






Languages
Pages
Legal


Phlebitis and thrombophlebitis

Phlebitis Overview
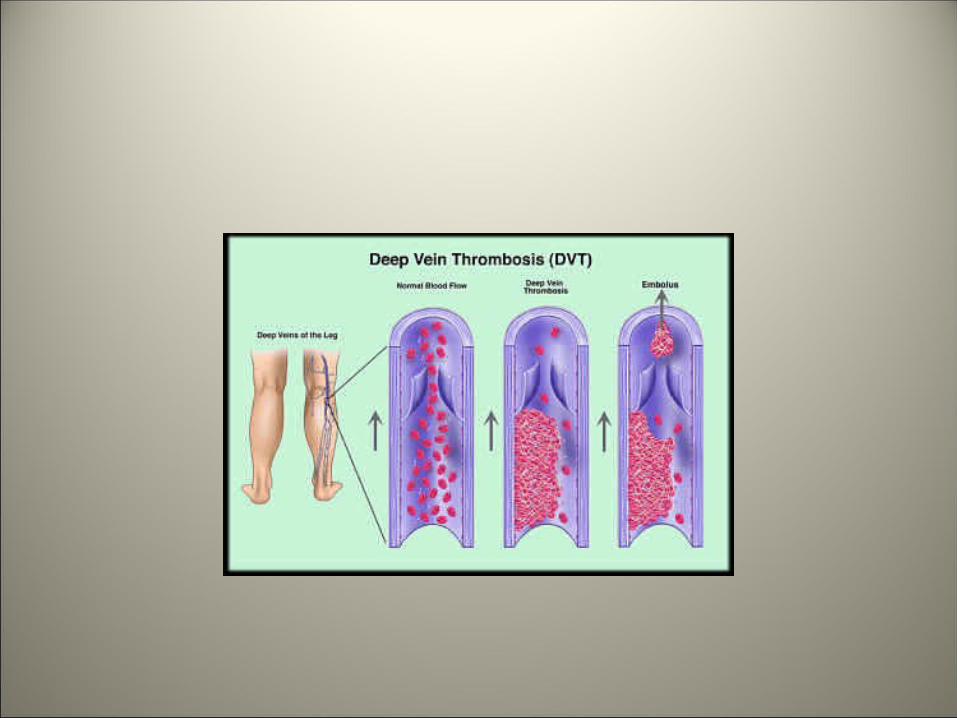
• Phlebitis -inflammation of a vein.• Thrombophlebitis -a blood clot in the vein
causes the inflammation. Thrombophlebitis usually occurs in leg veins, but it may occur in an arm. The thrombus (clot) in the vein causes pain and irritation and may block blood flow in the veins.
• Phlebitis can occur in both the surface (superficial) or deep veins.


• Superficial phlebitis affects veins on the skin surface. The condition is rarely serious and, with proper care, usually resolves rapidly.
• Sometimes people with superficial phlebitis also get deep vein thrombophlebitis, so a medical evaluation is necessary.
• Deep vein thrombophlebitis affects the larger blood vessels deep in the legs. Blood clots (thrombi) can form, which may break off and travel to the lungs. This is a potentially life-threatening condition called pulmonary embolism

Causes
• Phlebitis may occur spontaneously or as a complication of a medical procedure. Local trauma and injury to a vein also increase the risk of forming a blood clot
• Superficial phlebitis• There is usually a slow onset of a tender red area along the superficial veins on the
skin. A long, thin red area may be seen as the inflammation follows the path of a superficial vein.
• This area may feel hard, warm, and tender. The skin around the vein may be itchy and swollen.
• The area may begin to throb or burn.
• Symptoms may be worse when the leg is lowered, especially when first getting out of bed in the morning.
• A low-grade fever may occur.


• Sometimes phlebitis may occur at the site where a peripheral intravenous (IV) line was started. The surrounding area may be sore and tender along the vein.
• If an infection is present, symptoms may include redness, fever, pain, swelling, or breakdown of the skin.
• Thrombophlebitis migrans can be a non-metastatic manifestation of malignancies such as pancreatic carcinoma

• Deep vein thrombophlebitis• This can be similar in presentation to
superficial phlebitis, but some people may have no symptoms.
• The classic signs and symptoms include redness, warmth, swelling, and pain in the leg.
One may have pain and swelling throughout the entire limb.
• Treatment• In general, treatment may include support
stockings and wraps to reduce discomfort as well as medications such as:
• Analgesics • Antibiotics (if infection is present)• Anticoagulants (blood thinners) to prevent
new clots from forming

:• Elevate the affected area to reduce swelling.• Keep pressure off of the area to reduce pain and
decrease the risk of further damage.• Apply moist heat to reduce inflammation and
pain.• Surgical removal, stripping, or bypass of the
vein is rarely needed but may be recommended in some situations.

RISK FACTORS
• Older age (> 40 years)• Male gender• Smoking• Diabetes mellitus• Hyperlipidemia• Hypertension• Hyperhomocysteinemia
When risk factors coexist, the risk increases several-fold

Symptoms
• Most asymptomatic • Intermittant claudication• Rest pain• Ulcers and gangrene

INTERMITTENT CLAUDICATION (LEG ATTACK)
• Derived from the Latin word claudicatio i.e. “to limp”• Caused by PAD in the lower extremities• Characterized by pain, ache, cramp, tightness or sense
of fatigue in leg muscles with activity • Symptoms relieved by rest • Results in reduced mobility and quality of life
WHAT CAUSES INTERMITTENT CLAUDICATION?
• Atherosclerosis in peripheral arteries of legs
During exercise, oxygen demand increases
Muscles operate anaerobically
Produce lactic acid and other metabolites
Leg pain• Lactic acid and other metabolites washed away on rest

INTERMITTENT CLAUDICATION IS INDICATIVE OF SYSTEMIC ATHEROSCLEROSIS
• 40-60% of patients with intermittent claudication have concomitant CAD

PRIMARY SITES OF INVOLVEMENT
Femoral & Popliteal arteries: 80-90%
Tibial & Peroneal arteries: 40-50%
Aorta & Iliac arteries: 30%

DIAGNOSIS
• History taking• Careful examination of leg• Pulse evaluation• Ankle-brachial index (ABI):
SBP in ankle (dorsalis pedis and posterior tibial arteries)___________________________________
SBP in upper arm (brachial artery)


WHY IS IT NECESSARY TO TREAT INTERMITTENT CLAUDICATION ?
• Symptoms worsen in 25% of patients• Approximately 5% will require
amputation within 5 years• Around 5-10% have critical limb
ischemia; risk of limb loss

GOALS OF TREATMENT
• To relieve exertional symptoms and improve walking capacity
• To improve quality of life• To reduce total mortality as well as
cardiac and cerebrovascular morbidity and mortality

MANAGEMENT
• Risk factor modification• Exercise therapy• Antiplatelet therapy• Medical therapy targeted at symptoms• Revascularisation procedures• Amputation needed in some cases

Thank you …
Top Related