







Languages
Pages
Legal


Royal Free London
NHS Foundation Trust
Our Integrated Care Journey
Dr. Alexandra Wu
Clinical Director
Service Transformation

The Royal Free
Integrated Care Journey
Scope and Contents
• What is integrated care?
• Why do integrated care?
• What is involved?
• How did we do it?
• What did we learn?
• How did we evolve from our learning?
• Summary and conclusions
• Questions & Answers

The Royal Free• Licensed as a Foundation
Trust since April 2012
• Merged with Barnet and
Chase Farm Hospitals
(July 2014)
• £1 Billion turnover
• 10,000 full-time staff
• 1100 beds approximately
• Teaching hospital and a
tertiary with district
general function

1. What is integrated care?
• Meeting the needs of individuals by flexible and
seamless working across multiple organisations to
deliver optimal and personalised care whether in
hospital or at home
• This is a collective responsibility between the
primary and secondary sectors.
2. Why do integrated care?
• Current economic environment for the NHS
• QIPP - Imperative is to achieve ‘best in class’
clinical productivity (length of stay, re-admissions,
excess bed days)
• Clinically led pathway redesign focused on patient
cohorts
• Results in length of stay reductions and admissions
avoidance

3. What’s involved• Two innovations in September 2010
– Post Acute Care Enablement (PACE)
– Triage Rapid Elderly Assessment Team (TREAT)
• Patient cohort
– Complex, elderly patients
– Urgent care division
• Department involved
– Health Services for Elderly People (HSEP)
– 3,200 emergency admissions/year, 40% of acute take
– Chronic long-term conditions, care homes, variable acuity
• Aim to deliver a different model of care
– Reduce admissions
– Early support discharge
– As safe and as high quality but in a lower cost setting
• Funding and resources
– Closure of 18 bedded acute medical ward to re-direct funding for the innovations
– Appointed Dr. Alexandra Wu as clinical champion and Kam Karilai as project
manager under the direction of Katie Donlevy, Director of Integrated Care

4. How did we do it?• Brainstorm with multi agencies in May 2010
• Build relationships, establish capabilities and facilities available
• Identify patient groups and wards
• Map out patient’s pathway, define process and logistics
• Define joint clinical governance with clear roles and responsibilities
• Agree data collection criteria
• Estimate staffing requirements
• Define outcomes and performance measures
• Set up steering team (led by clinical champion) and weekly meeting
• Agree timeline for implementation, starting in September 2010.
POST ACUTE CARE ENABLEMENT
(PACE)
8

What is PACE?
• Early supportive discharge service
• Later part of an acute episode delivered in an out of hospital setting
• But still under auspices of the acute team
• On site community case finders integrate with acute team to ‘Pull’ patients
• Patient no longer requires 24hour inpatient medical care
• Patient has on-going nursing & medical monitoring needs that can be safely met outside of the hospital environment
• Content of care more medical and intensive than traditional intermediate care
• Provider to provider collaboration
An Integrated
model of care
linking with the
community
Increased
patient choice
Reduced
number of
Admissions
Reduced
Length of StayBeds closed
as a result
Delivering high
quality care
at a lower cost
Aim of PACE
• Provide an integrated model of care linking with the
community
• Increase patient choice
• Reduce number of admissions (supporting admission
avoidance team TREAT)
• Reduce length of stay
• Make bed day savings
• Deliver high quality care at a lower cost
Royal Free PACE
• Provider to provider collaboration:
– RFH
– Barnet Community Services
– Camden Provider Services
– London Boroughs of Barnet and Camden
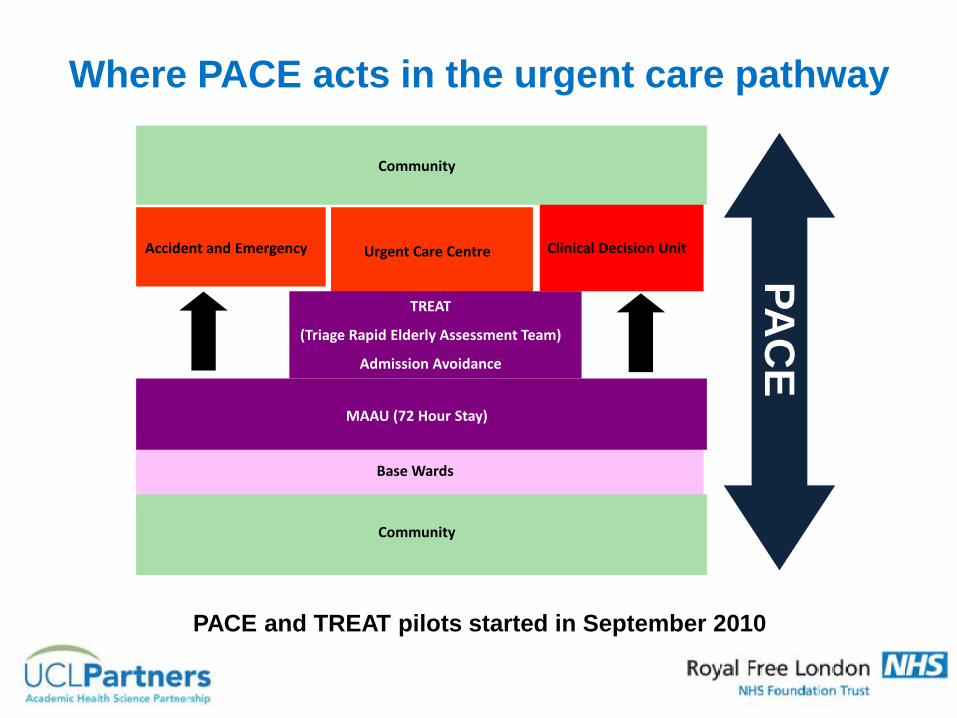
Clinical Decision Unit
Base Wards
Urgent Care CentreAccident and Emergency
Community
Community
PACE
PA
CE
TREAT
(Triage Rapid Elderly Assessment Team)
Admission Avoidance
MAAU (72 Hour Stay)
PACE and TREAT pilots started in September 2010
Where PACE acts in the urgent care pathway

Sample case• Elderly man
• Septic
• Acute urinary retention
• Faecal impaction
• Reduced mobility
• Needs increased care package
Management plan:
PRE PACE PACE
Day 1 Catheterisation Day 1 HOME
Bowel clearance
Intravenous antibiotics
Day 2 Physiotherapy & Occupational Therapy assessment
Social services review
Day 3 Trial without catheter
Day 4 Observations for improvement
Wait for care package
Day 5 Discharge – MAY BE?
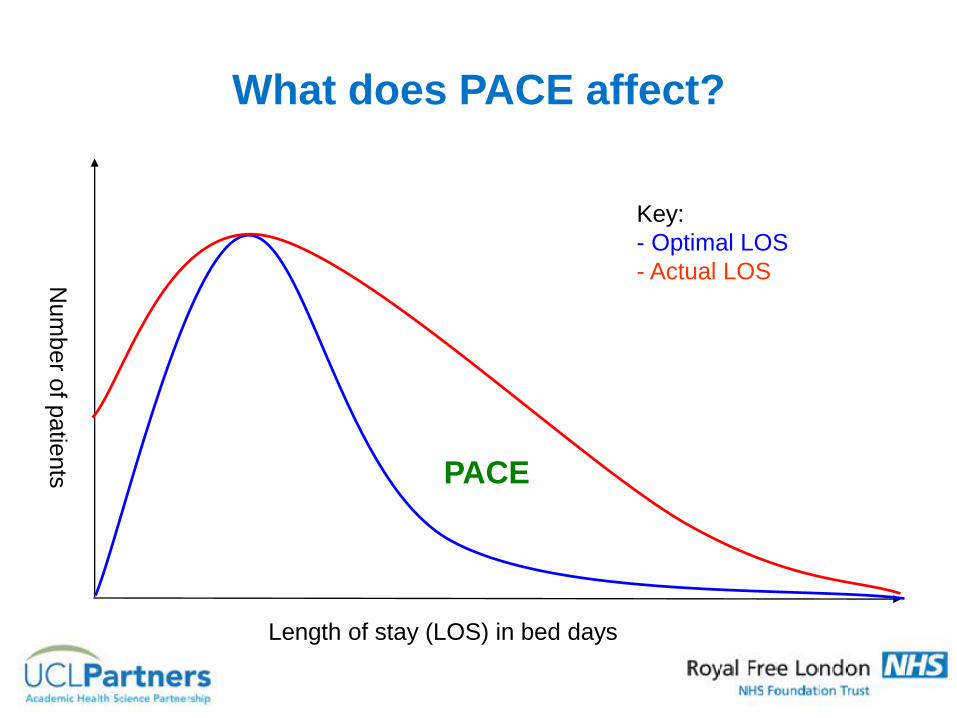
What does PACE affect?
Length of stay (LOS) in bed days
Num
ber o
f patie
nts PACE
Key:
- Optimal LOS
- Actual LOS
Conditions Suitable for PACE
• Exacerbation of COPD
• Faecal Impaction/ Urinary retention
• Simple infections- Cellulitis , UTIs
• Deep Vein Thrombosis
• Falls
• Diabetes
• All of the above + cognitive impairment
Low Acuity Patients

Typical PACE Patients Monitoring
• General observations including Postural Blood Pressure, Peak Flow, Oxygen Saturation, Blood Sugar Monitoring etc.
• Blood Tests including INR
• Administer medications including enemas & IV antibiotics
• Monitor medication & titrating analgesia
• Bowel care
• Catheter care and bladder scanning
• Wound care
• Ambulatory 24 hour ECG
• ! Assess daily & Escalate : Signs of deterioration
• ! Signposting

The clinical model
• Daily MDT board rounds (clinical champion present)
• Patients identified by medical team and on site ‘pulling’ case finders(senior experience community staff)
• Comprehensive assessment undertaken
• Clear follow-up and escalation process in place
• Patient goes home within 4 hours of acceptance onto PACE
• All onward social care needs managed by PACE team
• Up to 5 days input (flexible) and clinical responsibility remains underdischarging team

Implementation
• Must be clinically led & driven - CHAMPIONS
• Focus on few cohorts with high gains e.g. frail elderly
• Agree evaluation measures up front and make sure you capture the data
• Create the evidence base as the service develops
• PACE will surface operational issues requiring weekly meetings
• Improve by pathway mapping
• Marketing - engage and communicate with patients or clinicians (RFH and GPs)
• Educate – road shows, workshops and work alongside

Data and Outcome Measures
• Health Resource Group (HRG)
• Attendances
• Admissions
• Length of Stay (LoS)
• Re-admissions
• Patient satisfaction
• Clinical Incidents and Discharge Alerts

Evaluation of RFH PACE
• Patient satisfaction high
• Beds closed as a consequence – LOS reduction average 3 days per patient
Week 234 ( Feb 2015) Borough
Barnet Camden
Referred 4255 4654
Accepted 2995 3142
Discharged 2927 3090
Readmitted 92 153
Summary
Total Patients Referred 8909
Total Number of Patients Accepted 6137 (69%)
Total Number of Patients Discharged 6017 (98%)
Total Number of Patients Re-admitted (5 days) 245 ( 4%)

All patients with PACE
diagnosis

Length of stay now
Management Support
• Monthly PACE Operational group: – Alex Wu (chair, Clinical Director Service Transformation),
– Fran Gertler (Head of Integrated Care)
– Kam Kalirai (Associate Director of Service Improvement)
– Community MDT
• LOS and QIPP Steering group: – Katie Donlevy (Director of Service Transformation)
– Kate Slemeck (Chief Operating Officer)
– Janet Mustoe (hospital director)
– Operations and nursing managers
• Data Analysts/Administration support
• Funding

T.R.E.A.TAdmission
Avoidance
Avoid admissions through rapid multi-disciplinary assessment and treatment
7 days a week consultant led service based in A&E
Rapid access investigations and interventions.
Emergency Social packages
Work proactively with GPs, community teams and care homes
Return patients safely to the community
Specialist nurses- triage/outreach
Enhanced patient experience supported by post-discharge follow-up phone call
Prepared by Kam Kalirai Head of Service Redesign 190511
• Set up on a daily basis
• Responsive to urgent referrals
• Aim to avert crisis leading to hospital admission.
• Rapid multi-disciplinary review
• Rapid communication with primary care
• Hot lines manned by consultants
SINGLE POINT OF CONTACT
T.R.E.A.TAdmission
Avoidance
‘Hot Clinics’
‘Hot Lines’

TREAT results
• Reduced length of stay
• Patient satisfaction extremely high
• Has now attracted substantial commissioner funding
No. of patients 2011/2012 2012/2013 2013/2014
Triaged 1614 2461 2306
Suitable for TREAT
584 (30%) 863 (35%) 866 (37%)
Discharged by TREAT
477 (82%) 628 (78%) 621 (72%)
Discharged with PACE
216 (45%) 289 (48%) 268(31%)Rapid Response started
New TREAT team
• 6 consultant geriatricians
• 2 acute specialist nurses (Band 6 and 7)
• 2 community specialist nurses (Band 6)
• 2 juniors doctors F2/ST/SpR
• Occupational therapist
• Pharmacist
• Social Services
• Administrator and data analyst
• PACE/ RAPID RESPONSE TEAM


5. What did we learn?

BEFORE - The urgent care pathway
Clinical Decision Unit
Base Wards
Urgent Care CentreAccident and Emergency
Community
Community
TREAT
(Triage Rapid Elderly Assessment Team)
Admission Avoidance
MAAU (72 Hour Stay)
PACE and TREAT pilots started in September 2010
PACE
PA
CE
PACE
TREAT ADMISSIONS
LENGTH OF STAY
Increase patients’ choice of care
Lay foundation for integrated care
Increase capacity for new business
What we’ve learnt - 1

PACE
TREAT
RE-ADMISSIONS
(30 days)
ADMISSIONS
We need more than just
PACE and TREAT to drive
these down
LENGTH OF STAY
A&E ATTENDANCES
What we’ve learnt - 2

6. How did we evolve from our learning?

P
A
C
E
AFTER - New Integrated Health Care System
Extending into the Community
Community Hub
Purpose: Players:
- Case management MDT - GPs
- Multi-specialty clinics - Consultants
- Identify gaps in care - Therapists
- Social Services
- Community Matrons
- Mental Health Teams
Medical Admission
Unit (72 hours)
Attendance
PreventionFrailty screening
Target re-attenders
Care Home
Medicine
Elective
Ambulatory Care
Unit (PITU)
Day Surgery Unit
Surgical Admission
Unit (72 hours)
Base Ward (>72 hours)
Consultant-led
Assessment &
Discharge
Co-ordination Fast Diagnostics,
Clear Outcomes,
Get it right first time
E
D
U
C
A
T
I
O
N
Robust Administration, Data Collection & Quality Outcome Measures
Outreach
Domiciliary Visits
A&E Rapid Assessment Triage (RAT)
A&E (4 hours) Urgent Care Centre
Admission Avoidance (TREAT) + HOT Clinics
23 hour Emergency Assessment Unit
R
R
T

TREAT and PACE
Urgent Care Centre
A&E Re-design
Emergency Ambulatory Care Unit
RE-ADMISSIONS
(30 days)
ADMISSIONS
LENGTH OF STAY
A&E ATTENDANCES
Care Navigation Service
Community Hubs
Care Home Outreach
Elective Ambulatory Care Unit (PITU)
Day Surgery Unit
We need all the above components to achieve these targets
How we need to evolve
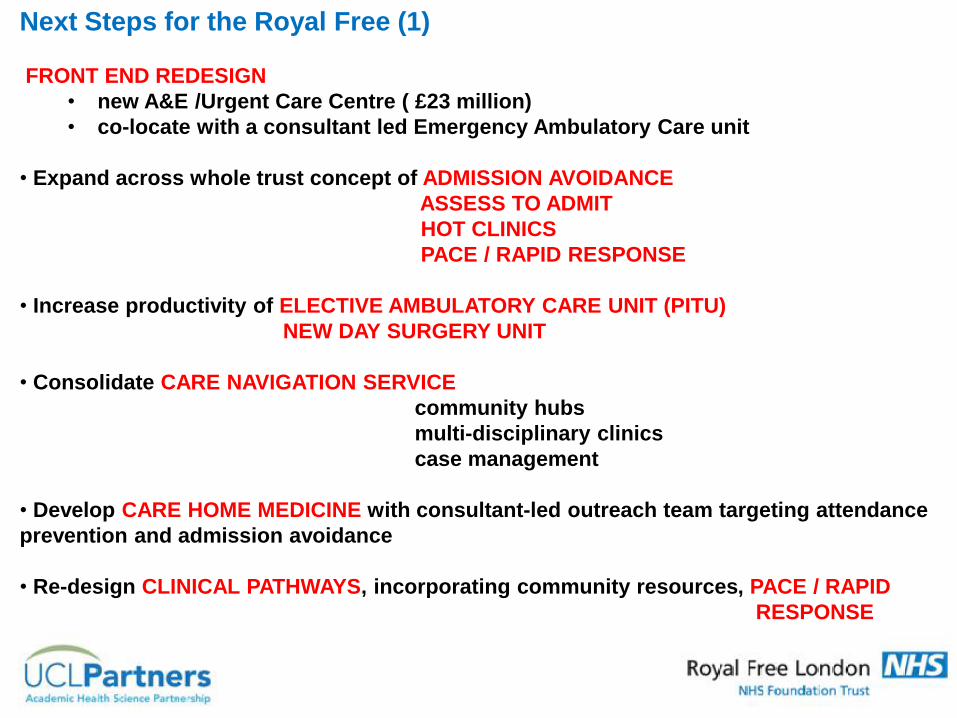
Next Steps for the Royal Free (1)
FRONT END REDESIGN
• new A&E /Urgent Care Centre ( £23 million)
• co-locate with a consultant led Emergency Ambulatory Care unit
• Expand across whole trust concept of ADMISSION AVOIDANCE
ASSESS TO ADMIT
HOT CLINICS
PACE / RAPID RESPONSE
• Increase productivity of ELECTIVE AMBULATORY CARE UNIT (PITU)
NEW DAY SURGERY UNIT
• Consolidate CARE NAVIGATION SERVICE
community hubs
multi-disciplinary clinics
case management
• Develop CARE HOME MEDICINE with consultant-led outreach team targeting attendance
prevention and admission avoidance
• Re-design CLINICAL PATHWAYS, incorporating community resources, PACE / RAPID
RESPONSE
Current Cellulitis Pathway
Referral routes
GP
OPD Clinics
Diabetic Foot
Plastics
Dermatology
Vascular
Scleroderma
Rheumatology
Dermatology
Heart Failure
Community Hubs
Camden and Barnet
A&E
Medical Expected ID or other speciality
Hot Clinics
ID clinics on Thursdays
Dermatology?
Vascular ?
Register patient in
Cerner
Patient assessed in
A&E
Register patient in
Cerner
Register patient in
Cerner
Patient assessed in Hot
Clinic
Patient assessed in ID
clinic
Patient treated in A&E
Patient Treated in Hot Clinic
Patient Treated in ID clinic
Does pt needs
Admission
Request a bed
OPATS 11 West day case ID Thursday
Pt given oral antibiotics and
home
PACE Ambulatory
A&EAmbulatory
first dose given in A&E
first dose IV given in A&E
Discharged to PACE
Patient attends Daily for 2ND & 3rd
dose given in GQ clinical review
Has patient
responds to iv
Pt given oral antibiotics and
home
Patient referred to ID 15% admitted
NO
NO
YES
YES
Patient assessed in
A&E by medical team
Patient treated in A&E
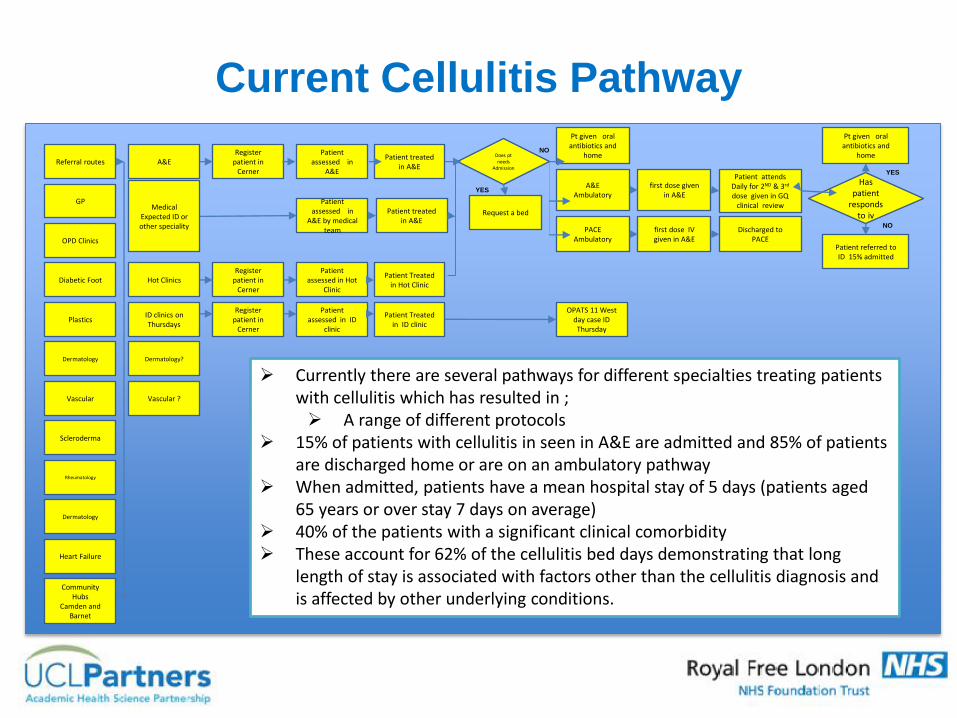
Currently there are several pathways for different specialties treating patients with cellulitis which has resulted in ; A range of different protocols
15% of patients with cellulitis in seen in A&E are admitted and 85% of patients are discharged home or are on an ambulatory pathway
When admitted, patients have a mean hospital stay of 5 days (patients aged 65 years or over stay 7 days on average)
40% of the patients with a significant clinical comorbidity These account for 62% of the cellulitis bed days demonstrating that long
length of stay is associated with factors other than the cellulitis diagnosis and is affected by other underlying conditions.
Streamlined Cellulitis Pathway
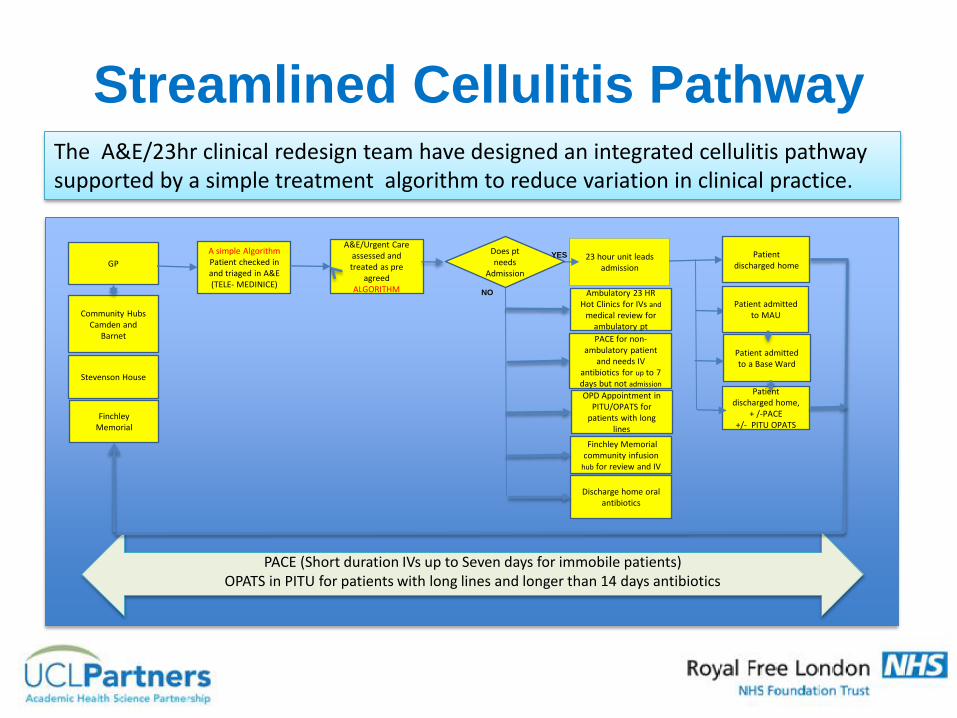
PACE (Short duration IVs up to Seven days for immobile patients)OPATS in PITU for patients with long lines and longer than 14 days antibiotics
GP
Community HubsCamden and
Barnet
A&E/Urgent Care assessed and treated as pre
agreed ALGORITHM
Stevenson House
Finchley Memorial
A simple AlgorithmPatient checked in and triaged in A&E(TELE- MEDINICE)
Ambulatory 23 HR Hot Clinics for IVs and
medical review for ambulatory pt
23 hour unit leads admission
Discharge home oral antibiotics
Patient discharged home
OPD Appointment in PITU/OPATS for
patients with long lines
Finchley Memorial community infusion
hub for review and IV
Patient discharged home,
+ /-PACE +/- PITU OPATS
PACE for non-ambulatory patient
and needs IV antibiotics for up to 7 days but not admission
Does pt needs
Admission
NO
Patient admitted to MAU
Patient admitted to a Base Ward
YES
The A&E/23hr clinical redesign team have designed an integrated cellulitis pathway supported by a simple treatment algorithm to reduce variation in clinical practice.

Next Steps for the Royal Free (2)
•Extend the PACE &TREAT model for other specialities & our newly merged Trust
• PACE delirium/dementia
• PACE surgical (colorectal and vascular)
• PACE specialist services (infectious diseases)
• PACE rehabilitation
• PACE renal medicine
• Use of voluntary services to follow up PACE discharge
• Build an integrated IT system to provide real-time patient information
• Robust training programme established focusing on practical skills & acute
medical problems
• Create joint primary (GPs) & secondary care appointments
• Marketing - conduct regular workshops & GP forums to create awareness
• Evaluation, research & consultancy
• 7-DAY WORKING

oDrop in to meet & talk to specialist nurses
oAsk questions about policies & practices
oFind out more about competencies
oSupport your PREP requirements
Many specialist nursing teams will be available on the day:Infection control Stoma nurses Medical electronicsNursing directorate Dementia nurse consultant Palliative careUrology nurses Continence nurses Diabetes nursesBlood transfusion & many, many more....
oPractice your clinical skills
oCheck your knowledge & skills
oSeek advice and support
oPick up some literature
More information to follow...
7. Summary & Conclusions

Integrated Care - Summary & Conclusions
Clinical Champions &
Strong OperationalManagement
& Governance
Communications &
Marketing
EliminateService
silos
Education &
Training
Years
Good patient outcome
Enhanced patient
experience
Avoidance of
inappropriate or
unnecessary hospital
based activities
Value for money
Value
Making integrated health care system works take years not months. The true
value of the new Integrated Health Care System is about developing
partnerships and new ways of working, delivering good patient outcome
and value for money in the long term.
Integrated IT
System
Data Analysis
& Research
This takes years and
subject to evolution!
A champion is essential

LEARNING POINTS
• Champions – Grow your own and clone them !
• Marketing
• Educate – Work alongside
• Learn from the best
• Spot the gaps and evolve
• Tough on data / clear on process
• Ask daily – What can be done better? And it
can be done!
• Don’t give up too soon

Thank You
Questions?
Top Related