






Languages
Pages
Legal


Akin Akinc, PhD Alnylam Pharmaceuticals
2014 ASH Annual Meeting
Special Scientific Symposium on RNA Therapeutics in Hematology
RNAi Therapeutics for Hemophilia and
Complement-Related Diseases

RNA Interference (RNAi) A New Class of Innovative Medicines
2
RNAi Therapeutics
Harness natural pathway
» Catalytic mechanism
» Mediated by small interfering
RNA or “siRNA”
Therapeutic gene silencing
» Any gene in genome
» Distinct mechanism of action vs.
other drug classes
» Unique opportunities for
innovative medicines
Clinically validated platform

GalNAc-siRNA Conjugates as RNAi Therapeutics
3
ASGPR
(pH>5)
GalNAc-siRNA
conjugate
Clathrin-coated pit
Clathrin-coated
vesicle
Endosome
Recycling
ASGPR
mRNA
Nucleus
protein
RISC
Asialoglycoprotein Receptor (ASGPR)
Highly expressed in hepatocytes
High rate of uptake
Recycling time ~15 minutes
Conserved across species
GalNAc-siRNA Conjugates (revusiran, ALN-AT3,
ALN-CC5, ALN-PCSsc, other programs) siRNA conjugated to N-acetylgalactosamine (GalNAc)
ligand
Efficient delivery to hepatocytes following subcutaneous administration
“Enhanced stabilization chemistry” (ESC) used with
ALN-AT3, ALN-CC5, ALN-PCSsc, and other programs
» Significantly improved potency and durability compared
with revusiran
GalNAc3

Discovery Development Phase 1 Phase 2 Phase 3
TTR-Mediated Amyloidosis
Hemophilia and Rare Bleeding Disorders
Complement-Mediated Diseases
Hypercholesterolemia
Hepatic Porphyrias
Alpha-1 Antitrypsin Deficiency
Hepatitis B Virus Infection
Beta-Thalassemia/Iron-Overload Disorders
Mixed Hyperlipidemia/Hypertriglyceridemia
Hypertriglyceridemia
Hypertension/Preeclampsia
Primary Hyperoxaluria Type 1
Additional Genetic Medicine/Other Programs
4
Alnylam Development Pipeline
ALN-TTRsc
Patisiran (ALN-TTR02)
ALN-AT3
Standard Template Chemistry (STC)-GalNAc Conjugate (SC)
LNP (IV) Enhanced Stabilization Chemistry (ESC)-GalNAc Conjugate (SC)
Delivery Technology:
ALN-CC5
ALN-PCSsc
ALN-AS1
ALN-AAT
ALN-HBV
ALN-TMP
ALN-ANG
ALN-AC3
ALN-AGT
ALN-GO1

Hemophilia and Complement-Mediated Diseases
5
Why RNAi Therapeutics? RNAi human translation achieved in multiple clinical
programs
GalNAc-siRNA conjugates have solved delivery challenge to liver
Hemophilia and complement-mediated diseases are technical and strategic fit » Significant unmet medical need
» Hepatocyte-expressed, secreted plasma protein targets
» Utilize existing delivery platform
» Well-validated, genetically defined pathways/diseases
» Phase 1 proof-of-concept possible
» Clear and rapid development

Hemophilia and Rare Bleeding Disorders Program Unmet Need and Product Opportunity
6
RNAi to treat hemophilia and rare bleeding
disorders (RBD) Hemophilias are recessive X-linked
monogenic bleeding disorders
» Hemophilia A: loss of function in Factor VIII
– >40,000 Patients in EU/US
» Hemophilia B: loss of function in Factor IX
– ~9,500 Patients in EU/US
Segments of high unmet need remain
» E.g., “Inhibitor” patients1,2 – 2,000 Patients in major markets; up to 6,000 WW
– >15-25 Bleeds/year; >5 in-hospital days/year
– ~$300,000/year avg. cost; up to $1M/year
RBD patients3 » Includes deficiencies in Factors II, V, VII, X, and XI
» ~1,000 patients WW with severe bleeding phenotype
1 WFH 2012 Global Survey; 2 Antunes et al., Haemophilia. 20:65-72 (2014); 3Peyvandi et al., J Thromb Haemost; 10, 615-621 (2012)

AT
FIX
FVIII
Antithrombin and ALN-AT3 Program
7
Antithrombin (AT) is genetically defined
target AT is key natural anticoagulant
» Inactivates factors Xa and thrombin
» Attenuates thrombin generation
Human AT deficiency associated
with increased thrombin generation
Expressed in liver; circulates in plasma
Co-inheritance of thrombophilic traits in hemophilia Associated with milder bleeding, reduced factor
requirements, fewer complications
Includes heterozygous
» Antithrombin deficiency
» Factor VLeiden
» Protein C deficiency
» Protein S deficiency
Kurnik et al., Haematologica; 92:982-5 (2007); Ettingshausen et al., Thromb Haemost; 85:218-20 (2001);
Negrier et al., Blood; 81:690-5 (1993); Shetty et al., Br J Haematol; 138:541-4 (2007)
FVIIIa
FVIIa FVII
FIXa
FVa FV
FX
FXa
Fibrinogen Fibrin
Thrombin Prothrombin
Blood clot
Intrinsic system Extrinsic system
Hemophilia A
Hemophilia B
FIX
FVIII
AT
ALN-AT3 in clinical development ESC-GalNAc-siRNA for SC dosing
Positive top-line SAD Phase 1 results
Orphan drug status in US and EU (HA/HB)
Phase 1 MAD study in patients ongoing

Antithrombin Depletion Increases Thrombin
Generation in Hemophilia Plasma
8
Antithrombin depletion increases peak height and delays inhibition of thrombin
HB Donor Plasma HA Donor Plasma
0
20
40
60
80
100
120
140
0 10 20 30 40 50 60
Time (min)
Th
rom
bin
(n
M)
FVIII=100%, AT=100%
FVIII<1%, AT=100%
FVIII<1%, AT=60%
FVIII<1%, AT=40%
FVIII<1%, AT=20%
FVIII<1%, AT=10%
FVIII<1%, AT=0%
0 10 20 30 40 50 60
FIX=100%, AT=100%
FIX<1%, AT=100%
FIX<1%, AT=60%
FIX<1%, AT=40%
FIX<1%, AT=20%
FIX<1%, AT=10%
FIX<1%, AT=0%
Time (min)
Th
rom
bin
(n
M)
0
50
100
150
200

WT
HA + PBS
HA + 1 mg/kg
HA + 30 mg/kg
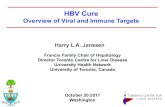
ALN-AT3 Improves Hemostasis Microvessel Laser Injury Model (HA Mice)
Deposition of Platelets
Akinc, ISTH, July 2013; In collaboration with Dr. Lacra Ivanciu and Dr. Rodney Camire
Group Animals (N) Injuries (N) Stable Thrombus (N) Percent AT mRNA in liver
WT 5 25 25 100%
HA + PBS 5 25 0 100%
HA + 1 mg/kg ALN-AT3 5 25 25 50%
HA + 30 mg/kg ALN-AT3 6 30 30 5%
0 30 60 90 120 160 180
0
100
200
300
400
500
Pla
tele
ts A
rea
(m
icro
ns
2)
Time (sec)
9
0
100
200
300
Time (sec)
Fib
rin
Are
a (
mic
ron
s2)
0 30 60 90 120 160 180
WT
HA + PBS
HA + 1 mg/kg
HA + 30 mg/kg
HA + 100U/kg Advate
Deposition of Fibrin
HA + 100U/kg Advate

ALN-AT3 Improves Hemostasis Saphenous Vein Bleeding Model (HA Mice)
Saphenous vein bleeding model adapted from Whinna1
Saphenous vein exposed and transected to initiate bleeding
Thirty seconds after cessation of blood loss, clot dislodged to re-initiate bleeding
Number of hemostatic events in 30 min observation period recorded
Protocol details2 Treated animals received single SC
dose of ALN-AT3 to yield ~70% AT knockdown at time of model initiation
Control animals received 25 IU/kg Advate via IV administration 15 min prior to model initiation
N = 8 N = 15 N = 6 N = 9
p < 0.0001
Akinc, WFH 2014; 1Buyue et al., Blood; 112:3234-3241 (2008); 2In collaboration with Dr. Brian Cooley 10
0
5
10
15
20
-- Saline ALN-AT3 Advate
25 IU/kg
WT HA
Nu
mb
er
of
He
mo
sta
tic
Ev
en
ts
~70%
AT
KD

ALN-AT3 Single-Dose Pharmacology in NHP AT Silencing Leads to Increased Thrombin Generation
11
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
-14 0 14 28 42 56
Re
lati
ve
Se
rum
AT
Le
ve
ls
(Pre
-do
se
=1
)
Days
30 mg/kg 10 mg/kg 3 mg/kg 1 mg/kg
ASH, Dec 2012
ED50 for ALN-AT3 is ~1 mg/kg
Nadir for AT level ~Day 14
Fo
ld C
ha
ng
e P
ea
k T
hro
mb
in
% Antithrombin Knockdown
0.0
1.0
2.0
3.0
4.0
0 20 40 60 80 100
Experimental data
Computer-simulated model results

ALN-AT3 Repeat-Dose Pharmacology in NHP Monthly, SC Dosing
12
Animals: Cynomolgus monkeys (N=3 per group)
Dose levels: 0.5, 1 mg/kg, and 2 mg/kg (SC, monthly dosing)
# Dosing suspended in 2 mg/kg group after 3 doses due to AT levels <20%
0.0
0.2
0.4
0.6
0.8
1.0
1.2
-20 0 20 40 60 80 100 120
Re
lative
Pla
sm
a A
T
(Pre
-do
se
=1
)
Days
0.5 mg/kg 1 mg/kg 2 mg/kg
ALN-AT3 Treatment Groups
#

ALN-AT3 Treatment Normalizes Thrombin
Generation in Hemophilic NHPs with Inhibitors
13
Induction of Hemophilia A
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
Saline 0.25 0.50
Re
lati
ve
FV
III L
ev
els
Pre Ab 4 hr Post Ab
ALN-AT3 (mg/kg) qw
<0.01 <0.01 <0.01
Normalization of Thrombin Generation†
Pre-dose Saline 0.25 0.50
Normal Induced HA
Pe
ak
Th
rom
bin
(n
M)
0
20
40
60
80
100
120
140
ALN-AT3 (mg/kg) qw
60%
AT reduction
80%
AT reduction
†similar results obtained by ETP (p<0.01 at 0.50 mg/kg)
** (p<0.01)
ISTH, July 2013

ALN-AT3 Survival Benefit in HA Mice Results from 26-Week GLP Chronic Toxicity Study
14
Groups
Animals: Hemophilia A (HA) mice (B6;129S4-F8tm1Kaz)
Dosing: Saline, 10 mg/kg, and 30 mg/kg (SC, weekly dosing)
Group sizes: (N=70; 35 per sex) powered to account for spontaneous loss due to background
sensitivity of HA mouse strain
Interim results (through Week 25):
No adverse clinical signs; no changes in body weight, hematology or clinical chemistry
Survival benefit noted in treated animals (p <0.0001; Log-rank, Mantel-Cox test)
Survival of HA Mice
Days
0 50 100 150 200
0
50
100
% S
urv
ival
Saline
10 mg/kg ALN-AT3
30 mg/kg ALN-AT3
ALN-AT3 Treatment Groups

ALN-AT3 Phase 1 Study Dose-escalation Study in Two Parts
Study Design Randomized, single-blinded,
placebo-controlled SAD study in
healthy volunteers
Primary Objective Safety and tolerability of single
doses with AT knockdown <40%
Secondary Objectives Assess clinical activity
» AT knockdown
Study Design Open-label, MAD study in
subjects with moderate to severe
hemophilia A or B (N=up to 18)
Primary Objective Safety and tolerability of multi-
dose in hemophilia subjects
Secondary Objectives Assess clinical activity
» AT knockdown
» Increase in thrombin generation
Part
A Part
B
15
See Sorensen, Oral Abstract 0693;
322. Disorders of Coagulation or Fibrinolysis: Novel Hemostatic
Therapies and Assays; Mon Dec 08 6:45-7:00PM.

Complement Disease Program Unmet Need and Program Opportunity
Complement-Mediated Diseases Excessive complement activity drives disease
pathophysiology in many indications
» Paroxysmal nocturnal hemoglobinuria (PNH)
» Atypical hemolytic uremic syndrome (aHUS)
» Neuromyelitis optica (NMO)
» Myasthenia gravis
» Many others
SolirisTM (eculizumab) is blockbuster drug
» >$1.5B in reported 2013 sales
» >$2.0B in forecasted 2014 revenue
New therapeutic options needed Consistent level of efficacy
SC delivery for more tolerable treatment regimen
Reduce access barriers to treatment
16

17
Complement C5 and ALN-CC5 Program
Complement C5 is genetically validated target Key component of terminal pathway
» C5 cleavage releases C5a; initiates membrane
attack complex (MAC) formation
C5 deficiency associated with minimal
complications » Susceptibility to increased Neisserial infections
» Many C5 deficient mouse strains
Majority expressed in liver; circulates in
plasma
Complement C5 is clinically validated target Eculizumab is anti-C5 Mab
Approved in PNH and aHUS » In PNH, >80% inhibition of hemolytic activity
associated with clinical benefit1
Potential advantages of synthesis inhibition
vs. protein binding approach
ALN-CC5 CTA filed ESC-GalNAc-siRNA for SC dosing
Efficacy in pre-clinical animal models
CTA filed; initial data mid ’15
Initiation
C3 Convertase
C5 Convertase
Terminal Pathway
Factor B
Alternative Pathway Classical Pathway Lectin Pathway
C3 C1
C3 C4 and C2
C3b
C3bBb C4bC2a
C3a Opsonization
Inflammation C3bBbC3b C4bC2aC3b
C5 C5a
C5b
Membrane attack complex (MAC)
C5b-C9
ALN-CC5
1Hillmen et al., NEJM; 350:552-9 (2004)
See Borodovsky Poster Abstract 1606;
508. Bone Marrow Failure: Poster I; Sat Dec 06 5:30-7:30

Robust and Sustained C5 Knockdown in NHP
18
Robust knockdown of serum C5 with SC dosing in NHP for >7 months
Q2W Regimen: Every other week dosing (5 mg/kg, qw x 8, q2w thereafter)
QM Regimen: Every month dosing (5 mg/kg, qd x 5, qw x 8, 10 mg/kg qm thereafter)
2xW Regimen: 5 mg/kg 2xw x 8
Up to 99.2% knockdown of serum C5
98.4 ±0.7% knockdown as group average
Low inter-animal variation
Q2W Regimen provides optimal C5 knockdown results in NHP
» Expect QM dosing regimen in humans based on translation of ESC-GalNAc-siRNA conjugates
Serum C5
Q2W and QM Regimens
2xW Regimen Days 0 20 40 60 80 100 120 140 160 180 200 220
-20
0
20
40
60
80
100
2xw q2w qm
Days
%C
5 K
no
ck
do
wn
(N
orm
ali
ze
d t
o P
re-b
lee
d)
Individuals (Q2W and QM)
60 80 100 120 140 160 180 200 220
60
70
80
90
100
NHP3
NHP2
NHP1
NHP4
NHP5
NHP6
%C
5 K
no
ck
do
wn
(N
orm
alize
d t
o P
re-b
lee
d)

Both Classical and Alternative Pathways Strongly
Inhibited
19
Up to 96.9% inhibition of alternative pathway (CAP) activity (mean 95.1±0.93%), and up to
96.2% inhibition of hemolysis (mean 88.0±6.1%)
» Q2W Regimen provides optimal inhibition of complement activity in NHP but monthly likely in humans
based on translation of ESC-GalNAc conjugates
In line with results observed in published reports on eculizumab
Days 0 20 40 60 80 100 120 140 160 180 200 220
0
20
40
60
80
100
CAP Hemolysis
Complement Activity (Q2W)
Days 0 20 40 60 80 100 120 140 160 180 200 220
0
20
40
60
80
100
Complement Activity (QM)
%A
cti
vit
y o
r h
em
oly
sis
re
du
cti
on
QM Regimen
%A
cti
vit
y o
r h
em
oly
sis
re
du
cti
on
CAP Hemolysis
Q2W Regimen

C5 Knockdown Reduces Proteinuria
Rat Membranous Nephropathy Model
20
D4 D-10
Anti-Fx1A
C5 siRNA
D-7 D-3 D1 D5 D0
Urine
D-2
Urine
CVF
~90% reduction in urinary albumin levels with C5 knockdown in rat model of Passive Heymann Nephritis (PHN) Nephritis induced by injection of sheep anti-rat kidney fraction antiserum (anti-Fx1A)
» Cobra venom factor (CVF) treated rats receive daily injections
Similar reduction in urinary albumin excretion to CVF complement depletion
Urinary Albumin
a Fx1a only CVF C5 siRNA 0
2
4
6
8
10
12
U r i
n a
r y A
L B
( m
g / 2
4 h
r s ) Day -2
Day 5/6
Hemolytic Activity
a Fx1a only CVF C5 siRNA 0
20
40
60
80
100
% H
e m
o l y
s i s
Pre-dose Day 6

Glomerular MAC Deposition is Prevented with C5
Silencing
No glomerular C5b-9 deposition with C5 siRNA or CVF treatment Equivalent glomerular sheep IgG deposition regardless of
treatment, as expected
αFx1a alone C5 siRNA CVF
C5b-9
Sheep
IgG
21

C5 Knockdown Results in Equivalent Activity to Anti-C5 Ab
Mouse CAIA Model
Circulating liver-derived C5 key driver of pathology in mouse CAIA Little or no role for locally produced C5
-4 -2 0 2 4 6 8 10
0
2
4
6
8
10
12
Day
Maximal CDA score = 12 Anti-C5 Ab – BB5.1
PBS (N=7)
Anti-C5 Ab (50 mg/kg, N=7)
siRNA-Ctr (10 mg/kg, N=6)
siRNA-C5 (5 mg/kg, N=7)
Clin
ica
l Dis
ea
se
Ac
tiv
ity
D0 D3 D5 D10 D-5
Col Ab LPS
siRNA C5
Anti-C5 Ab
Disease Activity
22

ALN-CC5 Phase 1 Study
23
ALN-CC5 CTA filed
Phase 1/2 study expected to start in early ’15; Initial data
expected in mid ’15
ALN-CC5 with SC dosing
Parts A/B: SAD/MAD in up to 60 normal healthy volunteers
» Randomized, double-blind, placebo-controlled study
» Assess safety, tolerability, PK/PD, and clinical activity
Part C: Multi-dose in up to 8 PNH patients
» Open-label study
» Assess safety, tolerability, PK/PD, clinical activity, and LDH reduction

Summary
24
RNAi therapeutics continue to progress in clinical trials
ALN-AT3 and ALN-CC5 are Alnylam’s first programs in hemophilia and complement-mediated disease, respectively » Robust AT and C5 target knockdown observed with
monthly SC dosing in NHPs
» Pharmacodynamic activity observed in multiple preclinical models
ALN-AT3 currently in Phase 1 in hemophilia patients, and ALN-CC5 will be in Phase 1/2 in early 2015

Thank You
Top Related