





Languages
Pages
Legal


PRIVATE & CONFIDENTIAL HEALTH QUESTIONNAIRE for Nadiya Kondratyeva Clinical Naturopathic Nutritionist & Functional Medicine Practitioner
www.tunbridgewellsnutritionist.co.uk

PERSONAL DETAILS
FULL NAME
INSTRUCTIONS
HEIGHT (cm / metres / feet) WEIGHT (lbs / kg / stone)
BLOOD PRESSURE
NORMAL
PHONE
DATE OF BIRTH 1) Acrobat Reader is required to fill in this form. You can download it for free here: get.adobe.com/uk/reader/
2) Before you start filling in the questionnaire please make sure you read and sign the Terms and Conditions which were sent to you together with this questionnaire.
3) Once you have open the form please save it on your computer and re-open to make sure you will not lose any details.
4) By signing below you are confirming that you have read and understood the Terms and Conditions.
5) Please allow yourself at least 30 minutes to complete this questionnaire.
CHILDREN'S AGE
LOW
HIGH
DATE
CHILDREN IF SO, HOW MANY?
Living with partner/spouse
LIVING CIRCUMSTANCES:
ADDRESS (street, town, county and post code)
I agree for you to contact my GP if it becomes necessary. * All personal data is kept private with accordance to our Terms & Conditions.
I agree to the above statements.
I would like to receive special offers, monthly newsletter and health tips.
Living with family or relative (s)
Living alone
GP (name and address)
TW NUTRITIONIST
.............................................................................................................
.............................................................................................................
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
.
1 .................................................................................. ....................................................................................

2
MAIN SYMPTOM SEVERITY
NOTES
MILD SEVERE
1 2 3 4 5 6 7 8 9 10
HEALTH ISSUE THAT YOU WISH TO ADDRESS
DURATION OF THIS SYMPTOM & TRIGGERS THAT AGGRAVATE IT Please list onset, duration, possible cause, previous treatment, relieving or aggravating factors.
OTHER HEALTH CONDITIONS / SYMPTOMS YOU ARE SEEKING SUPPORT FORPlease list also all diagnosed conditions and include duration (e.g. eczema - since childhood, acid reflux - 3 months).
CURRENT MEDICATIONS AND / OR SUPPLEMENTSPlease advise of any medications and / or supplements you are currently taking. These should include all over-the-counter medication (dosage, brand and frequency).
WHAT IS YOUR APPROXIMATE MONTHLY BUDGET FOR SUPPLEMENTS?
.................................................................................. ....................................................................................
TW NUTRITIONIST
.................................................................................................................................................................................

3................................................................................... ....................................................................................
FAMILY HISTORY
PREVIOUS MEDICAL HISTORY..................................................................................................................................................................................
.....................................................................................................................
NOTES
CANCER
ECZEMA
OBESITYCELIAC DISEASESTROKE
DEMENTIAANAEMIA
DIABETES ARTHRITIS
AUTOIMMUNE CONDITIONS HIGH BLOOD PRESSURE
HEART DISEASE THYROID ISSUES DEPRESSION
NATURAL
CHILDHOOD
CHICKEN POX WOOPING COUGH OTHER - LIST IN NOTES
MEASLES MUMPS RUBELLA
HOW LONG
PREMATURE CAESARIANYOUR BIRTH
VACCINESPlease include all vaccine history and dates if known.
WERE YOU BREASTFED
TW NUTRITIONIST

DIGESTIVE SYSTEM (Please tick if you experience any of the following)
4................................................................................... ....................................................................................
..................................................................................................................................................................................NOTES
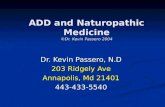
Type 2
Type 1
Type 3
Type 4
Type 5
Type 6
Type 7
Separate hard lumps, (hard to pass).
Hard consistency,but lumpy.
Softer than type 2, but with cracks on the surface.
Smooth and soft.
Soft blobs with clear-cut edges.
Fluffy pieces with ragged edges, a mushy stool.
Watery, no solid pieces.Entirely liquid.
Bristol Stool Chart (BSC)Your poo is important! Please tick below the type/s which are most common to you.
How many bowel movements do you have a day?
BSC is a diagnostic medical chart used as a clinical assessment tool since 1997.
ULCERS
BLOATING
ACID REFLUX
URGENCY
BLOOD IN STOOL
OTHER - SPECIFY IN NOTES
HAEMORRHOIDS
ANAL ITCHING
PARASITES
FLOATING STOOL
CRAMPS
INDIGESTION
UNDIGESTED FOOD IN STOOL
DIVERTICULITIS
CONSTIPATION
NAUSEA
DIARRHOEA
ABDOMINAL PAIN BELCHING
IBS
IBD COLITIS STOMA
ABDOMINAL HERNIA
MUCUS IN THE STOOL
SUDDEN CHANGES IN BOWEL MOVEMENTS
TW NUTRITIONIST

NERVOUS SYSTEM (Please tick if you experience any of the following)
5................................................................................... ....................................................................................
..................................................................................................................................................................................NOTES HEADACHE
ANXIETY
UNRESTED SLEEP
WEIGHT GAIN
COLD EXTREMITIES
LUNCH TIME MID AFTERNOON EVENINGON WAKING
FAIREXCELLENT GOOD POOR
HAIR LOSS
WEIGHT LOSS LOW BODY TEMPERATURE
EMOTIONAL INSTABILITY EXCESSIVE THIRST FREQUENT URINATION
MIGRAINES
SWEET CRAVINGS SALT CRAVINGS TEARFUL
BAD SHORT TERM MEMORY
BAD LONG TERM MEMORY
LOW CONCENTRATION DEPRESSION SWEATS
VISUAL DISTURBANCE DIZZINESS FAINTING
ENERGY LEVELS ( When do you feel most energetic?)
DAILY ENERGY LEVEL
What do you use to boost energy when it is low?
TW NUTRITIONIST
ENDOCRINE SYSTEM..........................................................................................................................
..........................................................................................................................

CARDIOVASCULAR SYSTEM (Please tick if you experience any of the following)
6................................................................................... ....................................................................................
..................................................................................................................................................................................NOTES OEDEMA
REGULAR CYCLE
CHILDREN
FREQUENT URINATION ERECTILE DISFUNCTION
SURGERY - PLEASE PROVIDE DETAILS IN NOTES
LOSS OF LIBIDO STDs ENLARGED PROSTATE
HYSTERECTOMY
PRE-MENSTRUAL SYNDROME (PMS)
HRT
SURGERY - PLEASE DETAIL
INCREASED FACIAL/BODY HAIR
UTERINE FIBROIDS
TENDER BREASTS
PRE-MENSTRUAL MENOPAUSE
PAINFUL INTERCOURSE BIRTH CONTROL PILL
STDs ABORTION/S THRUSH LOW LIBIDO
CHEST PAIN SHORTNESS OF BREATH PALPITATIONS
LIGHTHEADEDNESS COLD HANDS & FEET IRREGULAR HEARTBEAT
REPRODUCTIVE SYSTEM
FEMALE
MALE
..........................................................................................................................
..........................................................................................................................
TW NUTRITIONIST

ALLERGIES
FREQUENT BRONCHITIS
BLOCKED SINUSITIS
TONSILS REMOVED
JOINT PAIN
FREQUENT URINATION
STONG SMELLING URINE DARK COLOURED URINE FREQUENT UTIs
PAIN/BURNING ON URINATION BLOOD IN URINE
SPASMS INJURIES - PLEASE DETAIL
JOINT SWELLING BACK PAIN CRAMPS NECK PAIN
DRY THROAT EAR INFECTIONS PERSISTENT COUGH
SHORTNESS OF BREATH TONSILLITIS
POST NASAL DRIP EXCESSIVE MUCUS
PSORIASIS
AUTOIMMUNE CONDITIONS SLOW WOUND HEALING OTHER - PLEASE DETAIL
URTICARIA FREQUENT INFECTIONS COLD SORES
INTOLERANCES ASTHMA FREQUENT COLDS
IMMUNE SYSTEM (Please tick if you experience any of the following)
7................................................................................... ....................................................................................
..................................................................................................................................................................................NOTES
RESPIRATORY SYSTEM..........................................................................................................................
..........................................................................................................................
MUSCULO-SKELETAL SYSTEMS..........................................................................................................................
..........................................................................................................................
EXCRETORY SYSTEM..........................................................................................................................
..........................................................................................................................
TW NUTRITIONIST

DO YOU EXERCISE REGULARLY? YES NO
ACNE
NO FILLINGS MORE THAN 2 FILLINGS
DENTAL IMPLANTS MERCURY FILLINGS
ROOT CANALS
FUNGAL INFECTION (e.g. athlete's feet)
ECZEMA DANDRUFF DERMATITIS
RASHES
SKIN (Please tick if you experience any of the following)
8................................................................................... ....................................................................................
..................................................................................................................................................................................
NOTES
TW NUTRITIONIST
DENTAL HEALTH..........................................................................................................................
..........................................................................................................................
EXERCISE..........................................................................................................................
..........................................................................................................................
SLEEP..........................................................................................................................
..........................................................................................................................HOW MANY HOURS DO YOU SLEEP?
AT WHAT TIME DO YOU USUALLY GO TO BED?
AT WHAT TIME DO YOU USUALLY WAKE UP?
GOOD DREAM RECALL
DO YOU FEEL UNRESTED WHEN YOU WAKE UP?
NIGHTMARES
(please describe below)

WORK-LIFE BALANCE
9................................................................................... ....................................................................................
..................................................................................................................................................................................NOTES WHAT ARE THE MAJOR CHALLENGES IN YOUR LIFE AT THE MOMENT?
WHAT DO YOU DO TO RELAX AND HOW OFTEN?
DO YOU FEEL YOU HAVE ENOUGH SUPPORT? YES NO
DO YOU SWITCH OFF EASILY? YES NO
DO YOU LIKE YOUR JOB?
HOW SATISFYING IS YOUR JOB?
YES NO
1 2 3 4 5 6 7 8 9 10
DAILY STRESS LEVELS VERY HIGH HIGH MODERATE LOW
TW NUTRITIONIST

FOOD
10................................................................................... ....................................................................................
..................................................................................................................................................................................NOTES MIXED DIET
SKIP BREAKFAST
GENERALLY EAT ON THE RUN
ADD SUGAR TO DRINKS
ADD LOTS OF SALT TO FOOD
GRAZE ALL THE TIME REGULARLY MISS MEALS
I LOVE FOOD & I COOK MOSTLY FROM SCRATCH
I PREFER PRE-COOKED / TAKE AWAY MEALS
FOOD EXCLUSIONS (Please list any foods you don't eat or you don't like)
WHICH BEST DESCRIBES YOUR RELATIONSHIP WITH FOOD?
VEGETARIAN VEGAN OTHER - PLEASE DETAIL
EATING HABITS
HAVE YOU EVER PERFORMED A FOOD INTOLERANCE TEST? YES NO
TW NUTRITIONIST

FOOD LIST
11................................................................................... ....................................................................................
..................................................................................................................................................................................TW NUTRITIONIST
Please list how many servings you usually have of each food per week. If you don’t eat a certain food, leave it blank.If you eat it less than once a week, mention it in the notes, along with any other foods you regularly eat that are not listed.
CARBOHYDRATES SUGARS ANIMAL PROTEIN
PLANT PROTEIN
VEGETABLES (per cup)
FRUITS
WHITE BREAD
SUGAR (brown or white)
WHOLEMEAL BREAD
SOURDOUGH BREAD
HONEY
AGAVE SYRUP
MAPLE SYRUP
ARTIFICIAL SWEETENER
BANANA
NECTARINES
PERSIMMONS
KIWI
GRAPES
PEAR
APPLE
ORANGES
AVOCADO
TROPICAL (papaya, mango)
BERRIES (RAW)(blueberries, strawberries)
BEEF Red (red chicory, onions bell peppers, beetroot)Orange (pumpking, sweet potatoes, carrots)
Green (asparagus, baby salad, spinach, zucchini)
White (cauliflower, cabbage)
Cruciferous (broccoli, bok choy, cress, kale)Bitter (rocket, chicory, radishes, watercress)
Sauerkraut
Kvass
Kefir
Kombucha
Miso
Kimchi
Single/Double cream
Cow's milk
Goat's milk
PORK
CHICKEN
TURKEY
EGGS
PROCESSED MEAT (sausages, salami, bacon)
LIVER
WHITE FISH (cod, haddock)
OILY FISH (salmon, mackerel, anchovies)
SHELLFISH(crab, prawns, mussels)
TOFU/TEMPEH
CHICKPEA
BEANS/PULSES
QUINOA
NUTS
PROTEIN POWDER
PASTA/NOODLES
OATS/CEREALS
WHITE RICE
BROWN RICE
BUCKWHEAT
COUSCOUS
POTATOES
BISCUITS
CAKES
MUFFINS
PEAS
CROISSANTS
SWEET POTATOES
OTHER (please detail)
SERVING SERVING SERVING SERVING
SERVING
SERVING
SERVING
SERVING
ORGANIC YES
ORGANIC YES
ORGANIC YES
ORGANIC YES
ORGANIC YES
ORGANIC YES
ORGANIC YES
ORGANIC YES
FERMENTED
DAIRY
(per tsp)

NOTES
FOOD LIST
12................................................................................... ....................................................................................
..................................................................................................................................................................................TW NUTRITIONIST
Please list how many servings you usually have of each food per week. If you don’t eat a certain food, leave it blank.If you eat it less than once a week, mention it in the notes, along with any other foods you regularly eat that are not listed.
Water
HYDRATION Alcohol
Other drinks
Natural yogurt
Flavoured yogurt
Pasteurised cheeses
Unpasteurised cheeses
Tap water
Filtered water
Distilled water
Bottle water
Fizzy water
Instant coffee
Decaf coffee
Decaf tea
Black tea
Herbal tea
Freshly ground coffee
Juice
Cordial
Energy drink
Soft drink
Wine
Spirits
Beer/Cider
Please list below any other foods/drinks and the frequency.
Cottage cheese
Chia seeds
Linseeds
Hemp seeds
Sesame seeds
Olive oil
Butter
Pumpkin seeds
Rapeseed oil
Coconut oil
Margarine
Other vegetable oil
SEEDS
FATS
SERVING
SERVING
SERVING
SERVING
SERVING ORGANIC YES
ORGANIC YES
ORGANIC YES
ORGANIC YES
ORGANIC YES

FOOD DIARY
13................................................................................... ....................................................................................
..................................................................................................................................................................................TW NUTRITIONIST
Please write down all the foods and drinks you would consume over a typical 3 day period. Please complete as accurately and honestly as possible. These should include breakfast, mid-morning snack, lunch, mid-afternoon snack, dinner and fluids.
Day 2Day 1 Day 3

14................................................................................... ....................................................................................
Thank you for taking the time to complete this form. Your detailed information will allow us to create a plan tailored to your exact needs.
Please save a copy for yourself before emailing [email protected]
How to send the questionnaire:
1) Kindly note you can send this form by clicking on“file” > "share" > "mail" and a new email window will open and the file will be included in it.
2) Save the completed questionnaire, open your email and select attach the file or drag and drop the questionnaire to the email.
If you experience any difficulties please get in touch and we will help you.
Kind regardsNadiya KondratyevaClinical Naturopathic Nutritionist & Functional Medicine PractitionerDip. CNM (College of Naturopathic Medicine, London)
Website: www.tunbridgewellsnutritionist.co.uk Phone: +44 (0)7474794947





Top Related