







Languages
Pages
Legal

Service Navigation Resolving Challenging and Complex Issues
for Children to Improve Health, Safety, and Well-being
Joelle Aboytes, Esq.Circuit 5 Community Development
AdministratorFlorida Department of Children and
Families
Zackary GibsonChief Child Advocate and Director
Office of Adoption and Child ProtectionExecutive Office of the Governor

AGENDA
• POLL - Which Region are You From?• POLL - Which System do you work in?• Florida Children and Youth Cabinet
o Agency Prevention Serviceso Social Determinants of Healtho Prevention Frameworko Protective Factors & Protective Capacitieso Social-Ecological Model
• Cabinet Interagency Agreement and Process Framework• Service Navigation Worksheet• Case Examples• Q & A
Florida Children and Youth CabinetSection 402.56, F.S.
• Ensures the public policy relating to children and youth is developed to promote interdepartmental collaboration and program implementation.
• To improve:
o Healtho Safetyo Economic Stability o Self-sufficiencyo Quality of Life
https://www.flgov.com/childrens-cabinet

Agency Prevention ServicesAcross the Life Course

Social Determinants of Health
The conditions of the social, economic, and physical environments in which we live, work, play, worship, and age
that affect our health and the health of the community.
Education Access & Quality
(Self-sufficiency)
Health Care Access & Quality
(Health)
Social & Community Context
(Quality of Life)
Neighborhood & Built Environment
(Safety)
Economic Stability
(Economic Stability)
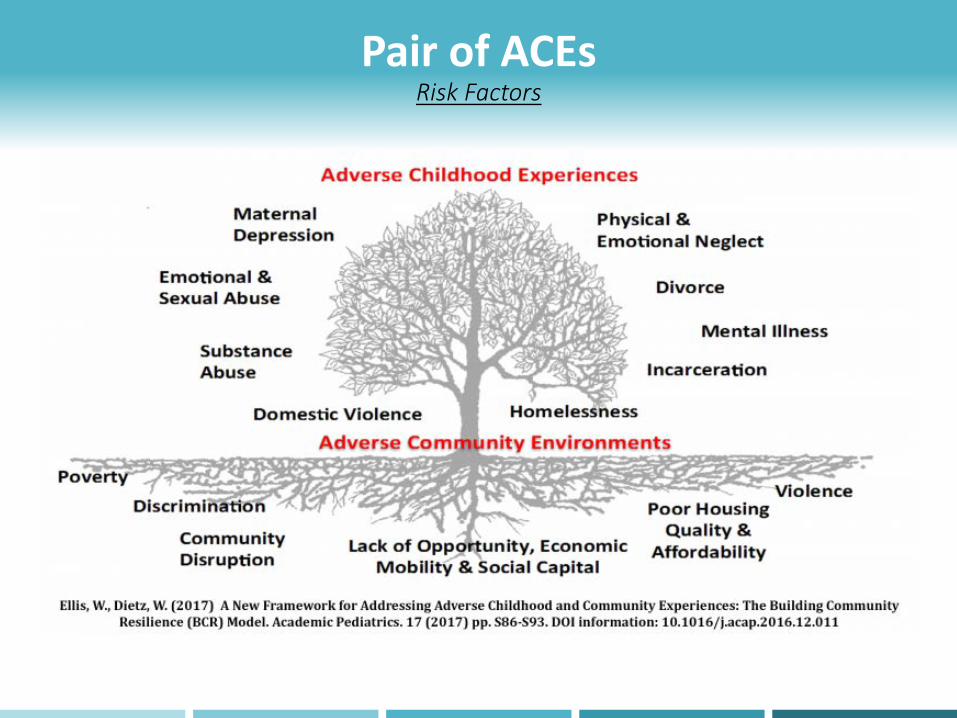
Pair of ACEsRisk Factors
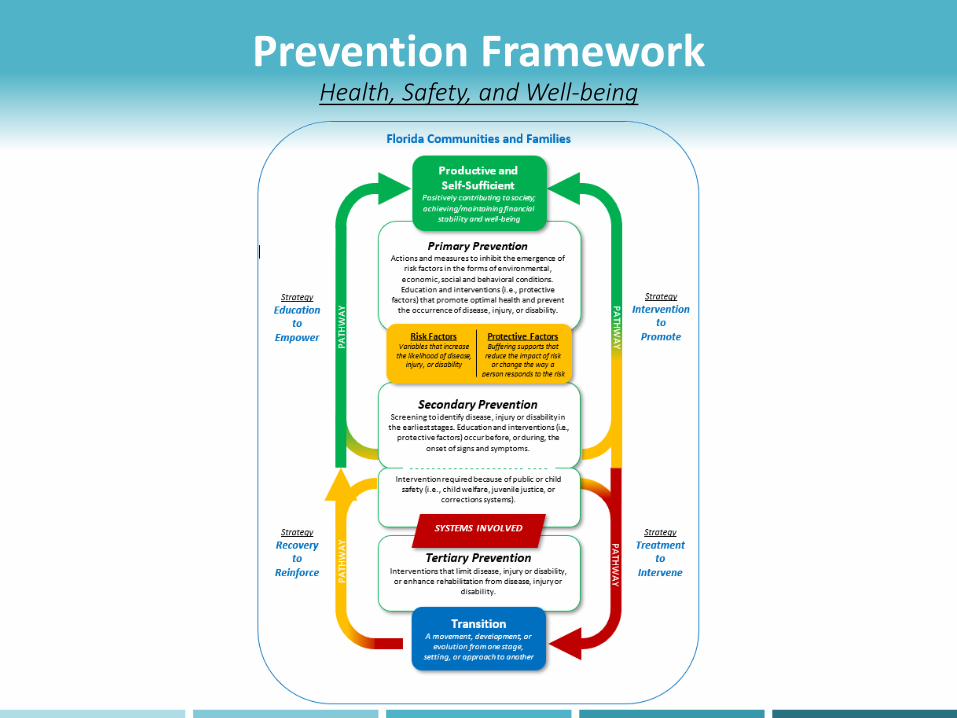
Prevention FrameworkHealth, Safety, and Well-being
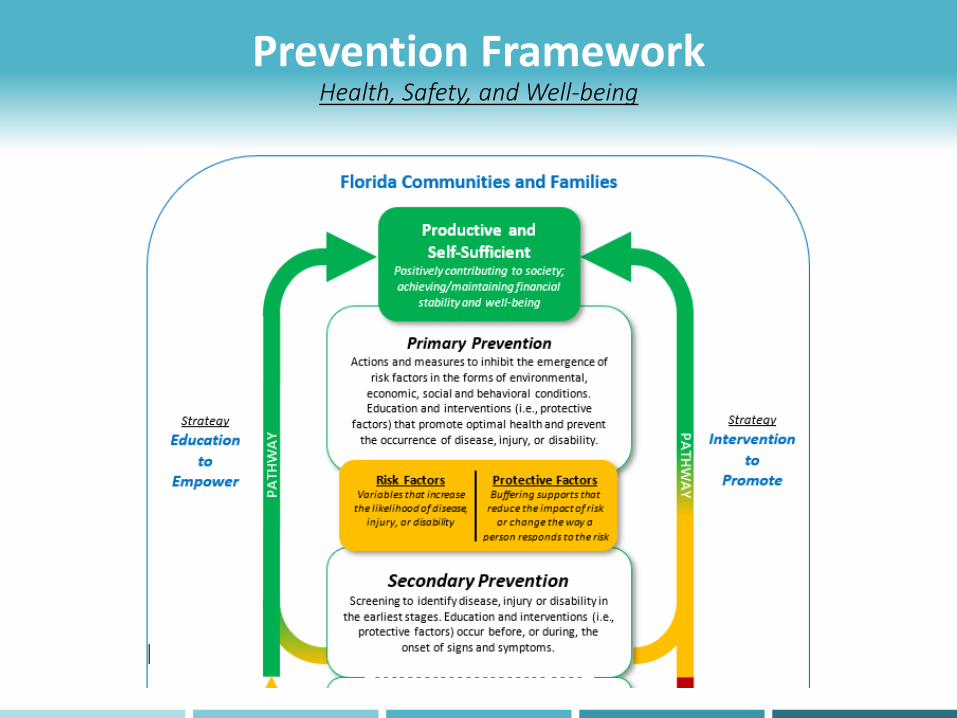
Prevention FrameworkHealth, Safety, and Well-being

Prevention FrameworkHealth, Safety, and Well-being

Prevention FrameworkHorizontal Perspective
Education to Empower
Intervention to Promote
Treatment to Intervene
Recovery to Reinforce
Florida Communities and Families
Primary Prevention Secondary Prevention Tertiary Prevention
Strategy Treatment to
Intervene
SYSTEMS INVOLVED
Strategy
Recovery to Reinforce
Strategy
Intervention to Promote
Strategy
Education to Empower
COMMUNITY INVOLVED
Productive and Self-Sufficient
Risk and Protective Factors
Transition

Protective Factors and Protective CapacitiesStrength-based Approaches
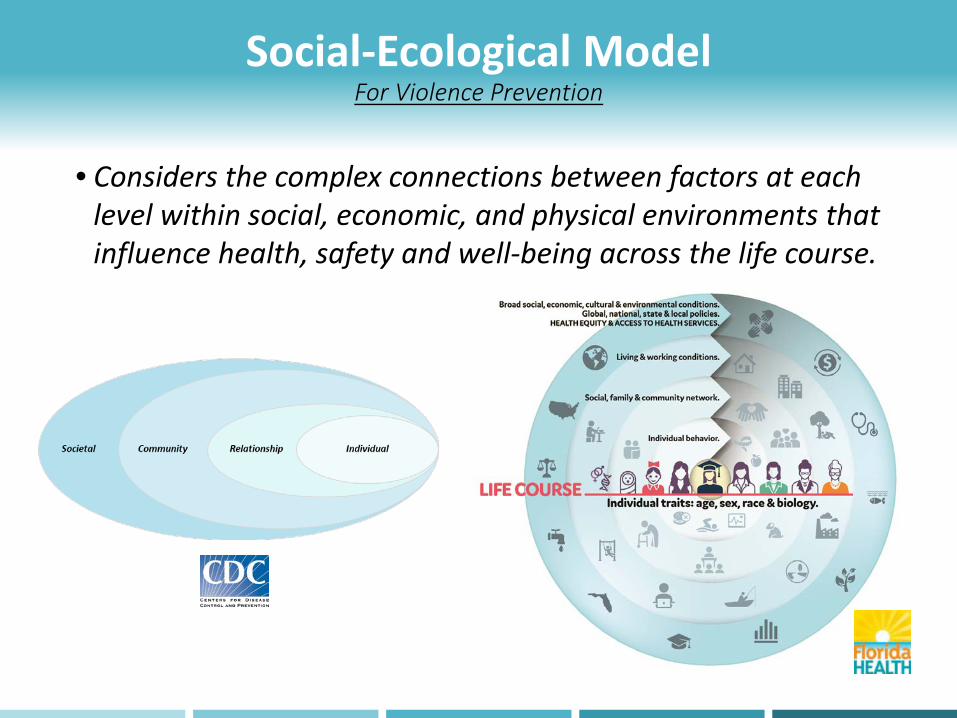
Social-Ecological ModelFor Violence Prevention
• Considers the complex connections between factors at each level within social, economic, and physical environments that influence health, safety and well-being across the life course.

Cabinet Interagency Agreement
http://centerforchildwelfare.fmhi.usf.edu/CoordServices.shtml
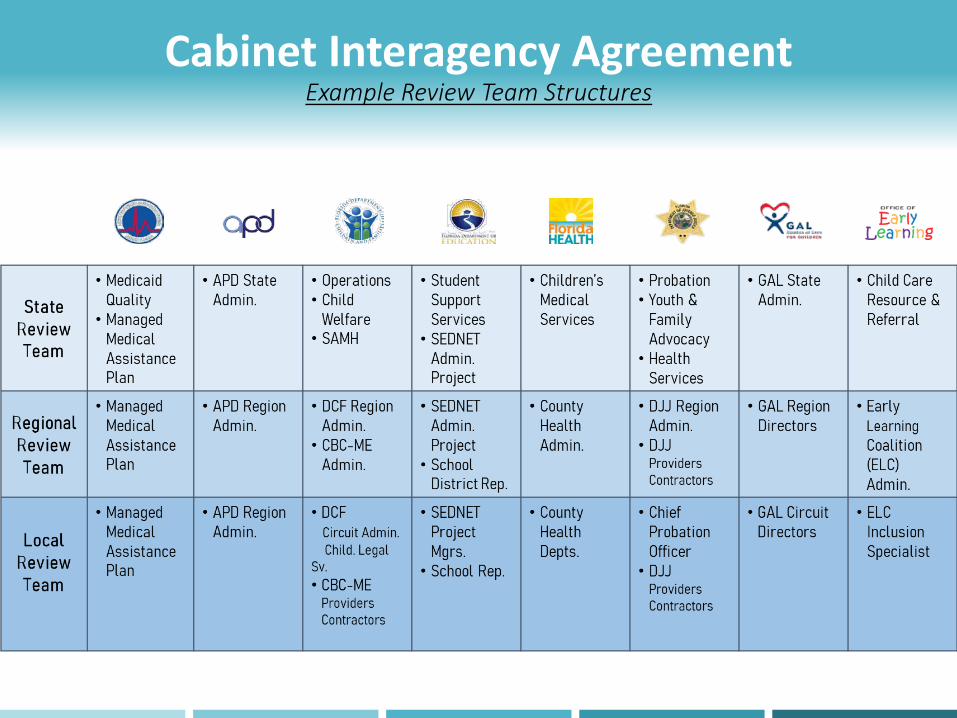
Cabinet Interagency AgreementExample Review Team Structures
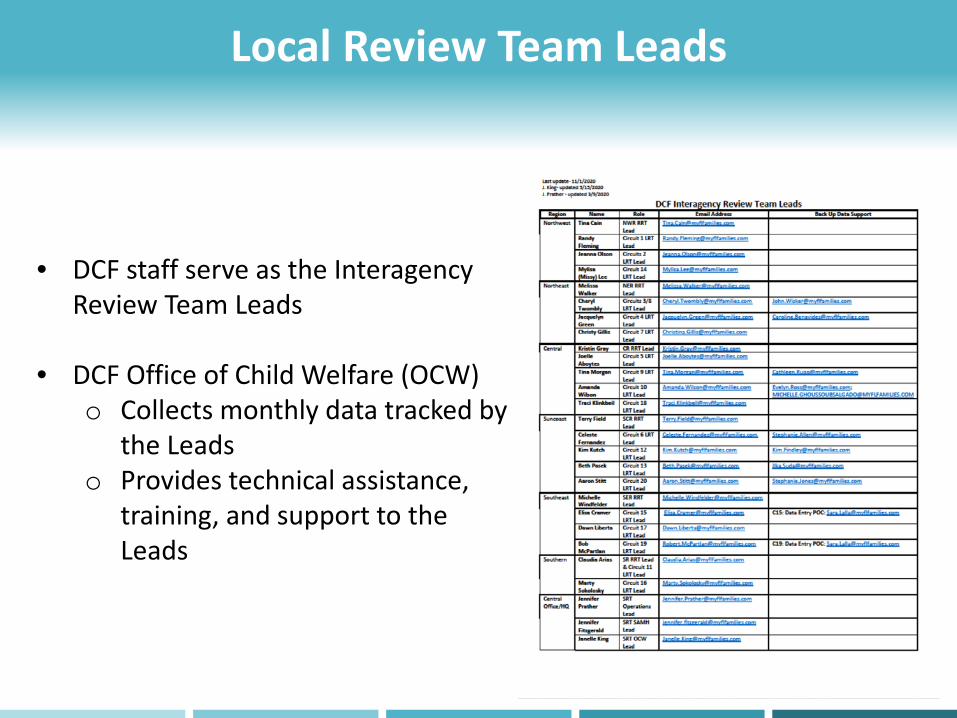
Local Review Team Leads
• DCF staff serve as the Interagency Review Team Leads
• DCF Office of Child Welfare (OCW) o Collects monthly data tracked by
the Leadso Provides technical assistance,
training, and support to the Leads

Local Review Team – Quick Reference Guide
• Who are the points of contact for the different child-serving systems?
• Contact your respective LRT Lead for help with connecting to the right contacts.
• Some Circuits have developed a Local Review Team – Quick Reference Guide or Other Point of Contact Sheet.

Services Navigation Worksheet
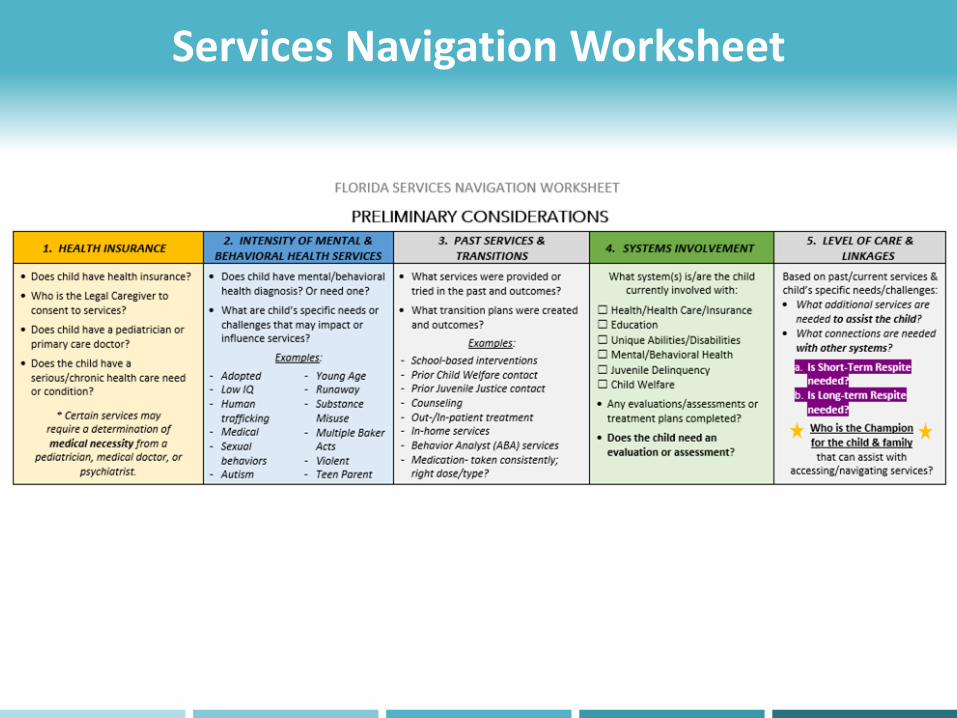
Services Navigation Worksheet

Services Navigation Worksheet

Florida Medicaid PlansFlorida State Medicaid Managed Care - Letters and Brochures (flmedicaidmanagedcare.com) (SMMC Brochure CY19)
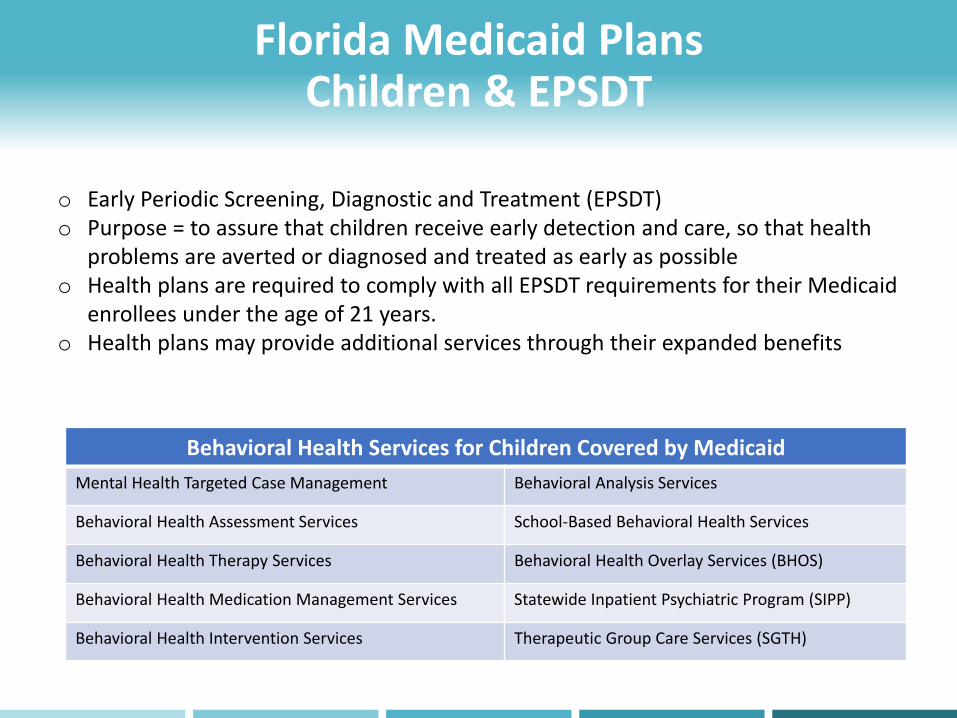
Florida Medicaid PlansChildren & EPSDT
o Early Periodic Screening, Diagnostic and Treatment (EPSDT) o Purpose = to assure that children receive early detection and care, so that health
problems are averted or diagnosed and treated as early as possibleo Health plans are required to comply with all EPSDT requirements for their Medicaid
enrollees under the age of 21 years.o Health plans may provide additional services through their expanded benefits
Behavioral Health Services for Children Covered by MedicaidMental Health Targeted Case Management Behavioral Analysis Services
Behavioral Health Assessment Services School-Based Behavioral Health Services
Behavioral Health Therapy Services Behavioral Health Overlay Services (BHOS)
Behavioral Health Medication Management Services Statewide Inpatient Psychiatric Program (SIPP)
Behavioral Health Intervention Services Therapeutic Group Care Services (SGTH)
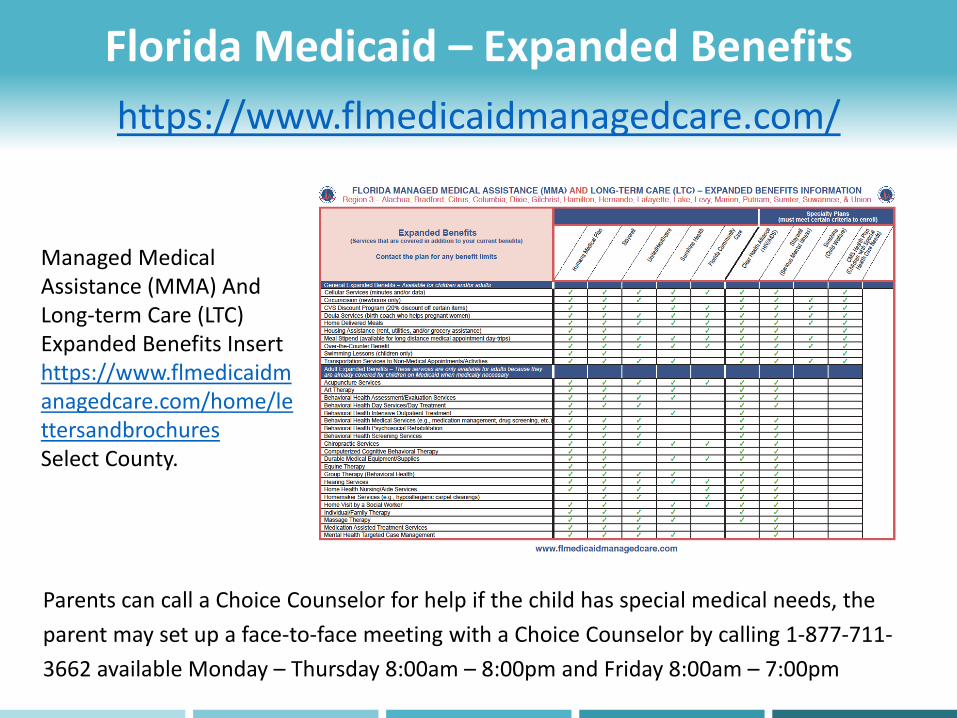
Florida Medicaid – Expanded Benefitshttps://www.flmedicaidmanagedcare.com/
Managed Medical Assistance (MMA) And Long-term Care (LTC) Expanded Benefits Insert https://www.flmedicaidmanagedcare.com/home/lettersandbrochuresSelect County.
Parents can call a Choice Counselor for help if the child has special medical needs, the parent may set up a face-to-face meeting with a Choice Counselor by calling 1-877-711-3662 available Monday – Thursday 8:00am – 8:00pm and Friday 8:00am – 7:00pm

Service Navigation: Health Insurance Child Abuse Investigation for 7 yr. old, M.R Allegations included: “M.R. has multiple bruises on the inside of both of her upper thighs and injuries on her hand. M.R. is nonverbal, and she is not able to say how she got the injuries. The bruises are the size of finger bruises and they are dark in color. Abuse is suspected with the bruises. M.R. does self abuse by biting her wrists. M.R lives with the mother and the mother's boyfriend. It is believed that there is shared custody with the father. M.R is primarily with the mother. There is suspected drug abuse in the mother's house. The mother's language is very slurred.”
During the investigation the following additional information is obtained:
• Child is highly self-injurious and frequently has outbursts at school and at home. The family has trouble controlling the youth's behaviors, and requires supports and services
• Per the school, the child is language impaired and requires occupational and speech therapy each week.
• Per school, child has been referred to an endocrinologist and psychiatrist.
• Child has multiple bite marks where skin is draining and the back of her left hand was oozing.
• Child had ABA services in the home but closed out due to multiple no-shows and appointment cancellations.
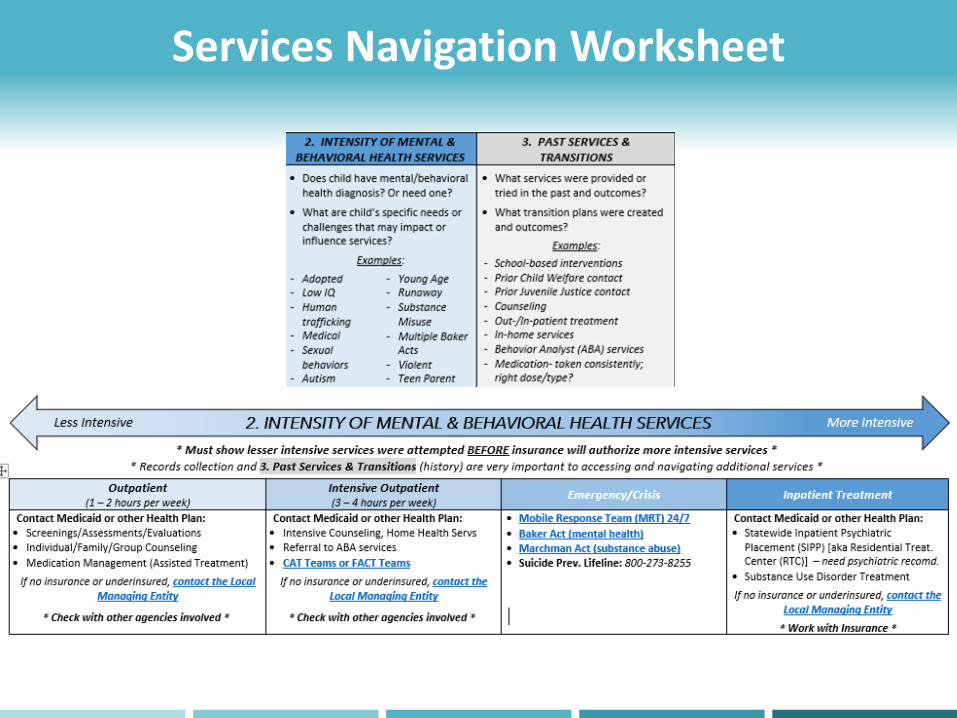
Services Navigation Worksheet
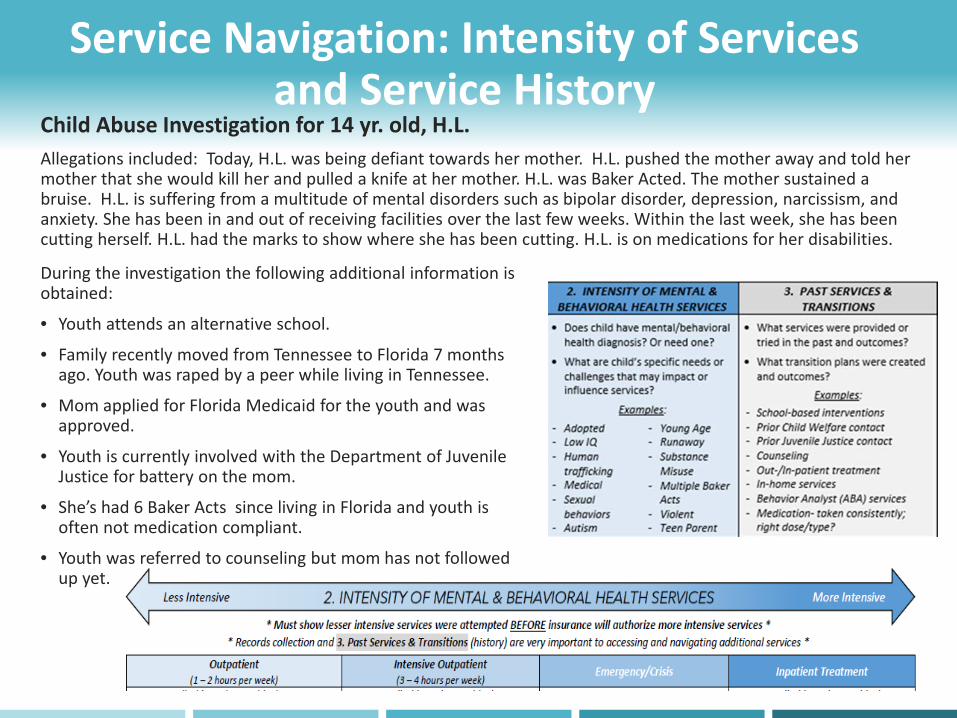
Service Navigation: Intensity of Services and Service History
Child Abuse Investigation for 14 yr. old, H.L. Allegations included: Today, H.L. was being defiant towards her mother. H.L. pushed the mother away and told her mother that she would kill her and pulled a knife at her mother. H.L. was Baker Acted. The mother sustained a bruise. H.L. is suffering from a multitude of mental disorders such as bipolar disorder, depression, narcissism, and anxiety. She has been in and out of receiving facilities over the last few weeks. Within the last week, she has been cutting herself. H.L. had the marks to show where she has been cutting. H.L. is on medications for her disabilities.
During the investigation the following additional information is obtained:
• Youth attends an alternative school.
• Family recently moved from Tennessee to Florida 7 months ago. Youth was raped by a peer while living in Tennessee.
• Mom applied for Florida Medicaid for the youth and was approved.
• Youth is currently involved with the Department of Juvenile Justice for battery on the mom.
• She’s had 6 Baker Acts since living in Florida and youth is often not medication compliant.
• Youth was referred to counseling but mom has not followed up yet.
PART 1 CONCLUSION: Q & A
This Photo by Unknown Author is licensed under CC BY-NC

Services Navigation Worksheet
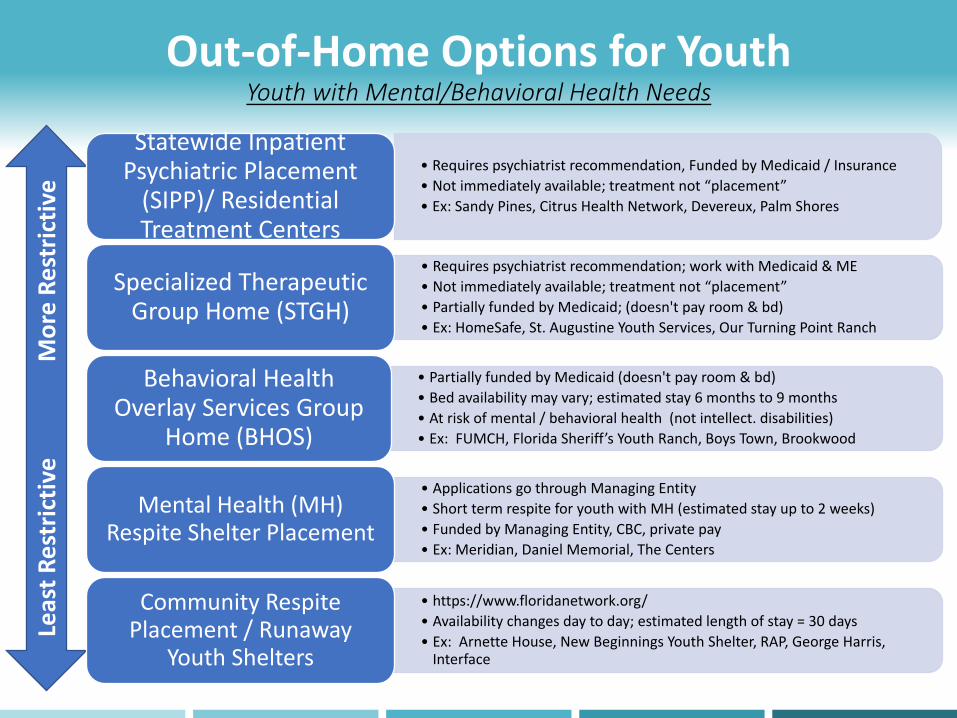
Out-of-Home Options for YouthYouth with Mental/Behavioral Health Needs
Leas
t Res
tric
tive
M
ore
Rest
rictiv
e
• Requires psychiatrist recommendation, Funded by Medicaid / Insurance• Not immediately available; treatment not “placement”• Ex: Sandy Pines, Citrus Health Network, Devereux, Palm Shores
Statewide Inpatient Psychiatric Placement
(SIPP)/ Residential Treatment Centers
• Requires psychiatrist recommendation; work with Medicaid & ME• Not immediately available; treatment not “placement”• Partially funded by Medicaid; (doesn't pay room & bd)• Ex: HomeSafe, St. Augustine Youth Services, Our Turning Point Ranch
Specialized Therapeutic Group Home (STGH)
• Partially funded by Medicaid (doesn't pay room & bd)• Bed availability may vary; estimated stay 6 months to 9 months• At risk of mental / behavioral health (not intellect. disabilities) • Ex: FUMCH, Florida Sheriff’s Youth Ranch, Boys Town, Brookwood
Behavioral Health Overlay Services Group
Home (BHOS)
• Applications go through Managing Entity • Short term respite for youth with MH (estimated stay up to 2 weeks)• Funded by Managing Entity, CBC, private pay• Ex: Meridian, Daniel Memorial, The Centers
Mental Health (MH) Respite Shelter Placement
• https://www.floridanetwork.org/ • Availability changes day to day; estimated length of stay = 30 days• Ex: Arnette House, New Beginnings Youth Shelter, RAP, George Harris,
Interface
Community Respite Placement / Runaway
Youth Shelters

Services Navigation Worksheet

Services Navigation Worksheet

Instructions
You will review (2) case scenarios and answer some questions pertaining to how you may navigate services for the families:
• Scenario #1 - Child Investigation
• Scenario #2 – Lockout / Abandonment
We will utilize the poll function for some of the questions.
For open-ended questions, please use the hand-raise button and the organizer will unmute you so that you can answer the question or feel free to utilize the chat function to submit your answers.

Scenario #1 - Child Investigation DCF Received a Child Investigation for 9 ½ yr old L.M.
The mother hit L.M. and left him with a bruise on the left side of his bottom or hip. She hit him with a wooden grill spatula. L.M. has significant behavioral problems and is in a special program.
The mother asked L.M. if he had taken his medication and he advised that he did. L.M. is diagnosed with autism spectrum disorder (ASD). L.M. takes Abilify and ADHD medication prescribed by his primary care doctor. It is unknown if the child is really taking his medication. He has Staywell Medicaid. For the past three days, L.M.'s behavior has been "ramping up." It is unknown why L.M. wants to harm himself. Today, L.M. ran out of his class, threw sticks at teachers (as he ran away) and threatened to kill himself. He has difficulty regulating his emotions. He is educated in a self-contained classroom. He does get some counseling through Big Bear Counseling.
L.M.'s father is in jail for possession of child porn. The father has mental health history, and the child has been previously exposed to domestic violence. There is a suspicion of possible child abuse.

Navigating Services L.M. Exercise
1. What type of issues/ needs does the family have? EducationalMedicalMental Health/ Behavioral Health Services Records Collection – Baker Acts, Prior
Services, Evaluations TraumaParenting Support
2. What additional information do you need/ want to know?What health insurance plan does he have?Evals/ Assessments?Current / Past Services & Agency
Involvement?What is the child’s medication regimen?Whether mom has any supports for herself?Any other family support? (i.e. respite)Family mental health history?Extent of child’s trauma history?
3. Who / what agencies would you invite to a multi-disciplinary team staffing?MomCounselor School officials / School Resource OfficerCenter for Autism Related Disabilities
(CARD)Health Insurance PlanAgency for Persons with Disabilities
4. What ideas do you have for placement and services for the child?Behavioral Health Coordination through
health planCase Management Services either through
Targeted Case Management or CBC Diversion ServicesIncreased Counseling services and/ or
Referral to the CAT teamPsychiatric evaluationIn-Home Respite OptionsNon-Traditional Therapy

Scenario #2 - Lockout/ AbandonmentThe DCF Hotline received two reports on siblings from the same household: (1) Child Investigation for 17 ½ yr old youth, D.V., and (2) Adult Protective Investigation for 19 yr old, E.R. Both youth are autistic, severely intellectually disabled and non-verbal and attend a special school. The family home burned down. The grandmother and the Uncle have joint permanent guardianship over D.V. from a prior dependency case. The grandmother is the one listed on the both youth’s Children’s Medical Services Medicaid plan and the grandmother receives SSI for both youth. The family does not receive food stamps. The biological mother has a long history of substance use and mental health issues. The father is deceased.
There is no family at the hospital with D.V. and E.R. Their family was not present upon arrival. Grandmother and Uncle usually care for them. Grandmother is in a physical rehab facility due to E.R. breaking her arm and foot. E.R. is aggressive and has a history of Baker Acts but is released quickly due to her intellectual disabilities. It is unknown if grandmother can continue to care for the youth. The Police Department tried to locate other family but the only potential relative is the Uncle. The Uncle is staying at a friend’s house in a 55 and older community. Both youth have been medically cleared and are currently being discharged from the hospital today.

Navigating Services D.V. & E.R. Exercise
1. What type of issues/ needs does the family have? EducationalMedicalMental Health/ Behavioral Health Services Records Collection – Baker Acts, Prior
Services, Evaluations HousingFinancial
2. What additional information do you need/ want to know?What health insurance plan?Evals/ Assessments?Current / Past Services & Agency
Involvement?Require any special medical equipment/
meds?Any other family support? (i.e. respite)Status with Agency for Persons With
DisabilitiesStatus of the SSI funds?
3. Who / what agencies would you invite to a multi-disciplinary team staffing? Uncle School officials Center for Autism Related Disabilities Health Insurance Plan Adult Protective Investigations (API) ESS/ ACCESS staff Community Based Care (CBC) Agency for Persons with Disabilities Homeless Coalition Staff
4. What ideas do you have for placement and services for the child? Behavioral Health Coordination through health
plan Prevention Services through Community Based
Care (CBC) (hotel funding) Housing Assistance through Health Plan In-Home Respite Options Work with Agency for Persons With Disabilities
for group home placement Guardianship Advocacy
Q & A
This Photo by Unknown Author is licensed under CC BY-NC

Thank you!!Joelle Aboytes, Esq.
Circuit 5 Community Development Administrator
Florida Department of Children and Families
Zackary GibsonChief Child Advocate and Director
Office of Adoption and Child Protection-Executive Office of the Governor
Top Related