







Languages
Pages
Legal

Physical DevelopmentPhysical Development
Physical DevelopmentPhysical Development
What Changes?What Changes? Biological agingBiological aging
• PhysicalPhysical• Physiological and sensoryPhysiological and sensory• Health statusHealth status
Biological AgingBiological Aging
Deterioration of organism from time-Deterioration of organism from time-dependent, irreversible changesdependent, irreversible changes
Intrinsic to allIntrinsic to all Human life span fixed, but life Human life span fixed, but life
expectancy at birth changingexpectancy at birth changing

Females: Females: 82 years82 years
Males:Males:77 years77 years
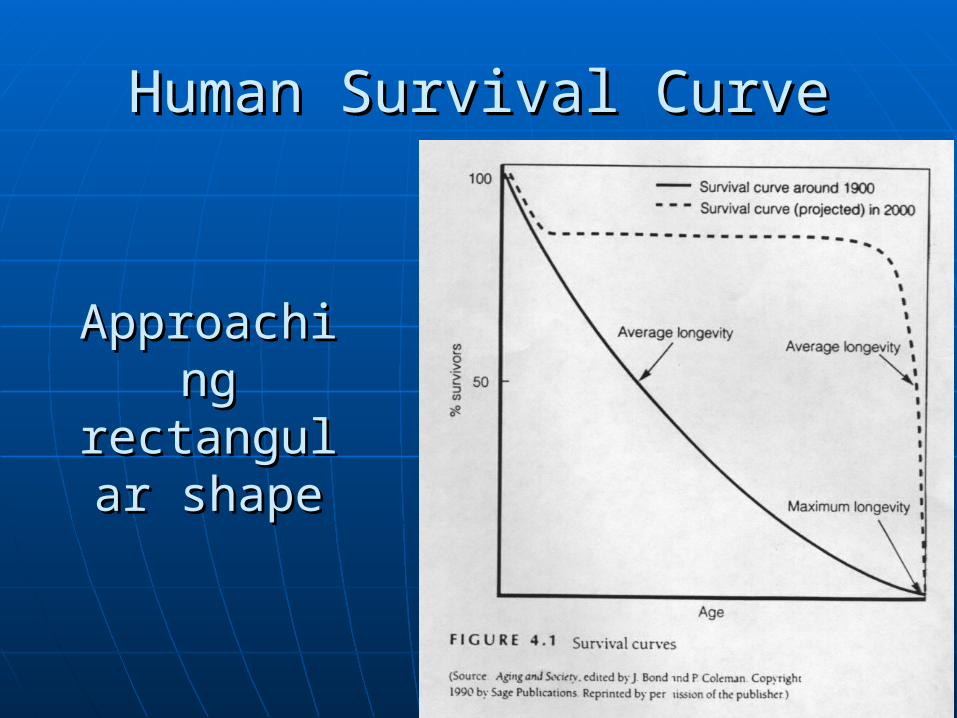
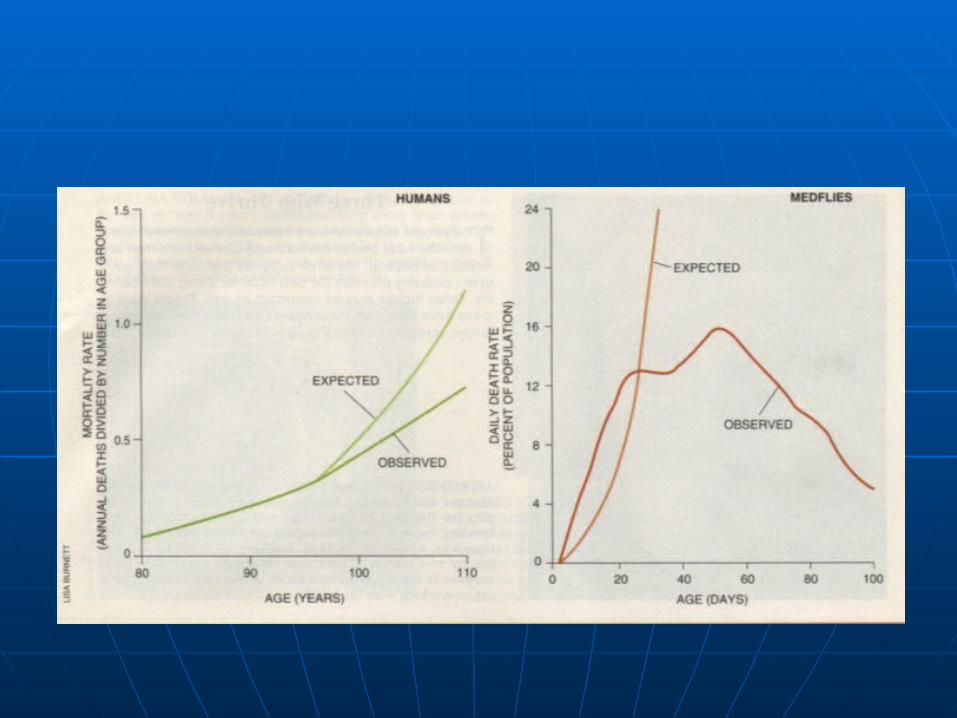
Human Survival CurveHuman Survival Curve
Approaching Approaching rectangular rectangular
shapeshape
Primary agingPrimary aging• SenescenceSenescence• Weakening/decline of bodyWeakening/decline of body• Normal processNormal process
Secondary agingSecondary aging• Increase in rate of senescence due to Increase in rate of senescence due to
extrinsic factorsextrinsic factors Environment (UV light: cataracts; noise Environment (UV light: cataracts; noise
pollution: hearing loss)pollution: hearing loss) Behaviour (smoking: decline in respiration)Behaviour (smoking: decline in respiration)
Primary agingPrimary aging• SensorySensory• physical: physical:
PhysiologicalPhysiological Musculo-skeletalMusculo-skeletal
• Theories of agingTheories of aging• Factors affecting healthFactors affecting health• Trends in disabilityTrends in disability

Sensory ChangesSensory Changes
Gradual decrease in sensory capacityGradual decrease in sensory capacity Often undermine cognitive Often undermine cognitive
functioningfunctioning
VisionVision
Field of vision restricts (changing Field of vision restricts (changing retinal metabolism)retinal metabolism)
Presbyopia: Accommodation declines Presbyopia: Accommodation declines (loss of near vision from decreased (loss of near vision from decreased flexibility of lens)flexibility of lens)
Sensitivity to glare, recovery time Sensitivity to glare, recovery time increasesincreases
Colour sensitivity declines (70 years)Colour sensitivity declines (70 years)• Blue/green discrimination difficulty due Blue/green discrimination difficulty due
to yellowing of lensto yellowing of lens Dark adaptation decreases: reduced Dark adaptation decreases: reduced
light transmitting properties of lenslight transmitting properties of lens
HearingHearing
Presbycusis Presbycusis • Decreased sensitivity to high-frequency Decreased sensitivity to high-frequency
soundssounds
Taste, smell: Taste, smell: • Taste not affectedTaste not affected• Smell diminishes in mid-50sSmell diminishes in mid-50s
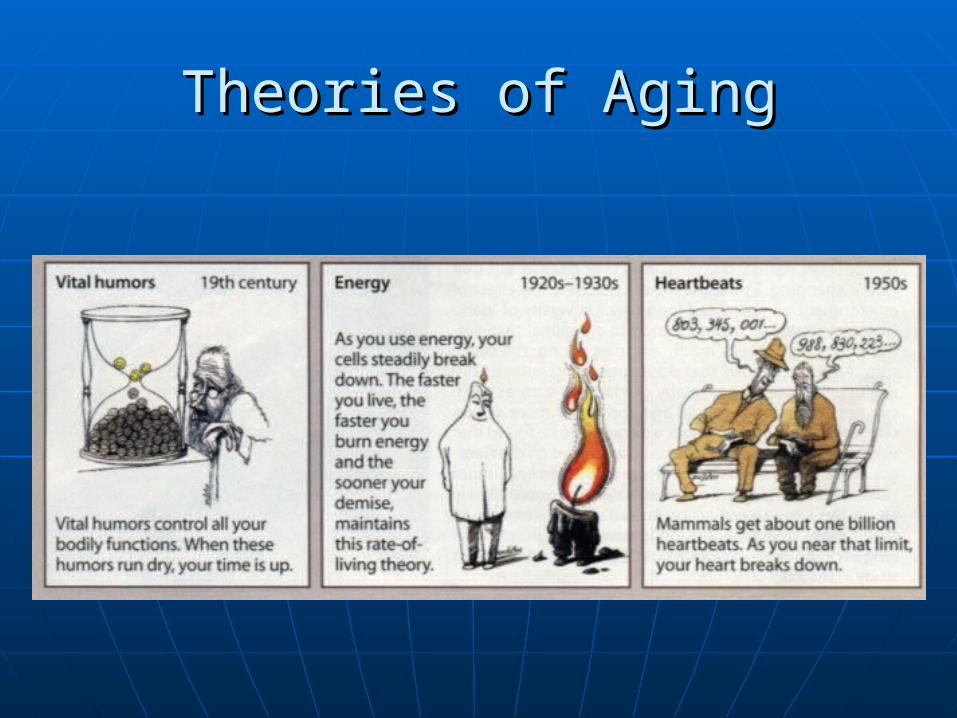
Theories of AgingTheories of Aging
Programmed theoryProgrammed theory• Metabolic theoryMetabolic theory
Damage to mitochondria impairs function in Damage to mitochondria impairs function in older cellsolder cells
Restricted diet?Restricted diet?


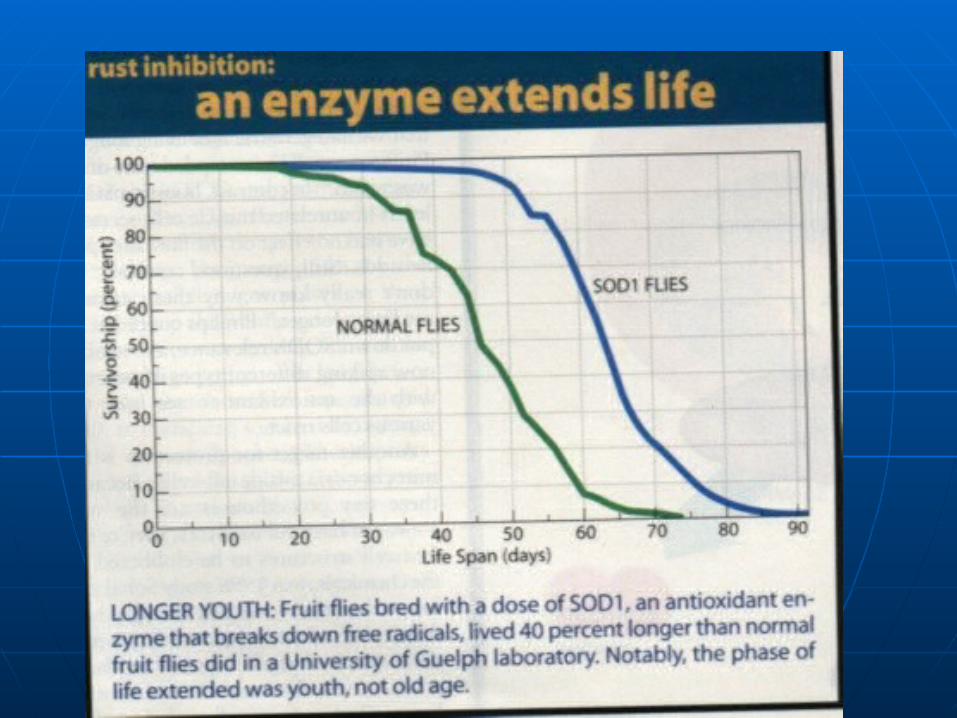
Stochastic theoriesStochastic theories• Random wear and tearRandom wear and tear• Free radicalsFree radicals
Reactive molecules produced in cell from Reactive molecules produced in cell from oxygen metabolismoxygen metabolism
• Oxygen-free radicalOxygen-free radical• Accumulate, destroy fats, protiens critical to cell Accumulate, destroy fats, protiens critical to cell
functioningfunctioning• Damage DNADamage DNA• Genetic therapy?Genetic therapy?• Diet: antioxidant enzymes neutralize free radicalsDiet: antioxidant enzymes neutralize free radicals
Anti-oxidantsAnti-oxidants
Physical HealthPhysical Health
Mortality: death rate (deaths per Mortality: death rate (deaths per 100,000 per year)100,000 per year)• DroppingDropping
Morbidity: prevalence of disease in a Morbidity: prevalence of disease in a populationpopulation• Chronic (long-term)Chronic (long-term)• Acute (short, suddent)Acute (short, suddent)
DisabilityDisability• Inability to perform activities of daily Inability to perform activities of daily
livingliving• Later in life, shorter durationLater in life, shorter duration
VitalityVitality• Subjective rating of health and energySubjective rating of health and energy
Factors affecting healthFactors affecting health
GenderGender• Mortality: men higher than womenMortality: men higher than women• Morbidity: women higher than menMorbidity: women higher than men
Chronic: women>menChronic: women>men Serious acute: men>womenSerious acute: men>women
• Heart disease: diagnostic procedures, treatment, Heart disease: diagnostic procedures, treatment, protective factors may have different effects on protective factors may have different effects on women than on menwomen than on men
FactorsFactors
IncomeIncome• Directly related to perception of healthDirectly related to perception of health
AgeAge• Much variationMuch variation• Young adulthoodYoung adulthood
Good healthGood health Few hospitalizationsFew hospitalizations Respiratory ailments most common (colds)Respiratory ailments most common (colds) Few chronic ailmentsFew chronic ailments Fatal diseases rareFatal diseases rare Leading causes of death: M: accidents/F: cancerLeading causes of death: M: accidents/F: cancer
Middle adulthoodMiddle adulthood• Common daily symptomsCommon daily symptoms
Musculo-skeletal problems (pain, stiffness in Musculo-skeletal problems (pain, stiffness in joints)joints)
Respiratory ailments (colds)Respiratory ailments (colds)• Disease more commonplaceDisease more commonplace
Chronic: main source of discomfortChronic: main source of discomfort Arthritis, hypertension, sinusitis, heart Arthritis, hypertension, sinusitis, heart
conditions, hearing impairmentsconditions, hearing impairments Fatal diseases: diabetes, ateriosclerosis, Fatal diseases: diabetes, ateriosclerosis,
emphysema, canceremphysema, cancer Death: heart disease, cancerDeath: heart disease, cancer
Late AdulthoodLate Adulthood• Common: musculoskeletal symptoms Common: musculoskeletal symptoms
(arthritis)(arthritis) 90%: pain symptoms, stiffness90%: pain symptoms, stiffness
• Acute problems diminish sharplyAcute problems diminish sharply Predominant: arthritis, hypertension, Predominant: arthritis, hypertension,
heart conditions, hearing impairmentsheart conditions, hearing impairments More severe than in middle adulthoodMore severe than in middle adulthood Limit work and leisure actiitiesLimit work and leisure actiities Hospital stays: life-threatening Hospital stays: life-threatening
diseasesdiseases Death: heart disease, cancer, strokeDeath: heart disease, cancer, stroke
Subjective evaluation of health Subjective evaluation of health declines with age (less than declines with age (less than expected)expected)
Types of symptoms changeTypes of symptoms change Rate of acute conditions drops, Rate of acute conditions drops,
chronic riseschronic rises Nonfatal disease: arthritis, sensory Nonfatal disease: arthritis, sensory
impairmentsimpairments Fatal: increase with ageFatal: increase with age Limitations to daily activities Limitations to daily activities
increase with ageincrease with age
Trends in disabilitlyTrends in disabilitly
Compression-of-Morbidity hypothesisCompression-of-Morbidity hypothesis• James FriesJames Fries• Prevention, better treatmentPrevention, better treatment
Portion of life spent in disease and disability Portion of life spent in disease and disability compressed, delayedcompressed, delayed
Poor health later in life, shorter durationPoor health later in life, shorter duration More healthy yearsMore healthy years Lack of data on incidence of disease and Lack of data on incidence of disease and
disabilitydisability But: falling rates of disability among elderly, But: falling rates of disability among elderly,
falling rates of chronic diseasefalling rates of chronic disease
Successful AgingSuccessful Aging
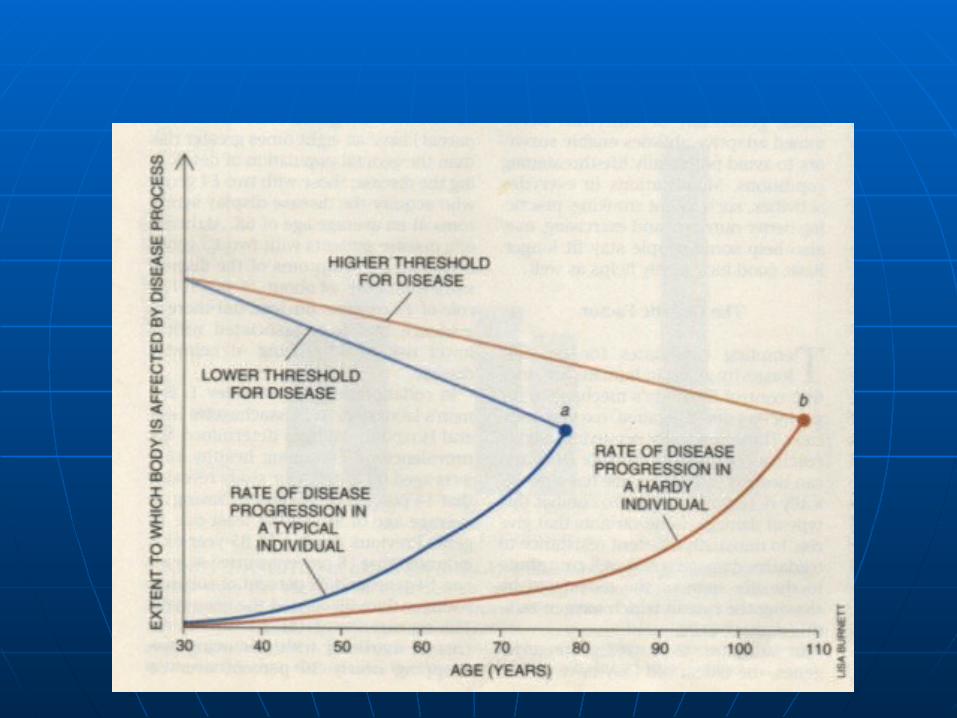
Hardiness and thriving (Perls, 1995)Hardiness and thriving (Perls, 1995)• Genetic determiners of “hardiness” in Genetic determiners of “hardiness” in
oldest oldoldest old• Adaptive capacity (ability to overcome Adaptive capacity (ability to overcome
disease or injury)disease or injury)• Functional reserve: how much of organ Functional reserve: how much of organ
required for adequate performance required for adequate performance (determines ability to deal with disease)(determines ability to deal with disease)
More hardyMore hardy• Slower rate of progressSlower rate of progress• Higher thresholdHigher threshold• Symptoms of age-related disease (e.g., Symptoms of age-related disease (e.g.,
Alzheimers) appear laterAlzheimers) appear later• Morbidity, mortality, disability Morbidity, mortality, disability
compressed into shorter periodcompressed into shorter period
More hardyMore hardy• Slower rate of progress of symptoms of Slower rate of progress of symptoms of
disease than in less hardydisease than in less hardy• Threshold for disease lowers more Threshold for disease lowers more
slowlyslowly
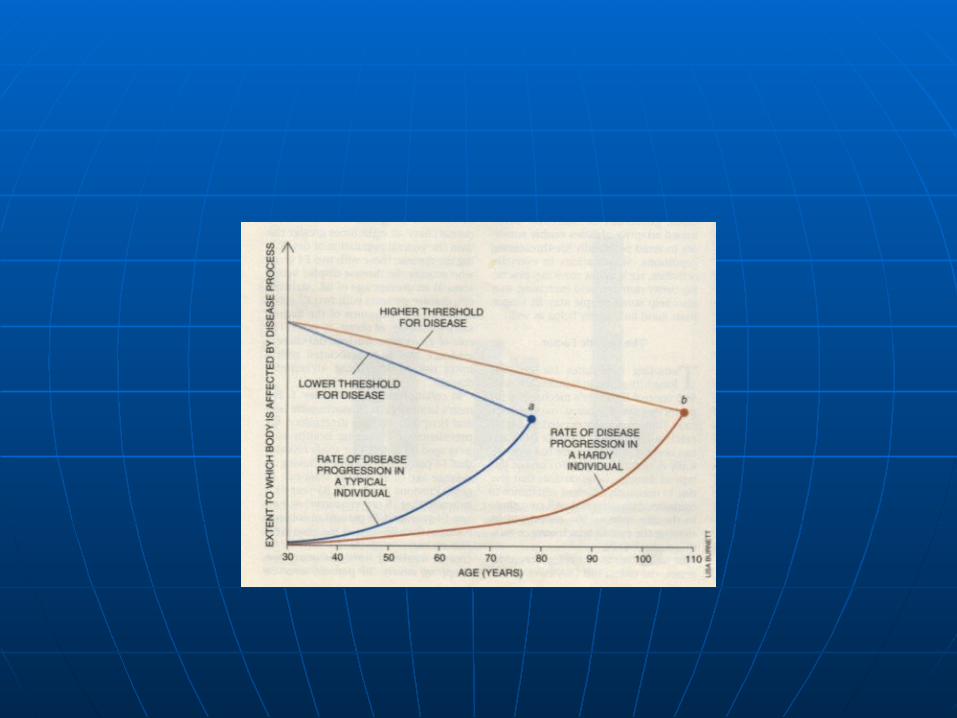
• Symptoms of age-related disease (e.g., Symptoms of age-related disease (e.g., Alzheimers) appear later (b vs. a)Alzheimers) appear later (b vs. a)
• Morbidity, mortality, disability Morbidity, mortality, disability compressed into shorter periodcompressed into shorter period
Possible explanations for Possible explanations for hardinesshardiness
Longevity genes: increased resistance Longevity genes: increased resistance against oxygen radicalsagainst oxygen radicals• Slow rate of damageSlow rate of damage
Low complement of deleterious genesLow complement of deleterious genes• E.g., Apolipoprotien E (apo-E) related to risk of E.g., Apolipoprotien E (apo-E) related to risk of
Alzheimer'sAlzheimer's• Gene for protein apo-E less prevalent in oldest-Gene for protein apo-E less prevalent in oldest-
old survivorsold survivors 18% of 90-103 year-olds18% of 90-103 year-olds 25% of under-65 year-olds25% of under-65 year-olds
• Adaptive capacity (ability to cope with Adaptive capacity (ability to cope with and overcome disease or injury) higher and overcome disease or injury) higher in more-hardyin more-hardy
• Functional reserve (how much of an Functional reserve (how much of an organ is required for its adequate organ is required for its adequate performance) higherperformance) higher
Autopsy studies of “healthy” oldest-Autopsy studies of “healthy” oldest-old brainsold brains• No outward signs of disease, but level of No outward signs of disease, but level of
neurofibrillary tangles would indicate neurofibrillary tangles would indicate dementia in younger braindementia in younger brain
• Excess reserve of brain function Excess reserve of brain function compensates for processes damaging compensates for processes damaging the brainthe brain
Two Basic Principles of Normal Two Basic Principles of Normal AgingAging
Variability of aging ratesVariability of aging rates• Longitudinal studies (e.g., Baltimore Longitudinal studies (e.g., Baltimore
Study)Study) Aging rates vary remarkably (60 year olds Aging rates vary remarkably (60 year olds
like 40; some 40 year-olds like 60, like 40; some 40 year-olds like 60, physically)physically)
Differences in appearance mirrored on Differences in appearance mirrored on physiological testsphysiological tests
Variability increases as age increasesVariability increases as age increases Individual aging rates vary across years, and Individual aging rates vary across years, and
across physical systemsacross physical systems
Variability of Aging PatternsVariability of Aging Patterns• Several aging paths:Several aging paths:
• Cross-sectional researchCross-sectional research Some functions decline in a regular way Some functions decline in a regular way
over timeover time Other functions are stable, unchanged or Other functions are stable, unchanged or
decline only in terminal phase of lifedecline only in terminal phase of life
• Physiological loss, but only when an Physiological loss, but only when an age-related illness is experiencedage-related illness is experienced
E.g., heart disease correlated with a decline E.g., heart disease correlated with a decline in heart pumping capacity with agein heart pumping capacity with age
Without heart disease, pumping capacity as Without heart disease, pumping capacity as well at age 70 as at age 30well at age 70 as at age 30
• Terminal Loss PatternTerminal Loss Pattern Loss in a normally stable function may be Loss in a normally stable function may be
sign of impending deathsign of impending death E.g., immune system: # of lymphocytes E.g., immune system: # of lymphocytes
(white blood cells) stable normally stale(white blood cells) stable normally stale• Decline occurred in minority of Baltimore Study Decline occurred in minority of Baltimore Study
samplesample• Reported good health; good physical examsReported good health; good physical exams• At next follow-up for study – subgroup more likely At next follow-up for study – subgroup more likely
to have diedto have died
Loss occurs, but body compensates for the Loss occurs, but body compensates for the changechange• E.g., brain: neural loss but robust individual cell E.g., brain: neural loss but robust individual cell
growth (new dendrites, new connections) may growth (new dendrites, new connections) may help preserve thinking and memoryhelp preserve thinking and memory
Physical Aging: not only lossPhysical Aging: not only loss• StabilityStability• ResiliencyResiliency• Capacity for growthCapacity for growth

Term Test 1Term Test 1
50 MC50 MC 5 (out of 7) short answer5 (out of 7) short answer

Ideas and IssuesIdeas and Issues
Why study adult developmentWhy study adult development Demographic changesDemographic changes Life-span perspectiveLife-span perspective Social Realities of AgingSocial Realities of Aging
• Special needsSpecial needs• Stereotypical attitudesStereotypical attitudes• AgeismAgeism
Research in Adult DevelopmentResearch in Adult Development
Developmental research designsDevelopmental research designs Special problems in studying adult Special problems in studying adult
developmentdevelopment• Sources of biasSources of bias• Identifying samplesIdentifying samples
Theories and Psychosocial Theories and Psychosocial DevelopmentDevelopment
““World Views”World Views”• ContextualContextual• OrganismicOrganismic• MechanisticMechanistic
Psychosocial DevelopmentPsychosocial Development
ContextualContextual• Bronfenbrenner: Ecological system’s Bronfenbrenner: Ecological system’s
theorytheory• Neugarten: Timing of EventsNeugarten: Timing of Events
OrganismicOrganismic• Stages (psychoanalytic)Stages (psychoanalytic)• EriksonErikson• LevinsonLevinson
MechanisticMechanistic• Trait approachTrait approach• McCrae & Costa: Five-Factor modelMcCrae & Costa: Five-Factor model
Stability vs. change in adult Stability vs. change in adult personality developmentpersonality development
IdentityIdentity
Self-conceptSelf-concept EriksonErikson James MarciaJames Marcia
Physical DevelopmentPhysical Development
Biological agingBiological aging• Primary, secondaryPrimary, secondary
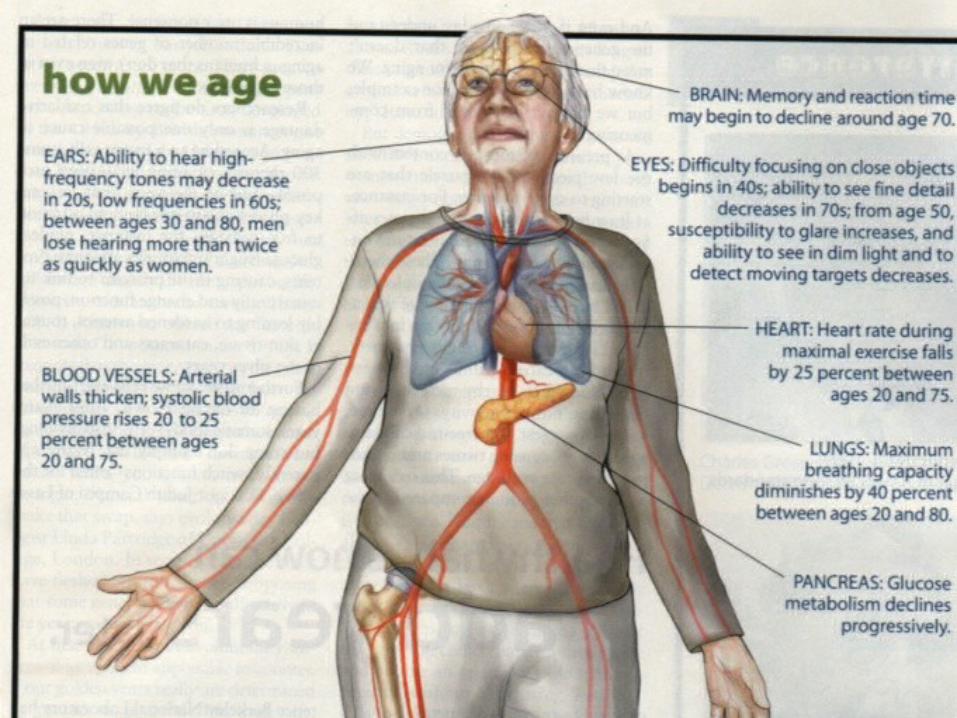
Physical changesPhysical changes• Body systems (heart, lungs, musculoskeletal)Body systems (heart, lungs, musculoskeletal)• Sensory systems (vision, hearing)Sensory systems (vision, hearing)
Theories of AgingTheories of Aging• ProgrammedProgrammed• StochasticStochastic
Hardiness in Oldest-OldHardiness in Oldest-Old
Top Related