







Languages
Pages
Legal

Reducing harmful use of alcohol: Reducing harmful use of alcohol: from global strategy to actionfrom global strategy to action
Dag Rekve
Management of Substance Abuse
Department of Mental Health and Substance Abuse
WHO Headquarters

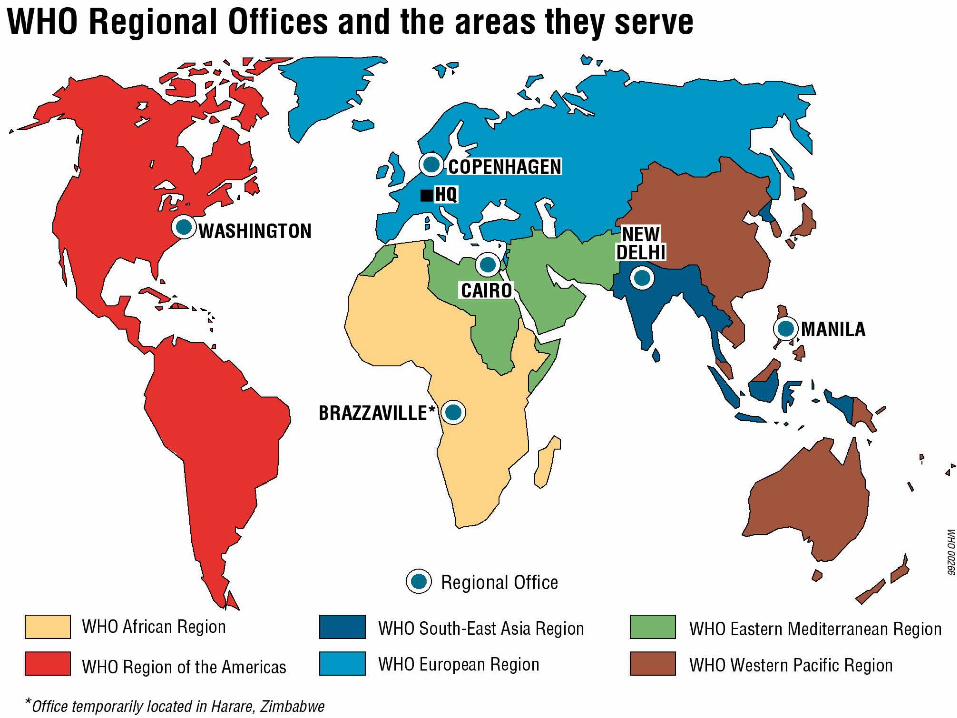
WHO governing structureWHO governing structureWHO governing structureWHO governing structure
UN specialized health agency
194 Member States
The World Health Assembly
Executive Board
6 Regional Committees
Consensus driven
Mostly non-binding

Global Status Report on Alcohol and Global Status Report on Alcohol and Health (WHO, 2011)Health (WHO, 2011)
Global Status Report on Alcohol and Global Status Report on Alcohol and Health (WHO, 2011)Health (WHO, 2011)
Continues series of the global status reports on alcohol and health from WHO
Based on the data from the Global Information System on Alcohol and Health (GISAH) and the Global Burden of Disease study
Contains country profiles for WHO Member States
Launched in Geneva on 11.02.2011 at the Global meeting of the WHO national counterparts to reduce the harmful use of alcohol
Highly commended in the public health category in the British Medical Association (BMA) Book competition 2012
Alcohol consumption Alcohol consumption in the world (WHO, 2011)in the world (WHO, 2011)
Alcohol consumption Alcohol consumption in the world (WHO, 2011)in the world (WHO, 2011)
Estimated ~2.5 billion people consuming alcoholic beverages
– on average 6.1 litres of pure alcohol per capita of adult (15+) population, including 1.8 litres (28.6%) of "unrecorded" alcohol
Estimated ~ 45% of the world adult population has never consumed alcohol
– Men – 35%– Women – 55%
In addition, 13.1% of men and 12.5% of women have not consumed alcohol during the past year
Source of data: WHO Global Information System on Alcohol and Health (GISAH)Source of data: WHO Global Information System on Alcohol and Health (GISAH)
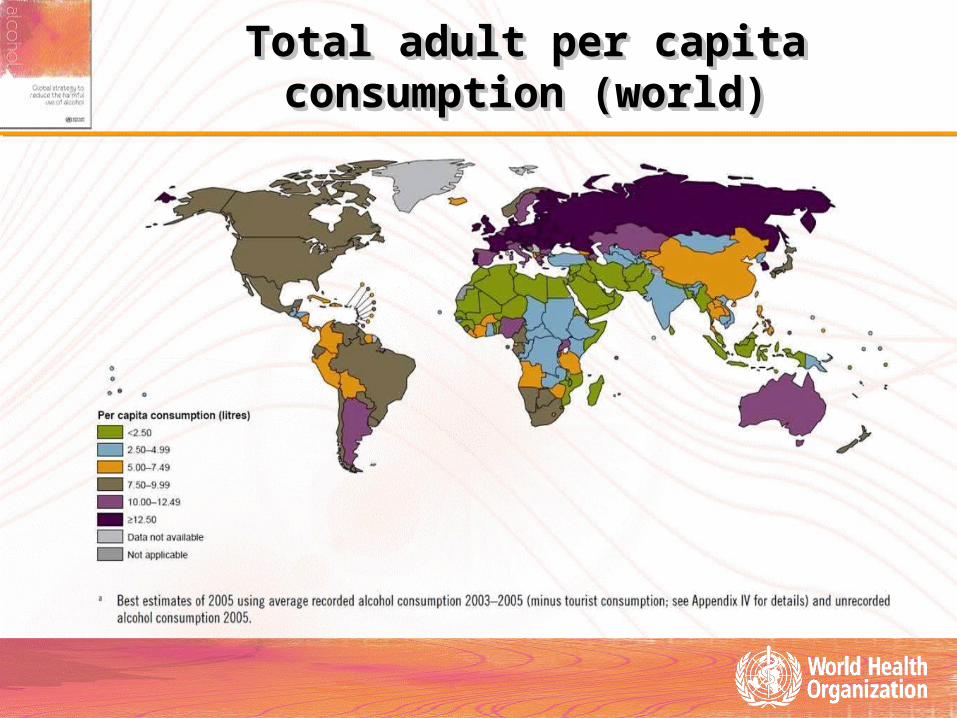
Total adult per capita consumption (world)Total adult per capita consumption (world)Total adult per capita consumption (world)Total adult per capita consumption (world)

Lifetime prevalence of abstention (world) Lifetime prevalence of abstention (world) Lifetime prevalence of abstention (world) Lifetime prevalence of abstention (world)

Patterns of drinkingPatterns of drinkingPatterns of drinkingPatterns of drinking

1. Impact on the individual drinker
2. Impact on people other than the drinker
3. Impact on overall health burden
4. Impact on social and economic development
Risks and consequencesRisks and consequencesRisks and consequencesRisks and consequences

Disease burden attributable to alcohol Disease burden attributable to alcohol consumption worldwide (WHO, 2011)consumption worldwide (WHO, 2011)Disease burden attributable to alcohol Disease burden attributable to alcohol consumption worldwide (WHO, 2011)consumption worldwide (WHO, 2011)
In 2004 estimated 2.5 million people died worldwide of alcohol-related causes which accounted for 3.8% of global mortality in all age groups
– 6.1% in men– 1.1% in women– 320 000 young people between 15 and 29 years old
4.6% of all DALYs lost worldwide due to harmful use of alcohol
– 7.1% in men– 1.4% in women
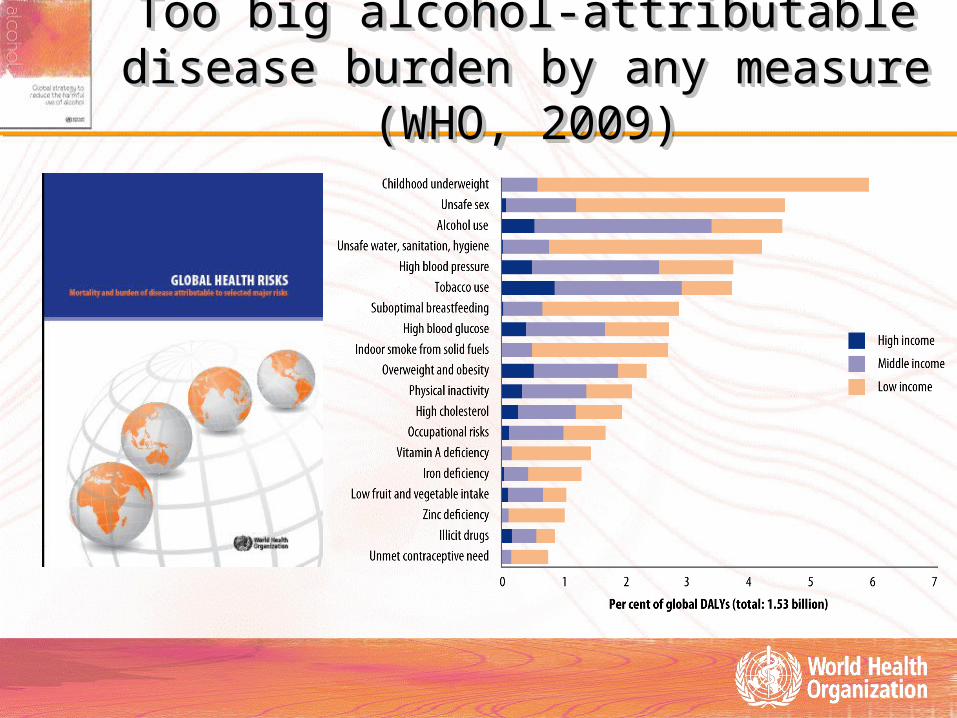
Too big alcohol-attributable disease Too big alcohol-attributable disease burden by any measure (WHO, 2009)burden by any measure (WHO, 2009)Too big alcohol-attributable disease Too big alcohol-attributable disease
burden by any measure (WHO, 2009)burden by any measure (WHO, 2009)

Global distribution of Global distribution of alcohol-attributable deaths and DALYsalcohol-attributable deaths and DALYs
Global distribution of Global distribution of alcohol-attributable deaths and DALYsalcohol-attributable deaths and DALYs
Deaths DALYs

DALYs attributed to 10 leading risk factors for the DALYs attributed to 10 leading risk factors for the age group 15 to 59 years old in the world age group 15 to 59 years old in the world
(WHO, 2009)(WHO, 2009)
DALYs attributed to 10 leading risk factors for the DALYs attributed to 10 leading risk factors for the age group 15 to 59 years old in the world age group 15 to 59 years old in the world
(WHO, 2009)(WHO, 2009)
- 10,000,000 20,000,000 30,000,000 40,000,000 50,000,000 60,000,000 70,000,000
Iron deficiency
Physical inactivity
High cholesterol
Overweight and obesity
High blood pressure
Occupational risks
High blood glucose
Tobacco use
Unsafe sex
Alcohol use

Distribution of alcohol-attributable male Distribution of alcohol-attributable male deaths (of all male deaths)deaths (of all male deaths)
Distribution of alcohol-attributable male Distribution of alcohol-attributable male deaths (of all male deaths)deaths (of all male deaths)

Effective prevention policy measures Effective prevention policy measures existexist
Effective prevention policy measures Effective prevention policy measures existexist
Regulating and restricting availability of alcoholic beverages;
Reducing demand through taxation and pricing mechanisms;
Regulating the marketing of alcoholic beverages (in particular to younger people);
Enacting appropriate drink-driving policies;
Raising awareness and support for effective policies.
Implementing screening programmes and brief interventions for hazardous and harmful use of alcohol.

Global strategy to reduce Global strategy to reduce the harmful use of alcoholthe harmful use of alcohol Global strategy to reduce Global strategy to reduce the harmful use of alcoholthe harmful use of alcohol
Developed through a long and intense collaboration between the WHO Secretariat and Member States.
Incorporates, when relevant and appropriate, the outcomes of consultations with stakeholders, including the industry and NGOs.
Represents a unique consensus among WHO 194 Member States on ways to tackle harmful use of alcohol at all levels.
Definition of "harmful use of alcohol" in Definition of "harmful use of alcohol" in the WHO global strategythe WHO global strategy
Definition of "harmful use of alcohol" in Definition of "harmful use of alcohol" in the WHO global strategythe WHO global strategy
Drinking that causes detrimental health and social consequences for
– the drinker– people around the drinker and – society at large.
Patterns of drinking that are associated with increased risk of adverse health outcomes ("hazardous use")
– Level and pattern of alcohol consumption• Heavy episodic drinking
WHO Global strategy to reduce the WHO Global strategy to reduce the harmful use of alcohol: five objectivesharmful use of alcohol: five objectivesWHO Global strategy to reduce the WHO Global strategy to reduce the
harmful use of alcohol: five objectivesharmful use of alcohol: five objectives
(a) raised global awareness of the magnitude and nature of the health, social and economic problems caused by harmful use of alcohol, and increased commitment by governments to act to address the harmful use of alcohol;
(b) strengthened knowledge base on the magnitude and determinants of alcohol-related harm and on effective interventions to reduce and prevent such harm;
(c) increased technical support to, and enhanced capacity of, Member States for preventing the harmful use of alcohol and managing alcohol-use disorders and associated health conditions;
(d) strengthened partnerships and better coordination among stakeholders and increased mobilization of resources required for appropriate and concerted action to prevent the harmful use of alcohol;
(e) improved systems for monitoring and surveillance at different levels, and more effective dissemination and application of information for advocacy, policy development and evaluation purposes.
What actions are needed to reduce What actions are needed to reduce the harmful use of alcohol?the harmful use of alcohol?
What actions are needed to reduce What actions are needed to reduce the harmful use of alcohol?the harmful use of alcohol?
Global, regional and national actions on:– levels of alcohol consumption– patterns of alcohol consumption– contexts of alcohol consumption– wider social determinants of health
Special attention needs to be given to reducing harm to people other than the drinker and to populations that are at particular risk from harmful use of alcohol.
The content of the strategyThe content of the strategyThe content of the strategyThe content of the strategy
The global strategy: – complements and supports public
health policies in Member States;
– gives guidance for action at all levels;
– sets priority areas for global action;
– contains a portfolio of policy options and measures that could be considered for implementation and adjusted as appropriate at the national level
National policies and measuresNational policies and measuresNational policies and measuresNational policies and measures
Member States have a primary responsibility for formulating, implementing, monitoring and evaluating public policies to reduce the harmful use of alcohol. Such policies require a wide range of public health-oriented strategies for prevention and treatment.
All countries will benefit from having a national strategy and appropriate legal frameworks to reduce harmful use of alcohol, regardless of the level of resources in the country.
Sustained political commitment, effective coordination, sustainable funding and appropriate engagement of subnational governments as well as from civil society and economic operators are essential for success.
Health ministries have a crucial role in bringing together the other ministries and stakeholders needed for effective policy design and implementation.

Regional initiatives Regional initiatives following the global strategyfollowing the global strategy
Regional initiatives Regional initiatives following the global strategyfollowing the global strategy
Regional office for Africa– Reduction of the harmful use of alcohol:
A strategy for the WHO African Region
Regional office for the Americas/PAHO– Plan of Action to Reduce the Harmful Use of Alcohol
Regional office for Europe– European action plan to reduce
the harmful use of alcohol 2012–2020

Priority areas for global actionPriority areas for global action
Public health advocacy and partnership
Technical support and capacity building
Production and dissemination of knowledge
Resource mobilization

Recommended ten target areas for policy Recommended ten target areas for policy measures and interventionsmeasures and interventions
Recommended ten target areas for policy Recommended ten target areas for policy measures and interventionsmeasures and interventions
1. Leadership, awareness and commitment
2. Health services' response
3. Community action
4. Drink-driving policies and countermeasures
5. Availability of alcohol
6. Marketing of alcoholic beverages
7. Pricing policies
8. Reducing the negative consequences of drinking and alcohol intoxication
9. Reducing the public health impact of illicit alcohol and informally produced alcohol
10. Monitoring and surveillance
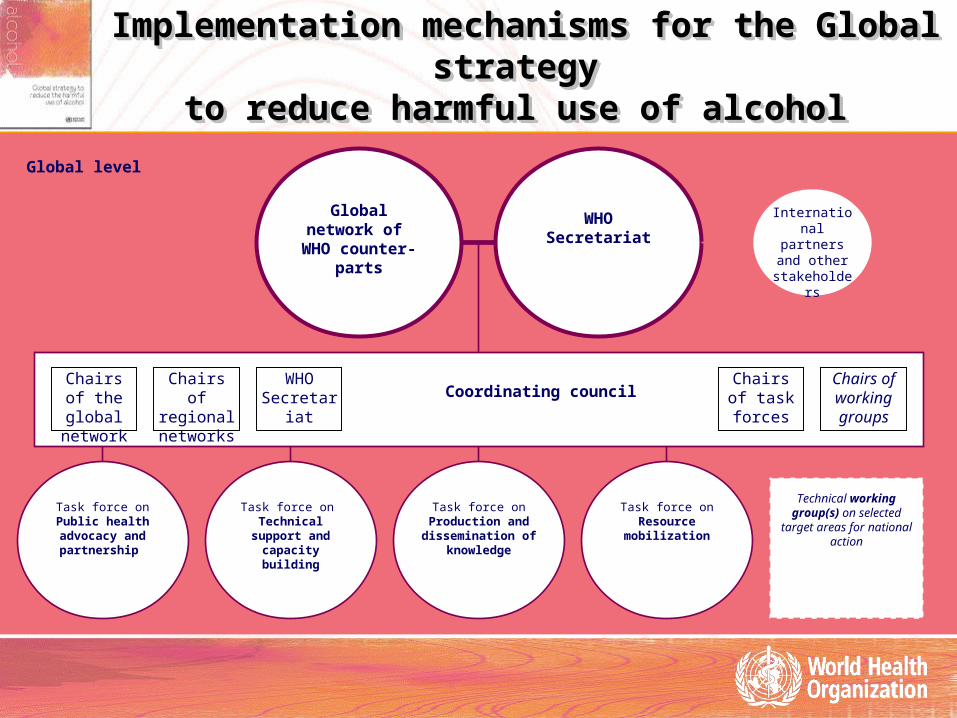
Implementation mechanisms for the Global strategy Implementation mechanisms for the Global strategy
to reduce harmful use of alcohol to reduce harmful use of alcohol
Implementation mechanisms for the Global strategy Implementation mechanisms for the Global strategy
to reduce harmful use of alcohol to reduce harmful use of alcohol
Global network of
WHO counter-parts
WHOSecretariat
Global level
Coordinating council
Task force on Public health advocacy and
partnership
Chairs of the global network
Chairs of regional networks
Chairs of task forces
WHO Secretariat
Chairs of working groups
Task force on Technical support
and capacity building
Task force on Resource
mobilization
Task force on Production and
dissemination of knowledge
International partners and
other stakeholders
Technical working group(s) on selected
target areas for national action

WHO global counterparts networkWHO global counterparts networkfirst meeting 8-11 February 2011first meeting 8-11 February 2011
WHO global counterparts networkWHO global counterparts networkfirst meeting 8-11 February 2011first meeting 8-11 February 2011
Advocacy, partnerships and resource mobilization
Advocacy, partnerships and resource mobilization
Support for the Global network of WHO national counterparts and collaborative implementation (WHO Secretariat- MS) mechanisms (task forces and the working groups)
– Meetings of the Coordinating Council (2012, 2013)– Second meeting of the Global network (2013)
Co-hosting Global Alcohol Policy Conference (Thailand, 13-15 February 2012)
Implementation/action plan elaborated in collaboration with MS, published and disseminated
Interagency UN task force on implementation of the global strategy (2012)
Meeting of interested parties (2012)
Global Alcohol Policy Conference Global Alcohol Policy Conference co-hosted by WHOco-hosted by WHO
Bangkok, Thailand, 13-15 February 2012, Bangkok, Thailand, 13-15 February 2012,
Global Alcohol Policy Conference Global Alcohol Policy Conference co-hosted by WHOco-hosted by WHO
Bangkok, Thailand, 13-15 February 2012, Bangkok, Thailand, 13-15 February 2012, 1216 participants from more
than 50 countries
Participants of the Conference adopted the Declaration calling on intergovernmental agencies, NGO networks, governments, academia, civil society, professional organizations, communities, and individuals, at all levels to take action
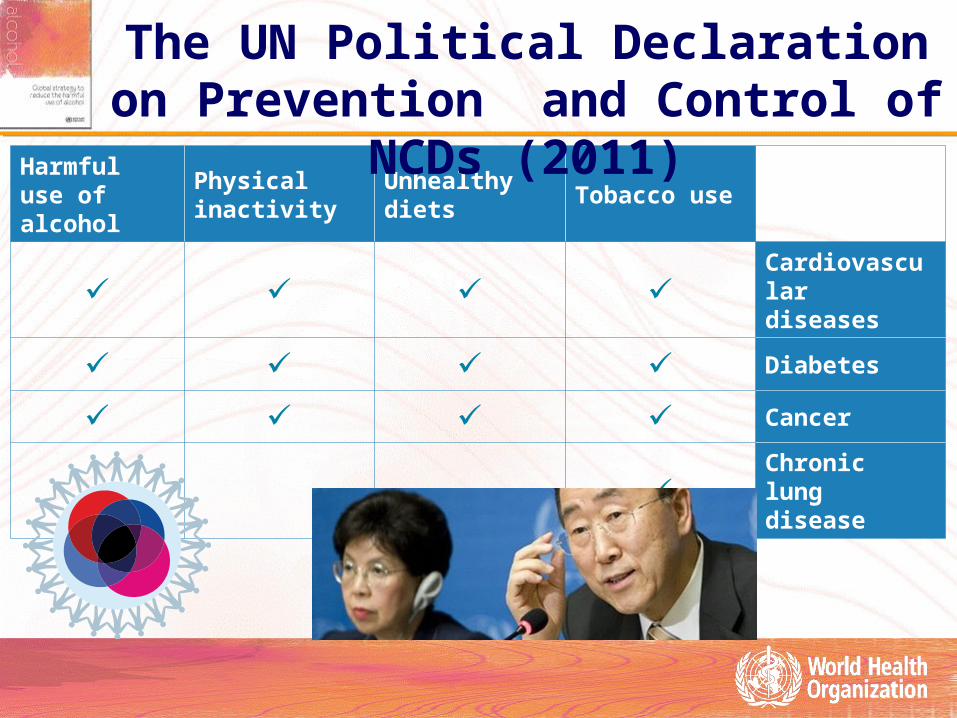
Tobacco useUnhealthy dietsPhysical inactivity
Harmful use of alcohol
Cardiovascular diseases
DiabetesCancerChronic lung disease
The UN Political Declaration on Prevention and Control of NCDs (2011)
UN Political Declaration on Prevention and UN Political Declaration on Prevention and Control of NCDs (2011)Control of NCDs (2011)
UN Political Declaration on Prevention and UN Political Declaration on Prevention and Control of NCDs (2011)Control of NCDs (2011)
…underline the importance for MS to continue addressing common risk factors for non-communicable diseases through the implementation of the World Health Organization … Global Strategy for the Prevention and Control of Non-communicable Diseases as well as the Global Strategy on Diet, Physical Activity and Health and the Global Strategy to Reduce the Harmful Use of Alcohol;
Promote the implementation of the WHO Global Strategy to Reduce the Harmful Use of Alcohol…as well as raise awareness of the problems caused by the harmful use of alcohol, particularly among young people, and call upon WHO to intensify efforts to assist Member States in this regard…
Building capacity for national actionBuilding capacity for national actionBuilding capacity for national actionBuilding capacity for national action
This aim will be achieved through three outputs:
Development of technical tools for the 10 different areas for alcohol policy development listed in the global alcohol strategy
Regional capacity building workshops for training of national civil servants (national counterparts on alcohol, NCD focal points or other relevant government officials).
Direct technical support in selected countries.
Department of Mental Health and Substance Abuse
Draft 4/19/2012
BUIL DING CAPACITY
FOR NATIONAL
AL COHOL POL ICIES PROJ ECT PLAN, phase 1: Addressing the harmful use of alcohol as a risk factor for noncommunicable diseases (NCDs)

Production and dissemination of knowledge
Production and dissemination of knowledge
WHO Research initiative on Alcohol, Health and Development– Global prevalence study on Fetal Alcohol Spectrum Disorder (FASD)
• To be implemented first in selected countries of Europe and Africa– International study "Harm to others"
• To be implemented in selected countries of Asia, Africa, Americas and Europe– Internataional research project on alcohol and infections diseases
• To be developed and implemented in HIV/AIDS and TB high prevalence countries of Africa and Europe
Supporting production and dissemination of new GBD/CRA estimates of alcohol-attributable burden
– Meeting of the WHO Reference Group on Alcohol Epidemiology (2012-early 2013)
Global Survey on Alcohol and Health 2012 – launched 24 January 2012– Web-based (Datacol) data collection in collaboration with the regional offices
Global Information System on Alcohol and Health– Full integration with regional information systems on alcohol and health (2012)– Preparation of the Global Status Report on Alcohol and Health (2013-2014)

E-health project on alcohol and healthE-health project on alcohol and healthE-health project on alcohol and healthE-health project on alcohol and health

Global Information System on Alcohol and Health (GISAH)
Global Information System on Alcohol and Health (GISAH)
There are over 200 indicators on GISAH.
Data can be exported as EXCEL files.
Definitions for each indicator are provided through a link to the WHO Indicator and Measurement Registry (IMR). This allows downloading of an Indicator booklet of GISAH indicators.
Indicators can be highlighted on the theme page including interactive maps. Static maps are accessible in the Global Health Observatory Map Gallery.
Country profiles can be downloaded from the theme page.
http://www.who.int/gho/alcoholhttp://www.who.int/gho/alcohol

Realizing the commitments included in the UN Political Declaration on NCDs:
Developing a global monitoring framework and targets for NCDs
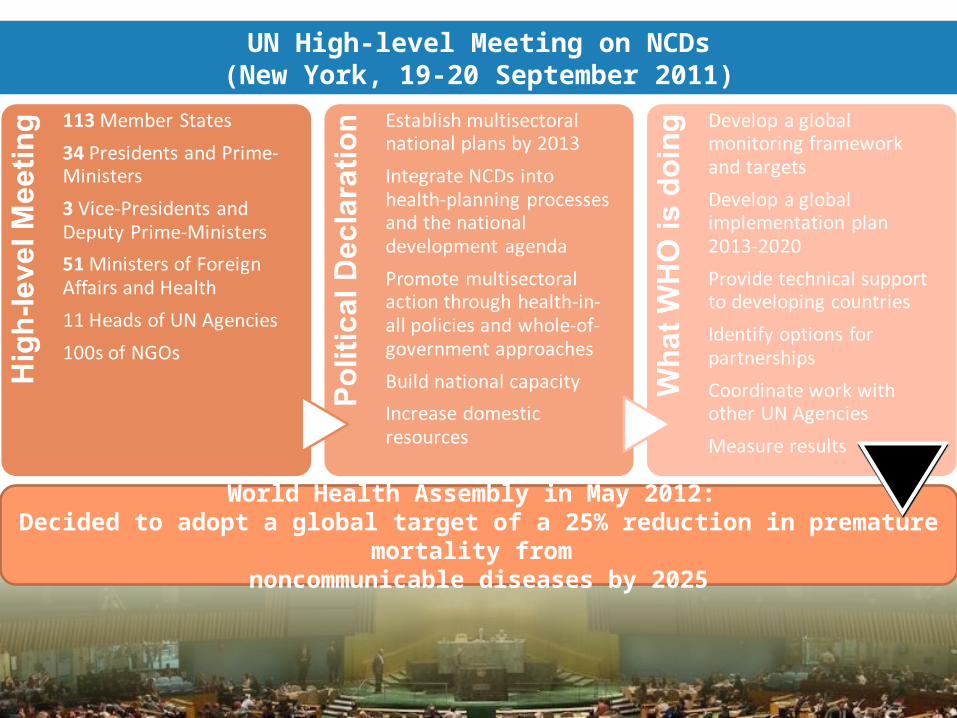
UN High-level Meeting on NCDs(New York, 19-20 September 2011)
World Health Assembly in May 2012: Decided to adopt a global target of a 25% reduction in premature mortality from
noncommunicable diseases by 2025
Draft indicators and targets on alcoholDraft indicators and targets on alcoholDraft indicators and targets on alcoholDraft indicators and targets on alcohol
Indicator: Total (recorded and unrecorded) adult (persons aged 15+ years) per capita consumption (APC) of pure litres of alcohol within the calendar year.
Target: 10 per cent relative reduction in total APC.
Suggested alternatives:– Indicators of pattern of drinking (e.g. heavy episodic drinking)– Indicators of alcohol-related harm (e.g. prevalence/incidence of
alcohol psychoses or alcohol liver cirrhosis)– Policy-related process indicators

Key professes and milestones in developing global Key professes and milestones in developing global monitoring framework with indicators and targets monitoring framework with indicators and targets
Key professes and milestones in developing global Key professes and milestones in developing global monitoring framework with indicators and targets monitoring framework with indicators and targets
Informal consultations organized by the WHO Secretariat (2012, ongoing)
National consultation processes
Discussion at the Regional committees in all six WHO regions
Formal consultation with Member States at WHO HQ, Geneva, 5-7 November 2012
Executive Board Meeting (January 2013) and 66th WHA (May 2013)

Development of the WHO Global Mental Development of the WHO Global Mental Health Action PlanHealth Action Plan
Development of the WHO Global Mental Development of the WHO Global Mental Health Action PlanHealth Action Plan
Mandated by the 65th World Health Assembly resolution adopted in May 2012
In the process of development in intense consultations with Member States and other stakeholders, also at the regional level
Mental health conditions include alcohol use disorders
To be submitted to the 66th World Health Assembly through the Executive Board (January 2013)

ConclusionsConclusionsConclusionsConclusions
Harmful use of alcohol should be a continuing concern at local, national, regional and global levels with political and professional attention and allocation of resource in line with the magnitude of the problem.
The global strategy represents a unique opportunity historically for sustainable actions to reduce the harmful use of alcohol.
Thank you for your attention
Further information at:
http://www.who.int/substance_abuse/
Top Related