






Languages
Pages
Legal

7/31/2019 Prodromal Schizophrenia
1/13
Prodromal schizophrenia: To treat or not to treat?
Rupert Kelly PrizeAlhafidz Hamdan, MRes (Neuroscience)
Stage 4 MBBS, Newcastle University
7/31/2019 Prodromal Schizophrenia
2/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 1
Content
Introduction.. 2
The ethics of early interventions in prodromal schizophrenia. 3
Principles of prodromal schizophrenia.. 3
The potential benefits of being at risk.. 5
Pharmacological interventions. 5
Nonpharmacological interventions
7
The potential risks of being at risk 7
False positives 7
Stigma. 8
Issues regarding confidentiality and autonomy 9
Prodromal intervention: A clinical equipoise 10
References. 11
Cover illustration:Louise Wain (5 Aug 1860 4 July 1939) was an English artist best known for his drawings,
which consistently antropomophised large-eyed cats and kittens. In his later years he suffered from
schizophrenia which, according to some psychologists, can be seen in his works. The image on the cover
illustrates his differing perceptions of a cat as he progressed through the spectrum of schizophrenia from the
premorbid (top left), prodromal (top right), acute (bottom left) and chronic (bottom right) phases.
7/31/2019 Prodromal Schizophrenia
3/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 2
Prodromal schizophrenia: To treat or not to treat?Alhafidz Hamdan, MRes (Neuroscience),
Fourth year medical student, Newcastle University.
Introduction
Sarah* was a 17-year-old student when she first developed a gradual and distinct change in personality in
1964. She was a bright young girl prior to the deterioration, leading the schools cheerleading team to win the
Nationals and being awarded the Best Performing Student at her high school. However, when she entered
university, things started to become different; she was no longer the centre of attention nor the high achieving
teachers pet and this deflated her self-confidence. Little did she know that her life was going to be taken over
by a relentless disease, stripping off her sanity. She began to hear external voices for brief periods of the day
once a week and these voices relentlessly called out her name Sarah, Sarah, Sarahand instructed her to do
things. At times her surroundings would seem unreal to her, she would avoid sunlight which she found
excessive and unbearable and she would experience an unusual sensation in her head a brainstorm,
according to her. She would weep when she was not sad, laugh when not happy. She was understandably
frustrated and decided to quit university, preferring to spend time at a college nearer to home, where she
could seek solace from her parents. Retrospectively it was clear that she was exhibiting prodromal symptoms
of schizophrenia. Back then in the 1960s, it was not so. When she saw a psychiatrist a few months later, he
attributed the symptoms to stress and anxiety and told her to go on a holiday.
Fast-forward 48 years later, Sarah was 65 years old, diagnosed with schizophrenia and living in a psychiatrichospital. She was one of the patients I was privileged to interview during my mental health rotation. As I sat in
front of her for the first time, listening to her talking about faces that she can see behind me, I cannot help
but wonder if something could have been done to prevent the development of her illness. What if she was
identified early on, still a 17-year-old precocious teenager, as having prodromal symptoms and then treated?
Would this have prevented the deterioration or would this label contribute to another potentially equally
devastating downward social trajectory? What if we had an effective treatment for prodromal schizophrenia
without any significant side effects? Do we have enough evidence to conclude that treating patients with
prodromal symptoms is ethically acceptable, beneficial and not detrimental?
In this essay, I will attempt to answer these questions. I begin by introducing the concept of prodromal
schizophrenia and then go on to explore the benefits and the risks of identifying and treating patients with
prodromal schizophrenia.
*The actual name of the patient has been changed to protect her identity
7/31/2019 Prodromal Schizophrenia
4/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 3
The ethics of early interventions in prodromal schizophrenia
Principles of prodromal schizophrenia
Schizophrenia has been conceptualised as a chronic disease with lasting cognitive, social and functional
impairments since dementia praecox was first described at the dawn of the twentieth century. Up until the
1950s Sarah would probably have just been born then those with psychotic illnesses were locked away,
entrapped by the notion that life could not exist beyond the desolate walls of hospitals. With
deinstitutionalisation, while many patients with psychotic illnesses relished the newfound freedom, others
were relegated to lives of poverty, homelessness and loneliness. In the past three decades, schizophrenia
researchers have challenged this notion of inevitable decline, postulating that early interventions may mitigate
deteriorations in psychotic illness and improve functional outcome, providing hope for patients and families.1
Despite the more favourable prognosis for patients with psychotic illness compared to Kraeplins time, the
majority of patients with schizophrenia nowadays never return to their previous state of normal functioning
after the first psychotic episode. Sarahs symptoms were initially intermittent and mild but then progressed to
become constant and severely disabling, which warranted actual disease diagnosis. Indeed, studies have
shown that significant functional deficits present in the psychotic episode may have been inoculated even
before the illness began.2-4
Therefore, it is clear that schizophrenia cannot be defined to begin with the onset of frank psychosis; it is
rather a continuum characterised by premorbid, prodromal, acute and chronic phases. The premorbid phase
encompasses a period of stable social and cognitive deficits, alongside frequent subtle neurological
abnormalities, long preceding the first psychotic episode.5
On the contrary, the prodromal phase is
characterised by its lack of stability, worsening positive and negative symptoms and deteriorating trajectory of
psychosocial impairment, culminating in the onset of frank psychosis.6
After the first psychotic episode, there
comes a period of recurrent exacerbations and remissions as well as ongoing functional decline until an
individual settles into the chronic phase of illness where deficits and symptoms stabilise. While in the latter
two phases (acute and chronic) symptoms are more easily identifiable, the subtle nonspecific symptoms that
first emerge during the prodrome are often overlooked (as in Sarahs case). The failure to recognise these early
changes is particularly concerning as the duration of untreated psychosis (DUP) corresponds significantly to
further functional decline.7
As the prodromes can only be accurately identified retrospectively, research efforts have focussed on
developing measures to predict future psychosis risks with high sensitivity and specificity. The Comprehensive
Assessment of At-Risk Mental State (CAARMS)(Table 1)8
and the Structured Interview of Prodromal Symptoms
(SIPS)9
defined three similar at-risk criteria, which can predict conversion to psychosis at rates as high as 50-
54% over the course of 6 months to 1 year, implying increased sensitivity. In addition, the North American
Prodromal Longitudinal Studies (NAPLS)
10
revealed that individuals who were most likely to convert topsychosis had a family history of psychosis, symptoms of suspiciousness or delusional-like experiences, a
7/31/2019 Prodromal Schizophrenia
5/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 4
decline in social functioning and/or a history of drug abuse; any three combination of these criteria increased
the positive predictive probability up to 80%, suggesting that an algorithm for treatment for those who are at
the highest risks may be developed.
A few months after the first onset of her psychotic symptoms, Sarah presented to the local psychiatrist, who
then attributed her symptoms to stress and anxiety. Had the CAARMS/SIPS/NALPS criteria be applied to her,
she would have qualified for the diagnosis of prodromal schizophrenia. However, the existence of these
criteria would be of little use to her or other patients if early interventions that ensue prove to be ineffective
or worse, detrimental. In Sarahs case, this is unknown since she was not managed prodromal ly. Studies
elucidating the effectiveness of early interventions are thus important; some of them will be discussed in the
next section.
Table 1. Prospective diagnostic criteria for three schizophrenia prodomes.8-10
7/31/2019 Prodromal Schizophrenia
6/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 5
The potential benefits of being at risk
Classifying an individual as being at risk for schizophrenia may usher in possible therapeutic interventions.
Various studies have highlighted the potential of intervening in the early phases of the disease with both
pharmacological and psychosocial treatments. However, relatively few psychopharmacological studies have
assessed patients meeting the prodromal criteria.12-15
Reasons for this include: the short history of prodromal
research, difficulties in sufficient subjects willing to enter a clinical trial for nonspecific symptoms, the majority
of at-risk patients are adolescents and there are many ethical issues associated with performing such studies.
Pharmacological interventions
In 2002, the Personal Assessment and Crisis Evaluation (PACE) study11
randomised 59 individuals meeting the
at-risk criteria with low dose risperidone and cognitive behavioural therapy (CBT) vs needs -based
intervention (NBI) and found that individuals who received the specific treatments were significantly less
likely to develop psychosis at 6 months than those who received NBI only (10 out of 28 people receiving NBI
converted to psychosis compared to 3 of 31 from the intervention group)(Figure 1). However, the difference
was no longer significant at 12 months. Interestingly, during the subsequent 6-month follow-up period, it
appeared that those who did not adhere to risperidone treatment were those who were most likely to convert
to psychosis.
Figure 1. Rate of transition to psychosis in the PACE study.11
NBI: needs-based intervention, SI: specific intervention (low
dose risperidone and cognitive behavioural therapy), SI-NC: SI with no or partial drug compliance and SI-C: SI with full
compliance.
7/31/2019 Prodromal Schizophrenia
7/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 6
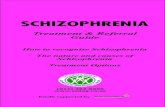
The Prevention through Risk Identification, Management and Education (PRIME) study,12
conducted in 2003 to
further evaluate the benefit of interventions in prodromal schizophrenia, is the only placebo-controlled
double-blinded study of an antipsychotic for the prodromal illness. Olanzapine vs placebo was compared in 60
at-risk individuals over the course of 1 year with subsequent 1-year follow-up. In the placebo group, 38% of
patients converted to psychosis compared to 16% in the olanzapine group and the hazard of conversion
among placebo patients was 2.5 times that of olanzapine-treated patients. However, these were not
statistically significant, probably due to the small sample size. It is interesting however, that all of the
psychoses in the olanzapine group occurred in the first 4 weeks of clinical trial when doses of olanzapine were
relatively low, implying that perhaps those who converted may not have had sufficient time on olanzapine for
it to affect the active processes leading to psychosis. The Global Assessment of Functioning (GAF) score, an
observer rated scale for measuring overall severity of functional impairment, was also non-significant.
Another study from the PRIME clinic (2007)13
included 15 participants in an open-label trial with fixed-flexible
dosing of aripiprazole (5-30 mg/day) for 8 weeks. There was improvement from baseline in the total number of
prodromal symptoms and none of the participants converted to psychosis. While the results are promising, the
significance of these findings is complicated by small sample size and lack of control group and blinding.
Figure 2. Time to onset of psychosis among patients with prodromal psychotic symptoms during 1 year of treatment with
olanzapine or placebo (PRIME study).12
7/31/2019 Prodromal Schizophrenia
8/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 7
Nonpharmacological interventions
In the three studies mentioned above, the benefits of nonpharmacological interventions were either not
assessed (in the case of the PRIME studies12,13
) or insufficiently analysed (in the PACE study,11
the relative
contributions of risperidone treatment and CBT were not investigated). Perhaps, some patients could betreated with psychological therapy alone as a first-line therapy. The Early Detection and Intervention
Evaluation (EDIE) trial14
randomised 58 people with prodromal symptoms to 6 months of CBT or a monitoring
group. The CBT group had a lower risk for conversion to psychosis at 1-year follow-up and displayed fewer
indicators toward conversion on all outcome measures. However, an analysis of the EDIE data in the Cochrane
report15
stated that of the outcomes reported, the rate of psychotic conversion was not significantly different
between the groups.
As rigorous trials involving nonpharmacological interventions conducted in at-risk youths are limited, those
conducted in the first episode patients may also be examined because of their applicability in this age-specific
population. One example is the OPUS-Scandinavia study16
which included 547 people with a diagnosis of first
episode schizophrenia; 275 were randomly assigned to integrated treatment (consisting of an assertive
community treatment, family therapy, social skills training, and modifications of medication regime) and 272
to standard treatment. The results show that the GAF symptom score significantly favoured integrated
treatment by 1 year, but neither group differed significantly at 2-year follow-up. Two patients committed
suicide, one from each group. While psychosocial interventions often complement pharmacological
treatments in chronic schizophrenia, further studies are necessary to validate such strategies in the
prodromes.
The potential risks of being at risk
The results of the intervention studies while being positive in some cases are still preliminary, requiring
large-scale collaborative efforts with sufficient sample power and rigorous statistical analyses for more
adequate validation. Nonetheless, it is worth noting that success in treating the prodromal population as
described will not serve to clarify the issues of who to treat. If outcome can be affected by pre-emptive
interventions, there will be a great incentive to expand the profile of eligible candidates likely to benefit from
treatment; this may include increasingly younger patients or even those without symptoms. Hence, strict
scrutiny of possible ethical concerns arising from unintended consequences of false positives (those who
would not have developed the disease even without the intervention), stigma, and loss of confidentiality and
autonomy is crucial. These will be discussed in turn in the sections below.
False positives
There is no method of screening a population for susceptibility to schizophrenia existing or envisaged that can
eliminate the issue of false positives. The current range of specificity of the at-risk criteria is 71-74%, reflecting
a substantial false positive rate.9 One apparent problem for false positives is the risk of over-treatment. The
use of antipsychotic medication for those who have not yet developed frank psychotic symptoms is
7/31/2019 Prodromal Schizophrenia
9/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 8
controversial as the data regarding the efficacy and safety are inconclusive. Investigators from the PACE and
PRIME studies11,12
believe that the newer atypical agents, such as risperidone and olanzapine provide a safer
alternative than previous neuroleptic medications while others argue that this is questionable, particularly in
this population, which are primarily young adults and teenagers.15,17
Taking an example from the PRIME study
(2003),12 patients who were given olanzapine had higher increases in weight gain (mean weight gain of 8.79
kg) compared to those taking placebo (0.30 kg) at 1-year follow-up. This supports other recent reports of
olanzapines association with weight gain.15,18
The issue of weight gain should be taken seriously as it poses
threat not only to self-image and social functioning but also adds to serious long-term health risks of obesity
and diabetes mellitus, especially as these medications have been associated with insulin resistance and
metabolic syndrome.18
Stigma
Beyond the issue of side effects of treatments, it is worth considering whether there are any ethical
considerations specific to the idea of participating in a programme designed to study and prevent incipient
psychosis. Prodromal research subjects could feel that they are labelled as at risk for psychosis in a way that
could cause negative repercussions. This does not necessarily imply that researchers would use such a label, or
that the idea of being considered at risk for psychosis is inherently pejorative. Nonetheless, it raises the issues
of stigma. In a population that is not immediately at risk or impaired, the idea of being vulnerable for psychosis
could leave the false positives with a lasting sense of being fragile or damaged. It might alter their goals or
make them less likely to achieve; it could be harder to find motivation for a future threatened by impending
illness. Families might well reorganise their priorities in the light of this information. Sarahs family was very
supportive of her predicament especially after she stopped going to university even when the actual
diagnosis of prodromal schizophrenia was not made. Indeed, some families, like Sarahs, tend to be
protective, allowing them to protect at-risk individuals from stress and redefining behavioural problems as
illness rather than character flaws. In others, the protective impulse might in effect, result in discouragement
of growth or achievement.
The issues of stigma surrounding false positive results should be viewed in context of the stigma associated
with actually suffering from the disease, the true positives. Is there a risk of stigma if we do not identify
individuals early? If we do not, and a person becomes schizophrenic, he or she may violate societal norms in a
situation that may be detrimental or embarrassing. Which is more stigmatising? For the true positives
identified early, the potential of effective treatment must be balanced against heightened anxiety and
medicalisation of their presymptomatic years, a period of time that could represent their best shot at
normalcy in the face of what might be a lifelong struggle with mental illness. Sarahs early psychotic symptoms
were severe enough to warrant her quitting university and she had only worked for two years as a secretary
before being forced into retirement, due to her cognitive instability. Would knowing and treating the
prodromal symptoms make her lifes trajectory any better? As we have seen in the studies above, this is
unlikely. Would the stigma associated with being labelled as at risk be less severe than that linked with the
7/31/2019 Prodromal Schizophrenia
10/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 9
disease itself? This is unknown. Nonetheless, the stigma associated with schizophrenia is widely recognised,
creating challenges for sufferers and discrimination in society. This demonstrates the need for education
concerning mental illness amongst family members and society. The importance of addressing stigma, along
with early detection and treatment of schizophrenia may help to reduce the morbidity associated with
schizophrenia.
Issues regarding confidentiality and autonomy
At-risk individuals should also have concerns about whether intervention for susceptibility will make them
unemployable or uninsurable and whether it will constitute a diagnosis in the eyes of employers or insurers,
meaning that from this point forward they will have on record a pre-existing condition. Confidentiality is an
important tool for protecting the at-risk population from this discrimination. It includes not only who is told
and what is told but what type of language is used and what sort of messages are implied. The PACE (Personal
Assessment and Crisis Evaluation) study11 was named deliberately as such (i.e. using neutral language) to avoid
frightening the at-risk population of youths and to prevent suggestion of diagnosis of schizophrenia/psychosis
to the observers. The PACE clinic was situated in a teen centre within a shopping mall rather than in a hospital
setting to further minimise association with mental illness. Even with such a sensitive and thoughtful
approach, confidentiality issues regarding prodromal interventions may still arise. One problem is that it relies
on the discretion of parents and families. It is not reasonable to assume that patients and families will keep
information to themselves even if that is in their best interests. It is safest to assume that any information
given to patients could become available to their community, schools, employers, insurers and other potential
third parties, by virtue of what the families choose to share.
One potential solution that has been debated by researchers is that it might be possible to just limit the
information given to patients and families using language that is neutral and avoiding specific mention of
schizophrenia/psychosis as a risk. This circumvents the problems of relying on the discretion of the patient and
family members. However, filtering information is not compatible with our understanding of patient autonomy
or the requirements of informed consent. Indeed protecting patient autonomy in medicine has come to be
synonymous with informed consent. In the prodromal period, patients are on the cusp of competence both in
terms of age and mental status. Interventions at an earlier stage imply that patients will be less compromised
by the disease, in terms of cognition and insight, but will also be younger and thus less able to participate in
the decision-making process. Presumptively, parents/guardians will often be very much involved in any
decision to pursue treatment. Most of the time, the best interests of the child and the best interests of the
family converge. However, family members, as potential caregivers, may at times have an agenda that
deviates from the best interests of the patient. Psychosis can place an enormous burden on family members;
they may feel that with regard to treatment, limiting unnecessary risks is more important than any treatment
goal. Cultural issues, educational inadequacies and geographic or economic barriers might be at play in
influencing decisions. Doctors should therefore then take an active role in guiding the decision-making
process.
7/31/2019 Prodromal Schizophrenia
11/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 10
Prodromal intervention: A clinical equipoise
Exploring the ethical and social implications of early interventions in schizophrenia at this stage of the game
affords us a moment to consider the impact of schizophrenia has on public health. The estimated overall cost
of schizophrenia in the US is $62.7 billion, with total indirect cost of unemployment of $32.4 billion.
19
Althoughthe cost of early identification and intervention may initially appear to be higher, it is suggested that early
identification may be cost-saving.19
As a result, there has been an increase in the number of studies on
prodromal schizophrenia reported recently. The ED:IT programme20
in the UK targets engagement and
intervention for at-risk youths and improved access to care for at-risk populations and communities. Such
clinical research has led in the Department of Health funding a five-year public health programme to reduce
the rates of transitions to psychosis and the DUP.20
Nonetheless, in my opinion, current circumstances encourage but do not dictate intervention, as there exists a
state of clinical equipoise regarding evidence related to treatment efficacy and safety. Furthermore, the ethical
issues are complex and multifaceted, involving the issues of side effects in the false positives, significant stigma
associated with involvement in prodromal research and the unresolved aspects of confidentiality and
autonomy. As such, early intervention for prodromal schizophrenia is still very much in the realms of research
and the decision-making process on who to treat requires an individualised strategy rather than the one -size-
fits-all approach. However, as more trials are being conducted worldwide, this might change in the near
future.
During my first SSC earlier this year, I had the opportunity to visit Sarah again at the psychiatric hospital. She
recognised me, to my delight, but then proceeded to talking about another delusion she was having; this time
it was about nurses who tried to kill her whilst she was asleep. Much research has been done about
schizophrenia, but none is more important than those that contribute to the prevention of the disease, after
all, prevention is better than cure. But for now, most patients with schizophrenia would have followed a
disease course similar to that of Sarah: prodromal symptoms went unnoticed, schizophrenia diagnoses made
late into the disease progression, subsequent schizophrenia symptoms inadequately treated. Like Sarah, these
patients will end up imprisoned in their own body. Much effort needs to be done to prevent the onset of this
devastating disease.
(3495 words excluding headings and legends)
7/31/2019 Prodromal Schizophrenia
12/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 11
References
1. Addington J, Van Mastrigt S, Addington D. Duration of untreated psychosis: Impact on 2-yearoutcome. Psychol Med 2004, Feb;34(2):277-84.
2. Ballon JS, Kaur T, Marks II, Cadenhead KS. Social functioning in young people at risk for schizophrenia.Psychiatry Res 2007, May 30;151(1-2):29-35.
3. Bilder RM, Reiter G, Bates J, Lencz T, Szeszko P, Goldman RS, et al. Cognitive development inschizophrenia: Follow-Back from the first episode. J Clin Exp Neuropsychol 2006, Feb;28(2):270-82.
4. Caspi A, Reichenberg A, Weiser M, Rabinowitz J, Kaplan Z, Knobler H, et al. Cognitive performance inschizophrenia patients assessed before and following the first psychotic episode. Schizophr Res 2003,
Dec 15;65(2-3):87-94.
5. Davidson M, Reichenberg A, Rabinowitz J, Weiser M, Kaplan Z, Mark M. Behavioral and intellectualmarkers for schizophrenia in apparently healthy male adolescents. Am J Psychiatry 1999,
Sep;156(9):1328-35.
6. Yung AR, McGorry PD. The prodromal phase of first-episode psychosis: Past and currentconceptualizations. Schizophr Bull 1996;22(2):353-70.
7. Melle I, Haahr U, Friis S, Hustoft K, Johannessen JO, Larsen TK, et al. Reducing the duration ofuntreated first-episode psychosis -- effects on baseline social functioning and quality of life. Acta
Psychiatr Scand 2005, Dec;112(6):469-73.
8. Yung AR, Yuen HP, McGorry PD, Phillips LJ, Kelly D, Dell'Olio M, et al. Mapping the onset of psychosis:The comprehensive assessment of at-risk mental states. Aust N Z J Psychiatry 2005;39(11-12):964-71.
9. Miller TJ, McGlashan TH, Rosen JL, Cadenhead K, Ventura J, McFarlane W, et al. Prodromalassessment with the structured interview for prodromal syndromes and the scale of prodromal
symptoms: Predictive validity, interrater reliability, and training to reliability. Schizophr Bull
2003;29(4):703.
10. Addington J, Heinssen R. Prediction and prevention of psychosis in youth at clinical high risk. Annu RevClin Psychol 2011, Apr 4.
11. McGorry PD, Yung AR, Phillips LJ, Yuen HP, Francey S, Cosgrave EM, et al. Randomized controlled trialof interventions designed to reduce the risk of progression to first-episode psychosis in a clinical
sample with subthreshold symptoms. Arch Gen Psychiatry 2002, Oct;59(10):921-8.
12. McGlashan TH, Zipursky RB, Perkins D, Addington J, Miller T, Woods SW, et al. Randomized, double-blind trial of olanzapine versus placebo in patients prodromally symptomatic for psychosis. Am J
Psychiatry 2006, May;163(5):790-9.
13. Woods SW, Tully EM, Walsh BC, Hawkins KA, Callahan JL, Cohen SJ, et al. Aripiprazole in the treatmentof the psychosis prodrome: An open-label pilot study. Br J Psychiatry Suppl 2007, Dec;51:s96-101.
14. Morrison AP, French P, Walford L, Lewis SW, Kilcommons A, Green J, et al. Cognitive therapy for theprevention of psychosis in people at ultra-high risk: Randomised controlled trial. Br J Psychiatry 2004,Oct;185:291-7.
7/31/2019 Prodromal Schizophrenia
13/13
Rupert Kelly Prize Prodromal schizophrenia: To treat or not to treat?
Alhafidz Hamdan, Stage 4 MBBS 12
15. Marshall M, Rathbone J. Early intervention for psychosis. Cochrane Database Syst Rev 2006;4.16. Petersen L, Jeppesen P, Thorup A, Abel MB, hlenschlger J, Christensen T, et al. A randomised
multicentre trial of integrated versus standard treatment for patients with a first episode of psychotic
illness. BMJ 2005; 331: 6025.
17. Kumra S, Oberstar JV, Sikich L, Findling RL, McClellan JM, Vinogradov S, Schulz SC. Efficacy andtolerability of second-generation antipsychotics in children and adolescents with schizophrenia.
Schizophr Bull 2008;34(1):60-71.
18. Sacher J, Mossaheb N, Spindelegger C, Klein N, Geiss-Granadia T, Sauermann R, et al. Effects ofolanzapine and ziprasidone on glucose tolerance in healthy volunteers. Neuropsychopharmacology
2007;33(7):1633-41.
19. Kaur T, Cadenhead KS. Treatment implications of the schizophrenia prodrome. BehavioralNeurobiology of Schizophrenia and Its Treatment 2010:97-121.
20. Birchwood M, Patterson P, Lester H, Singh SP. Integrating UHR research and practice into the publichealth agenda: The birmingham ED: IT programme. Schizophr Bull 2009;35(Suppl. 1):134-5.
Top Related