially edentulous conditions. Theresults of these studies clearly indicatethat immediate loading under specificprotocols can work successfully.
There is a distinct difference betweenimmediate loading of multiple implants
and that of a single tooth. Whenfunctional loads are applied to a rigidlysplinted multiple implant system, themajority, if not all the implants, absorbthe load distribution in that system.However, any loading forces applied toa single tooth implant restoration areapplied to the one implant. For thisreason many clinicians believe that theinitial restoration placed on the implantshould be constructed in a manner thateliminates direct occlusal loading. Afterthe implant has osseointegrated, the finalprosthesis can be put into normalfunction. This is the procedure employedfor the following patient.
Patient Treatment ReviewThe patient is a very lovely, energetic,athletic and highly motivated 26-year-oldyoung woman who suffered a traumatic
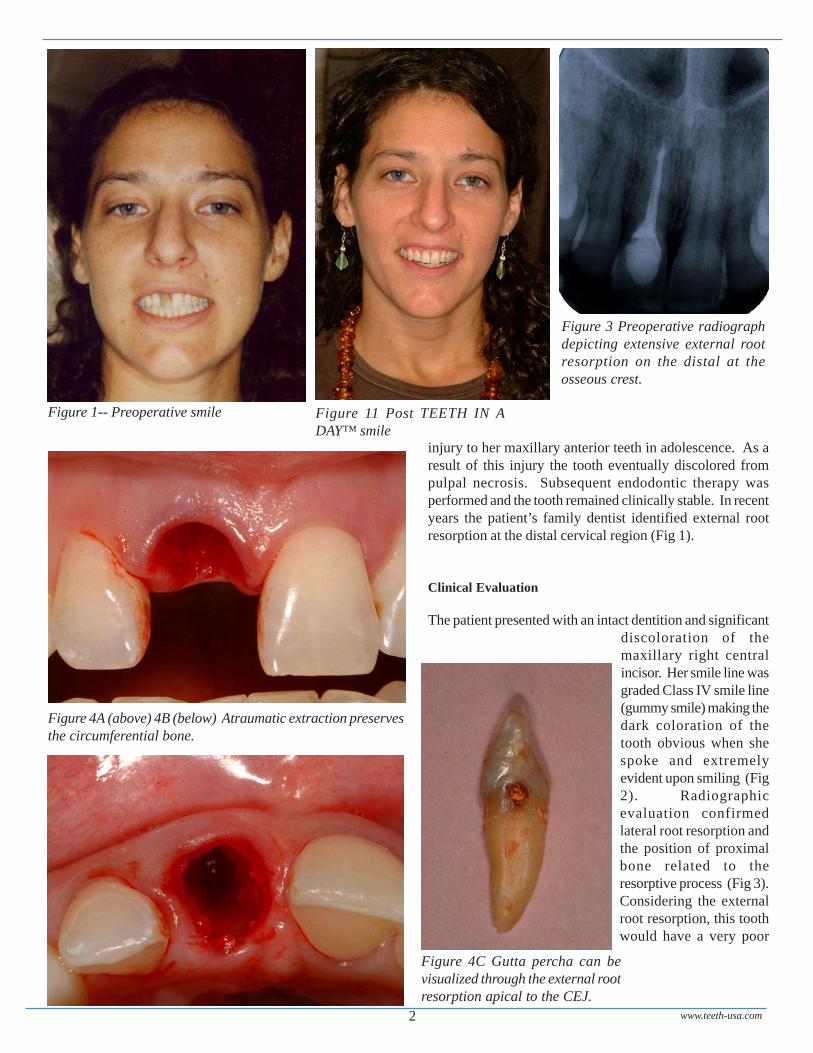
Figure 2 -- Class IV smile line reveals the traumaticallydiscolored right central incisor.
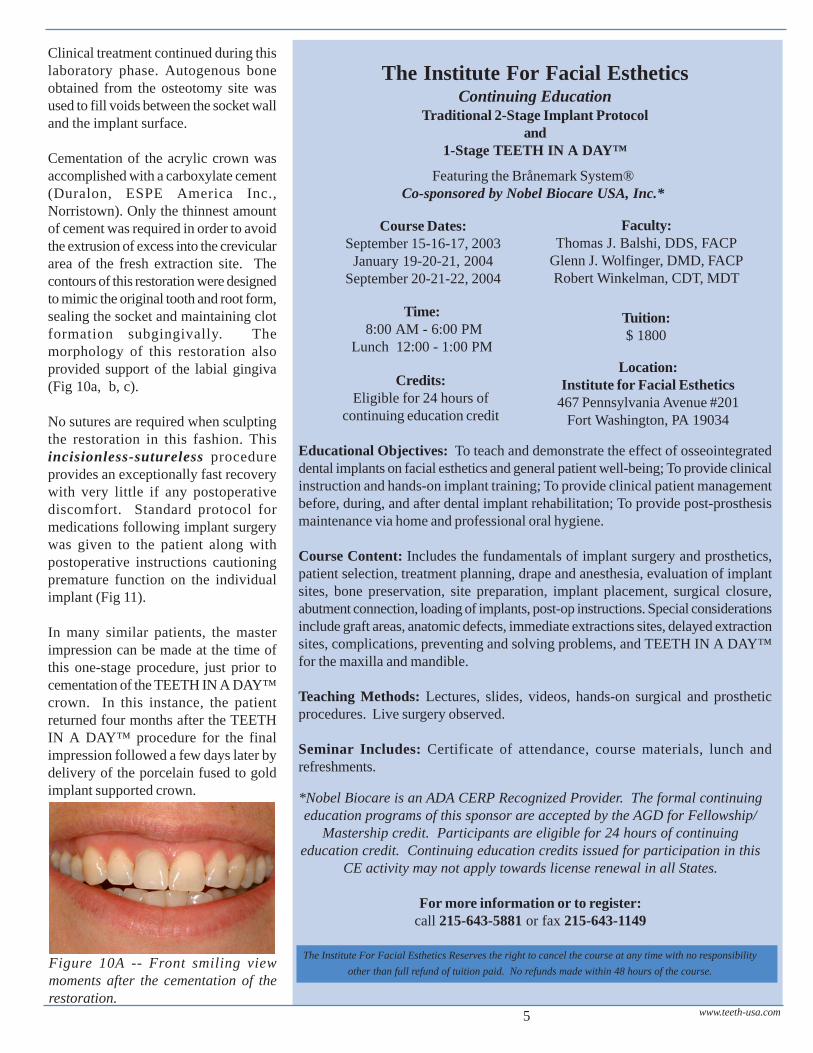
Figure 10A -- Front smiling view moments after the cementationof the restoration.
injury to her maxillary anterior teeth in adolescence. As aresult of this injury the tooth eventually discolored frompulpal necrosis. Subsequent endodontic therapy wasperformed and the tooth remained clinically stable. In recentyears the patient’s family dentist identified external rootresorption at the distal cervical region (Fig 1).
Clinical Evaluation
The patient presented with an intact dentition and significantdiscoloration of themaxillary right centralincisor. Her smile line wasgraded Class IV smile line(gummy smile) making thedark coloration of thetooth obvious when shespoke and extremelyevident upon smiling (Fig2). Radiographicevaluation confirmedlateral root resorption andthe position of proximalbone related to theresorptive process (Fig 3).Considering the externalroot resorption, this toothwould have a very poor
Figure 3 Preoperative radiographdepicting extensive external rootresorption on the distal at theosseous crest.
Figure 1-- Preoperative smile Figure 11 Post TEETH IN ADAY™ smile
Figure 4A (above) 4B (below) Atraumatic extraction preservesthe circumferential bone.
Figure 4C Gutta percha can bevisualized through the external rootresorption apical to the CEJ.
www.teeth-usa.com2
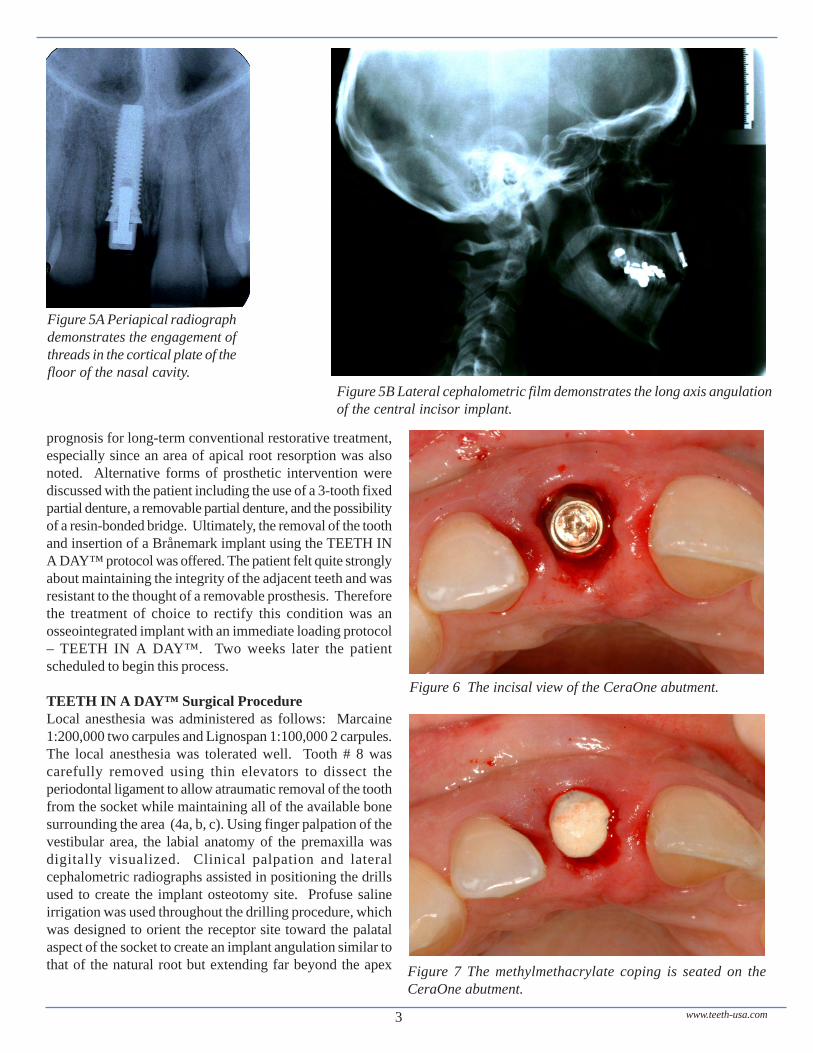
Figure 5A Periapical radiographdemonstrates the engagement ofthreads in the cortical plate of thefloor of the nasal cavity.
Figure 5B Lateral cephalometric film demonstrates the long axis angulationof the central incisor implant.
prognosis for long-term conventional restorative treatment,especially since an area of apical root resorption was alsonoted. Alternative forms of prosthetic intervention werediscussed with the patient including the use of a 3-tooth fixedpartial denture, a removable partial denture, and the possibilityof a resin-bonded bridge. Ultimately, the removal of the toothand insertion of a Brånemark implant using the TEETH INA DAY™ protocol was offered. The patient felt quite stronglyabout maintaining the integrity of the adjacent teeth and wasresistant to the thought of a removable prosthesis. Thereforethe treatment of choice to rectify this condition was anosseointegrated implant with an immediate loading protocol– TEETH IN A DAY™. Two weeks later the patientscheduled to begin this process.
TEETH IN A DAY™ Surgical ProcedureLocal anesthesia was administered as follows: Marcaine1:200,000 two carpules and Lignospan 1:100,000 2 carpules.The local anesthesia was tolerated well. Tooth # 8 wascarefully removed using thin elevators to dissect theperiodontal ligament to allow atraumatic removal of the toothfrom the socket while maintaining all of the available bonesurrounding the area (4a, b, c). Using finger palpation of thevestibular area, the labial anatomy of the premaxilla wasdigitally visualized. Clinical palpation and lateralcephalometric radiographs assisted in positioning the drillsused to create the implant osteotomy site. Profuse salineirrigation was used throughout the drilling procedure, whichwas designed to orient the receptor site toward the palatalaspect of the socket to create an implant angulation similar tothat of the natural root but extending far beyond the apex
Figure 6 The incisal view of the CeraOne abutment.
Figure 7 The methylmethacrylate coping is seated on theCeraOne abutment.
www.teeth-usa.com3
into the pre-maxillary basal bone (Fig 5a, b).
Following preparation of the socket, a 15 X 4 mm TiUniteMK4 Brånemark implant was placed with the shoulder ofthe implant 4 mm below the crest of the gingiva on the labial
aspect. A bone guide was installed and the accompanyingtrephine used to remove peripheral bone from the proximalsurfaces of the socket. Then a 1 mm CeraOne abutment wasinstalled (Fig 6). The gold fastening screw was tightened withan electronic torque driver to 32 Ncm of torque force.
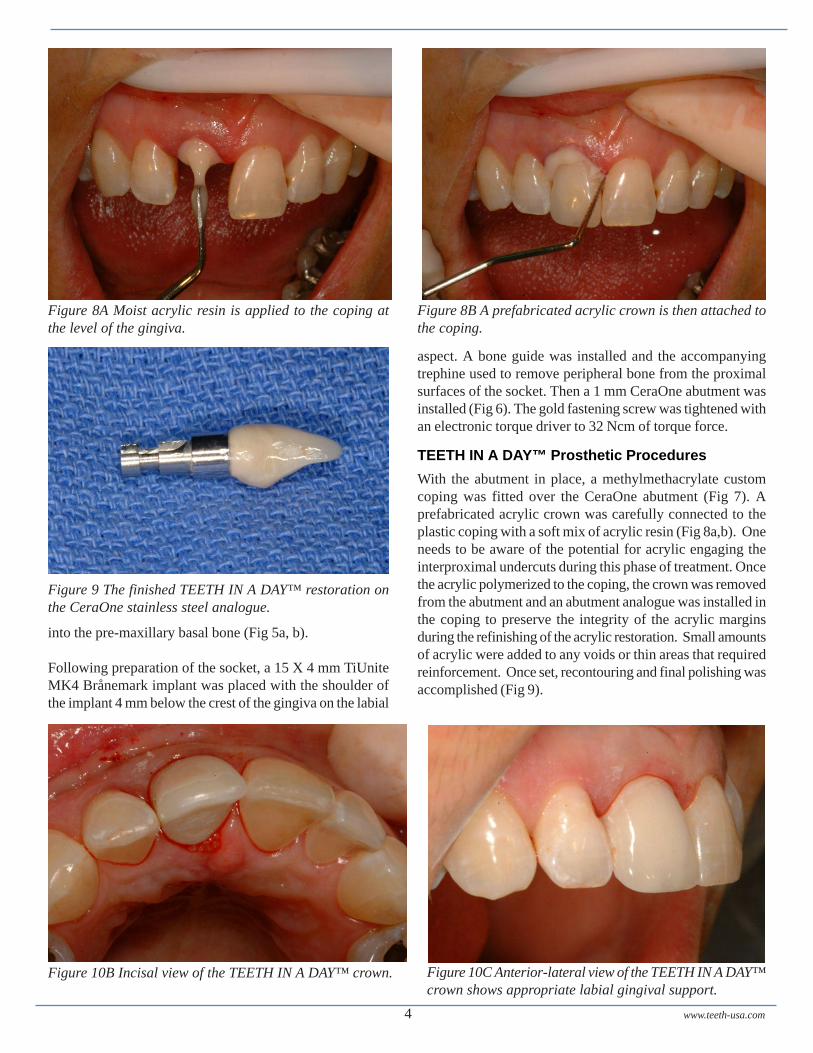
TEETH IN A DAY™ Prosthetic ProceduresWith the abutment in place, a methylmethacrylate customcoping was fitted over the CeraOne abutment (Fig 7). Aprefabricated acrylic crown was carefully connected to theplastic coping with a soft mix of acrylic resin (Fig 8a,b). Oneneeds to be aware of the potential for acrylic engaging theinterproximal undercuts during this phase of treatment. Oncethe acrylic polymerized to the coping, the crown was removedfrom the abutment and an abutment analogue was installed inthe coping to preserve the integrity of the acrylic marginsduring the refinishing of the acrylic restoration. Small amountsof acrylic were added to any voids or thin areas that requiredreinforcement. Once set, recontouring and final polishing wasaccomplished (Fig 9).
Figure 8A Moist acrylic resin is applied to the coping atthe level of the gingiva.
Figure 8B A prefabricated acrylic crown is then attached tothe coping.
Figure 10B Incisal view of the TEETH IN A DAY™ crown. Figure 10C Anterior-lateral view of the TEETH IN A DAY™crown shows appropriate labial gingival support.
www.teeth-usa.com4
Figure 9 The finished TEETH IN A DAY™ restoration onthe CeraOne stainless steel analogue.
The Institute For Facial EstheticsContinuing Education
Traditional 2-Stage Implant Protocoland
1-Stage TEETH IN A DAY™
The Institute For Facial Esthetics Reserves the right to cancel the course at any time with no responsibilityother than full refund of tuition paid. No refunds made within 48 hours of the course.
Location:Institute for Facial Esthetics
467 Pennsylvania Avenue #201Fort Washington, PA 19034
Faculty:Thomas J. Balshi, DDS, FACP
Glenn J. Wolfinger, DMD, FACPRobert Winkelman, CDT, MDT
Time: 8:00 AM - 6:00 PM
Lunch 12:00 - 1:00 PM
Course Dates:September 15-16-17, 2003
January 19-20-21, 2004September 20-21-22, 2004
Educational Objectives: To teach and demonstrate the effect of osseointegrateddental implants on facial esthetics and general patient well-being; To provide clinicalinstruction and hands-on implant training; To provide clinical patient managementbefore, during, and after dental implant rehabilitation; To provide post-prosthesismaintenance via home and professional oral hygiene.
Course Content: Includes the fundamentals of implant surgery and prosthetics,patient selection, treatment planning, drape and anesthesia, evaluation of implantsites, bone preservation, site preparation, implant placement, surgical closure,abutment connection, loading of implants, post-op instructions. Special considerationsinclude graft areas, anatomic defects, immediate extractions sites, delayed extractionsites, complications, preventing and solving problems, and TEETH IN A DAY™for the maxilla and mandible.
Teaching Methods: Lectures, slides, videos, hands-on surgical and prostheticprocedures. Live surgery observed.
Seminar Includes: Certificate of attendance, course materials, lunch andrefreshments.
Tuition:$ 1800
*Nobel Biocare is an ADA CERP Recognized Provider. The formal continuingeducation programs of this sponsor are accepted by the AGD for Fellowship/
Mastership credit. Participants are eligible for 24 hours of continuingeducation credit. Continuing education credits issued for participation in this
CE activity may not apply towards license renewal in all States.
For more information or to register:call 215-643-5881 or fax 215-643-1149
Credits:Eligible for 24 hours of
continuing education credit
www.teeth-usa.com5
Clinical treatment continued during thislaboratory phase. Autogenous boneobtained from the osteotomy site wasused to fill voids between the socket walland the implant surface.
Cementation of the acrylic crown wasaccomplished with a carboxylate cement(Duralon, ESPE America Inc.,Norristown). Only the thinnest amountof cement was required in order to avoidthe extrusion of excess into the creviculararea of the fresh extraction site. Thecontours of this restoration were designedto mimic the original tooth and root form,sealing the socket and maintaining clotformation subgingivally. Themorphology of this restoration alsoprovided support of the labial gingiva(Fig 10a, b, c).
No sutures are required when sculptingthe restoration in this fashion. Thisincisionless-sutureless procedureprovides an exceptionally fast recoverywith very little if any postoperativediscomfort. Standard protocol formedications following implant surgerywas given to the patient along withpostoperative instructions cautioningpremature function on the individualimplant (Fig 11).
In many similar patients, the masterimpression can be made at the time ofthis one-stage procedure, just prior tocementation of the TEETH IN A DAY™crown. In this instance, the patientreturned four months after the TEETHIN A DAY™ procedure for the finalimpression followed a few days later bydelivery of the porcelain fused to goldimplant supported crown.
Figure 10A -- Front smiling viewmoments after the cementation of therestoration.
Featuring the Brånemark System®Co-sponsored by Nobel Biocare USA, Inc.*

Prosthodontic Insights is published byProsthodontics Intermedica and distributed
without charge to qualified individuals. Pleaserequest a subscription on your organization’s
letterhead.Prosthodontics Intermedica
467 Pennsylvania Avenue, Suite 201, FortWashington, PA 19034 U.S.A.
Tel: 215-646-6334 Fax: 215-643-1149Email: [email protected]
www.teeth-usa.com6
Immediate Functional Loading ofBrånemark Single Tooth Implants.A 5-year clinical follow-up study.
Ingvar Ericsson et al
In a long-term prospective study (5 years), thetreatment outcome of single tooth replacementswith artificial crowns retained to implantsinstalled according to a one-stage surgicalprocedure and immediate loading (ExperimentalGroup) in comparison to the original 2-stageconcept (Control Group) was challenged.
The Experiment Group consisted of fourteenpatients with a total of 14 missing single teeth.One Brånemark implant was placed in eachpatient according to the standard protocol (Table1). A Brånemark System CeraOne abutment wasthen connected and a provisional crown wascemented to the abutment within 24 hours. Goodclinical initial stability was obtained in all cases.Two of these fixtures were lost (14%) withinthe first 5 months of function. No further losseswere observed. Thus, it is obvious that ifcomplications occur, they occur early followingplacement and immediate loading.
The Control Group consisted of 8 patientstreated with 8 single tooth replacements onBrånemark implants during the same period oftime and according to the traditional two-stageprotocol. No implants were lost up to 5 yearsfollow-up.
This study indicates that immediate functionalloading of implant-supported single-toothrestorations is possible. The design of the studywas based on knowledge obtained mainly fromprevious studies.
Applied Osseointegration ResearchVolume 2, Number 1, 2001
Four dental implant specialists explain dental implant treatment step by step, in a first-of-its-kind book. Among the topics the authors cover: who is a candidate for implants, theadvantages of implants, how implants are surgically placed, how to find a qualified dentist,and follow-up care. The book is loaded with before and after photos of patients.
This book can be ordered from Prosthodontics Intermedica as early as March 2003.
By Thomas Balshi, DDS, William Becker, DDS, Edmond Bedrossian, DDS, Peter Wohrle, DMD
Top Related