







Languages
Pages
Legal


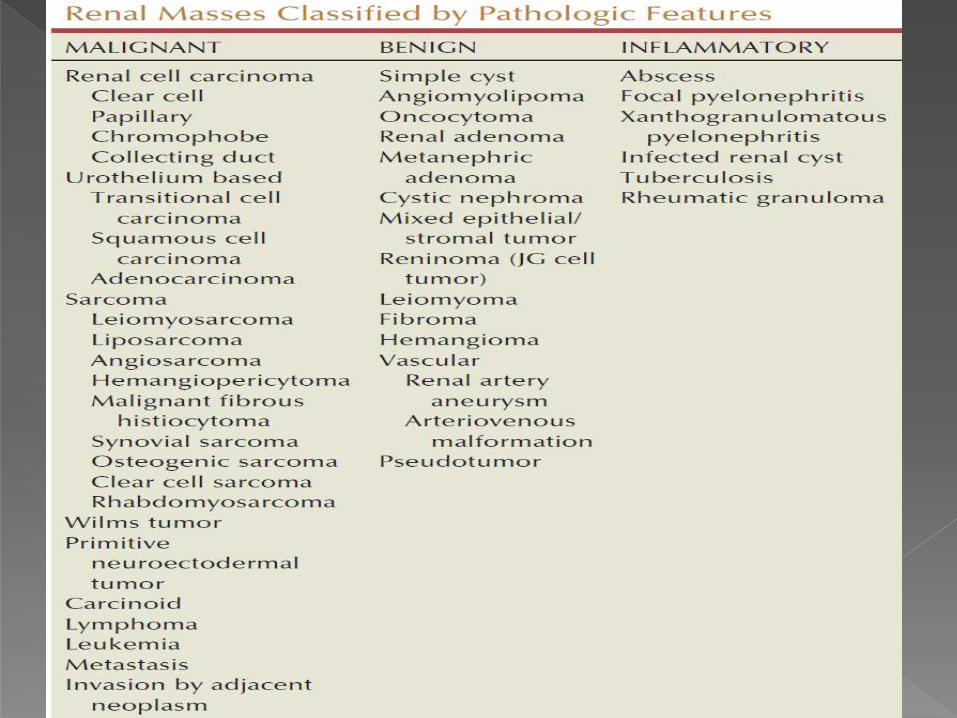

INCIDENCE-2% to 3% of all adult malignant neoplasms.
30% to 40% of patients with RCC have died of their cancer.
Typical presentation in 6th & 7th decade.
Majority are sporadic, only 2% to 3% are familial.
RCCs arise primarily from the proximal convoluted tubules-clear cell and papillary variants.
Chromophobe and Collecting duct RCC-the more distal components of the nephron.

FAMILIAL FACTORS
ENVIRONMENTAL FACTORS

Established
Tobacco exposure
Obesity
Hypertension
Putative
Lead compounds
Various chemicals (e.g., aromatic hydrocarbons)
Trichloroethylene exposure
Occupational exposure (metal, chemical, rubber, and printing
industries)
Asbestos or cadmium exposure
Radiation therapy
Dietary (high fat/protein and low fruits/vegetables)

Potential mechanisms linking obesity to RCC
include lipid peroxidation leading to DNA adducts,
increased insulin-like growth factor-1 expression,
increased circulating estrogen levels, and increased
arterionephrosclerosis and local inflammation.
Hypertension-induced renal injury and inflammation
or metabolic or functional changes in the renal
tubules that may increase susceptibility to
carcinogens.


Familial form of clear cell RCC is von Hippel-Lindau disease. AD
VHL- tumor suppressor gene.
chromosome 3p25-26, role as tumor suppressor gene for both the sporadic and the familial forms of clear cell RCC has been confirmed.
VHL protein ,bind to elongins B and C, CUL-2, and RBX1 to form an E3 ubiquitin ligase complex and thereby modulates the degradation of important regulatory proteins


ORGAN SYSTEM LESION INCIDENCE (%)
Eye Benign retinal angiomas 49-59
CNS Benign hemangioblastomas 42-72
Kidney Clear cell renal cell carcinoma
Renal cysts
24-70
22-59
Adrenal gland Pheochromocytoma 18
Pancreas Islet cell tumors
Malignant islet cell tumor
Pancreatic cysts
12
2
21-72
Epididymis Cystadenoma 10-26
Ear Endolymphatic sac tumor 10

2nd most common,AD trisomy for chromosomes 7
and 17 as well as abnormalities on chromosomes 1,
12, 16, 20, and Y.
HPRCC do not develop tumors in other organ
systems.
CECT is the preferred imaging modality for patients
with HPRCC because it has the greatest sensitivity for
detecting the small, hypovascular lesions that are
common in this syndrome.

Cutaneous and uterine leiomyomas and type 2 papillary RCC.
Around 40’s, unusual for familial RCC in that they are often
solitary and unilateral, and they are more likely to be aggressive
than other forms of familial RCC.
Collecting duct RCC –HLRCC syndrome.
1q42-44, fumarate hydratase gene.
Prompt surgical management is recommended in this syndrome,
given their tendency toward invasive and aggressive behavior in
contrast to other syndromes where conserative Mx is more.

Cutaneous fibrofolliculomas, lung cysts, spontaneous pneumothoraces, and a variety of renal tumors primarily derived from the distal nephron.
Renal tumors typically include chromophobe RCC, oncocytomas, and hybrid or transitional tumors that exhibit features of both of these entities.
B/L & multifocal.
17p12q11.2, folliculin gene

Round to ovoid and circumscribed by a pseudocapsule of
compressed parenchyma and fibrous tissue rather than a true
histologic capsule.
Unlike upper tract transitional cell ca’s, most RCCs are not
grossly infiltrative, with the notable exception of collecting duct
RCC and some sarcomatoid variants.
RCCs consist of yellow, tan, or brown tumor interspersed with
fibrotic, necrotic, or hemorrhagic areas; few are uniform in gross
appearance.
Cystic degeneration is found in 10% to 25% of RCCs and appears
to be associated with a better prognosis compared with purely
solid RCC

The kidney
contains a large
irregular
neoplasm with
a variegated cut
surface. Yellow
areas
correspond to
lipid-containing
cells.


•80-90%
•Islands of neoplastic
cells with abundant
clear cytoplasm.
•specific deletion of
chromosome 3p and
mutation of the VHL
gene.

•10-15%
•Papillary fronds covered
by neoplastic cells.
•type 1 with small cells and
pale cytoplasm and
•type 2 with large cells and
eosinophilic cytoplasm, the
latter having a worse
prognosis.
•Trisomies of
chromosomes 3q, 7, 8, 12,
16, 17, and loss of the y
chromosome.

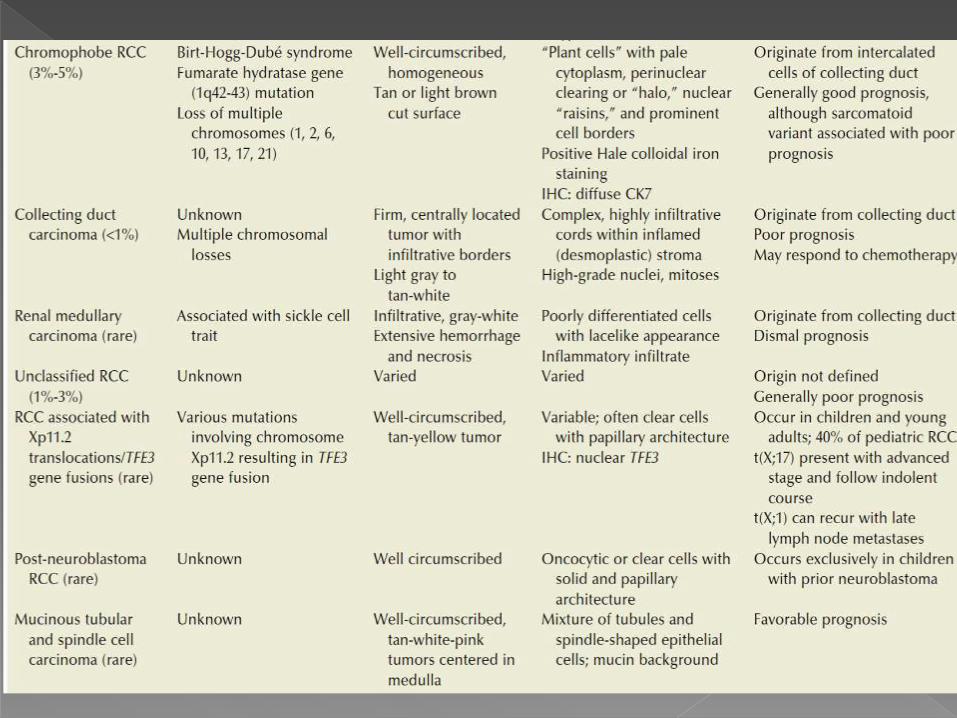
•4-5%
•Photomicrograph
showing pale
acidophilic granular
cells with prominent
cell borders.
•loss of chromosomes
1, 2, 6, 10, 13, and 17.

Local Tumor Growth
Hematuria
Flank pain
Abdominal mass
Obstruction of the Inferior Vena Cava
Bilateral lower extremity edema
Nonreducing or Left-sided varicocele

Paraneoplastic Syndromes-30% of symptomatic
RCC
Hypercalcemia
Hypertension
Polycythemia
Stauffer’s syndrome
Neuromyopathy
Amyloidosis
Elevated erythrocyte sedimentation rate
Anemia

Persistent cough
Bone pain
Cervical lymphadenopathy
Constitutional symptoms
Weight loss/fever/malaise
Hemogram,RFT,LFT,ESR.
CXR
USG
IVP
CT SCAN-INVESTIGATION OF CHOICE.
MRI SCAN
RMB(RENAL MASS BIOPSY)
RENAL ARTERIOGRAPHY
RENAL SCAN

Approx 98% accurate in distinguishing simple cysts from solid lesions.
A renal mass that is not clearly a simple cyst by strict ultrasound criteria should be evaluated further with computed tomography (CT).
USG helpful in suggesting the fat content of an
angiomyolipoma (AML) by its characteristic increased echogenicity

Malignancy on IVP –
1.Calcification within the mass.
2.Increased tissue density,
3.Irregularity of the margin, and
4.Distortion of the collecting system.

Renal mass that enhances with IV administration of contrast material on CT by >15(HU) should be considered an RCC until proved otherwise.
Solid masses that also have substantial areas of negative CT attenuation numbers (< −20 HU) indicative of fat are diagnostic of AMLs.
In 10-20% its indeterminate.
Occassionally, CT demonstrates an enhancing renal segment that is isodense with the remainder of the kidney, suggestive of a renal pseudotumor,which is confirmed by isotope renography with technetium-labeled dimercaptosuccinic acid or glucoheptonate

A, CT scan after administration
of contrast material shows
isodense hilar mass in solitary
right kidney. B, Right renal
arteriography shows no
neovascularity.
C,Glucoheptonate isotope
renal scan shows increased
density of mass indicative of
hypertrophied column of
Bertin.

Alternate to patients who are highly allergic to iodinated
contrast. Using Gadolinium.
Disadvantage-nephrogenic systemic fibrosis (NSF),
which is more common in patients with renal
insufficiency.
Avoid MRI, particularly serial studies, in CKD patients
whenever possible, and to dialyze patients after the study
if severe chronic kidney disease (CKD) is present.

Demonstrate enhancement in renal masses.
Investigate locally advanced malignancy.
Investigate venous involvement if the extent of
an inferior vena cava tumour thrombus is poorly
defined on CT scanning.

The sensitivities of CT for detection of renal venous tumor thrombus and IVC involvement are 78% and 96%, respectively.
MRI is well established as the premier study for the evaluation and staging of IVC tumor thrombus, although recent data suggest that multiplanar CT is likely equivalent.
Venacavography is now best reserved for patients with equivocal MRI or CT findings or for patients who cannot tolerate or have other contraindications to cross-sectional imaging.
Transesophageal echocardiography also appears to be accurate for establishing the cephalad extent of the tumor thrombus, but it is invasive and provides no distinct advantages over MRI or CT in the preoperative setting
Renal mass biopsy-RMB- not recommended routinely.
Accuracy,sensitivity &specitivity hae improved recently,but still it has imperfect NPV <50%
Indications-
1.Suspicion of renal abscess.
2.RCC must be differentiated from metastatic malignant disease.
3. Renal lymphoma.
4. Obtain histology before ablative treatments.
5. To select the most suitable form of targeted pharmacologic therapy in the setting of metastatic disease.


Contrast enhanced USG using microbubbles has
also shown promise for the safe characterization and
assessment of enhancement of renal masses and may
play an important role in patients with CKD in the
future.
Renal arteriography has a limited role in the
diagnostic evaluation of renal masses and is
primarily reserved for patients with concomitant
renal artery disease.

Chest radiograph.
Careful and systematic review of the abdominal
and pelvic CT or MRI findings.
Liver function tests.
Bone scintiscan can be reserved for patients with
elevated serum alkaline phosphatase or bone
pain.
Chest CT scan can be reserved for patients with
pulmonary symptoms or an abnormal CXR.

Bosniak developed a useful classification scheme
primarily based on CT imaging criteria that divides
renal cystic lesions into categories that are distinct
from one another in terms of the likelihood of
malignancy.


Patients with End-Stage Renal Disease
Screen only patients with long life expectancy and
minimal major comorbidities.
Perform periodic ultrasound examination or CT scan
beginning during third year on dialysis.
Patients with Known von Hippel-Lindau Syndrome
Obtain biannual abdominal CT or ultrasound study
beginning at age 15 to 20 years. Perform periodic
clinical and radiographic screening for nonrenal
manifestations.

Relatives of Patients with von Hippel-Lindau Syndrome
Obtain genetic analysis. If positive, follow screening
recommendations for patients with known VHL
Syndrome.
If negative, less stringent follow-up is required
Relatives of Patients with Other Familial Forms of RCC
Obtain periodic ultrasound or CT study and consider
genetic analysis.
Patients with Tuberous Sclerosis
Perform periodic screening with ultrasound examination
or CT scan.
Patients with ADPCKD-
Routine screening is not justified.

T: Primary Tumor
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor ≤7.0 cm and confined to the kidney
-T1a Tumor ≤4.0 cm and confined to the kidney
-T1b Tumor >4.0 cm and ≤7.0 cm and confined tothe kidney.
T2 Tumor >7.0 cm and confined to the kidney
-T2a Tumor >7.0 cm and ≤10.0 cm and confined to the kidney
-T2b Tumor >10.0 cm and confined to the kidney

T3 Tumor extends into major veins or perinephric tissues but not into the ipsilateral adrenal gland and not beyond the Gerota fascia
T3aTumor grossly extends into the renal vein or its segmental (muscle containing) branches or tumor invades perirenal and/or renal sinus fat but not beyond the Gerotafascia.
T3b Tumor grossly extends into the vena cava below the diaphragm
T3c Tumor grossly extends into the vena cava above the diaphragm or invades the wall of the vena cava
T4 Tumor invades beyond the Gerota fascia(including contiguous extension into the ipsilateral adrenal gland)

N: Regional Lymph Nodes
NX: Regional lymph nodes cannot be assessed
N0: No regional lymph nodes metastasis
N1: Metastasis in regional lymph node(s)
M: Distant Metastases
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis present

Stage Grouping
Stage I -T1 N0 M0
Stage II -T2 N0 M0
Stage III - T1 or T2 N1 M0
-T3 Any N M0
Stage IV -T4 Any N M0
-Any T Any N M1

Radical nephrectomy (RN)-gold standard
Partial nephrectomy (PN)
Thermal ablation (TA) and
Active surveillance (AS)

66% and 64% overall survival for stage I and II tumors, respectively compared with pericapsularnephrectomy.
RN has more recently fallen out of favor for small renal tumors due to concerns about CKD, and should only be performed when necessary.
CONCEPT-1. basic principles of early ligation of the renal artery and vein,2. Removal of the kidney with Gerota fascia, 3. Ipsilateral adrenal gland, and complete regional lymphadenectomy.

Types of incisions used in
radical nephrectomy.
A: Full flank
(thoracoabdominal).
B:Anterior
thoracoabdominal.
C: Subcostal.
D: Chevron.
E: Midline.

PATHOLOGIC
TUMOR
STAGE
HISTORY,
EXAMINATION,
AND BLOOD
TESTS
CHEST
RADIOGRAPH
ABDOMINAL
CT SCAN
pT1aN0M0 Yearly - -
pT1b-2bN0M0 Yearly Yearly -
pT3-4N0M0 6monthly Every 6 mo for
3 yr, then
yearly
At 1 yr, then
every 2 yr
pTxN1M0 Every 6 mo for
3 yr, then
yearly
Every 4 mo for
2 yr, then
every 6 mo
Every 6 mo for
1 yr, then
yearly
*Blood tests should include serum creatinine, blood urea nitrogen,
electrolytes, serum calcium, alkaline phosphatase, and a LFT

INDICATIONS:1.Solitary kidney
2.Bilateral RCC or RCC involving a solitary functioning kidney.
3.pre-existing CKD.
4.genetic tumor syndromes.
Margin width appears to be immaterial as long as the final margins are negative; this is particularly relevant when the tumor is located within the hilumand preservation of renal function is at a premium.

A functioning renal remnant of at least 20% of one
kidney is necessary to avoid end-stage renal failure
PN is standard care in management of clinical T1a
and T1b masses in the presence of a normal
contralateral kidney.
A 24-hour urinary protein measurement should be
obtained yearly in patients with a solitary remnant
kidney to screen for hyperfiltration nephropathy.

PATHOLOGIC
TUMOR STAGE
HISTORY,
EXAMINATION,
AND BLOOD
TESTS
CHEST
RADIOGRAPH
ABDOMINAL
CT SCAN
pT1aN0M0 yearly - -
pT1b-2bN0M0 yearly yearly Every 2yr
pT3N0M0 Every 6 mo for
3 yr, then
Yearly
Every 6 mo for
3 yr, then
yearly
Every 6 mo for
3 yr, then
every 2 yr

Renal cryosurgery
Radiofrequency ablation
Can be administered percutaneously or through laparoscopic exposure
Reduced morbidity and more rapid recovery
Disdvantages: 1.Longterm efficacy not known
2. Local recurrence.
3. lack of accurate histologic & pathologic staging associated with these modalities, because the treated lesion is left in situ.

Candidates for TA- Advanced age,co-
morbidities,local recurrence after PN, patients with
hereditary renal cancer who present with multifocal
lesions for which multiple PNs might be
cumbersome if not impossible and tumor size
<3cms.
successful local control in 90% to 95% of patients.
Central or nodular enhancement within the tumor
bed on extended follow-up has been considered
diagnostic of local recurrence.
Experience with RFA is more limited
Exciting new technologies, such as High-intensity focused
ultrasound (HIFU) and frameless, image-guided radiosurgical
treatments (CyberKnife).

Incidental discovery of many small RCCs in asymptomatic elderly patients or those of poor surgical risk has provided the opportunity to observe the growth rate of these tumors in patients who are unable or unwilling to undergo surgery.
Studies suggest that patients with small, solid, enhancing, well-marginated, homogeneous renal lesions, who are elderly or poor surgical risks, can safely be managed with observation and serial renal imaging at 6-month or 1-year intervals.
AS is not appropriate-
1.patients with larger (>3 to 4 cm), poorly marginated, or nonhomogeneous solid renal lesions.
2.In younger, otherwise healthy patients with small, solid tumors that have radiographic characteristics consistent with RCC.

A. Inferior Vena Caval Involvement- 4-10%
1. Unique feature-venous tumor thrombus-Rx- IVC thrombectomy.
2. Tumor extending into the perinephric fat, lymph node involvement, or direct invasion of the wall of the IVC -higher risk of recurrence.
3. Thrombus extending above the main hepatic veins requires more extensive dissection, venovenous bypass, or cardiopulmonary bypass and circulatory arrest.

LEVEL I- Adjacent to the ostium of renal vein.
LEVEL II- Extending up to the lower aspect of
the liver.
LEVEL III- Involving the intrahepatic portion of
the IVC but below the diaphragm and
LEVEL IV- Extending above the diaphragm.
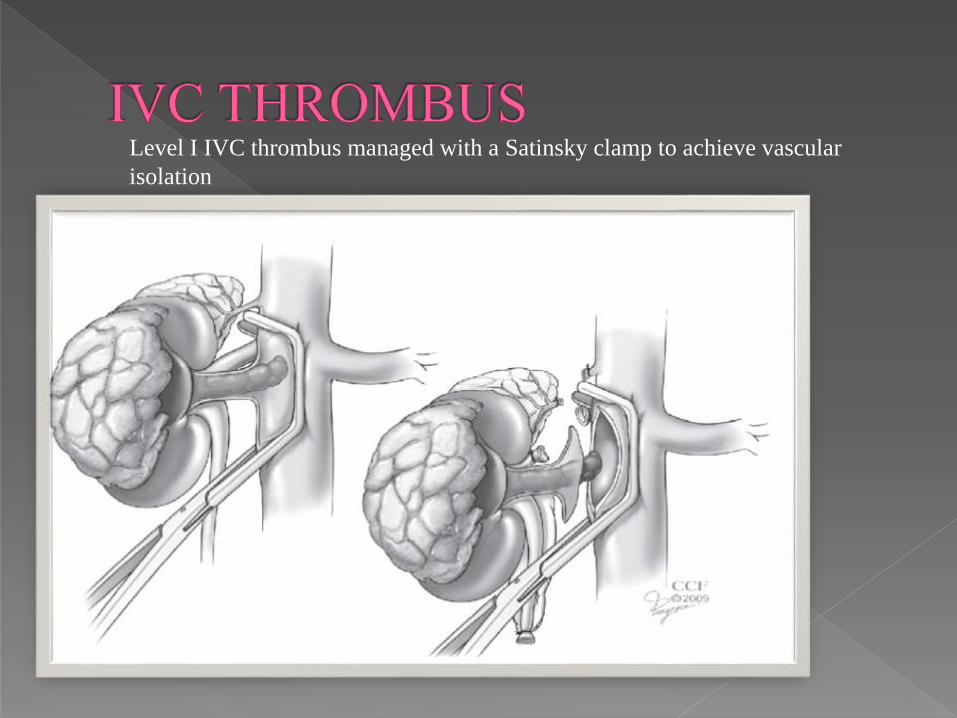
Level I IVC thrombus managed with a Satinsky clamp to achieve vascular
isolation

Level II IVC thrombus managed by sequential clamping of
the lower IVC, contralateral renal vein, and cephalad
IVC,along with mobilization of the IVC and occlusion of
lumbar veins, allowing for vascular isolation.

•Level III IVC thrombus
managed by mobilization of the
liver providing exposure of the
intrahepatic IVC and retraction
of the thrombus to facilitate
placement of the upper IVC
clamp just below the level of the
hepatic veins.
•If the cephalad clamp
must be placed above the level of
the hepatic veins, a Pringle
maneuver should be
performed to temporarily
occlude the hepatic blood flow.

B. Locally Invasive Renal Cell Carcinoma-
Present with pain, generally from invasion of the posterior abdominal wall, nerve roots, or paraspinous muscles.
Large, invasive upper quadrant abdominal masses, differential diagnosis should be considered, including adrenocorticalcarcinoma, infiltrative transitional cell carcinoma, sarcoma, and lymphoma, in addition to locally invasive RCC.
Because surgical therapy is the only potentially curative management for RCC, extended operations with en-bloc resection of adjacent organs are occasionally indicated.
Complete excision of the tumor, including resection of the involved bowel, spleen, or abdominal wall muscles, is the aim of therapy.
Most reports suggest that less than 5% of patients with extension into adjacent viscera (stage pT4) survive 5 years after surgery.

1.Debulking or Cytoreductive Nephrectomy-
Improved survival in carefully selected metastatic RCC patients undergoing cytoreductive nephrectomy f/b cytokine therapy (IFN-α) compared with those receiving cytokine therapy alone.
Factors inflencing outcome; patients with poor performance status, comorbid medical conditions, rapidly progressive disease, presence of brain metastases, and so on, are unlikely to benefit from this approach.
The role of cytoreductive nephrectomy as a prelude to systemic therapy with currently available novel targeted agents is unclear and is the subject of ongoing clinical trials.

Resection of isolated metastatic lesions is appropriate in selected
patients.
Median overall survival rates of 35% to 50%.
Factors a/w improved outcome- including complete resection,
solitary metastatic lesions, age <60 years, smaller tumor size,
presence of pulmonary metastases, and development of
metachronous metastatic disease.
There are no prospective, randomized studies demonstrating a
favorable outcome with metastasectomy..

Cytoreductive nephrectomy -Help alleviate
symptoms related to the primary tumor (e.g.,
intractable pain, hematuria) or paraneoplastic
manifestations.
Resection of metastatic lesions (often in
combination with radiation or systemic therapy)
is sometimes performed for relief of symptoms or
to prevent life-threatening or disabling sequelae.

Interferons-Alfa
High dose IL-2-Patients with clear cell RCC
appear most likely to benefit from IL-2 therapy.
Allogeneic Hematopoietic Stem Cell Transplantation
remains an experimental approach in the
management of RCC

VEGFR active in clear cellRCC is not active in
HPRCC.

Nephroblastoma, also known as Wilms tumor, is the MC solid renal tumor of childhood, 5% of childhood cancers.
3rd yr of life, no sex predilection.
Mostly U/L, 5% are B/L.
1% are familial.
10% a/w congenital malformations.ex:-WAGR, Beckwith-Wiedemann syndrome.
5–10% of sporadic Wilms tumors have been demonstrated to have WT1 mutations.11p13

WT consists of blastemal, epithelial, and stromalelements in varying proportions.
Generally large, multilobulated, and gray or tan in color with focal areas of hemorrhage and necrosis.
Tumor dissemination direct extension -renal capsule, hematogenously via the renal vein and vena cava, or via lymphatic spread.
Metastatic disease at diagnosis in 10–15% of patients, with the lungs (85–95%) and liver (10–15%) the most common sites of involvement.

A cross-section of a
pale tan neoplasm
attached to a residual
portion of the
kidney.

This shows highly
cellular areas
composed of
undifferentiated
blastema, loose
stroma containing
undifferentiated
mesenchymal
cells and immature
tubule

Abdominal pain and distention, anorexia, nausea and vomiting, fever, and hematuria.
Most common sign is an abdominal mass.
Hypertension is seen in 25–60% of cases and is caused by elevated renin levels.
30%-hematuria and 10%-coagulopathy.

Abnormal urine findings and LFT if mets.
USG
CT
MRI
CXR –lung metastasis
NEEDLE BIOPSY-large tumors for safe Sx
resection and safe pr-op CT & RT.

a) Hydronephrosis,
b) Cystic kidneys
c) Intrarenal neuroblastoma. (drooping lily).
d) Mesoblastic nephroma, and
e) various very rare sarcomas.
Mesoblastic nephromas are benign hamartomasand cannot be preoperatively distinguished from Wilms tumors. Most commonly seen in the neonatal period and are typically identified by surgical pathology after nephrectomy.

Stage I:—Tumor limited to kidney and completely excised. No penetration of renal capsule or involvement of renal sinus vessels. Tumor was not ruptured before or during removal. There is no residual tumor apparent beyond the margins of resection.
Stage II:—Tumor extends beyond the kidney but is completely removed. There is either penetration through the outer surface of the renal capsule, invasion of renal sinus vessels, biopsy of tumor before removal or spillage of tumor locally during removal. There is no residual tumor apparent at or beyond the margins of excision and no lymph node involvement.

Stage III:—Residual non-hematogenous tumor confined to abdomen. Any one or more of the following occur:
(a) regional lymph node involvement
(b) diffuse peritoneal contamination by tumor, such as spillage of tumor beyond the flank before or during surgery, or by tumor growth that has penetrated through the peritoneal surface.
(c) Implants are found on the peritoneal surfaces;
(d) Tumor extends beyond the surgical margins either microscopically or grossly .
(e) The tumor is not completely resectable because of local infiltration into vital structures.
(f) tumor spill not confined to the flank occurred either before or during surgery.
(g) transected tumor thrombus.

Stage IV:—Hematogenous metastases to lung,
liver, bone, and brain.
Stage V:—Bilateral renal involvement at
diagnosis. An attempt should be made to stage
each side according to the previously given
criteria on the basis of extent of disease before
biopsy.

SURGICAL-Radical nephrectomy. Avoid
spillage because there is evidence that this
increases abdominal recurrence.
RLND-not of proven value.
Biopsy of regional lymphatics (renal hilum and
para-aortic nodes) and careful examination of the
opposite kidney and the remainder of the
abdomen provide crucial data for staging and
prognosis.

B/L tumor with favourable histology-pre-op CT.
f/b renal sparing Sx. A biopsy for diagnosis and
staging is indicated in these cases.
Unfavourable histology-aggressive surgery
followed by CT & RT.

CT- A) favourable histology
1) stage I & II Sx resection + vincristine and dactinomycin combinations without radiotherapy
2) Stage III &IV Sx resection + vincristine,dactinomycin& doxorubicin with RT.
B)Unfavourable histology-
1)Stage I & II same as III & IV of faourable
2) stage II–IV vincristine, doxorubicin, cyclophosphamide,and etoposide
Salvage chemotherapy- cyclophosphamide, ifosfamide, carboplatin and etoposide

stage V-CT f/b 6-8weeks 2nd look Sx.
Renal sparing procedures-High rate of renal
failure .
RADIOTHERAPY- stage III or IV disease with
favorable histology, stages II–IV with focal
anaplasia and clear cell sarcoma, and all stages of
rhabdoid tumor of the kidney.



The origin of the right renal artery is beneath the left
renal vein. It typically passes posterior to the IVC.
During transabdominal left radical nephrectomy,
knowledge of this anatomic relationship may prevent
inadvertent ligation of the right renal artery.
The kidney is divided into four segments (superior,
anterior, posterior, inferior) that are supplied by one or
more segmental renal arteries, which are end arteries.
Ligation or occlusion of a segmental artery, or any of
its branches, leads to devitalization of renal tissue.

The renal venous system is characterized by a rich anastomotic
network between the various renal segments. One may ligate and
divide segmental veins without compromising drainage.
The right renal vein does not receive significant branches.
Tributaries draining into the main left renal vein include the
gonadal vein, the left adrenal vein, and one or two large lumbar
veins, all of which can be injured during mobilization of the left
renal vein. Because of these collateral vessels,one is at liberty to
ligate the left renal vein at the caval junction without eliminating
venous return.
Frequent anatomic variation in the renal vasculature contribute to
the complexity of open renal surgery. Multiple renal arteries, which
typically arise from the aorta or iliac arteries, are the most common
variation, occurring in 25% to 30% of the population
Top Related