







Languages
Pages
Legal

Recommendation to ACHDNC regarding Newborn Screening for Spinal Muscular Atrophy
Beth Tarini M.D., M.S. Dietrich Matern M.D., Ph.D.
Committee Representatives to the Condition Review Workgroup
ACHDNC Meeting February 8, 2018 Not for distribution without permission.
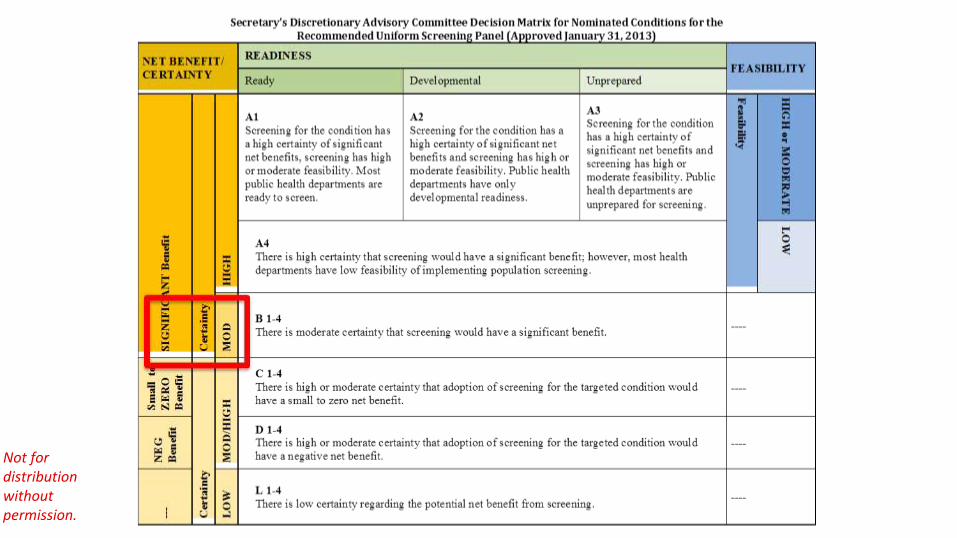
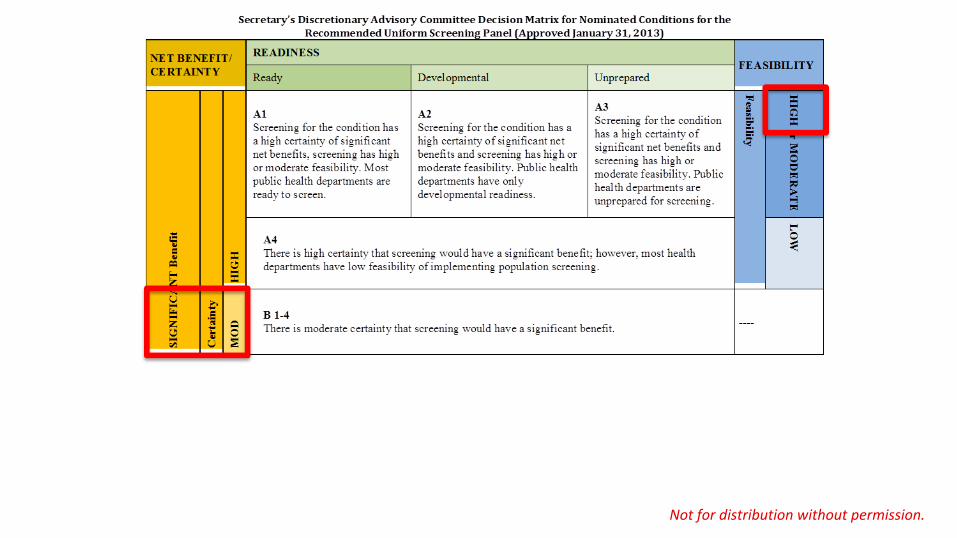
Decision Matrix • Magnitude and certainty of the net benefit of
screening for SMA to the population of affectednewborns.
• Feasibility of newborn screening for SMA.
• Readiness of states to implement population-widescreening for SMA.
Not for distribution without permission.

Not for distribution without permission.
Spinal Muscular Atrophy (SMA)
• Autosomal recessive inheritance.
• Majority of SMA patients are homozygous for adeletion of exon 7 of SMN1 independent of severity(5% of cases are compound heterozygotes).
• Incidence estimated at 1 in 10,000 live births.
• Carrier frequency of 1 in 40 – 80 live births.
• SMN2 copy number modifies the severity of disease.Not for distribution without permission.
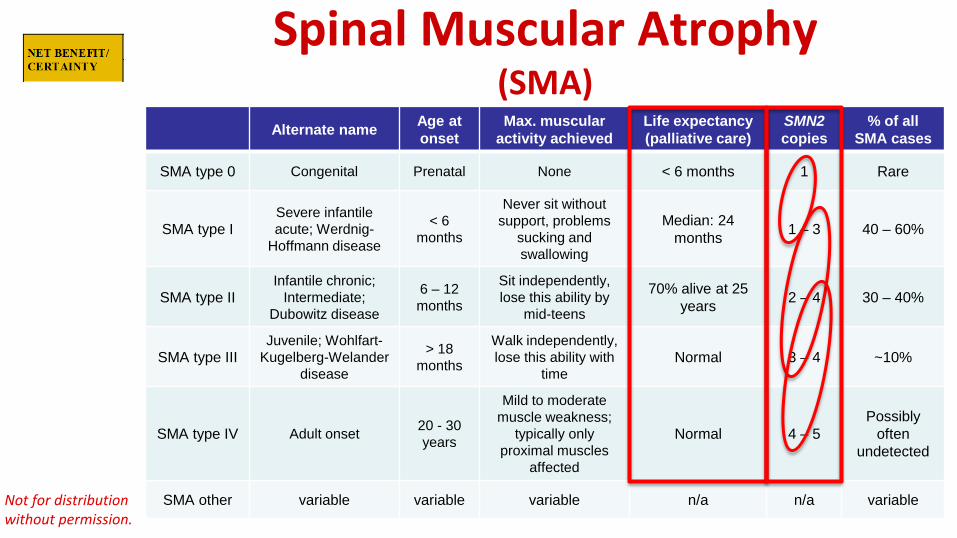
Spinal Muscular Atrophy (SMA)
Alternate name Age at onset
Max. muscular activity achieved
Life expectancy (palliative care)
SMN2 copies
% of all SMA cases
SMA type 0 Congenital Prenatal None < 6 months 1 Rare
SMA type I Severe infantile acute; Werdnig-
Hoffmann disease
< 6 months
Never sit without support, problems
sucking and swallowing
Median: 24 months 1 – 3 40 – 60%
SMA type II Infantile chronic;
Intermediate; Dubowitz disease
6 – 12 months
Sit independently, lose this ability by
mid-teens
70% alive at 25 years 2 – 4 30 – 40%
SMA type III Juvenile; Wohlfart-
Kugelberg-Welander disease
> 18months
Walk independently, lose this ability with
time Normal 3 – 4 ~10%
SMA type IV Adult onset 20 - 30 years
Mild to moderate muscle weakness;
typically only proximal muscles
affected
Normal 4 – 5 Possibly
often undetected
SMA other variable variable variable n/a n/a variable Not for distribution without permission.

Spinal Muscular Atrophy (SMA)
Alternate name Age at onset
Max. muscular activity achieved
Life expectancy (palliative care)
SMN2 copies
% of all SMA cases
SMA type 0 Congenital Prenatal None < 6 months 1 Rare
SMA type I Severe infantile acute; Werdnig-
Hoffmann disease
< 6 months
Never sit without support, problems
sucking and swallowing
Median: 24 months 1 – 3 40 – 60%
SMA type II Infantile chronic;
Intermediate; Dubowitz disease
6 – 12 months
Sit independently, lose this ability by
mid-teens
70% alive at 25 years 2 – 4 30 – 40%
SMA type III Juvenile; Wohlfart-
Kugelberg-Welander disease
> 18months
Walk independently, lose this ability with
time Normal 3 – 4 ~10%
SMA type IV Adult onset 20 - 30 years
Mild to moderate muscle weakness;
typically only proximal muscles
affected
Normal 4 – 5 Possibly
often undetected
SMA other variable variable variable n/a n/a variable Not for distribution without permission.
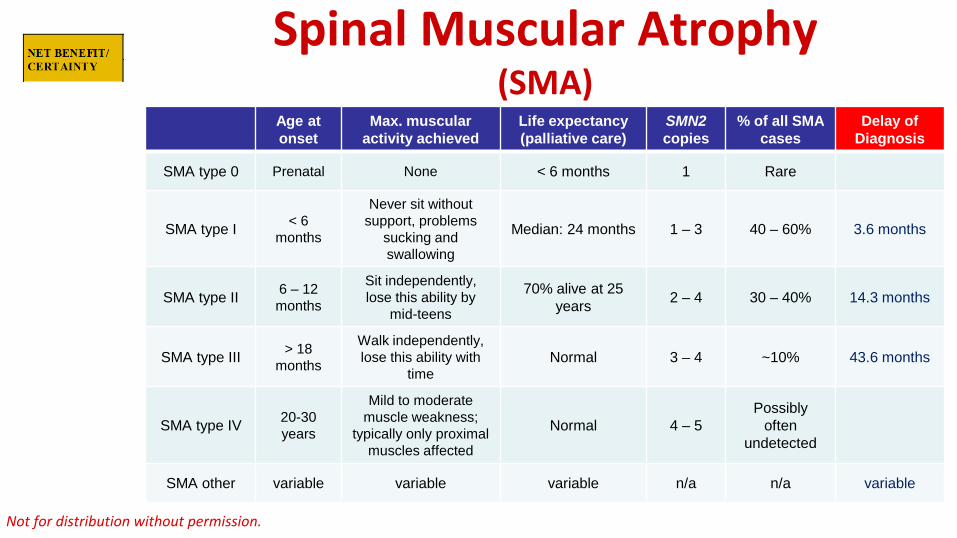
Spinal Muscular Atrophy (SMA)
Age at onset
Max. muscular activity achieved
Life expectancy (palliative care)
SMN2 copies
% of all SMA cases
Delay of Diagnosis
SMA type 0 Prenatal None < 6 months 1 Rare
SMA type I < 6 months
Never sit without support, problems
sucking and swallowing
Median: 24 months 1 – 3 40 – 60% 3.6 months
SMA type II 6 – 12 months
Sit independently, lose this ability by
mid-teens
70% alive at 25 years 2 – 4 30 – 40% 14.3 months
SMA type III > 18months
Walk independently, lose this ability with
time Normal 3 – 4 ~10% 43.6 months
SMA type IV 20-30years
Mild to moderate muscle weakness;
typically only proximal muscles affected
Normal 4 – 5 Possibly
often undetected
SMA other variable variable variable n/a n/a variable
Not for distribution without permission.
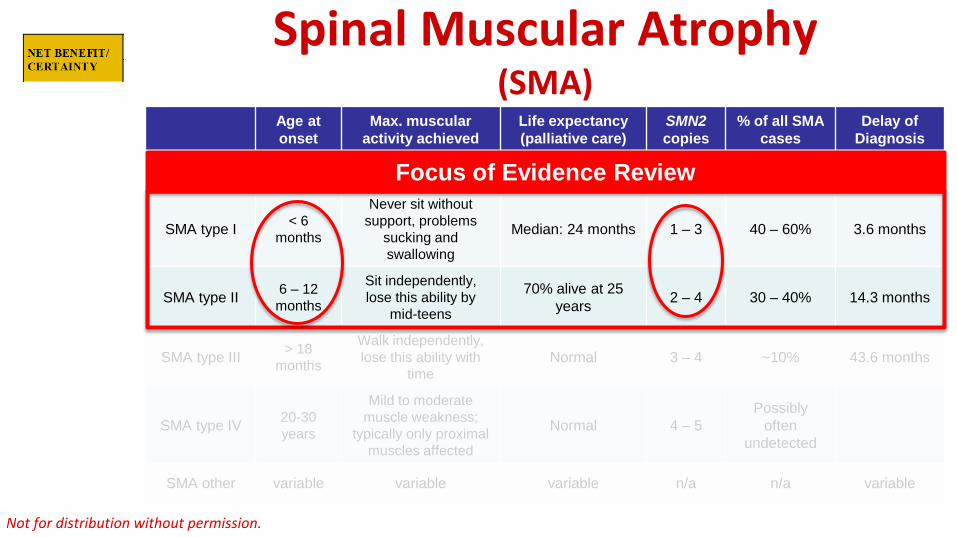
Spinal Muscular Atrophy (SMA)
Age at onset
Max. muscular activity achieved
Life expectancy (palliative care)
SMN2 copies
% of all SMA cases
Delay of Diagnosis
SMA type 0 Prenatal None < 6 months Rare
SMA type I < 6 months
Never sit without support, problems
sucking and swallowing
Median: 24 months 1 – 3 40 – 60% 3.6 months
SMA type II 6 – 12 months
Sit independently, lose this ability by
mid-teens
70% alive at 25 years 2 – 4 30 – 40% 14.3 months
SMA type III > 18months
Walk independently, lose this ability with
time Normal 3 – 4 ~10% 43.6 months
SMA type IV 20-30years
Mild to moderate muscle weakness;
typically only proximal muscles affected
Normal 4 – 5 Possibly
often undetected
SMA other variable variable variable n/a n/a variable
Focus of Evidence Review
Not for distribution without permission.

Treatment • Palliative/symptomatic (ventilator, gastrostomy
feeding, physical therapy).
• Nusinersen (only FDA approved SMA-specific treatment).
• Gene therapy (ongoing trial).
Not for distribution without permission.
Treatment Nusinersen (SpinrazaTM):
– The only FDA approved SMA-specific treatment.
– Intrathecal administration (6 doses in 1st year, then 1 doseevery 4 months).
– Expensive (reported cost: $125,000 per vial/dose).
– Limited data available suggest that treatment effect isgreater when:• initiated before symptoms develop,
• more SMN2 copies are present (likely because later onset andmilder phenotype). Not for distribution without permission.

Treatment Nusinersen (SpinrazaTM):
Limitations of treatment studies: • No data on long term outcomes (follow up limited to ≤2 years).
• Small study populations (20 presymptomatically treated infants).
• Anecdotally, 1 patient with two SMN2 copies had normaldevelopment at 12 months old (treatment started at 13 days oldfollowing positive NBS in NY; Kraszewski JN et al. Genet Med.doi:10.1038/gim.2017.152).
• No peer reviewed publications available on presymptomaticallytreated patients.
Not for distribution without permission.
Treatment Nusinersen (SpinrazaTM):
– Peer reviewed treatment guideline not (yet) published.
– Draft guideline has been developed by an “SMA NBSMultidisciplinary Working Group” using a modified versionof the Delphi technique to reach consensus
Not for distribution without permission.

Treatment Nusinersen (SpinrazaTM):
– Peer reviewed treatment guideline not (yet) published.
– Summary of draft guideline by Glascock J et al.:
“Probable” because SMA types cannot be reliably differentiated by SMN2 copy number. Presymptomatic treatment outcomes can therefore not be reliably assigned to SMA type.
Not for distribution without permission.
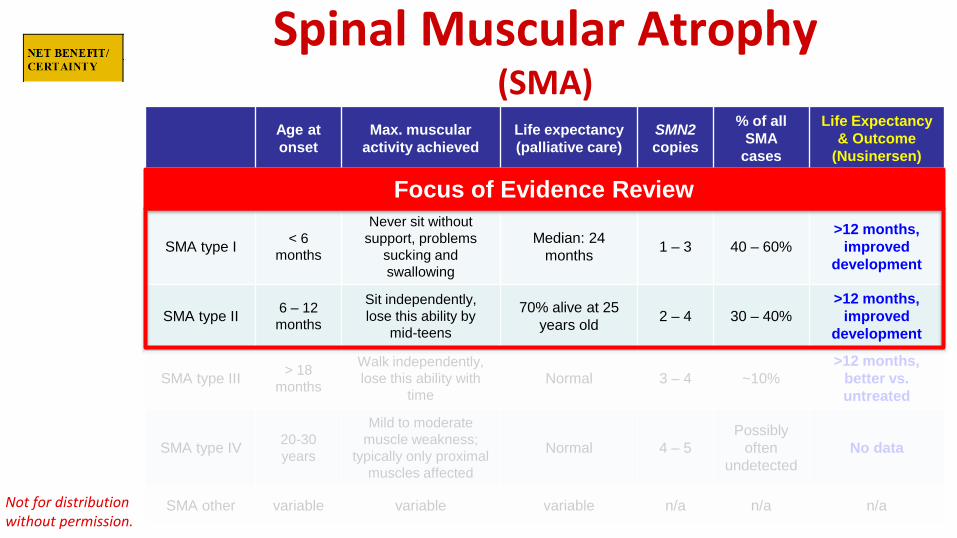
Spinal Muscular Atrophy (SMA)
Age at onset
Max. muscular activity achieved
Life expectancy (palliative care)
SMN2 copies
% of all SMA
cases
Life Expectancy & Outcome
(Nusinersen)
SMA type 0 Prenatal None < 6 months Rare
SMA type I < 6 months
Never sit without support, problems
sucking and swallowing
Median: 24 months 1 – 3 40 – 60%
>12 months,improved
development
SMA type II 6 – 12 months
Sit independently, lose this ability by
mid-teens
70% alive at 25 years old 2 – 4 30 – 40%
>12 months,improved
development
SMA type III > 18months
Walk independently, lose this ability with
time Normal 3 – 4 ~10%
>12 months,better vs.untreated
SMA type IV 20-30years
Mild to moderate muscle weakness;
typically only proximal muscles affected
Normal 4 – 5 Possibly
often undetected
No data
SMA other variable variable variable n/a n/a n/a
Focus of Evidence Review
Not for distribution without permission.
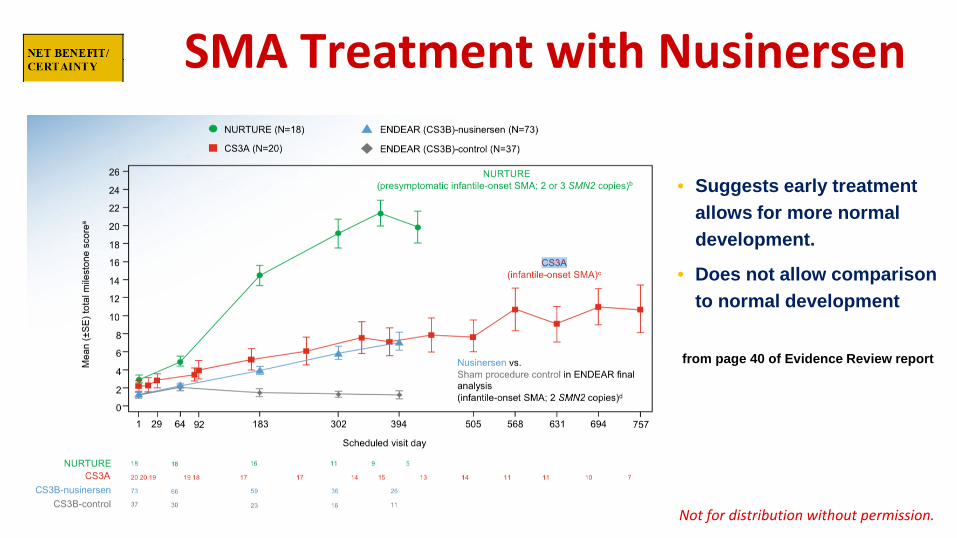
SMA Treatment with Nusinersen
• Suggests early treatmentallows for more normaldevelopment.
• Does not allow comparisonto normal development
from page 40 of Evidence Review report
Not for distribution without permission.
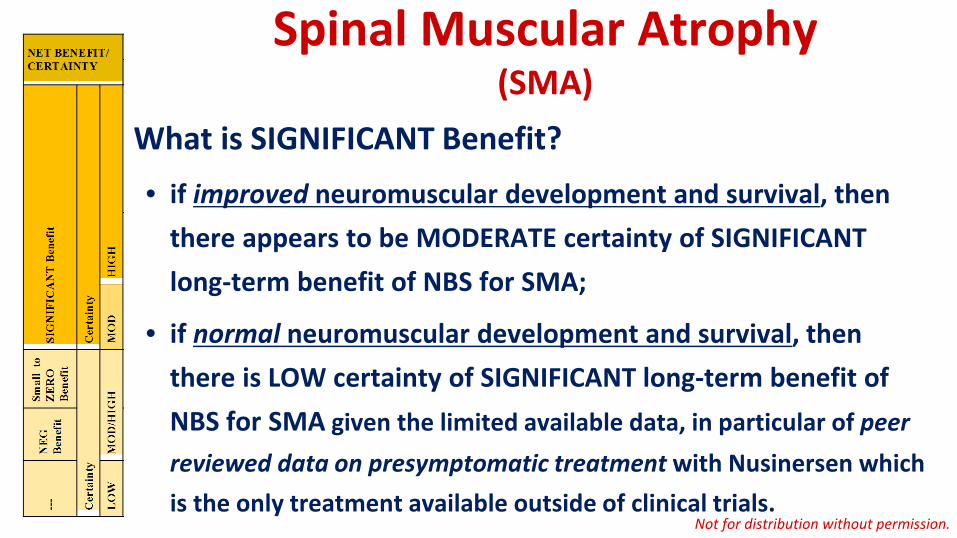
Spinal Muscular Atrophy (SMA)
What is SIGNIFICANT Benefit? • if improved neuromuscular development and survival, then
there appears to be MODERATE certainty of SIGNIFICANTlong-term benefit of NBS for SMA;
• if normal neuromuscular development and survival, thenthere is LOW certainty of SIGNIFICANT long-term benefit ofNBS for SMA given the limited available data, in particular of peerreviewed data on presymptomatic treatment with Nusinersen whichis the only treatment available outside of clinical trials.
Not for distribution without permission.
Not for distribution without permission.
Newborn Screening for SMA Newborn screening test is available:
– real-time PCR assay specific for exon 7 deletion in SMN1,
– expected to identify at least 95% of SMA cases,
– will miss ca. 5% of SMA cases that are not homozygous forexon 7 deletion unless:• carriers for the deletion will be reported (most will not harbor a 2nd mutation),
• a 2nd tier test is performed to rule out a 2nd pathogenic (!) mutation.
Not for distribution without permission.
Not for distribution without permission.

Newborn Screening for SMA most NBS programs
could implement screening within 1 year after the
state makes the decision to
include the condition and
funding is made available.
most NBS programs face barriers that
would require 1–3 years
to address.
most NBS programs
would take longer than 3
years to implement,
even with the decision to add the condition
and the availability of
funding to begin
comprehensive screening.
Not for distribution without permission.
Newborn Screening for SMA
Newborn screening test is available – test can be multiplexed with SCID screening test;
– CDC’s Newborn Screening Quality Assurance Program (NSQAP) can providetraining, quality control and reference materials;
– incremental cost is small when multiplexed with SCID screening assay;
– higher incremental cost if 100% sensitivity is expected because:
• 2nd tier test needed on ca. 1 in 60 newborns heterozygous for exon 7 deletion, or
• ca. 1 in 60 newborns will require follow up but are only carriers.Not for distribution without permission.
Newborn Screening for SMA
Newborn screening tests are available and used already: – pilot study with consent in 3 hospitals in New York City (1:72 carriers);
– MA began in January 2018 (consent; no carriers identified; not multiplexed);
– Utah began 1/29/2018 (no consent; no carriers identified; multiplexed with SCID);
– Minnesota to begin in March 2018 (no consent; no carriers will be identified;multiplexed with SCID);
– WI to begin in 2018; MO to begin in 2019; NC to begin pilot study in April 2018;
– APHL’s PHSI Assessment found:• majority of states can implement within 1-3 years;
• addition of SMA to RUSP would “bolster implementation activities.” Not for distribution without permission.

NBS Programs with Mandates/Pilots State SMA added to
NBS panel Start Select or Whole Population Funds Carriers Costs
MA 12/5/2015 (Adv. Cmte.) 1/29/2018 Whole, consent,
PILOT N/A Not identified n/a
MN 12/27/2018 3/5/2018 Whole NBS fee Not identified < $1.00
MO 7/11/2017 (Senate Bill 50)
Must start by 1/1/2019
Whole, likely no reporting initially NBS fee Decision expected
4/2018 ~$1.00
NC - Apr 2018 Select, consent, PILOT NICHD contract
Not reported or identified n/a
NY - Jan 2016 3 hospitals, consent, PILOT Biogen Reporting for pilot;
undecided future 0.15-$1.00
UT August 2017 (Rule R438-15) 1/29/2018 Whole NBS fee Not identified TBD
WI Expected for July 2018
TBD (likely before
7/2019) Whole
Cure SMA as bridge funding
Not identified $1.00
modified from APHL PHSI report Not for distribution without permission.
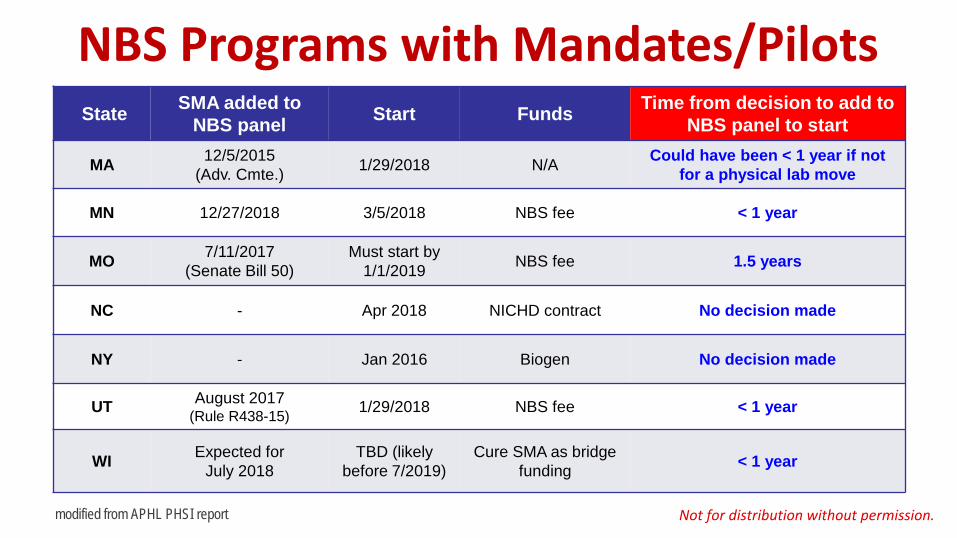
NBS Programs with Mandates/Pilots State SMA added to
NBS panel Start Funds Time from decision to add to NBS panel to start
MA 12/5/2015 (Adv. Cmte.) 1/29/2018 N/A Could have been < 1 year if not
for a physical lab move
MN 12/27/2018 3/5/2018 NBS fee < 1 year
MO 7/11/2017 (Senate Bill 50)
Must start by 1/1/2019 NBS fee 1.5 years
NC - Apr 2018 NICHD contract No decision made
NY - Jan 2016 Biogen No decision made
UT August 2017 (Rule R438-15) 1/29/2018 NBS fee < 1 year
WI Expected for July 2018
TBD (likely before 7/2019)
Cure SMA as bridge funding < 1 year
modified from APHL PHSI report Not for distribution without permission.

Not for distribution without permission.

• Do we need to wait for peer reviewed guidelines for the management of specific SMA types?
• What role do disclosure (or not) of carriers and cost of treatment play in the decision?Not for distribution without permission.

• Do we need to wait for peer reviewed guidelines for the management of specific SMA types?
• What role do disclosure (or not) of carriers and cost of treatment play in the decision?
NO
NONE
Not for distribution without permission.
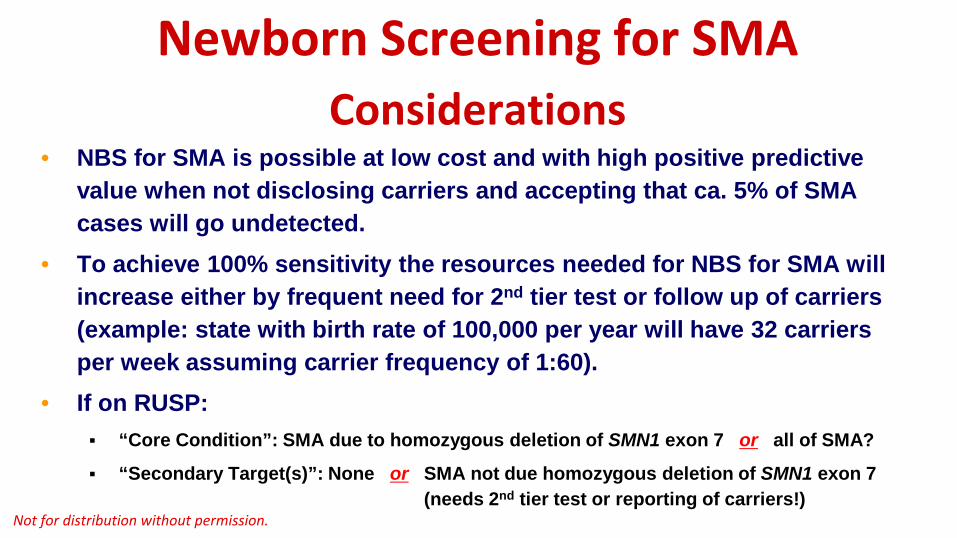
Newborn Scree
ning for SMA Considerations
• NBS for SMA is possible at low cost and with high positive predictivevalue when not disclosing carriers and accepting that ca. 5% of SMAcases will go undetected.
• To achieve 100% sensitivity the resources needed for NBS for SMA willincrease either by frequent need for 2nd tier test or follow up of carriers(example: state with birth rate of 100,000 per year will have 32 carriersper week assuming carrier frequency of 1:60).
• If on RUSP: “Core Condition”: SMA due to homozygous deletion of SMN1 exon 7 or all of SMA?
“Secondary Target(s)”: None or SMA not due homozygous deletion of SMN1 exon 7(needs 2nd tier test or reporting of carriers!)
Not for distribution without permission.

• Follow up protocols are needed for: Patients with four or more SMN2 copies to determine when to start treatment
(draft exists: Glascock et al.)
Patients on treatment (to justify to insurance continuation of treatment)
Newborn Scree
ning for SMA Considerations
• NBS would likely show that the majority of SMA cases have SMAtype II, III or IV
• SMA types II and III are likely to benefit the most from earlytreatment
most patients with SMA will benefit from early treatment!
Not for distribution without permission.
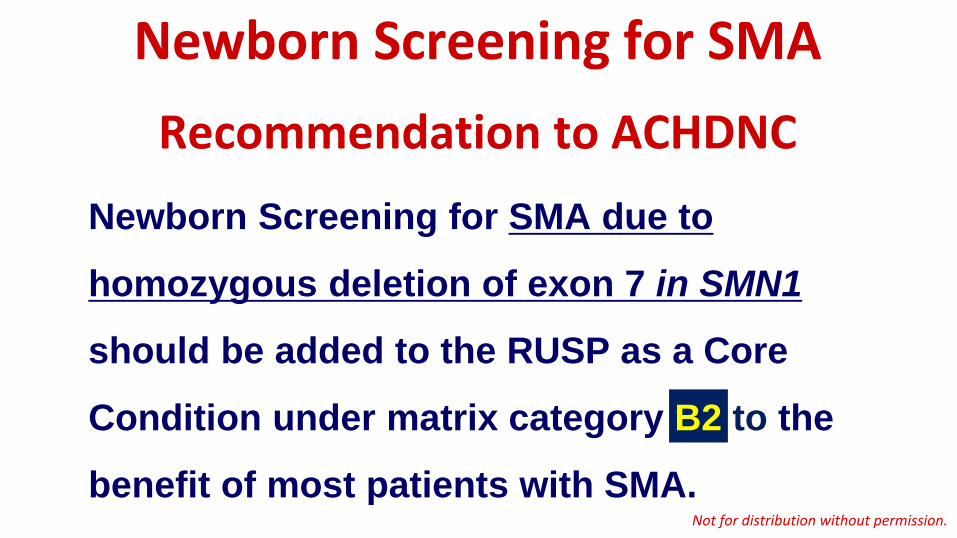
Newborn Screening for SMA Recommendation to ACHDNC
Newborn Screening for SMA due to
homozygous deletion of exon 7 in SMN1
should be added to the RUSP as a Core
Condition under matrix category B2 to the
benefit of most patients with SMA. Not for distribution without permission.
Top Related