






Languages
Pages
Legal


Reforming the Consultant Contract – the journey so far
Reforming the Consultant Contract – the case for change
Workforce Developments
• The Temple Report, which argued for more consultant presence out of hours to better support trainees
• The Doctors and Dentists Review Body Report on Clinical Excellence Awards
• Parallel reforms to Agenda for Change to help sustainability and affordability
• Challenges to the notion of long scales of time-served incremental progression.

Reforming the Consultant Contract – the case for change
Supporting Seven Day Services
− NHS England’s report on 7 day services
− The Academy of Medical Royal Colleges standards for 7 day consultant presence
− NHS England’s Commissioning Standards.

Reforming the Consultant Contract – the case for change
System Reform
• The Francis Report
“The core values expressed in the NHS Constitution should be given priority of place and
the overriding value should be that patients are put first, and everything done by the NHS
and everyone associated with it should be informed by this ethos”
• Simon Stevens Five Year Forward View
“Over the next several years, NHS employers and staff and their representatives will need to consider how working patterns and pay and terms and conditions can best evolve to fully reward high performance, support job and service redesign, and encourage recruitment and retention in parts of the country and in occupations where vacancies are high”
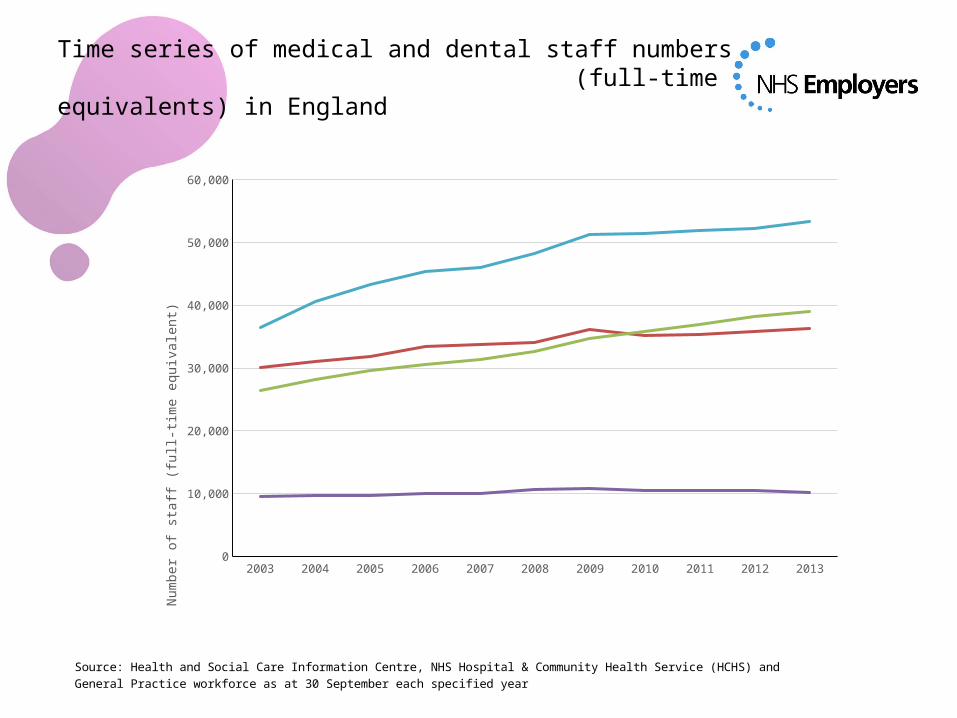
Time series of medical and dental staff numbers (full-time equivalents) in England
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
GPs
30084.3299999974
31020.9199999949
31901.439999995
33383.9099999999
33730.36 34043.01 36084.85 35242.66 35318.6079999994
35870.9269999996
36293.6309999993
Consultants
26340.687
28141.439
29612.648
30618.937
31429.95592
32678.851
34653.587
35780.7078000001
36964.6209299999
38196.60553
39013.64994
Other doctors
9517.461 9666.139 9661.27799999999
9934.047 10052.828894
10609.153
10728.68 10458.66227
10436.1740400001
10440.6747
10227.82394
Doctors in postgraduate training
36401.84 40654.161
43294.547
45422.139
46050.598484
48297.77 51216.02 51396.72743
51993.4876899992
52262.10651
53398.58139
5,000
15,000
25,000
35,000
45,000
55,000
Nu
mb
er o
f s
taff
(fu
ll-ti
me e
qu
iva
len
t)
Source: Health and Social Care Information Centre, NHS Hospital & Community Health Service (HCHS) and General Practice workforce as at 30 September each specified year
Reforming the Consultant Contract – a contract for the future
The key characteristics of any future contract are that it should
• Be cost neutral
• Meet the needs of patients, be fair to doctors and affordable for employers
• Provide for highest quality of excellence and professionalism
• Support the wider aims of the NHS.

Initial negotiations with the BMA resulted in some broad areas of agreement, including
• Recognition that patients deserved the same quality of care over the whole week
• That this would entail changes to traditional working patterns, including more senior clinical staff at weekends and evenings and the resources needed to help them deliver that care
• That this presented a significant affordability challenge• Modelling would be required to ensure that a new contract would
be cost neutral • Change would need to be accompanied by adequate safeguards to
protect the health and well being of doctors and patient care.
Reforming the Consultant Contract – preliminary negotiations
Safeguarding the core contract
• The retention of a negotiated national framework and the BMA’s role in collective bargaining
• a maximum 40-hour contract, unless extended by mutual agreement. No requirement for the majority of consultants to be contracted for more hours than they are currently contracted for
• no changes to any of the core contractual entitlements – redundancy, maternity, sick pay, leave entitlements, requests for flexible working etc.
Reforming the Consultant Contract – the employers’ side offer
Safeguarding pay
• retention of the current lifetime earnings potential• accelerated access to higher pay - consultants will be able to access
higher levels of pay earlier in their career than is possible under the current pay scales, as long as they meet all necessary access criteria
• the introduction of a fairer way to reward consultants who work frequent and intense shift patterns
• continued access to a national clinical excellence award (CEA) scheme, by competitive application
• transitional arrangements that provide protection to existing pensionable pay
• the introduction of a pay structure which is better suited to a Career Average Revalued Earnings (CARE) scheme
• local clinical excellence awards to be incorporated into the consultants’ contract as part of revised performance payments structure.
Reforming the Consultant Contract – the employers’ side offer
Safeguarding health and well-being and supporting professionalism
• jointly agreed safeguards (set out in the contract and supported by jointly agreed guidance), to ensure consultants are provided appropriate protections where service changes are necessary to deliver seven-day services
• a commitment to move towards consultant-led services which will require a growth in the consultant workforce
• greater emphasis on clinical engagement when determining service delivery priorities with a duty to consult being placed on employers
• a strengthened job planning process at the heart of the process for determining the appropriate clinical activity to support local service delivery
• A limit on the number of weekends that consultants will need to be available for work, without mutual agreement
• Protection of an environment where education, training, innovation and research by both NHS and academics can flourish.
Reforming the Consultant Contract – the employers’ side offer
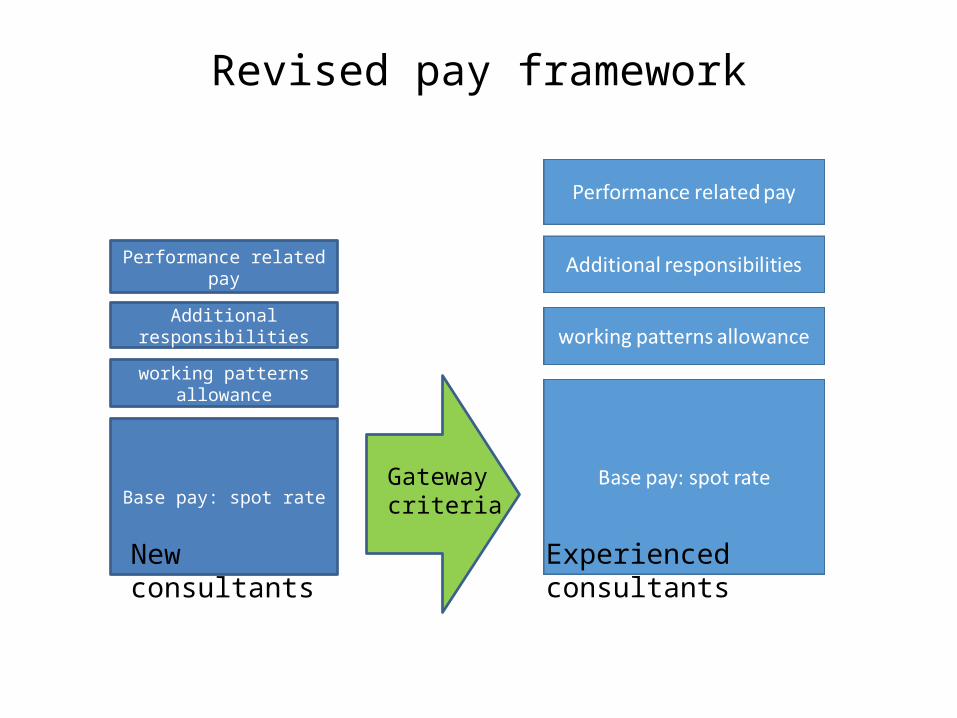
Revised pay framework
Base pay: spot rate
working patterns allowance
Additional responsibilities
Performance related pay
New consultants Experienced consultants
Gateway criteria

In the BMA’s own words, they could not continue with negotiations because of “unreasonable demands from the government that could undermine patient safety”.
• Patient welfare would be put at risk by employers demands• Priority should be given to urgent and emergency care• Data and modelling on future pay proposals was wholly inadequate
to allow their members to make an informed decision• There was an underlying lack of trust in the Government based
previous experiences on pay and pensions• Employers failed to move beyond broad statements of intent in
respect of safeguards contingent on removal of schedule 3 paragraph 6.
Reforming the Consultant Contract – the BMA response
What happens next?
− Ministerial remit to DDRB asking for ‘observations’ on consultant contract reform to support 7 day services
− Employer evidence submitted on 23 December 2014 with the publication of DDRB report expected July 2015 for consideration by Government, post election.
Reforming the Consultant Contract – not standing still
Possible options for employers to help meet current challenges
• Offering locally amended terms to new starters
• The development of local terms based on a national template
• Use of CCT holders in ‘other than consultant’ roles.

Maximising the flexibilities of the current contract
− Improving the quality of job planning so that all consultants have patient focused, outcomes based job plans designed to meet the needs of employers, consultants and patients
− Ensuring regular review of job plans so that they are up to date and relevant
− Ensuring that the criteria for pay progression are met. While pay progression is the norm for most consultants it is not necessarily automatic and depends, for example on participation in job planning and appraisal
− Strengthening appraisal and performance review processes
− Reviewing Additional Programmed Activities.

Meeting the challenge together
“Employee engagement will be absolutely crucial for the NHS over the coming years. Trusts which effectively engage their workforce have more satisfied staff, better clinical outcomes and are more efficient. If services are to be improved within a tight budget, trusts will have to unlock the immense potential creativity and innovation of their employees. And when change happens, staff need to be right at the heart of decision-making.”
Meeting the Challenge@ Successful Employee Engagement in the NHS – Involvement and Participation Association (IPA) April 2014.
Keeping informed and asking us questions
Doctors' contract talks - Q&As
www.nhsemployers.org/your-workforce/pay-and-reward/national-negotiations/doctors-contract-talks-qandas
Contact us at:[email protected]
@NHSE_Bill
Top Related