






Languages
Pages
Legal

Respiratory FailureRespiratory Failure

Respiration external respiration ( pulmonary ventilation and g
as exchange in lung) transport of gas
internal respiration
1.1. respiratory insufficiencyrespiratory insufficiency
The condition in which the lungs can not take in The condition in which the lungs can not take in
sufficient oxygen or expel sufficient carbon dioxide to sufficient oxygen or expel sufficient carbon dioxide to
meet the needs of the cells of the body. Also called meet the needs of the cells of the body. Also called
pulmonary insufficiency.pulmonary insufficiency.
Respiratory failure
concept and classification

2. respiratory failure2. respiratory failure
normal reference valuesnormal reference values ::
PaOPaO22 < 60mmHg< 60mmHg (( 8kPa8kPa ))
with or without PaCOwith or without PaCO22 > 50mmHg > 50mmHg (( 6.67kPa6.67kPa ) ) RFI = PaORFI = PaO22/FiO/FiO22 ≤ 300 ≤ 300
Respiratory failure is a syndrome in which the respiratory
system fails in one or both of its gas exchange functions:
oxygenation and carbon dioxide elimination.
In practice, respiratory failure is defined as a PaO2 value
of less than 60 mm Hg while breathing air or a PaCO2 of more than 50 mm Hg.
33 .. classificationclassification
(( 11 )) according to PaCOaccording to PaCO22
■■ hypoxemic (Group )Ⅰ)Ⅰ respiratory failure
a PaO2 of less than 60 mm Hg with a normal or low PaCO2.
Cause of: Edema, Vascular disease, Chest Wall.
■ ■ hypercapnic (Group ) respiratory failureⅡ
a PaO2 low 60 mm Hg and PaCO2 of more than 50 mm Hg.
Cause of: Airway obstruction, Neuromuscular disease.
(( 44 )) according to durationaccording to duration
■ ■ acute respiratory failureacute respiratory failure
■ ■ chronic respiratory failurechronic respiratory failure
(( 33 )) according to primary siteaccording to primary site
■ ■ centralcentral respiratory failurerespiratory failure
■■ peripheral respiratory failureperipheral respiratory failure
(( 22 )) according to pathogenic mechanismaccording to pathogenic mechanism
■ ■ ventilatory disorders ventilatory disorders
■ ■ gas exchange disordersgas exchange disorders

ventilatory disoventilatory disordersrders
gas exchange gas exchange disordersdisorders
respiratory failurerespiratory failure
obstructive ventilatoryobstructive ventilatory
disordersdisorders
restrictive ventilatory restrictive ventilatory
disordersdisorders
etiology and pathogenesisetiology and pathogenesis【【 classification of respiration failure mechanismclassification of respiration failure mechanism 】】
diffu
sion
diso
rders
diffu
sion
diso
rders
ventilatio
n-p
erfusio
nven
tilation
-perfu
sion
mism
atchin
g
mism
atchin
g

Ⅰ. ventilatory disorders
1. restrictive ventilatory disorders1. restrictive ventilatory disorders
Restrictive hypoventilation is caused by the diseases that affect tRestrictive hypoventilation is caused by the diseases that affect the distensibility of the alveolarhe distensibility of the alveolar..

Respiratory movement
forced breathing
Respiratory Respiratory
movementmovement
disorderdisorder
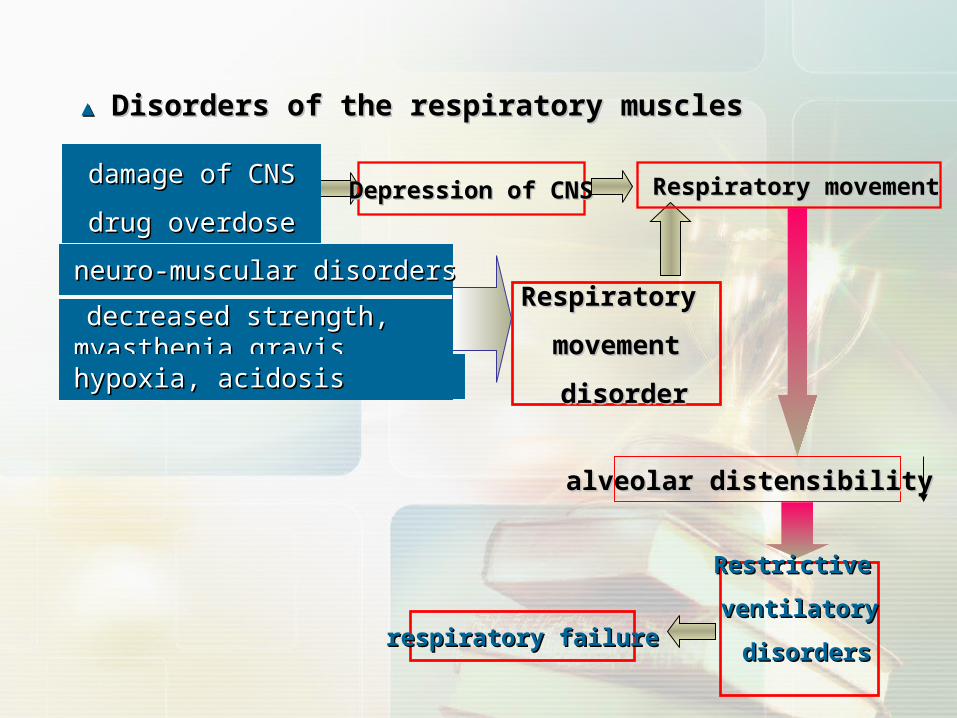
neuro-muscular disordersneuro-muscular disorders
decreased strength, myasdecreased strength, myasthenia gravisthenia gravishypoxia, acidosishypoxia, acidosis
Respiratory movement ↓Respiratory movement ↓Depression of CNSDepression of CNSdamage of CNSdamage of CNS
drug overdosedrug overdose
▲▲ Disorders of the respiratory muscles Disorders of the respiratory muscles
alveolar distensibility alveolar distensibility
Restrictive Restrictive
ventilatoryventilatory
disordersdisordersrespiratory failurerespiratory failure

●● decrease of pulmonary surfactantsdecrease of pulmonary surfactants and increase of and increase of
surface tension forcesurface tension force
●● diffuse interstitial fibrosisdiffuse interstitial fibrosis
▲ decreased lung compliancedecreased lung compliance
▲ decreased thoracic compliance of lung decreased thoracic compliance of lung
deformity of thorax , fracture of several ribs, tension deformity of thorax , fracture of several ribs, tension
pneumothorax, thickened constrictive pleural layer. pneumothorax, thickened constrictive pleural layer.
2. obstructive ventilatory disorders
■ obstructive ventilatory disorders are caused by the diseases which share the common characterestic of causing enough narrowing within the
tracheobronchial tree to increase resistance to the flow of air.
原因和机制原因和机制
■ etiologyetiology
asthma, emphysema, chronic bronchitis, and bronchiectasis.

■Obstruction is located in the
airway inside the thorax : expiratory dysnea
■Obstruction is located in the
airway outside the thorax : inspiratory dysnea
11 ) ) central airway obstructioncentral airway obstruction
defined as airway obstruction between the glottis and the carinadefined as airway obstruction between the glottis and the carina
+
expire inspire
three depression sign

22 ) ) peripheral airway obstructionperipheral airway obstruction
smaller airways less than 2 mm in diameter.smaller airways less than 2 mm in diameter.
equal pressure point (EPequal pressure point (EPP)P)In forced expiration, the point where intraIn forced expiration, the point where intrapleural pressure and alveolar pressure apleural pressure and alveolar pressure are equal. re equal.
Determinants of airway closure are the intrinsic caliber of peripheral airDeterminants of airway closure are the intrinsic caliber of peripheral airways.ways.
Smooth muscle tone, thickness of the wall, Smooth muscle tone, thickness of the wall,
mechanical properties of the surface film, mechanical properties of the surface film,
and secretions in the lumen ,bingding and secretions in the lumen ,bingding
effect of attachments of the surroundingeffect of attachments of the surrounding
lung parenchyma.lung parenchyma.
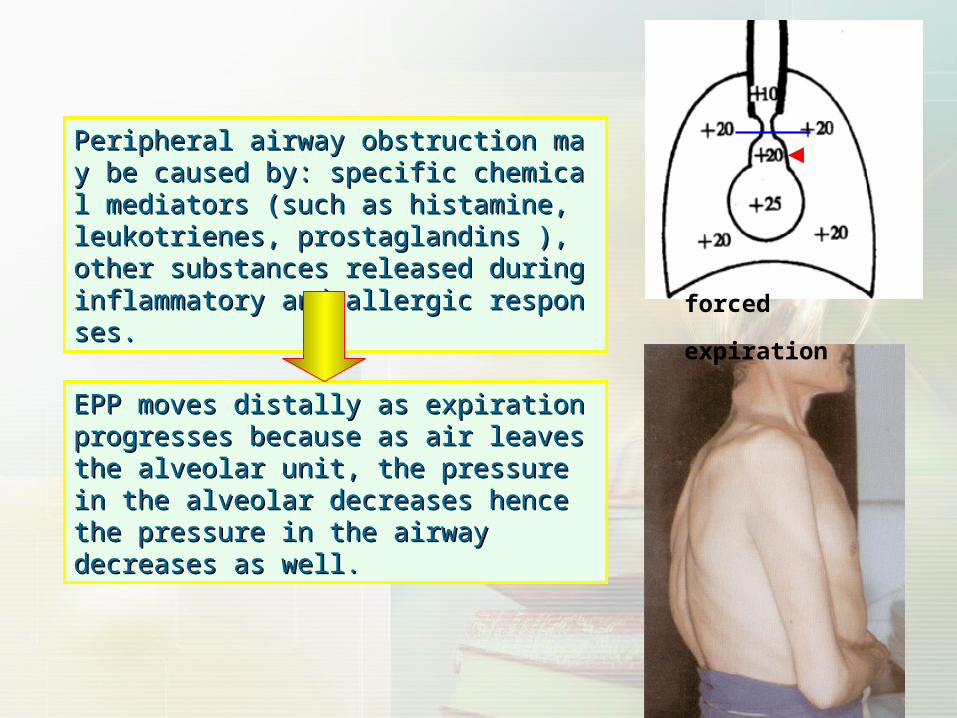
EPP moves distally as expiration EPP moves distally as expiration progresses because as air leaves the progresses because as air leaves the alveolar unit, the pressure in the alveolar unit, the pressure in the alveolar decreases hence the pressure alveolar decreases hence the pressure in the airway decreases as well.in the airway decreases as well.
Peripheral airway obstruction may be cauPeripheral airway obstruction may be caused by: specific chemical mediators (such sed by: specific chemical mediators (such as histamine, leukotrienes, prostaglandinas histamine, leukotrienes, prostaglandins ), other substances released during inflas ), other substances released during inflammatory and allergic responses.mmatory and allergic responses.
forced expiration
11 )) Low PaOLow PaO22 : : PaOPaO22 < 60mmHg < 60mmHg
22 )) PaCOPaCO2 2 changechange ::
A. hypoventilationA. hypoventilation :: high PaCOhigh PaCO2.2.
R=40/50 mmHg=0.8R=40/50 mmHg=0.8 ;;
B. part hypoventilation: Low PaOB. part hypoventilation: Low PaO2 2 and normal or low PaCO and normal or low PaCO22..
3. The alteration of blood gas 3. The alteration of blood gas
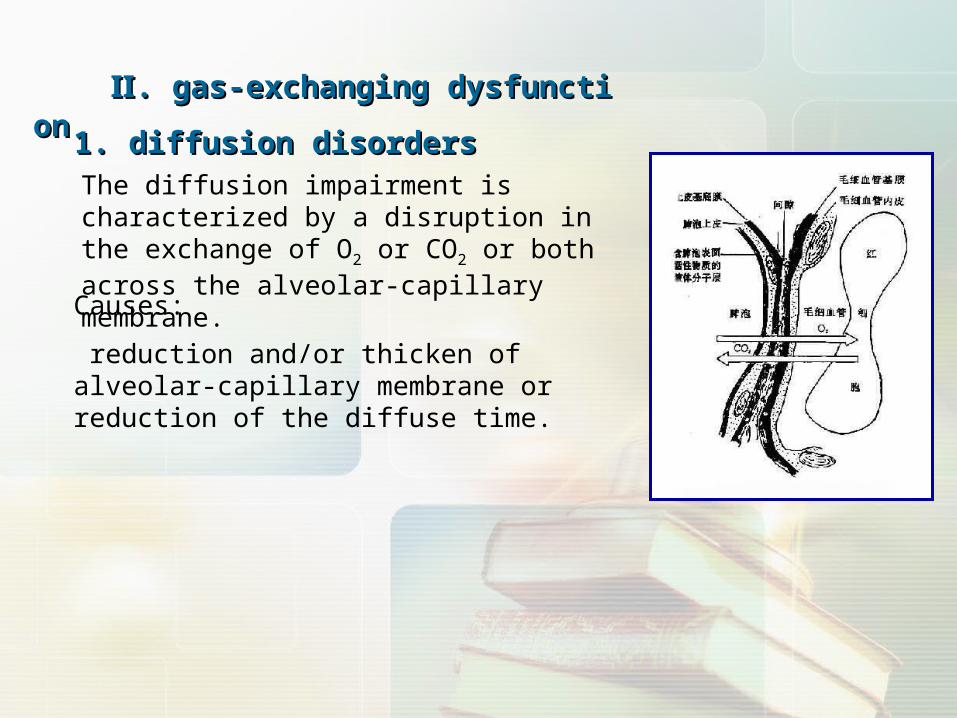
ⅡⅡ. gas-exchanging dysfunction. gas-exchanging dysfunction
1. diffusion disorders1. diffusion disordersThe diffusion impairment is characterized by a disruption in the exchange of O2 or CO2 or both across the alveolar-capillary membrane.
Causes:
reduction and/or thicken of alveolar-capillary membrane or reduction of the diffuse time.

11 ) ) etiology of diffusion disordersetiology of diffusion disorders
■ ■ reduction of diffusion membrane areareduction of diffusion membrane area
Abnormalities of diffusion may not cause arterial hypoxia inAbnormalities of diffusion may not cause arterial hypoxia in
persons at rest unless they are extremely severe.persons at rest unless they are extremely severe.
(total: 80 mm(total: 80 mm2; 2; at rest: 30~40 mmat rest: 30~40 mm22))
Causes: emphysema, pneumonia, lobectomyCauses: emphysema, pneumonia, lobectomy
■ increase of diffusion membrane thicknessincrease of diffusion membrane thickness
edema, fibrosis, capillary vessel dilatation edema, fibrosis, capillary vessel dilatation
■ decreased time of blood contacts with alveolardecreased time of blood contacts with alveolar
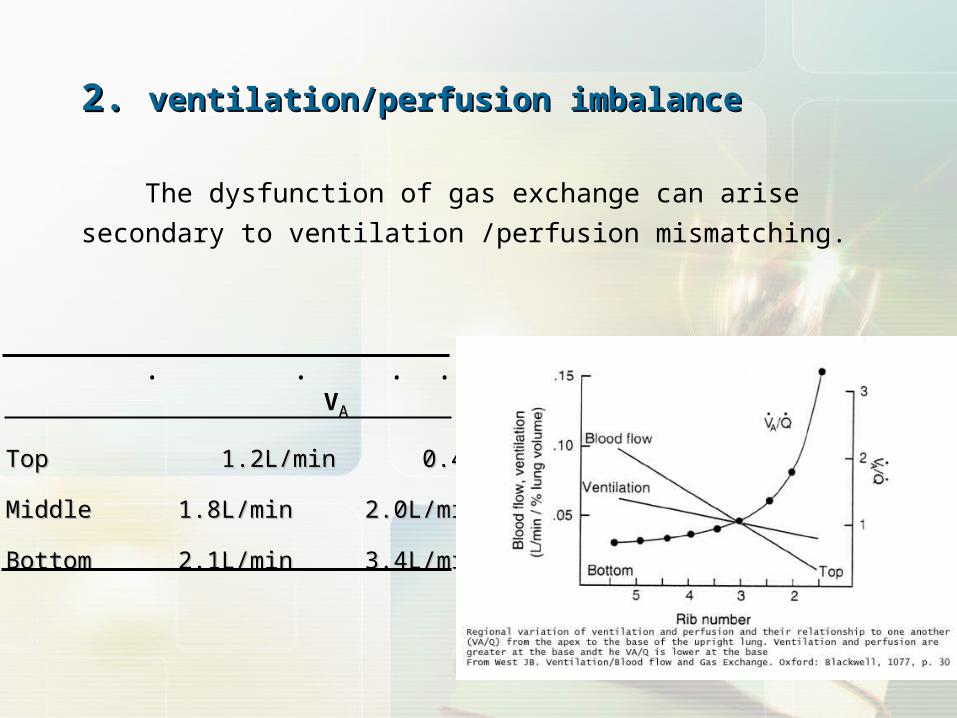
VAA Q VAA/ Q
Top Top 1.2L/min 0.4L/min 3.01.2L/min 0.4L/min 3.0
Middle 1.8L/min 2.0L/min 0.9Middle 1.8L/min 2.0L/min 0.9
Bottom 2.1L/min 3.4L/min 0.6Bottom 2.1L/min 3.4L/min 0.6
· · · ·
2. 2. ventilation/perfusion imbalanceventilation/perfusion imbalance
The dysfunction of gas exchange can arise secondary to ventilation
/perfusion mismatching.
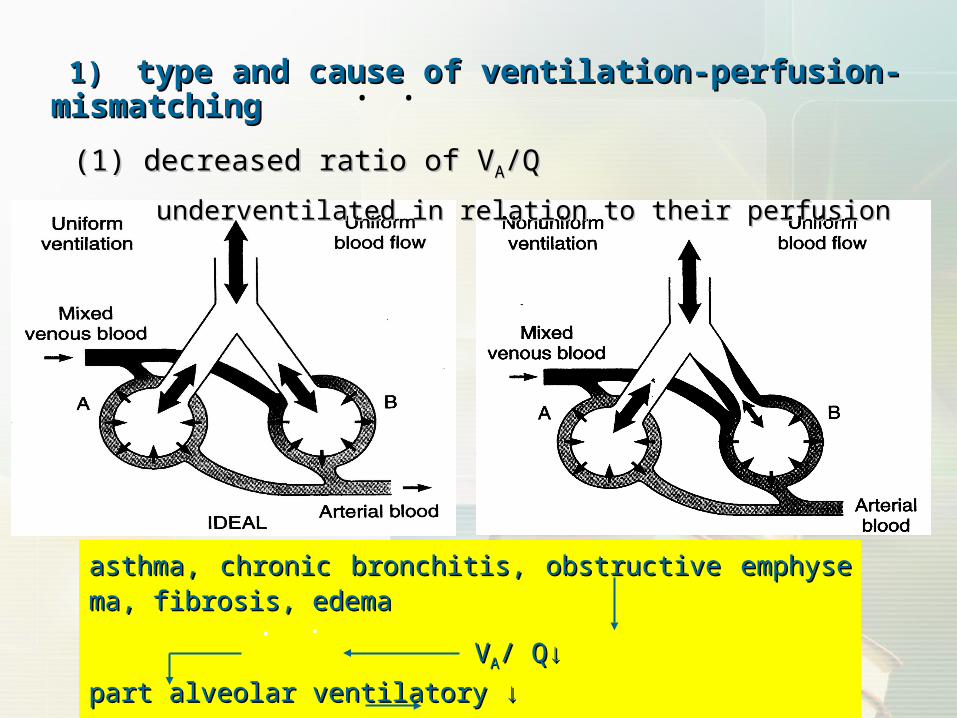
asthma, chronic bronchitis, obstructive emphysema, fibrosis, edasthma, chronic bronchitis, obstructive emphysema, fibrosis, edemaema
VVAA/ Q/ Q↓ ↓ part alveolar ventilatory ↓ part alveolar ventilatory ↓
functional shunt↑functional shunt↑>30% respiratory failure>30% respiratory failure
· ·
1)1) type and cause of ventilation-perfusion-mismatchingtype and cause of ventilation-perfusion-mismatching
(1) (1) decreaseddecreased ratio of Vratio of VAA/Q/Q
underventilated in relation to their perfusionunderventilated in relation to their perfusion
··

(2) (2) increased ratio of Vincreased ratio of VAA/Q /Q
poor perfusion in relation to their ventilation with airpoor perfusion in relation to their ventilation with air
··
pulmonary artery embolization, pulmonary artery embolization, DIC in lungDIC in lung, vessels contract, , vessels contract, pulmonary pulmonary
aarteritisrteritis, ,
dead space like ventilation dead space like ventilation V VAA/Q/Q↑ poor perfusion↓↑ poor perfusion↓
respiratory failurerespiratory failure
· ·
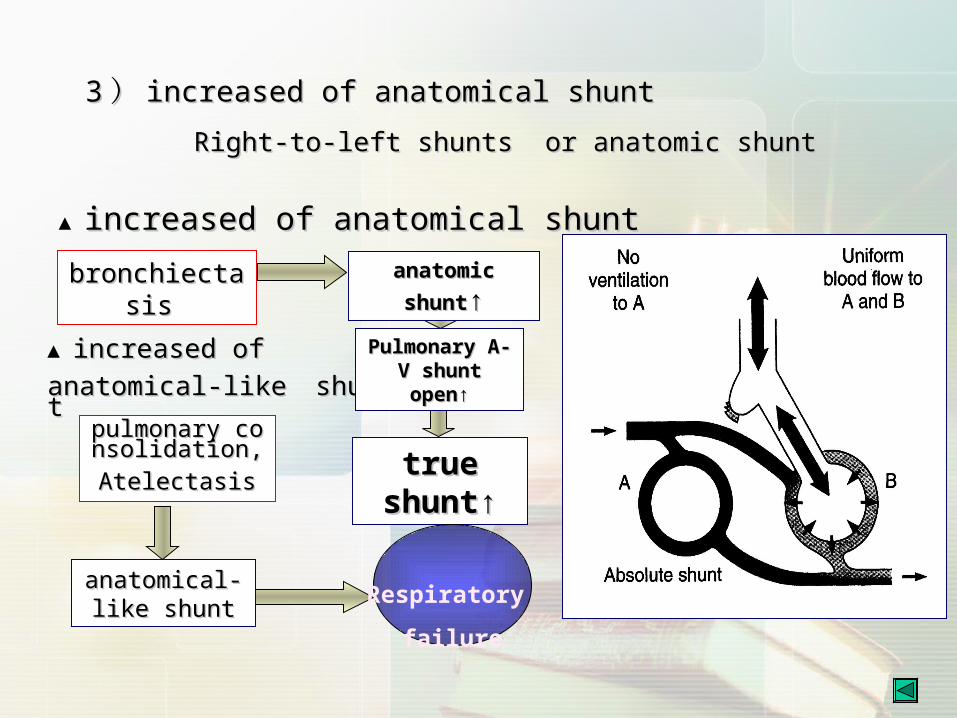
pulmonary conpulmonary consolidation,Atelesolidation,Atele
ctasisctasis
anatomical-anatomical-like shuntlike shunt
▲ increased of increased of anatomical-like shuntanatomical-like shunt
bronchiectasibronchiectasis s
anatomic shuntanatomic shunt↑↑
Pulmonary A-V Pulmonary A-V shunt open↑shunt open↑
true true shunt↑shunt↑
Respiratory
failure
▲ increased of anatomical shuntincreased of anatomical shunt
33 )) increased of anatomical shuntincreased of anatomical shunt
Right-to-left shunts or anatomic shuntRight-to-left shunts or anatomic shunt
ⅢⅢ. Acute respiratory distress syndrome. Acute respiratory distress syndrome (( ARDSARDS))
[concept][concept]
ARDS is a clinical description of severe lung injury characteriARDS is a clinical description of severe lung injury characteri
zed by increased permeability of alveolar-capillary membranezed by increased permeability of alveolar-capillary membrane
s, development of protein-rich pulmonary edema, marked hyps, development of protein-rich pulmonary edema, marked hyp
oxemia refractory to increase in inspired oxygen concentratiooxemia refractory to increase in inspired oxygen concentratio
n, and the absence of left ventricular failure.n, and the absence of left ventricular failure.

[etiology][etiology]
shock from any cause, shock from any cause,
multisystem trauma, multisystem trauma,
infection including bacterial and nonbacterial pneumonia, infection including bacterial and nonbacterial pneumonia,
inhaled toxic substances, inhaled toxic substances,
overdose of some drug, overdose of some drug,
acute pancreatitis.acute pancreatitis.
11.. direct injury of damage factordirect injury of damage factor
22.. indirect injury of inflammation mediumindirect injury of inflammation medium
[ [ pathogenesis of ARDS]pathogenesis of ARDS]

[Mechanisms of respiratory failure][Mechanisms of respiratory failure]
1. 1. diffusion disordersdiffusion disorders
damage of alveolar-capillary membrane increased permeabilitydamage of alveolar-capillary membrane increased permeability
diffusion disordersdiffusion disorders
ARDSARDS
2. ventilatory disorders2. ventilatory disorders
▲edema, type alveolar epithelial cells damage decreased lung volumeⅡedema, type alveolar epithelial cells damage decreased lung volumeⅡ
airway obstruction obstructive ventilatory restrictive ventilatory airway obstruction obstructive ventilatory restrictive ventilatory
disorders disordersdisorders disorders
▲inflammation mediuminflammation medium bronchia spasmbronchia spasm respiratory failurerespiratory failure
33.. VVAA/Q /Q mismatchingmismatching• •
Effects of respiratory failureEffects of respiratory failure
1.1. Acid-base disturbances & disorders of electrolyte balanceAcid-base disturbances & disorders of electrolyte balance
2.2. Alteration of the respiratory systemAlteration of the respiratory system
peripheral chemoreceptorperipheral chemoreceptor
■■ PaPaOO22↓↓ << 60mmHg60mmHg respiratory center(+) respiratory movement↑respiratory center(+) respiratory movement↑
<< 30mmHg respiratory center (-) respiratory movement ↓30mmHg respiratory center (-) respiratory movement ↓
■■ PaCO2↑ central chemoreceptor (+) respiratory movement↑PaCO2↑ central chemoreceptor (+) respiratory movement↑
>> 80mmHg respiratory center (-) respiratory movement ↓80mmHg respiratory center (-) respiratory movement ↓

3. Alteration of the respiratory system3. Alteration of the respiratory system
■ compensatory reactioncompensatory reaction
PaOPaO22<60 mmHg<60 mmHg ,, PaCOPaCO2 2 increase cardiovascular center(+)increase cardiovascular center(+)
increase in cardiac output : increase in stroke volume and heart ratincrease in cardiac output : increase in stroke volume and heart rat
ee
redistribution of blood flowredistribution of blood flow■ injurious changesinjurious changes
PaOPaO22< 40 mmHg< 40 mmHg ,, PaCOPaCO22> 80 mmHg cardiovascular center> 80 mmHg cardiovascular center
(-)(-)
rate slow, decreased blood pressure rate slow, decreased blood pressure
cardiac output decrease cardiac output decrease
pulmonary hypertension pulmonary hypertension

■■difficulty breathing difficulty breathing Restricted diastolicRestricted diastolic
■ co pulmonaleco pulmonale
■■pulmonary arterial embolism, capillary damagpulmonary arterial embolism, capillary damagee
co pulmonaleco pulmonale
afterload to right ventricleafterload to right ventricle↑↑
chronic pulmonary chronic pulmonary hypertensionhypertension
Pulmonary vascular Pulmonary vascular
wall wall
thickening and thickening and
hardeninghardening
■■PaOPaO22↓↓
blood resistanceblood resistance↑↑
pulmonary pulmonary vasoconstrictiovasoconstrictio
nn
RBC↑ blood viscosity RBC↑ blood viscosity ↑↑
StenosisStenosis
■■ Hypoxia, acidosis myocardial systolic Hypoxia, acidosis myocardial systolic and diastolic function(-) and diastolic function(-)

(2) Hypercapnia: CO(2) Hypercapnia: CO22 nacosis. nacosis.
a condition of confusion, tremors, convulsions, and possible coma a condition of confusion, tremors, convulsions, and possible coma
that that
may occur if blood levels of carbon dioxide increase to 80 mm Hg or may occur if blood levels of carbon dioxide increase to 80 mm Hg or
higher. higher.
(1) Hypoxia: the nervous system is very sensible to oxygen lack.(1) Hypoxia: the nervous system is very sensible to oxygen lack.
< 40~50 mmHg, serious but reversible deterioration in cerebral < 40~50 mmHg, serious but reversible deterioration in cerebral function function
( orientation, arithmetic tasks, memory) occurs, and ( orientation, arithmetic tasks, memory) occurs, and restlessness and restlessness and
confusion are common.confusion are common.
< 30 mmHg, loss of consciousness results.< 30 mmHg, loss of consciousness results.
< 20 mmHg, irreversible damage of neural cells.< 20 mmHg, irreversible damage of neural cells.
功能和代谢功能和代谢
4. Alteration of the nervous system4. Alteration of the nervous system

■ ■ Brain cell injuryBrain cell injury
lysosomal membrane stability↓ lysosomal membrane stability↓ lysosomal enzyme release nerve cell necrosislysosomal enzyme release nerve cell necrosis
GABA↑GABA↑
CSF pH↓CSF pH↓ << 7.25 7.25 EEG slow or stopEEG slow or stop
PaPaCOCO22↑, acidosis↑, acidosis Cerebral vasodilation Cerebral blood flowCerebral vasodilation Cerebral blood flow↑↑
hypoxia hypoxia vascular endothelial damage vascular endothelial damage extracellular brain edemaextracellular brain edema edema on brain cell edema on brain cell Vascular compressionVascular compression
Increased cerebral anoxiaIncreased cerebral anoxia
■ ■ cerebrovascular injurycerebrovascular injury
Intracranial pressureIntracranial pressure↑↑
pulmonary pulmonary encephalopathencephalopath
yy
[pulmonary encephalopathy][pulmonary encephalopathy]

4. Alteration of the renal function4. Alteration of the renal function
5. Alteration of the digestive system5. Alteration of the digestive system

Thanks for attention
Top Related