







Languages
Pages
Legal


REGIONAL ANAESTHESIA IN OPTHALMIC SURGERYMODERATOR :- Dr. RANI SUNDAR
PRESENTED BY :- UMAKANTH BIKASH
www.anaesthesia.co.in [email protected]

Introduction
Anaesthetic requirements for ophthalmic surgery :
- Nature of the surgery - Surgeon’s preference - Patient’s preference Local
Topical Regional
General

Local anaesthesia for eyes
Non-akinetic and akinetic methods
Non –akinetic techniques
Topical ( drops & gel )
Subconjunctival
Deep fornix anaesthesia
Akinetic techniques Akinetic blocks :
1. Needle techniques - Intraconal - Extraconal - Combined intraconal & extraconal 2. Cannula techniques - Sub- tenon’s block
Ophthalmic surgeons prefer immobile eyes Friedman et al - patients also prefer akinetic
regional ophthalmic block. Br J Ophthalmol 2004;88:333-5
Topical anaesthesia for eyes Non-invasive
Minimal complications
Challenging operating conditions – no akinesia Popular for phacoemulsification cataract surgery
Careful patient selection Co-operative Must be able to lie supine & still Sedation
Regional anaesthesia Advantages
Day cases Good akinesia & anaesthesia Minimal effect on IOP Minimal equipment required Low failure rate & high safety profile
Disadvantages Not suitable for all patients Complications Skill of anaesthetist Unsuitable for certain types of surgery

Anatomy
The orbit irregular four-sided pyramid Apex - pointing posteromedially & Base - facing anteriorly Annulus of Zinn → fibrous ring arising from the superior orbital fissure, forms the apex The surface of cornea, conjunctiva & lids → forms the base
Globe movements are controlled by - - Rectus muscles (inferior, lateral, medial &superior) - Oblique muscles (superior & inferior) Rectus muscles → origin - annulus of Zinn insertion - anterior to the equator of the globe,
Forms an incomplete cone

Orbit

Cone formed by rectus muscles
Nerve supply
Within the muscle cone :- - Optic nerve (II) - Oculomotor nerves (III) - Abducent nerve (VI nerve), - Nasociliary nerve (a branch of V nerve), - Ciliary ganglion and vessels
ALL3 SO4 LR6
Trochlear nerve runs outside & above annulus→ superior oblique (retained activity of this muscle is frequently observed ). Nasociliary nerve → Corneal & perilimbal conjunctival
Frontal & infraorbital nerves → remainder of the peripheral conjunctival

Cont.

Tenon’s space anatomy
Tenon’s capsule → thin membrane enveloping the globe & separating it from orbital fat
Inner surface separated from the outer surface of the sclera by a potential space the sub- tenon’s space
Sub- tenon’s space → lymphatic space
Follows the optic nerve & continues with subarachnoid space

Assessment and Preparation British Ophthalmic Anesthesia Society :- fasting regimen
there is difference in clinical practice by different anaesthesist Majority do not consider that it is necessary for the pt to be fasted
prior to local anesthesia for eye surgery ( 65 % did not restrict any food or liquid intake )
Complication rates of starvation or aspiration in ophthalmic regional anesthesia are unknown
Pre-op investigations Routine investigation of patients for catract surgery is not essential
Tests can be done to improve the general health of the patient if required.
Royal College of Anaesthetists and The Royal College of Ophthalmologists, 2001
Cont. Enquiry about bleeding disorders & related drugs
Konstantatos et al – Patients on anticoagulants to continue their medication Clotting results should be within therapeutic range. Anaesth Intensive Care 2001;29:11-8
Recommendation for patients receiving antiplatelet agents - Currently no recomendation Katz J et al Study - Ophthalmology 2003; 110: 1784-8
- Procedures under topical, subconjunctival, sub- Tenon’s blocks are recommended Konstantatos A et al - Anaesth Intensive Care 2001;29:11-8

Chassot et al :- Extra occular & anterior chamber surgery can be conducted
during dual antiplatelet theraphy
Posterior chamber procedures require cessation of
clopidogrel ( but not asprine )
Only emergency surgery should be performed on full antiplatelet theraphy
The risk/benefit ratio of preoperative withdrawal of antiplatelet drugs in order to perform regional blocked is not justified
BJA 99 (3):316-28 (2007)

Hamilton RC et al – Risk factors that predispose globe penetration - Presence of a long eye - Staphyloma or enophthalmos - Faulty technique - Lack of appreciation of risk factors - Uncooperative patient - Use of unnecessarily long needles OphthalmolClin North Am 1998;11:99-114.
Patients with axial myopia have greater risk of globe puncture
Risk rate is- 1 in 140 needle blocks with an axial length > 26 mm. Duker et al: Ophthalmology 1991;98:519-26. If axial length not known → power of patients spectacles
In highmyopia & in case of pre-existing scleral buckle a classical peribulbar block or a single medial peribulbar injection is advocated.
Johnson, International Practice of Anaesthesia. 1996 & Vohra SB ,Br J Anaesth 2000;85:242-5.

Cont. Anaesthetic & surgical procedures are explained All monitoring and anaesthetic equipments should be functional
Intravenous line :- # Mathew et al - ? insertion of an IV line for topical or sub- Tenon’s injection J Cataract Refract Surg 2003;29:1132-6. # Anaesthetists and The Royal College of Ophthalmologists, 2001 - IV line must be inserted before embarking on a needle block # Kumar CM, Dodds et al - - Presence of a secure IV line remains good clinical practice Ophthalmic Anaesthesia. The Netherlands, 2002.
Types of regional anaesthesia Akinetic Needle Technique
Peribulbar block (Pericone) Retrobulbar block (Intracone, Atkinson’s)
Sub- Tenon’s block
(parabulbar block, pinpoint anaesthesia,
medial episcleral block)
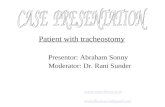
Retrobulbar block –
The Atkinson’s or classical retrobulbar block –
- Needle inserted through the skin, at the junction of
medial 2/3rd & lateral 1/3rd of the lower orbital margin
- 2 to 3 mL of local anaesthetic is injected deep into the
orbit behind the globe with the patient looking upwards
& inwards
- A separate 7th nerve block is required.

Cont.
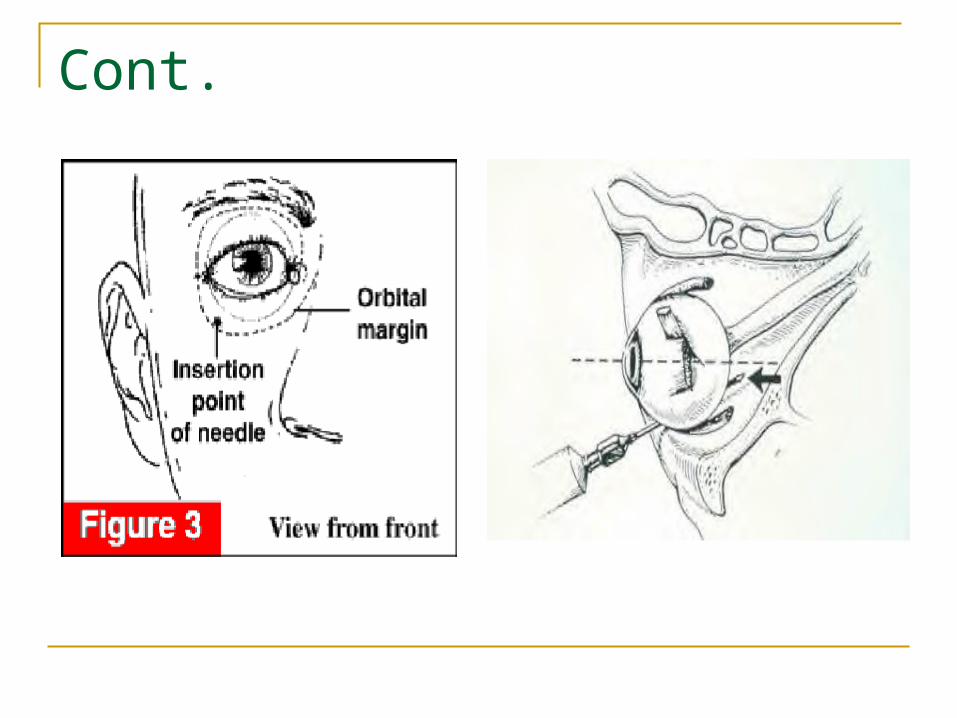
In modern retrobulbar block
- 25-G, 31-mm long needle is inserted through the
conjunctiva or skin in the inferotemporal quadrant as
far laterally as possible below the LR muscle.
- initial direction is tangential to the globe,
once past the equator ,needle goes upwards &
inwards to enter the space behind the globe
4 to 5 mL of local anaesthetic injected
Cont.
Cont.
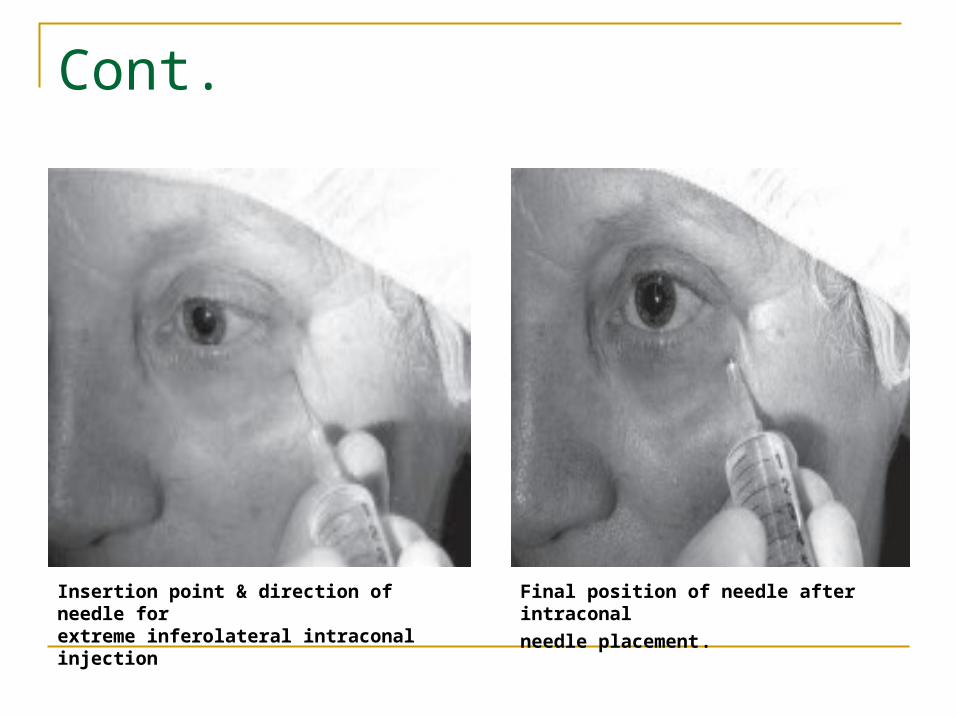
Insertion point & direction of needle forextreme inferolateral intraconal injection
Final position of needle after intraconal
needle placement.

Peribulbar block : 2 injections Inferotemporal injection
Injection is made outside the cone. A 25-G, 31-mm long needle inserted through the
conjunctiva as far laterally as possible in the inferotemporal quadrant.
Once the needle is under the globe, it is directed along the orbital floor.
5 mL of local anaesthetic agent is injected.
Many patients require a supplementary injection.

Cont.
Cont.
Nasal injection A medial peribulbar block is performed to
supplement inferotemporal retrobulbar or peribulbar injection, particularly when akinesia is not adequate.
Rubin A. Eye blocks. In: Principles and Practice of Regional Anaesthesia :
Churhill Livingstone, 2003
25 or 27-G needle is inserted in the blind pit between the caruncle & medial canthus to a depth of 15 to 20 mm
. 3 to 5 mL of local anaesthetic agent is injected

Cont.

Cont.
Direction and placement of needle formedial peribulbar injection

Needle Selection for Akinetic Block Historically → 38 mm long needle
Chandra M Kumar et al – Distance between inferior orbital rim & apex 42 to 54 mm Ciliary ganglion lie → 7 mm in front of the apex ( as per study in 120 cadaveric skull ) Hence ciliary ganglion is 35 mm from the inferior orbital rim Patients with shallow orbit are at a ↑ risk with needles ≥ 35 mm
Vanden Berg et al –
Shorter (25 mm) needles are recommended
Some authors claim excellent results with 16-mm needles Anaesthesia 2004;59:775-80
Bevel and tip of needle – controversy
Grizzard WS et al -
Sharp narrow-gauge needles (25 to 31 gauges) reduce Discomfort on insertion at the expense of a reduced tactile
feedback Theoretically higher risk to recognise a globe perforation
Ophthalmology 1991;98:1011-6 Kimble JA et al – Advantage of blunt needles
Blood vessels were pushed rather than traumatised Tissue planes could be more accurately defined
Arch Ophthalmol 1987;105:749 Grizzard WS et al – Blunt needles
More likely to cause greater damage when misplace Ophthalmology 1991;98:1011-6

Complication of agent
Systemic complication
- Over dose - Intravascular - Allergic or vasovagal reaction. - Into CSF within a cuff of dura around the optic nerve (confusion, convulsion, unconsiousness, respiratory & cardiac arrest)
- Over dose or intra vascular injection of adrenalin - Allergic reaction to hyaluronidase
Complications of the techniques Subconjuctival odema (chemosis )
Frequently follow large volume of peribulbar injection than retrobulbar injection
Resolves with use of pressure No intra or postoperative problem
Bruising (ecchymosis ) Disfiguring Conjuctival rather than skin injection to prevent
bruising
Retrobulbar hemorrhage Incidence = 0.1 -1.7 % Predisposing factor : Elderly Vascular or haematological disease Pt on steroids, aspirin, NSAIDS, anticoagulant Manifest by : Tight eyelids Subconjuctival or periorbital hemorrhage & Dramatic increase in IOP Central retinal artery pulsation should be monitored Impending retinal artery occlusion → Decompressive surgery or Anterior chamber paracentesis Postpone surgery Cionni et al :- If pressure reducing device decreases IOP, surgery can be carried out opthalmology 1991: 98
Globe perforation
Both in peribulbar & retrobulbar blocks
Incidence :- 1 in 874 Gillow et al, Eye 1996;10:533-536
1 in 12,000 Devis et al, J Catract Refract surg;1994:20
1 in 16,224 Manner et al, Eye 1996;10:367-370
More in long & thin eye
Globes longer than 26mm are at risk
Pt who had or presenting for retinal detachment surgery and pt with myopia have long globes
Cont. Diagnosis by- Pain at time of injection Sudden loss of vision Hypotonia Poor red reflex or vitrous haemorage
When suspected or diagnosed →discuss with the surgeon May be avoided by : - Knowledge of orbital anatomy and length of globe - Initial tangential niddle insertion - Not going “up and in “ till niddle tip past the equator - Aiming for inferior portion of superior orbital fissure rather than orbital apex

Optic nerve atrophy- Direct injury to optic nerve or retinal artery Injection into optic nerve sheath or hemorrhage in optic nerve
sheath Retrobulbar hemorrhage
May lead to partial or complete visual loss
Amaurosis Mainly with retrobulbar block due to optic nerve block Not with peribulbar block Pt should be explained
Occulo cardiac reflex Occasionally Pt should be monitored

Penatration of optic nerve sheath Injection into the dural cuff of optic nerve subarachnoid spread of anaesthetic agent
Nicoll et al :- In 6000 retrobulbar block , incidence is 1 in 375 with 1 in 700 life threatening Anesthesia and analgesia;1987:66
Hamilton et al - incidence is 3 per 1000 Canadian journal of anaesthesia;1988: 35
All injection should be made with the globe in primary gaze position
Symptoms usually appear within 8 min ( immediately or upto 40 min after block)

Sign & symptoms :- Drowsiness , vomiting Contralateral blindness Convulsion Respiratory depression or arrest Neurological deficit Cardiac arrest Myotoxicity - Most frequently affect the inferior rectus muscle
- Usually recover but sometimes required corrective surgery - Rainin etal Highest concentration of local anesthetic should not be
used as they are found to be myotoxic Archives of Opthalmology 1985;103
Direct injection into the muscle should be avoided
Sub Tenon’s Anaesthesia
Original idea of Turnbull (1884 )
Modified & popularised by Mein and Woodcock, Hansen, Stevens, Greenbaum & others
Also known as : Parabulbar block
Pinpoint anesthesia
Episcleral block
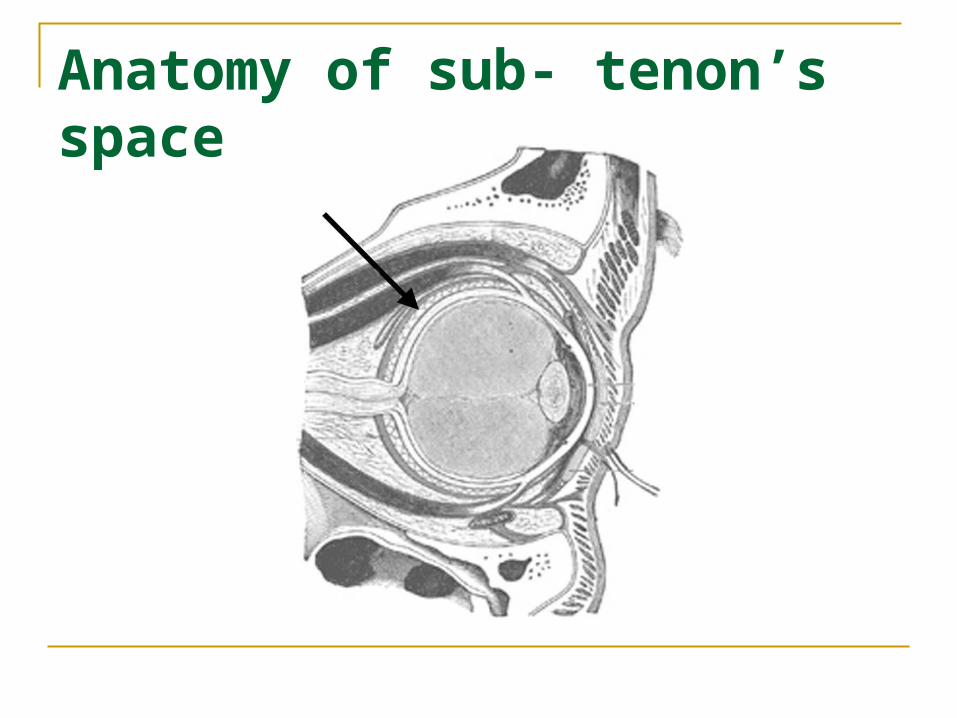
Anatomy of sub- tenon’s space

Sub- Tenon’s block Standard technique
Obtaining surface anaesthesia
Access to the sub-Tenon’s space
Insertion of a cannula
Administration of local anaesthetic agent

Inferonasal quadrant is the most common site of access (can be accessed from all 4 quadrants )
Stevens JD et al - Inferonasal quadrant allows good fluid distribution superiorly while avoiding area of surgery & damage to the vortex veins Br J Ophthalmol 1992; 76: 670–674
With the patient - looking upwards & outwards
Conjunctiva & Tenon’s capsule are gripped with non-toothed forceps (Moorfield forceps) ,5 to 10 mm away from the limbus
A small incision is made with scissors ( Westcott scissors) to expose the sclera & the cannula is inserted following the globe

Cont.

Cannulae for Sub-Tenon’s Block Metal or plastic
Commonly used cannula is → metal, 19-G, 2.54-cm long & curved with a blunt end
Others Southampton cannula Mid sub- Tenon cannula Anterior cannula Ultrashort cannula
Volume of LA varies from 1.5 -11 mL ( 3 to 5 mL is commonly used) Smaller volumes →provide globe anesthesia Larger volumes → if akinesia is desirable
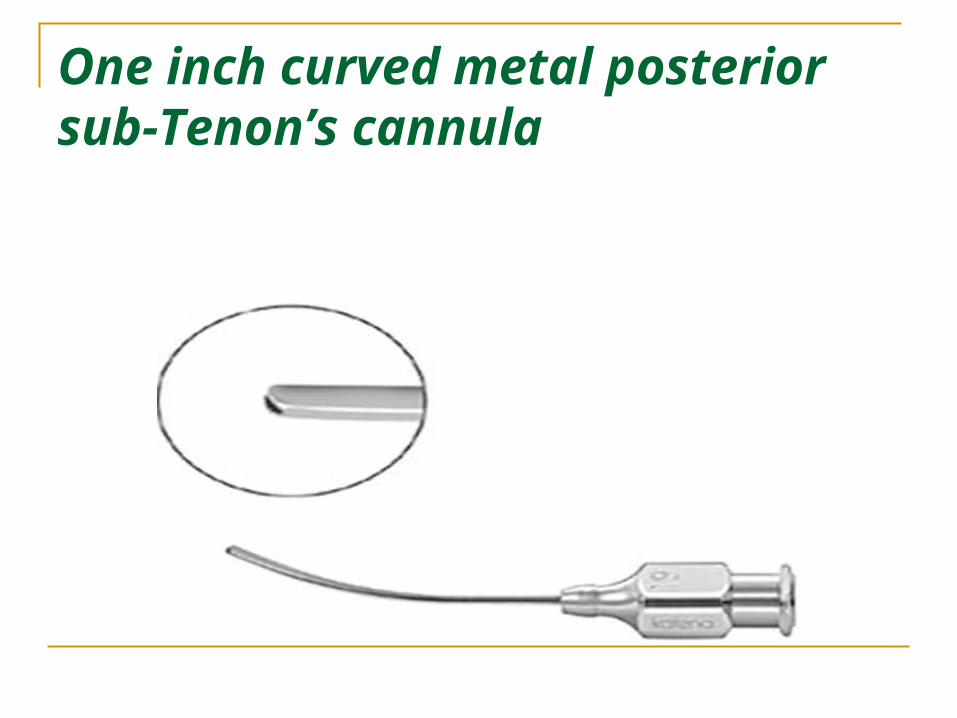
One inch curved metal posterior sub-Tenon’s cannula

Plastic anterior sub-Tenon’s cannula.
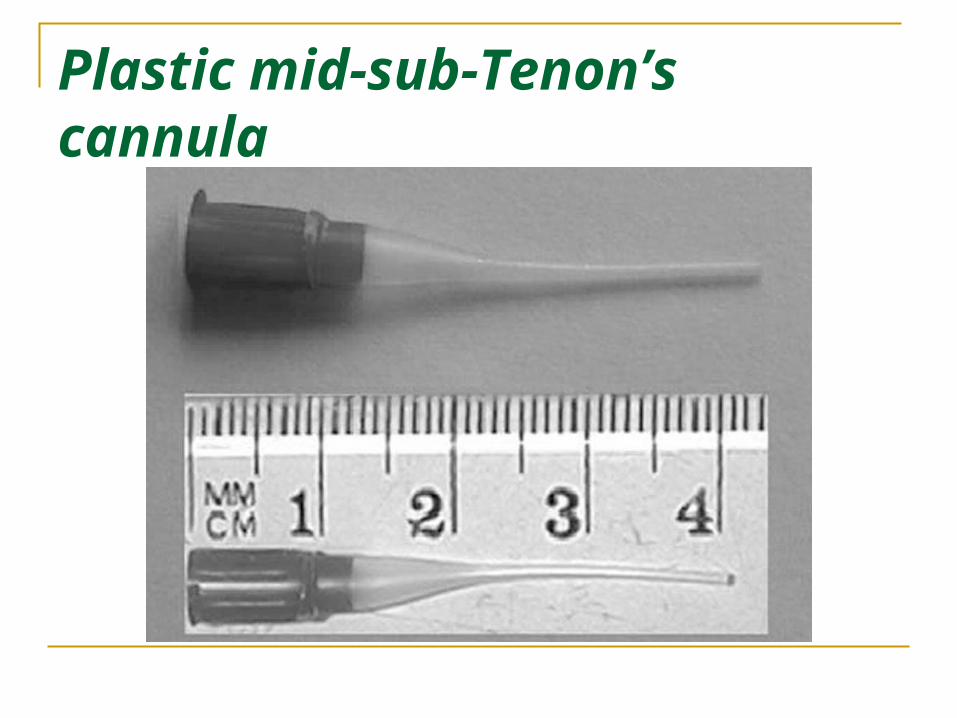
Plastic mid-sub-Tenon’s cannula

Cont. Behndig A et al – Prolonged anesthesia & analgesia are obtained by inserting a catheter in the sub-Tenon’s space. J Cataract Refract Surg 1998;24:1307-9
Sub-Tenon’s block used primarily for cataract surgery Also effective for →Viteroretinal surgery Panretinal photocoagulation Trabeculectomy Strabismus surgery Delivery of drugs
Sub-Tenon’s block favoured→ in patients on anticoagulants, aspirin & NSAIDs
Konstantatos A et al - Anaesth Intensive Care 2001;29:11-8

Passage of local anaesthetic agent during sub-Tenon’s injection Ultrasound & MRI studies shows –
injected anesthetic agent opens the sub-Tenon’s
space giving a characteristic ‘T-sign’
Local anaesthetic agent diffuses into intraconal & extraconal areas resulting in anesthesia & akinesia of the globe & eyelids
Intense analgesia is produced by blockade of the short ciliary nerves as they pass through the Tenon capsule

characteristics ‘T-sign’.
Complications of Sub-Tenon’s Block Minor complications → pain during injection, chemosis,
conjunctival hemorrhage & leakage of local anaesthetic Major complications → orbital & retrobulbar hemorrhage,
rectus muscle paresis & trauma, globe perforation, central spread of local anesthetic, orbital cellulites etc
Most of these complications occurs following use of 2.54- cm metal cannula.
Kumar CM et al - Eur J Anaesthesiol 2005;22:567-77.
Smaller or flexible cannulae appear to be safer but the incidence of minor complications increases.
Kumar CM & Dodds C et al - An Br J Anaesth 2001;87:631.

Pain during injection Multifactorial Incidence with posterior metal cannula ≈ up to 44%
Pain scores on a VAS have been reported as high as 5 Stevens JD - Br J Ophthalmol 1992; 76: 670–674
Smaller cannulae appear to offer a marginal benefit Kumar CM, & Dodds et al - Eye 2004; 18: 873–876 Guise PA et al -
Premedication or sedation during sub-Tenon’s injection does not add any benefit Anesthesiology 2003; 98: 964–968
Preoperative → explanation of the procedure, good surface anesthesia, gentle technique, slow injection of warm local anaesthetic agent & reassurance are considered good practice

Pharmacological Considerations during Ophthalmic Regional Block Local Anaesthetic Agent All the modern LA are suitable & studies have shown little difference in the quality of anesthesia, analgesia & akinesia Adjuvant Vasoconstrictors :- - Increases the intensity and duration of block & minimize bleeding from small vessels pH Alteration :- - Alkalization decreases onset time and prolong the duration of effect after needle block . Zahl K et al - Anesthesiology 1990;72:230
- No such benefit is seen during sub-Tenon’s block. Moharib et al - Reg Anesth Pain Med 2000;25:514-7
Hyaluronidase :-
Improves the effectiveness & quality of needle & sub- Tenon’s block
use remains controversial The amount of hyaluronidase used - 5 to150 IU / mL Orbital swelling - allergic actions or excessive doses & orbital
pseudotumour have been reported
Others :-
Muscle relaxants & clonidine are known to increase the onset & potency of orbital block
use is neither routine nor recommended.

Sedation and Ophthalmic Regional Blocks commonly used during topical anesthesia
patients, in whom explanation & reassurance have no benefit
Short acting BZP, opioids & small doses of IV anesthetic induction agents are used
The Royal College of Anaesthetists and The Royal College of Ophthalmologists, 2001 The routine use of sedation is discouraged A means of providing supplemental O2 should be available Sedation should only be used to allay anxiety & not to cover
inadequate block

Intraocular Pressure (IOP) and Ophthalmic Regional Blocks Changes in IOP after retrobulbar & peribulbar injections
are controversial
IOP is generally reported to increase immediately after injection
Bowman R et al - Br J Ophthalmol 1996;80:394-7. Palay DA et al - Ophthalmic Surg 1990;21:503-7. Watkins R et al - Br J Ophthalmol 2001;85:796-8.
IOP is not seen to increase after sub-Tenon’s block Ling R etal - J Cataract Refract Surg 2002;28:113-7. Vallance etal - J Cataract Refract Surg 2004;30:433-6. Alwitry etal - Eye 2001;15:733-5.
Retained Visual Sensations During Ophthalmic Regional Blocks Many patients experience intraoperative visual sensations
This include light, colours, movements & instruments during
all forms of local ophthalmic anesthesia
During sub- Tenon’s block (16%) found the experience to be unpleasant or frightening
Wickremasinghe et al - Eye 2003; 17: 501–-505
Patients receiving orbital blocks should receive preoperative
advice as this may alleviate an unpleasant experience

Intraoperative Care and Monitoring Patient should be comfortable with soft padding over
pressure areas
The Royal College of Anaesthetists and The Royal College of
Ophthalmologists
All patients undergoing major eye surgery under local anesthesia should be monitored with Spo2 ECG NIBP Maintenance of verbal contact
Choice of Technique Preference for anaesthetic technique by surgeons & patients varies
Recent article by Friedman et al - 72% patients preferred block anesthesia to topical anesthesia Br J Ophthalmol 2004;88:333-5.
Ruschen et al supports this view - Patients have higher satisfaction scores with sub- Tenon’s block over topical anesthesia alone. Br J Ophthalmol 2005;89:291-3
The choice of technique depend on a balance between - patient’s wishes - operative needs of the surgeon - skills of the anesthetist & - place where such surgery is being performed

The Rules
2001 Guidelines (RCA & Coll. of
Ophthalmologists) Trained staff Surgeons – topical /sub- conjunctival / sub- Tenon
( without anaesthetist ) Anaesthetist & iv access with retrobulbar &
peribulbar blocks Anaesthetist in charge when sedation is used
Top Related