





Languages
Pages
Legal


Clinical Endocrinology. 2018;89:535–553. wileyonlinelibrary.com/journal/cen | 535© 2018 John Wiley & Sons Ltd
Received:29April2018 | Revised:25May2018 | Accepted:28May2018DOI: 10.1111/cen.13753
R E V I E W A R T I C L E
Pharmacological and surgical treatment of nonreproductive outcomes in polycystic ovary syndrome: An overview of systematic reviews
Chau T. Tay1,2 | Anju E. Joham1,2 | Danielle S. Hiam3 | Moustafa A. Gadalla4,5 | Jyotsna Pundir6,7 | Shakila Thangaratinam7 | Helena J. Teede1,2 | Lisa J. Moran1,4
1MonashCentreforHealthResearchandImplementation,SchoolofPublicHealthandPreventiveMedicine,MonashUniversity,Melbourne,Vic.,Australia2DepartmentofDiabetesandVascularMedicine,MonashHealth,Melbourne, Vic.,Australia3InstituteofHealth,ExerciseandSport,VictoriaUniversity,Melbourne, Vic.,Australia4RobinsonResearchInstitute,DisciplineofObstetricsandGynaecology,UniversityofAdelaide,Adelaide,SA,Australia5DepartmentofObstetricsandGynaecology,Women’sHealthHospital,AssiutUniversity,Assiut,Egypt6CentreofReproductiveMedicine, StBartholomew’sHospital,London,UK7BartsResearchCentreforWomen’sHealth(BARC),BartsandtheLondonSchoolofMedicineandDentistry,QueenMaryUniversityofLondon,London,UK
CorrespondenceChauT.Tay,MonashCentreforHealthResearchandImplementation,SchoolofPublicHealthandPreventiveMedicine,MonashUniversity,Melbourne,Vic.,Australia.Email:[email protected]
Funding informationNationalHealthandMedicalResearchCouncil;NationalHeartFoundationofAustralia;CREinPCOSentrylevelscholarship
SummaryBackground: Polycystic ovary syndrome (PCOS) affects up to13%womenand isassociatedwith significant complications. The quality of evidence supporting therecommendationsontreatmentofnonreproductiveoutcomesinPCOSisunknown.Objective: To summarize and appraise the methodological quality of systematicreviewsandmeta-analysesevaluatingpharmacologicalandsurgicaltreatmentsfornonreproductiveoutcomesinPCOS.Methods: A literature search from MEDLINE, EMBASE, CINAHL PLUS andPROSPEROwas performed from inception until 15th of September 2017. Articleselection,dataextractionandqualityappraisalofincludedreviewswereperformedinduplicate.Anarrativesynthesisofthefindingswasconducted.Results:Thisoverviewincluded31reviews.Thequalitywaslowfor7(23%),moder-ateforsixteen(52%)andhighfor8reviews(26%).Tworeviewsassessedpsychologi-caloutcomes.Metforminimprovedanthropometric(7of10reviews),metabolic(4of14reviews)andendocrineoutcomes (3of twelve reviews).Thiazolidinediones im-provedmetabolic (2of5 reviews)andendocrineoutcomes (oneof5 reviews)butworsenedweightgain(5of5reviews).Combinedoralcontraceptivepill(COCP)im-provedclinicalhyperandrogenism(2of2reviews).Statinsimprovedlipidprofile(3of3reviews)andtestosteronelevel(2of3reviews).Therewasnoconclusiveevidencefromincludedsystematicreviewsregardingtheuseofotherinterventions.Conclusions:Thereisreliableevidenceregardingtheuseofmetforminforanthropo-metricoutcomesandCOCPsforhyperandrogenisminwomenwithPCOSbutnotforotherinterventions.ThereissignificantgapinknowledgeregardingthemanagementofpsychologicaloutcomesinwomenwithPCOSwhichneedsfurtherevaluation.
K E Y W O R D S
meta-analysis,overview,polycysticovarysyndrome,systematicreview,treatment
1 | INTRODUC TION
Polycysticovarysyndrome(PCOS)isacommonendocrinopathyaf-fectingupto13%ofreproductive-agedwomen.1PCOSisdiagnosed
basedonthepresenceof2ofthefollowing3reproductivefeatures:menstrualorovulatorydysfunction,clinicalorbiochemicalhyperan-drogenismand/orpolycysticovarianmorphologyonultrasonogra-phywithexclusionofothercausesofhyperandrogenism.2-5Whilst

536 | TAY eT Al.
theaetiology isnotfullyunderstood, insulinresistanceandhyper-androgenismarethe2keyhormonaldisturbancesthatunderpinthecondition.2,6,7
Polycystic ovary syndromehas a broad rangeof clinicalmani-festationsthatvaryacrossphenotypes,ethnicitiesand lifestages.Youngwomentypicallypresentwithdermatologicalcomplaints(hir-sutism or acne) or reproductive problems (oligo-/amenorrhoea orinfertility).4,8Metabolic features of PCOS include a predispositiontodevelopobesity,metabolicsyndrome,type2diabetes,hyperten-sionandnonalcoholicfatty liverdisease.9-12Psychologically,PCOSincreasestheriskofanxiety,depressionandlowqualityoflife.13-15 Thereare increasedpregnancycomplications includinggestationaldiabetes mellitus, gestational hypertension, preterm labour andpreeclampsiaandalso increased riskofendometrialneoplasia.16,17 ThesenonreproductivefeaturesinPCOScontributetoasignificanthealthandeconomicburden.18
The management of PCOS should encompass treating fertil-ity and nonreproductive outcomes such as reducing clinical symp-toms of hyperandrogenism, improvingmetabolic health, improvingpsychological well-being and preventing long-term health risks.6 Evidence-basedguidelinespublishedbytheAustralianPCOSAllianceandotherprofessionalspecialtysocietypositionstatementsrecom-mend lifestyle interventionsasfirst-linetreatmentforwomenwithPCOS.A5%-10%reductioninbodyweightiseffectiveinimprovinganthropometric, reproductive,metabolicandpsychological aspectsof PCOS.2-5,7,19,20Most guidelines discussed 3main pharmacologi-caltherapycategories,namelyinsulinsensitizers(eg,metforminand thiazolidinediones), anti-androgens (eg, spironolactone, flutamide and cyproterone acetate) and combined oral contraceptive pills(COCP).2-5,7,21,22 Bariatric surgery is also recommended for consider-ationinobesewomenwithPCOSgiventhatitisaneffectivemeansofweightreductionwhichmayimprovetheclinicalfeaturesofPCOS.2-5,7,23
However,thequalityofevidencesupportingtheserecommen-dationsforPCOS-relatednonreproductiveoutcomesisnotknown.Whiletherehasbeenan increasingnumberofsystematicreviewspublishedsummarizingtheevidenceofdifferentpharmacologicalorsurgicaltherapiesonthenonreproductiveoutcomesinPCOS,con-clusionsaredifficulttointerpretduetodiversemethodologiesandqualityofboththesystematicreviewsandtheirincludedstudies.
Theaimofthisstudywastoconductanoverviewofsystematicreviews evaluating pharmacological or surgical therapy for nonre-productiveoutcomes inwomenwithPCOS to summarize and ap-praisetheresultsandmethodologicalquality.
2 | METHODS
2.1 | Protocol and registration
This review was designed and reported in accordance with thePreferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)guidelines.24Anaprioristudyprotocolwasreg-isteredwithPROSPERO(CRD42016052649).Ethicsapplicationwasnotrequired.
2.2 | Literature search
TheelectronicdatabasesMEDLINEin-processandothernonindexedcitations(OvidMEDLINE(R)In-Process&OtherNon-IndexedCitations,OvidMEDLINE(R)DailyandOvidMEDLINE(R)1946toPresent),OvidEMBASE(EBMReviews—CochraneDatabaseofSystematicReviews2005to15September2017,EBMReviews—ACPJournalClub1991toSeptember2017,EBMReviews—DatabaseofAbstractsofReviewsofEffects1stQuarter2016,EBMreviews—CochraneCentralRegisterof Controlled Trials September 2017, EBM Reviews—CochraneMethodology Register 3rd quarter 2012, EBM Reviews—HealthTechnology Assessment 4th Quarter 2016, EBM Reviews—NHSEconomicEvaluationDatabase1stQuarter2016)andCINAHLPLUSweresearchedtoidentifyrelevantpublishedarticles.Additionalongo-ingreviewswereidentifiedfromsearchingtheinternationalprospec-tiveregisterofsystematicreviewsPROSPERO(http://www.crd.york.ac.uk/PROSPERO/).Theliteraturesearchwaslastupdatedonthe15th ofSeptember2017.The search termsused included “PCOS,” “poly-cysticovarysyndrome,”“Stein-Leventhal,”“systematic,”“review,”and“meta-analysis”withthecompletesearchstrategyforeachdatabaseprovided inAppendixS1 (found in theSupporting Information).Thesearchstrategywaslimitedtohumanstudiesonly.
2.3 | Eligibility criteria and study collection
Articleswereincludediftheymetthefollowinginclusioncriteria:originalsystematicreviewormeta-analysis;PCOSwastheprimaryfocusofthereviewwitharticlesinwhichPCOSwasasecondaryconditionassessedaspartofabroadertopicexcluded;clearsearchstrategywithatleastkeywordsortermsincluded,documentationofsearchreturnsandperformedqualityappraisaloftheincludedstudies; published in English; and published from year 2009 on-wardsgiventhiswaswhenthePRISMAstatementwaspublishedtoguidereportingofsystematicreviewsandmeta-analyses.24
The outcomes of interestwere anthropometric (weight, bodymass index (BMI), waist-hip ratio, waist circumference or bodycomposition), endocrine (total or free testosterone, sex hormonebinding globulin (SHBG), free androgen index (FAI), dehydroepi-androsteronesulphate(DHEAS),dehydroepiandrosterone(DHEA),androstenedioneorclinicalhyperandrogenism),metabolic(glucoseintolerance, surrogate markers of insulin resistance, lipid profileor blood pressure) and psychological (quality of life, anxiety ordepression).
2.4 | Study selection and data extraction
Identified articles from the literature searchwere screened in atwo-step process. First, the titles and abstracts were screenedforsuitability.Second,allarticlesthatmeettheinclusioncriteriafromthefirststepwereretrievedfordetailedfull-textassessmenttodetermineeligibility.Studyselectionwasperformed indepen-dentlyinduplicateby3investigators(C.T.T,D.S.HandL.J.M)withanydiscrepanciesresolvedbyconsensus.

| 537TAY eT Al.
Datacollectedfromtheeligiblearticlesincludedauthorship,pub-licationyear,countryofauthors’origin,typesofstudyeligibleforthesystematicreview,dateofliteraturesearch,languagerestriction,ad-herencetoasystematicreviewguideline,presenceofmeta-analysis,the authors’ interpretation of quality assessment of the includedstudies,numberofincludedstudiesandparticipantsinvolvedandtheParticipant,Intervention,Comparison,OutcomesandStudies(PICOS)frameworkofthestudy. If theauthorsdidnot interpretthequalityoftheincludedstudiesnorsummarizetheoverallqualityoftheen-tirestudy,thesectiononqualityassessmentwasbedocumentedas“unclear.”Dataextractionwasconductedindependentlyinduplicate(C.T.T,L.J.MandM.A.G)withanydiscrepanciesresolvedbyconsensusanddiscussionwithathirdinvestigator(D.S.H).
2.5 | Quality assessment (AMSTAR)
The Assessing the Methodological Quality of Systematic Reviews(AMSTAR)toolwasemployedtoappraisethequalityoftheincludedsystematic reviews.25,26 AMSTAR evaluates the methodological as-pectsof systematic reviewsusing11 items: (i) theprovisionofanaprioridesign,(ii)duplicationofstudyselectionanddataextraction,(iii)conductionofacomprehensiveliteraturesearch,(iv)inclusionofgreyliteratureinthereview,(v)availabilityofalistoftheincludedandex-cludedstudies, (vi)descriptionof thecharacteristicsof the includedstudies, (vii) clear documentation of the scientific quality of the in-cluded studies, (viii) considerationof the scientificqualityof the in-cludedstudiesinformulatingconclusions,(ix)appropriateanalysisofresultsdependingonheterogeneity,(x)assessmentofpublicationbiasand(xi)considerationofconflictofinterestofboththesystematicre-viewandtheincludedstudies.26Eachitemwasgiven1pointifitwasdeterminedas“yes”and0point if itwasdeterminedas“no”or“notapplicable.”The reviewswerecategorizedas lowquality if the totalAMSTARscorewas≤3,moderatequality ifthetotalAMSTARscorewasbetween4to7,andhighqualityifthetotalAMSTARscorewas≥8.
Qualityassessmentofalleligiblesystematic reviewswascon-ductedindependentlyinduplicate(C.T.T,L.J.MandM.A.G)withanydisagreements resolvedby consensusanddiscussionwitha thirdinvestigator(D.S.H).
2.6 | Data synthesis
Anarrativesynthesisoffindingsfromtheincludedreviewswasper-formed.Resultswerepresentedaccordingtothedifferenttypesofintervention.Statisticallysignificantoutcomesofinterestwerepre-sentedifameta-analysiswasperformedbythereview.
3 | RESULTS
3.1 | Literature search
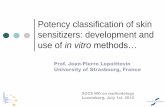
The electronic database search retrieved 978 articles, and an addi-tional60wereidentifiedfromPROSPERO.Afterremovingthedupli-cates,831articlesremainedforscreening.Atotalof564articleswere
excluded after reviewing the title and abstract leaving 267 articlesavailableforfull-textevaluation.Atotalof140articleswereeligibleforanalysisofwhich33wererelatedtotreatmentofnonreproductiveoutcomes.Ofthese,2articleswereapriorversionofasystematicre-view,andtherefore,weonlyincludedthemostrecentpublications.27,28 Finally,31systematicreviewswereincludedinthisstudy.ThePRISMAflowdiagramis illustrated inFigure1.The listofexcludedarticles isavailableinAppendixS2(foundintheSupportingInformation).
3.2 | Study characteristics
ThestudycharacteristicsandPICOframeworkoftheincludedsys-tematicreviewsaresummarizedinTable1.ThecountryoforiginoftheauthorsincludedChina(n=11),29-39Australia(n=6),40-45UnitedKingdom (n=5),43,45-48 the United States of America (n=4),49-52 India (n=3),44,52,53 Canada (n=3),50,54,55 Brazil (n=2),41,56 Iran (n=2),40,54Columbia(n=1),46Greece(n=1),57Italy(n=1),57Spain(n=1),58Scotland(n=1),59Luton(n=1),48Netherlands(n=1)41 and Saudi Arabia (n=1).46 Thirteen reviews explicitly included rand-omizedcontroltrials(RCTs)only29-32,34,36,38,42,43,46,53,57,59;5reviewsincluded RCTs and phase-1 data of cross-over trials39,41,44,45,52; 2 reviews included RCTs and prospective trials50,56; 2 reviews in-cluded RCTs and observational studies49,58; 1 review included RCTs, comparative studies and case series with >5 patients55; 2 reviews includedallclinical trials40,54;3 reviews includedall studytypes35,48,51;and3reviewsdidnotstateaninclusioncriteriaforthestudytype.33,37,47Fifteenreviewsdidnotsetalanguagerestrictionin their literature search30,31,39-41,43-46,49,50,52,56-58; 11 reviews re-strictedtheirsearchtoEnglishpublicationsonly32,34-38,42,51,53,55,59; 1reviewrestricteditslanguagetoEnglishandPersian54; 1 review re-stricteditslanguagetoEnglishandChinese33;and3reviewsdidnotstateifanylanguagerestrictionwasapplied.29,47,48Twelvereviewsreportedfollowingaguidelineongoodpracticeinconductingsys-tematic reviews30,31,35,39,41,44-47,53,57,58; 25 reviews included meta-analyses29-38,41-47,49-53,55-57; and18 reviewsdidnotprovideaclearstatementastotheoverallqualityassessmentoftheincludedarti-cles.31,33,34,36,37,41-44,47,51-58Thenumberofstudiesincludedineachsystematic review ranged from1 to35, and the total participantsrangedfrom16to3992.Eighteen(58%)ofthesystematicreviewshadlessthan10studiesincludedintotal.29-32,36,38-42,44,46-48,52,56,57,59
3.3 | Methodological quality of systematic reviews
TheAMSTARscoresoftheincludedsystematicreviewsareprovidedinAppendixS3(foundintheSupportingInformation).Majorityoftheincludedsystematicreviewswereoflow(n=7;23%)42,47,48,54,55,58,59 to moderate quality (n=16; 52%)29-34,36,37,39,40,43,49-51,53,56 withonly8gradedhighquality (n=8;26%).35,39,41,44-46,52,57Commonlyunreported itemswereconsiderationof conflictof interestof theincludedstudies(n=28;90%),presenceofanaprioristudydesign(n=23; 74%), a list of the excluded articles (n=23; 74%), inclu-sionofgrey literature (n=22;71%),duplicationofstudyselectionor data extraction (n=21; 68%), formulation of study conclusion

538 | TAY eT Al.
basedonthescientificqualityoftheincludedstudies(n=18;58%)andconductionofacomprehensiveliteraturesearch(n=18;58%).Assessmentofpublicationbiaswasnotappropriatelyperformedin9 reviews (29%),documentationof thescientificqualityof the in-cluded studieswasunsatisfactory in6 reviews (19%), andhetero-geneitywasnot taken intoaccountby2 reviews (6%).All reviewsreportedthestudycharacteristicsoftheincludedstudies.
3.4 | Types of intervention
The typesof treatments assessedweremetformin, thiazolidinedi-one,oralcontraceptivepills(OCP),anti-androgens,statins,orlistat,bariatric surgery and antidepressants. Nonconventional therapiessuchasvitaminD,inositol,N-acetyl-cysteineandantioxidantswerealsoincludedinthisreview.
3.4.1 | Insulin sensitizer: metformin
Sixteen reviews evaluated the efficacy of metformin(Table2).29,30,32,34-36,38,41,43,45,46,49,53,56,57,59 Five were rated highquality,10wereratedmoderatequality,and1wasratedlowquality.
A total of 174 trials and10525 adolescent and adult participantswere involved.
Anthropometricoutcomeswereassessedby10reviews.Sevenreviews (n=3 comparing metformin vs thiazolidinediones,29,30,34 n=2 comparing metformin vs placebo,45,53 n=1 comparing met-forminvsCOCPs46andn=1comparingcombinationtherapywithmetformin and clomiphene citrate vs clomiphene citrate alone)59 reportedresultsfavouringmetforminintermsofBMIand/orwaist-hipratio.Therewasnosignificantdifferenceinanthropometricout-comeswhenmetforminwascompared toacarbose38ororlistat,56 orwhencombinationtherapywithmetforminandstatinwascom-pared to metformin alone.36 Endocrine outcomes were assessedby 12 reviews. Three reviews (n=2 comparingmetformin vs pla-cebo45,53 and n=1 comparing metformin and clomiphene citratevsclomiphenecitratealone59) reportedreductions intestosteronewhenusingmetformin.Therewasno significantdifference in en-docrine outcomes whenmetformin was compared to acarbose,38 OCP,46vitaminD,32,57thiazolidinediones,29,30,34orlistat,56inositol43 or combination therapy with statin.36 Metabolic outcomes wereassessed by 14 reviews with 4 reviews reporting beneficial out-comes favouringmetformin for theprevalenceof type2diabetes
F IGURE 1 Studyselectionprocess

| 539TAY eT Al.
mellitusorprediabetes(n=1comparingmetforminvsOCP),46totalcholesterol and low-density lipoprotein (LDL) (n=1 comparingmetformin vsOCP),46 blood pressure (n=2 comparingmetforminvs placebo),45,53 triglycerides (n=1 comparing metformin vs pla-cebo,53n=1comparingmetforminvsthiazolidinediones),34glucose(n=1comparingmetforminvsplacebo),45 insulin (n=1comparingmetforminvsplacebo)45andglucose/insulinratio(n=1comparingmetformin vs placebo).53No significantmetabolic outcomesweredetected when comparing metformin to vitamin D,32,57 orlistat,56 inositol,43 acarbose38 orwith the additionofmetformin to folliclestimulatinghormone (FSH)-containinggonadotrophinovulation in-ductionorclomiphenecitrate.59Psychologicaloutcomeswerenotassessedbyanyoftheabovereviews.
3.4.2 | Insulin sensitizer: thiazolidinediones
Fivereviews29-31,34,45evaluatedtheefficacyofthiazolidinedionesinwhichonewashighqualityand4weremoderatequality(Table2).Atotalof74trialsand5282participantswithPCOSwereinvolved.All5reviewsassessedtheanthropometric,endocrineandmetabolicout-comesofthiazolidinediones(n=3comparedwithmetformin,29,30,34 n=2comparedwithplacebo).31,45BMIwassignificantlyincreasedwith thiazolidinediones in all 5 reviews while endocrine benefits(reducedfreetestosterone)werereportedinonereviewwhencom-paredtometformin.34Formetabolicoutcomes,onereviewshowedimprovedfastingglucoseandinsulinincomparisonwithplacebo,31 one review showed improved fasting insulin and homoeostaticmodelassessmentofinsulinresistance(HOMA-IR)whencomparedto metformin,30 and one review showed worsened triglycerideswhencomparedtometformin.34Psychologicaloutcomeswerenotassessedbyanyoftheabovereviews.
3.4.3 | Insulin sensitizer: inositol
Three reviews43,45,48 evaluated the efficacy of inositol (Table2).The reviewswereof low (n=1),moderate (n=1)andhigh (n=1)quality.Atotalof62trialswith5072womenwithPCOSwerein-volved. In all 3 reviews, inositol was compared against placebo.Anthropometric outcomes were reported by 2 reviews with onereview reporting reduced BMI and waist-hip ratio.48 Endocrineoutcomeswereassessedbyall3reviewswith2ofthesereportingbenefits(testosterone,DHEASorandrostenedione).43,48Metabolicoutcomeswerealsoassessedbyall3reviewswith2reviewsreport-ingreducedinsulin,43,48onereviewreportingreducedglucoseandHOMA-IR,43 and one review reporting improved blood pressure,triglycerides and high-density lipoprotein (HDL).48 Psychologicaloutcomeswerenotassessedbyanyoftheabovereviews.
3.4.4 | Hormonal therapy: combined oral contraceptive pill
The efficacy of COCPs was assessed by 4 reviews46,49,50,58 (Table3) of low to high quality (n=1 high, n=2moderate, and
n=1 low). Results from88 trials involving3722 adolescent andadult women with PCOS were analysed. Anthropometric out-comes were reported by one review with COCP being associ-atedwitha lesserreductionofBMIcomparedwithmetformin.46 Endocrineoutcomeswereassessedby2reviewswithonereport-ing greater acne reduction when compared to metformin46 and one review reporting general improvement in clinical hyperan-drogenismwhenusingCOCPasmonotherapyor in combinationwithmetformin.58 Two reviews assessedmetabolic outcomesofwhichonereviewreportedthatCOCPusewaslesseffectivethanmetformininreducingtheprevalenceofdysglycaemia,totalcho-lesterolandLDL,46andonereviewreportedthatCOCPusewasassociatedwith increasedHDL and triglycerides comparedwithbaseline.50Psychologicaloutcomeswerenotassessedbyanyoftheabovereviews.
3.4.5 | Hormonal therapy: anti- androgens
Onehigh-qualityreviewevaluatedthesideeffectsofanti-androgensandtheirefficacyonmetabolicoutcomes(Table3).49Nosignificanteffectsonmetabolicoutcomeswerereported.
3.4.6 | Weight loss therapy: orlistat
Orlistatwasevaluatedbyonemoderatequalityreviewincompari-sonwithplacebo,metforminorotheranti-obesitydrugs56(Table4)where9trialsand602adolescentandadultwomenwithPCOSwereinvolved.Meta-analysisofthestudiescomparingorlistattoplacebowasnotpossiblebutthesystematicreviewreportedimprovementsin anthropometric (BMI, weight, waist circumference or waist-hipratio), endocrine (testosterone) andmetabolicoutcomes (triglycer-ides,HDL,LDL,HOMA-IRandinsulin).Meta-analysisofthestudiescomparingorlistattometforminshowednosignificantdifferences.56 Psychologicaloutcomeswerenotassessedbytheabovereview.
3.4.7 | Weight loss therapy: bariatric surgery
TheeffectofbariatricsurgeryinwomenwithPCOSwasevaluatedin 2 low-quality reviews47,55 (Table4). They involved 19 trials and2394participantswithandwithoutPCOS.Bothreviewscomparedthesamegroupofwomenbeforeandafterbariatricsurgery.Bothreviewsassessedanthropometricandendocrineoutcomesandre-portedreductionsinBMI,percentageofexcessweightlossandhir-sutism.47,55Metabolicoutcomeswereassessedbyonereviewandshowedreductionsinbloodpressure,improvementindyslipidaemia,normalizationofglucose levels, improvementofglycaemiccontrolandresolutionoftype2diabetesmellitus.47Psychologicaloutcomeswereassessedbyonereviewandreportedbenefitsindepression.47
3.4.8 | Other therapy: statins
Three reviews evaluated the efficacy of statins36,42,44 (AppendixS3, found in the Supporting Information) with rating of one low,

540 | TAY eT Al.
TABLE 1 Studycharacteristics
Aut
hor (
y)Co
untr
yIn
clud
ed s
tudy
type
Dat
e of
last
lit
erat
ure
sear
chLa
ngua
ge
Syst
emat
ic
revi
ew
guid
elin
e fo
llow
ed
Met
a-
anal
ysis
pe
rfor
med
Num
ber o
f in
clud
ed
pape
rs
Tota
l num
ber
of in
clud
ed
part
icip
ants
Popu
latio
n an
d PC
OS
diag
nost
ic c
riter
ia
AlKhalifahetal
(2016)
46Canada,Saudi
Arabia,Columbia,
UnitedKingdom
RCTs
15-Jan
All
Yes
Yes
417
0Adolescents(11-19y)
ESHRE/ASRM
Aminietal(2015)54
Iran
Experimentalor
quasiexperimental
trials
13-Nov
English,
Persian
No
No
1183
4Ir
ania
n ESHRE/ASRM
Azadi-Yazdietal
(2017)
40Iran,Australia
Clinicaltrials
17-Jan
All
No
No
618
3Diagnosticcriterianotstated
Bordewijketal
(2017)
41Netherlands,
Australia,Brazil
RCTsandphase1of
cross-overtrials
16-Sep
All
Yes
Yes
526
4Anovulatorywomen
undergoingovulationinduction
withFSHESHRE/ASRM
Butterworthetal
(2016)
47UnitedKingdom
Notstated
15-Mar
Notstated
Yes
Yes
626
4ESHRE/ASRM
Domecqetal
(2013)
49UnitedStates
RCTsandcomparative
observationalstudies
11-Apr
All
No
Yes
2213
35Diagnosticcriterianotstated
Duetal(2012)31
China
RCTs
12-Jun
All
Yes
Yes
828
6ESHRE/ASRM
Duetal(2012)29
China
RCTs
12-Feb
Notstated
No
Yes
626
7ESHRE/ASRM
Duetal(2012)30
China
RCTs
11-Nov
All
Yes
Yes
627
8ESHRE/ASRM
Fangetal(2017)32
China
RCTs
15-Dec
English
No
Yes
950
2ESHRE/ASRM
Galazisetal
(2011)
48UnitedKingdom,
Luton
Allstudytypes
10-Jul
Notstated
No
No
847
9Diagnosticcriterianotstated
Gaoetal(2012)42
Australia
RCTs
11-Sep
English
No
Yes
425
4Diagnosticcriterianotstated
Gilletal(2014)59
Scotland
RCTs
13-May
English
No
No
412
9Clomipheneresistantwomen
Diagnosticcriterianotstated
Graffetal(2016)56
Brazil
RCTsandprospective
studies
15-May
All
No
Yes
960
2Withoutpre-existingdiabetes,
13-44y
ESHRE/ASRM
Halperinetal
(2011)
50Canada,United
States
RCTsandprospective
cohorts
10-Apr
All
No
Yes
3579
8Withoutpre-existingdiabetes,
13-44y
ESHRE/ASRM
Heetal(2015)51
UnitedStates
Allstudytypes
15-Jan
English
No
Yes
30 (7regarding
intervention)
3182
(2
83
includedfor
intervention)
ESHRE/ASRM
Jiaetal(2015)33
China
Notstated
14-Sep
English,
Chinese
No
Yes
1723
97ESHRE/ASRM

| 541TAY eT Al.
Aut
hor (
y)Co
untr
yIn
clud
ed s
tudy
type
Dat
e of
last
lit
erat
ure
sear
chLa
ngua
ge
Syst
emat
ic
revi
ew
guid
elin
e fo
llow
ed
Met
a-
anal
ysis
pe
rfor
med
Num
ber o
f in
clud
ed
pape
rs
Tota
l num
ber
of in
clud
ed
part
icip
ants
Popu
latio
n an
d PC
OS
diag
nost
ic c
riter
ia
Lietal(2011)34
China
Parallel-group
designedRCTs
10-May
English
No
Yes
1045
9Diagnosticcriterianotstated
Mendozaetal
(2014)
58Spain,Italy
RCTs,nonrandomized
studiesand
noncontrolled
studies
13-Oct
All
Yes
No
2715
89Diagnosticcriterianotstated
Mengetal(2016)35
China
Allstudytypes
15-Dec
English
Yes
Yes
34 (7regarding
interven-
tion)
3117
(1
41
includedfor
intervention)
ESHRE/ASRM
Pateletal(2017)53
Indi
aRCTs
16-May-
English
Yes
Yes
1459
316-45y(excludepregnancyor
clomipheneresistant)
Diagnosticcriterianotstated
Pergialiotisetal
(2017)
57Greece
RCTs
16-Sep
All
Yes
Yes
964
7Diagnosticcriterianotstated
Pundiretal(2017)43
UnitedKingdom,
Australia
RCTs
16-Aug-
All
No
Yes
1060
1Diagnosticcriterianotstated
Ravaletal(2011)44
India,Australia
RCTsandphase1of
cross-overtrials
11-Jul
All
Yes
Yes
424
4ESHRE/ASRM
Skublenyetal
(2016)
55Canada
RCTs,comparison
studies,andcase
series>5patients
Notstated
English
No
Yes
1321
30WomenwithorwithoutPCOS
Diagnosticcriterianotstated
Sunetal(2015)36
China
RCTs(excludingtrails
comparingstatins
withOCPorother
statins)
14-Oct
English
No
Yes
928
2Diagnosticcriterianotstated
Tangetal(2012)45
UnitedKingdom,
Australia
RCTsandphase1of
cross-overtrials
11-Oct
All
Yes
Yes
4439
92Oligo-oranovulatory
ESHRE/ASRM
Thakkeretal
(2015)
52India,UnitedStates
RCTsandphase1of
cross-overtrials
13-Sep
All
No
Yes
891
0ESHRE/ASRM
Xueetal(2017)37
China
Notstated
16-Apr
English
No
Yes
1685
5ESHRE/ASRM
Zhangetal(2014)38
China
RCTs
13-Sep
English
No
Yes
626
3ESHRE/ASRM
Zhuangetal
(2013)
39China
RCTsandphase1of
cross-overtrials
12-Jun
All
Yes
No
116
ESHRE/ASRM
RCT,randomizedcontroltrials;ESHRE,EuropeanSocietyofHumanReproductionandEmbryology;ASRM,AmericanSocietyforReproductive
Medicine;OCP,oralcontraceptivepill.

542 | TAY eT Al.
TABLE 2 Resultsofsystematicreviewsregardinginsulinsensitizers
Revi
ews
AM
STA
RQ
ualit
y of
in
clud
ed s
tudi
esO
utco
mes
ass
esse
dCo
mpa
rison
Sign
ifica
nt re
sults
Metformin
AlKhalifahetal
(2016)
46High
Verylowtolow
Anthropometric
BMI
MetforminvsOCP
Anthropometric
BMI(WMD−4.02,95%CI−5.23to−2.81)
Reproductive
Hirsutism,acne,
testosterone
Reproductive
Acnescores(W
MD0.3,95%0.05to0.55)
a
Metabolic
Dysglycaemia,
cholesterol,TG,
HDL,LDL
Metabolic
Dysglycaemia(riskratio0.41,95%CI0.19to
0.86)
Cholesterol(W
MD−43.23,95%CI−64.15to
−22.32)
LDL(WMD−35.5,95%CI−57.45to−13.33)
Psychologic
–N
A
Bordewijketal
(2017)
41High
Unclear
Anthropometric
–Metformin+
ovulation
inductionvs
ovulation
induction
Reproductive
–
Metabolic
Insulin,glucose
Psychologic
–
Mengetal
(2016)
35High
RCTs:lowto
moderateriskof
bias;observa-
tionalstudies:
highriskofbias
Anthropometric
–Metforminvsno
treatment
NA
Reproductive
–
Metabolic
–
Psychologic
–
Pergialiotisetal
(2017)
57High
Unclear
Anthropometric
–Metformin±vitD
vsvitaminD
NA
Reproductive
DHEAS,SHBG
Metabolic
Glucose,insulin
Psychologic
–
Tangetal
(2012)
45High
Verylowtolow
Anthropometric
BMI,waist-hipratio
Metforminvs
plac
ebo
Anthropometric
Waist-hipratio(MD−0.01,95%CI−0.01to
0.00)
Reproductive
Testosterone,SHBG
Reproductive
Totaltestosterone(MD−0.60,95%CI−0.73to
−0.48)
Metabolic
BP,glucose,insulin,
cholesterol,TG
Metabolic
SystolicBP(MD−3.59,95%CI−5.13to−2.04)
Glucose(MD−0.15,95%CI0.25to−0.06)
Insulin(MD−3.51,95%CI−6.50to0.53)
Psychologic
–
Domecqetal
(2013)
49Moderate
RCTs:lowto
moderateriskof
bias;observa-
tionalstudies:
highriskofbias
Anthropometric
–Metformin(no
comparators)
NA
Reproductive
–
Metabolic
–
Psychologic
–
(Con
tinue
s)

| 543TAY eT Al.
Revi
ews
AM
STA
RQ
ualit
y of
in
clud
ed s
tudi
esO
utco
mes
ass
esse
dCo
mpa
rison
Sign
ifica
nt re
sults
Duetal(2012)29
Moderate
High
Anthropometric
BMI
Metforminvs
thiazolidinediones
Anthropometric
BMI(SMD−0.4,95%CI0.16to0.65)
Reproductive
Testosterone
Metabolic
Glucose,HOMA-IR
Psychologic
–
Duetal(2012)30
Moderate
Verylowtolow
Anthropometric
BMI
Metforminvs
pioglitazone
Anthropometric
BMI(SMD−0.25,95%CI0.01to0.49)
Reproductive
Testosterone,hirsutism
Metabolic
Insulin(SMD0.37,95%CI−0.61to−0.13)a
HOMA-IR(SMD0.32,95%CI−0.57to−0.06)a
Metabolic
Glucose,insulin,
HOMA-IR
Psychologic
–
Fangetal
(2017)
32Moderate
Lowtomoderate
riskofbias
Anthropometric
–Metforminvs
vitaminD
NA
Reproductive
–
Metabolic
Cholesterol,TG,HDL,
LDL,insulin,glucose,
QUICKI,HOMA-IR
Psychologic
–
Graffetal
(2016)
56Moderate
Unclear
Anthropometric
BMI,weight,waist
circumference
Metforminvs
orlistat
NA
Reproductive
Testosterone
Metabolic
Insulin,HOMA-IR,
cholesterol,TG,HDL,
LDL
Psychologic
–
Lietal(2011)34
Moderate
Unclear
Anthropometric
BMI
Metforminvs
thiazolidinediones
Anthropometric
BMIat3-mo(SMD−2.47,95%CI−3.33to−1.62)
BMIat6-mo(SMD−0.70,95%CI−0.76to
−0.65)
Reproductive
Hirsutism,androsten-
edione,testosterone,
DHEA
Reproductive
Freetestosterone(SMD0.36,95%CI−0.03to
−0.69)
a
Metabolic
Glucose,insulin,
HOMA-IR,HDL,LDL,
TG
Metabolic
TGat6-mo(SMD−1.13,95%CI−1.68to−0.57)
Psychologic
–
TABLE 2 (Continued)
(Con
tinue
s)

544 | TAY eT Al.
Revi
ews
AM
STA
RQ
ualit
y of
in
clud
ed s
tudi
esO
utco
mes
ass
esse
dCo
mpa
rison
Sign
ifica
nt re
sults
Pateletal
(2017)
53Moderate
Unclear
Anthropometric
BMI,waist-hipratio
Metforminvs
plac
ebo
Anthropometric
BMI(MD−1.18,95%CI−2.0to−0.36)
WHR(MD−0.02,95%CI−0.03to0.00)
Reproductive
Hirsutism,testosterone,
freetestosterone,
FAI,SHBG,DHEAS
Reproductive
Testosterone(MD−14.32,95%CI−26.80to
−1.85)
Metabolic
Bloodpressure,
cholesterol,TG,HDL,
LDL,
glucose,insulin,
glucose/insulinratio,
HOMA-IR,
QUICKI
Metabolic
SystolicBP(MD−4.92,95%CI−7.51to−2.33)
DiastolicBP(MD−1.51,95%CI−2.23to−0.79)
TG(MD−10.74,95%CI−17.93to−3.56)
Glucose/insulinratio(MD2.28,95%CI1.16to
3.41)
Psychologic
–
Pundiretal
(2017)
43Moderate
Unclear
Anthropometric
–Metforminvs
inositol
NA
Reproductive
Androstenedione,
testosterone,DHEAS,
SHBG
Metabolic
Insulin,glucose,
glucose/insulinratio,
HOMA-IR
Psychologic
–
Sunetal(2015)36
Moderate
Unclear
Anthropometric
BMI
Metformin+statin
vsmetformin
Metabolic
Totalcholesterol(SMD−1.28,95%CI−1.59to
−0.97)
LDL(SMD−0.74,95%CI−1.03to−0.44)
TG(SMD−1.37,95%CI−2.46to−0.28)
Reproductive
Testosterone,andros-
tenedione,DHEAS,
SHBG,FAI
Metabolic
Cholesterol,LDL,HDL,
TG,glucose,insulin,
HOMA-IR
Psychologic
–
Zhangetal
(2014)
38Moderate
Poor
Anthropometric
BMI
Metforminvs
acarbose
NA
Reproductive
Hirsutism,testosterone
Metabolic
TG,HDL
Psychologic
–
TABLE 2 (Continued)
(Con
tinue
s)

| 545TAY eT Al.
Revi
ews
AM
STA
RQ
ualit
y of
in
clud
ed s
tudi
esO
utco
mes
ass
esse
dCo
mpa
rison
Sign
ifica
nt re
sults
Gilletal(2014)59
Low
3high,1low
Anthropometric
BMI
Metformin+
clomiphenevs
clomiphene
Anthropometric
2trials:BMIwasdecreased
Reproductive
SHBG,testosterone
Reproductive
2trials:testosteronewasdecreased
Metabolic
Insulin
Psychologic
–
Thiazolidinediones
Tangetal
(2012)
45High
Verylowtolow
Anthropometric
BMI,waist,hipratio
Rosiglitazonevs
plac
ebo
Anthropometric
BMI(MD+0.68,95%CI0.40to0.96)
Reproductive
Testosterone,SHBG
Pioglitazonevs
plac
ebo
NA
Metabolic
BP,glucose,insulin,
cholesterol,TG
Psychologic
–
Duetal(2012)31
Moderate
Unclear
Anthropometric
BMI
Thiazolidinediones
vsplacebo
Anthropometric
BMI(SMD+0.39,95%CI0.13to0.66)
Reproductive
Hirsutism,testosterone
Metabolic
Insulin(SMD−0.81,95%CI−1.5to−0.12)
Glucose(SMD−0.55,95%CI−1.06to−0.05)
Metabolic
Glucose,insulin
Psychologic
–
Duetal(2012)30
Moderate
Verylowtolow
Anthropometric
BMI
Pioglitazonevs
metformin
Anthropometric
BMI(SMD0.25,95%CI0.01to0.49)
a
Reproductive
Hirsutism,testosterone
Metabolic
Insulin(SMD−0.37,95%CI−0.61to−0.13)
HOMA-IR(SMD−0.32,95%CI−0.57to−0.06)
Metabolic
Glucose,insulin,
HOMA-IR
Psychologic
–
Duetal(2012)29
Moderate
High
Anthropometric
BMI
Thiazolidinediones
vsmetformin
Anthropometric
BMI(SMD0.4,95%CI0.16to0.65)
a
Reproductive
Testosterone
Metabolic
Glucose,HOMA-IR
Psychologic
–
TABLE 2 (Continued)
(Con
tinue
s)

546 | TAY eT Al.
Revi
ews
AM
STA
RQ
ualit
y of
in
clud
ed s
tudi
esO
utco
mes
ass
esse
dCo
mpa
rison
Sign
ifica
nt re
sults
Lietal(2011)34
Moderate
Unclear
Anthropometric
BMI
Thiazolidinediones
vsmetformin
Anthropometric
BMIat3-mo(SMD2.47,95%CI−3.33to−1.62)a
BMIat6-mo(SMD0.70,95%CI−0.76to−0.65)a
Reproductive
Hirsutism,androsten-
edione,testosterone,
DHEA
Reproductive
Freetestosterone(SMD−0.36,95%CI−0.03to
−0.69)
Metabolic
Glucose,insulin,
HOMA-IR,cholesterol,
TG,HDL,LDL
Reproductive
TGat6-mo(SMD1.13,95%CI−1.68to−0.57)a
Psychologic
–
Inositol
Tangetal
(2012)
45High
Verylowtolow
Anthropometric
BMI,waist,hipratio
D-chiro-inositolvs
plac
ebo
NA
Reproductive
Testosterone,SHBG
Metabolic
BP,glucose,insulin,
cholesterol,TG
Psychologic
–
Pundiretal
(2017)
43Moderate
Unclear
Anthropometric
–Inositol(myo-or
di-chiroisomers)
vsplacebo
Reproductive
Androstenedione(SMD−1.6,95%CI−2.3to
−0.6)
Totaltestosterone(SMD−3.3,95%CI−5.1to
−1.5)
DHEAS(SMD−3.2,95%CI−5.7to−0.6)
Reproductive
Androstenedione,
testosterone,DHEAS,
SHBG
Metabolic
Insulin(SMD−2.1,95%CI−3.2to−0.9)
Glucose(SMD−1.0,95%CI−1.7to−0.2)
HOMA-IR(SMD−1.8,95%CI−2.6to−1.0)
InsulinAUC(SMD−1.6,95%CI−2.8to−0.4)
Glucose/insulinratio(SMD2.9,95%CI2.2to
3.6)
Metabolic
Insulin,glucose,
glucose/insulinratio,
HOMA-IR
Psychologic
–
Galazisetal
(2011)
48Low
4low,4high
Anthropometric
Notspecified
D-chiro-inositolvs
plac
ebo
Anthropometric
2trials:improvedBMI,waist-hipratio
Reproductive
Reproductivesteroids
Reproductive
3trials:reducedtestosterone
Metabolic
BP,cholesterol,insulin
sensitivity
Metabolic
3trials:reducedinsulin,BP,TG
Psychologic
–1trial:increasedHDL
NA,notavailable;MD,meandifference;WMD,weightedmeandifference;SMD,standardizedmeandifference;CI,confidenceinterval;BMI,bodymassindex;SHBG,sexhormonebindingglobulin;FAI,
freeandrogenindex;DHEA,dehydroepiandrosterone;DHEAS,dehydroepiandrosteronesulphate;BP,bloodpressure;HDL,high-densitylipoprotein;LDL,low-densitylipoprotein;TG,triglycerides;
HOMA-IR,homoeostaticmodelassessmentofinsulinresistance;QUIKI,quantitativeinsulinsensitivitycheckindex;AUC,areaunderthecurve;OCP,oralcontraceptivepill.
a Resultslessbeneficialthancomparator.
TABLE 2 (Continued)

| 547TAY eT Al.
TABLE 3 Resultsofsystematicreviewsregardinghormonaltherapies
Revi
ews
AM
STA
RQ
ualit
y of
in
clud
ed s
tudi
esO
utco
mes
ass
esse
dCo
mpa
rison
Sign
ifica
nt re
sults
Oralcontraceptivepills
AlKhalifahetal
(2016)
46High
Verylowtolow
Anthropometric
BMI
OCPvs
metformin
Anthropometric
BMI(WMD4.02,95%CI−5.23
to−2.81)
a
Reproductive
Hirsutism,acne,testosterone
Reproductive
Acnescores(W
MD−0.3,95%
0.05to0.55)
Metabolic
Dysglycaemia,cholesterol,TG,HDL,
LDL
Metabolic
Dysglycaemia(riskratio0.41,
95%CI0.19to0.86)
a
Cholesterol(W
MD43.23,
95%CI−64.15to−22.32)
a
LDL(WMD35.5,95%CI−57.45
to−13.33)a
Psychologic
–
Domecqetal(2013)49
Moderate
RCTs:lowto
moderaterisk
ofbias;
observational
studies:high
riskofbias
Anthropometric
Weight,BM
IOCP(no
com
para-
tor)
NA
Reproductive
–
Metabolic
Fastingglucose,postprandialglucose,
glucosetolerancetest,random
glucose,areaunderthecurveof
glucose,glucose/insulinratio,
HOMA-IR,QUICKI
Psychologic
–
Halperinetal(2011)50
Moderate
17high,9
moderate,16
low
Anthropometric
–Pre-vs
post-OCP
Metabolic
HDL(SMD0.46,95%CI0.14to
0.78)
TG(SMD0.55,95%CI0.17to
0.93)
Reproductive
–
Metabolic
Insulin,glucose,cholesterol,TG,HDL,
LDL,hyperinsulinemiceuglycaemic
clamp(m-value),glucose/insulinratio,
HOMA-IR
Psychologic
–
Mendozaetal
(2014)
58Low
Unclear
Anthropometric
BMI,weight
OCP±
metformin/
anti-
androgen
(no
clea
r co
mpa
ra-
tor)
Reproductive
Relievedhyperandrogenismafter
6 m
o
Reproductive
Hirsutism,acne,seborrhoea,testoster-
one,DHEAS,SHBG,FAI,
androstenedione
Metabolic
Combinationwithmetformin
moreeffectiveinreducingIR
Metabolic
BP,cholesterol,TG,HDL,LDL,glucose,
insulin,HOMA-IR
Psychologic
–
(Con
tinue
s)

548 | TAY eT Al.
onemoderateandonehighquality.Resultswerederived from17trials and 780 participantswith PCOS. Statinswere evaluated ei-therasastandalone therapycomparedtoplaceboorascombina-tiontherapywithmetformincomparedtometformin.All3reviewsreported improvements inmetabolic outcomes (n=3 for the lipidprofile36,42,44 and n=1 for insulin),42 and 2 reviews reported im-provementinendocrineoutcomes(testosterone).42,44Theeffectsofstatinsonanthropometricoutcomeswerenotsignificant(n=2).36,44 Psychologicaloutcomeswerenotassessedbyanyofthereviews.
3.4.9 | Other therapy: vitamin D
Seven reviews evaluated vitamin D32,33,37,40,51,54,57 (Appendix S3,foundintheSupportingInformation)eitherasmonotherapyvspla-ceboormetformin,ascombinationtherapywithmetforminvsmet-forminorcomparingtheeffectsofbeforeandaftervitaminD.Onlyonereviewhadahighratingwhilethemajorityofthereviews(n=5)wereofmoderatequality,andonereviewwasoflowquality.Atotalof75trialsand5701participantswomenwithPCOSwereinvolved.
Five reviewsassessedendocrineoutcomeswith2 reviewsre-portingbenefitsDHEAS(n=1comparingvitaminDvsplaceboandvitaminDwithmetformin vsmetformin)57 or testosterone (n=1comparingvitaminDvsplacebo).40Metabolicoutcomeswereas-sessedby6reviewswith4reviewsreportedbenefitsasreductionsinHOMA-IR(n=1comparingvitaminDvsplaceboorcombinationtherapyvsmetformin),57totalcholesterol(n=1comparingvitaminDvsplacebo)57or triglycerides (n=2comparingbeforeandaftervitaminD).37,51One review reported significant improvements inblood pressure for vitamin D vs placebo.54 Anthropometric out-comeswereassessedbyonereviewwhichdidnotshowanysignif-icantresults.54Psychologicaloutcomeswerenotassessedbyanyofthereviews.
3.4.10 | Other therapy: N- acetyl- cysteine
Two reviews52,54 evaluated the efficacy of N-acetyl-cysteine ofwhichone reviewwasof highquality andone reviewwasof lowquality(AppendixS3,foundintheSupportingInformation).Atotalof19trialswith1744participantswithPCOSwereinvolved.Bothreviewsassessedanthropometric,endocrineandmetaboliceffectsof N-acetyl-cysteine in comparison with placebo or metformin.One review reported improvements in anthropometric anthropol-ogy (reducedBMI,weight andwaist-hip ratio) andmetabolic out-comes (improved lipidprofile, reduced fastingglucose, insulinandHOMA-IR).54Psychologicaloutcomeswerenotassessedbyanyofthereviews.
3.4.11 | Other therapy: antidepressants
One high-quality review39 aimed to investigate the efficacy ofantidepressants in PCOS (Appendix S3, found in the SupportingInformation)andidentifiedonestudyinvolving16womenwithPCOScomparingfluoxetine(antidepressant)andsibutramine(anti-obesityRe
view
sA
MST
AR
Qua
lity
of
incl
uded
stu
dies
Out
com
es a
sses
sed
Com
paris
onSi
gnifi
cant
resu
lts
Anti-androgens
Domecqetal(2013)49
Moderate
RCTs:lowto
moderaterisk
ofbias;
observational
studies:high
riskofbias
Anthropometric
–Anti-
androgen
(no
com
para-
tor)
NA
Reproductive
–
Metabolic
Fastingglucose,postprandialglucose,
glucosetolerancetest,random
glucose,areaunderthecurveof
glucose,glucose/insulinratio,
HOMA-IR,QUICKI
Psychologic
–
NA,notavailable;WMD,weightedmeandifference;SMD,standardizedmeandifference;CI,confidenceinterval;BMI,bodymassindex;SHBG,sexhormonebindingglobulin;FAI,freeandrogenindex;
DHEAS,dehydroepiandrosteronesulphate;BP,bloodpressure;HDL,high-densitylipoprotein;LDL,low-densitylipoprotein;TG,triglycerides;IR,insulinresistance;HOMA-IR,homoeostaticmodelassess-
mentofinsulinresistance;QUIKI,quantitativeinsulinsensitivitycheckindex;OCP,oralcontraceptivepill.
a Resultslessbeneficialthancomparator.
TABLE 3 (Continued)

| 549TAY eT Al.
TABLE 4 Resultsofsystematicreviewsregardingweightlosstherapies
Revi
ews
AM
STA
RQ
ualit
y of
in
clud
ed s
tudi
esO
utco
mes
ass
esse
dCo
mpa
rison
Sign
ifica
nt re
sults
Bariatricsurgery
Butterworthetal
(2016)
47Low
Unclear
Anthropometric
Percentageofexcess
weightloss
Pre-vspostbariatric
surgery
Anthropometric
1trial:improvedpercentageof
excessweightloss
Reproductive
Hirsutism
Reproductive
2trials:improvedhirsutism
Metabolic
T2DM,bloodpressure,
cholesterol,TG,HDL,
LDL,glucose
Metabolic
3trials:improvedglycaemicprofile
(resolutionofT2DM,improvement
ofglycaemiccontrol,ornormaliza-
tionofglucoselevels)
2trials:improvedbloodpressure
Psychologic
Depression
Psychologic
1trial:improveddyslipidaemia
1trial:improveddepression
Skublenyetal(2016)55
Low
Unclear
Anthropometric
BMI,weight,percentage
ofexcessweightloss
Pre-vspostbariatric
surgery
Anthropometric
Percentageofexcessweightloss
(weightedmean57.2%,range33%
to75%)
MeanBM
Iimprovedfrom46.3to
34.2
Reproductive
Hirsutism
Reproductive
Hirsutism(OR0.12,95%CI0.04to
0.36)
Metabolic
–
Psychologic
–
Orlistat
Graffetal(2016)56
Moderate
Unclear
Anthropometric
BMI,weight,waist
circumference
Insulin,HOMA-IR,
cholesterol,TG,HDL,
LDL
Anthropometric
8trials:reducedBMIand/orweight
5trials:reducedwaist-hipratioor
waistcircumference
Reproductive
Testosterone
Reproductive
7trials:reducedtestosterone
Metabolic
Insulin,HOMA-IR,
cholesterol,TG,HDL,
LDL
Metabolic
4trials:improvedlipidprofile(TG,
HDL,LDL)
5trials:reducedHOMA-IRand/or
insulin
Psychologic
–
OR,oddsratio;CI,confidenceinterval;T2DM,type2diabetesmellitus;BMI,bodymassindex;HDL,high-densitylipoprotein;LDL,low-densitylipoprotein;TG,triglycerides;HOMA-IR,homoeostaticmodel
assessment(ofinsulinresistance).

550 | TAY eT Al.
drug).Nosignificantdifferenceswerereportedbetweentreatmentsforanthropometric,endocrineormetabolicoutcomes.Nostudyas-sessingpsychologicaloutcomeswasfound.
3.4.12 | Other therapy: acarbose
Acarbosewas compared against placebo in onemoderate qualityreviewincluding6trialsand263womenwithPCOS(AppendixS3,found in the Supporting Information).38 Acarbose was associatedwith improvement in endocrine (testosterone) and metabolic (tri-glyceride andHDL) outcomes.No significant change in anthropo-metric outcomeswas detected. Psychological outcomeswere notassessedbythereview.
3.4.13 | Other therapy: antioxidants
One low-quality systematic review assessed the efficacy of anti-oxidants54 (AppendixS3, found in theSupporting Information) in-volving 11 trials and 834 Iranianwomenwith PCOS. This reviewreportedonetrialforsoyvsplacebowhichimprovedendocrineout-comes(DHEASandtestosterone);onetrialforfolicacidvsplacebowithout any significant outcome; 3 trials for omega-3 vs placebowhichimprovedmetabolicoutcomes(increasedHDL,reducedtotalcholesterol, total cholesterol/HDL ratio, LDL/HDL ratio, triglycer-ides,LDL,glucose, insulinand insulin resistance);andone trial forzincvsplacebowhichimprovedendocrine(testosterone)andmeta-bolic outcomes (HOMA-IR, cholesterol, triglycerides and LDL).54 Nosignificantimprovementsinanthropometricoutcomeswerere-ported.54Psychologicaloutcomeswerenotassessedbythereview.
4 | DISCUSSION
This is thefirstoverviewofsystematic reviewsassessingpharma-cologicalorsurgicalinterventionsfornonreproductiveoutcomesinwomenwithPCOS,anditdemonstratesalackofhigh-qualitysys-tematicreviewsormeta-analysespresentingdatafromhigh-qualitystudies.
There isdiversity in thequalityof identified reviews in regardtotheuseofmetformin.MostdemonstratedareductioninBMIorwaist-hipratio,andsomereportedbenefitsinmetabolicoutcomesincludingbloodpressure,triglycerides,markersofglucosetoleranceandinsulinresistanceincomparisonwithplaceboorCOCP.Efficacyin hyperandrogenism is less convincing.Our findings support cur-rentevidence-basedguidelinesandspecialitysocietypositionstate-ments where metformin is recommended for women with PCOSwhofailedtoachievetargetweightlosswithlifestylemanagementorthosewithimpairedglucosetoleranceortype2diabetesmellitus,anditisalsonotrecommendedasatreatmentforhirsutismoracneduetoalackofefficacy.2,3,5,7,21,22,60
We report that thiazolidinediones were more effective thanmetforminorplaceboinreducingmarkersofinsulinresistance.30,31 Onlyoneof5reviewsshowedsuperiorityforthiazolidinedionesin
reducing testosterone.34 However, these benefits come with theprice of increased weight which is contradictory for PCOS giventhe high prevalence of obesity and the negative impact onmeta-bolic, endocrine and reproductive outcomes. Thiazolidinedionesmayalsoincreaserisksofbladdercancerandosteoporosis.2,5,7,61,62 Consideringtheserisks,thiazolidinedionesarenotrecommendedasroutinetreatmentforwomenwithPCOS.2,3,5,7,21,22
WereportherethattheCOCPwastheonlytreatmentmodalitythatimprovedclinicalhyperandrogenism.TheuseofCOCPwasnotassociatedwithworseninginsulinresistanceinthisreview.46,49,50,58 TheeffectsonlipidprofileweremorecontroversialasthepositiveeffectofincreaseinHDLmaybeoffsetbyanunfavourableincreaseintriglyceride.50Notably,thereviewbyDomecqetal49didnotre-portanythromboembolicorcardiovasculareventswithCOCPuse.There is consensus in recommendingCOCPs as first-line pharma-cological therapy foracne,hirsutismandoligo-/amenorrhoeawithcareful consideration of the potential risk of increased venousthromboembolism extrapolated from evidence from the generalpopulation.2,3,5,21Althoughpreviousstudieshaveraisedconcernsofworseninginsulinresistanceandtriglycerides,thereisnoavailableevidenceofincreasedcardiovasculareventswithlong-termusewithCOCP.2,7,63-65There is inadequateevidence tocompareor recom-mendspecificCOCPpreparationsorhormonalcomponents.
Whileanti-androgenshavebeenusedwidelytotreathirsutism,especially inpatientswherehirsutism isnot resolvedbyCOCPorwhereCOCPiscontraindicatedorpoorlytolerated,ourstudyfailedtofindanyevidence.2,3,21,60Theonlyreviewweretrievedfocusedon reporting the adverse events where flutamide was associatedwith hepatotoxicity in 2 case series.49One reason for the lack offindingsinourstudyislikelyrelatedtoourrestrictionpublicationsafter2009.Two reviewsbySwigloetal andBrownetal involving12and9RCTs,respectively,concludedthatanti-androgensareaneffectivetreatmentofhirsutismbuttheevidenceisweak.66,67BothreviewsincludedRCTsofsmallsamplesizes(14to82participants)andhighlightedtheneedofmorewell-designedRCTsinvestigatingtheuseofanti-androgensinwomenwithPCOS.
WeightlosstreatmentsinPCOSwereexploredby3reviewsinourstudy.Tworeviewsinvestigatingbariatricsurgerywereoflowqual-itywhich impactsontherobustnessoftheirresults.47,55WereportthatinwomenwithPCOS,bariatricsurgery-inducedweightloss,im-provedhirsutism,bloodpressure,glycaemicandlipidprofile.Orlistatimprovedanthropometric,endocrineandmetabolicoutcomeswhencomparedtoplacebobutnotmetformin.56However,weacknowledgethat there isencouragingevidence inthegeneralpopulationshow-ing that bariatric surgery improves weight loss andmetabolic out-comessuchasglycaemiccontrol,lipidprofileandbloodpressure.68-70 Bariatricsurgerywasrecommendedasasecond-linetherapytoim-provefertilityoutcomesinwomenwithPCOSbytheevidence-basedAustralianguidelineandtobeconsideredinmorbidlyobesewomenwithPCOSbytheEuropeanSocietyofEndocrinology.2,4Otherso-cieties concluded that better quality trialswith long-term data arerequiredbeforeincorporatingbariatricsurgeryintotheirrecommen-dationsforwomenwithPCOS.5,20Wefoundthatstatins,afamilyof

| 551TAY eT Al.
cholesterol-loweringdrugs,areeffective in improvingthe lipidpro-file.36,42,44Giventhelackofdefinitebenefitsintreatmentofhyper-androgenaemiaoranovulation,paucityofdatainreproductive-agedwomenandconsideringthedisadvantageoftype2diabetesdevel-opment, statinsare reserved forwomenwithPCOSwhomeet thestandardindicationsforlipid-loweringtherapy.5,7,22,71
Ourreviewincludedseveralnonconventionalinterventionsthatarenot recommendedbyanyguidelinesor specialty societyposi-tion statements. Although the evidence is not robust, there maybesomebenefitswiththeuseofvitaminDandinositol.WefoundseveralmoderatequalityreviewsassessingvitaminDdemonstratedreductionsintriglycerideandtestosteronelevels.Onehigh-qualityreviewbyPergialiotisetalreportedbeneficialeffectsofvitaminDinreducingDHEAS, insulinresistanceandcholesterol.57 Inositol isa nutritional supplementwith proposed insulin-sensitizing charac-teristics.5,43,48Asreportedhereinlowtomoderatequalityreviews,they may have advantageous effects in nonreproductive-relatedendocrine andmetabolic outcomes including improving biochemi-calhyperandrogenismandinsulinresistance.Noconclusioncanbemade regarding the use of acarbose, N-acetyl-cysteine, soy, folicacid,omega-3orzincinwomenwithPCOSasthenumberofstudiesinvolvedislimited.
Ourstudyhasseveralstrengths.Beinganoverviewofsystem-atic reviews,we collated evidence of interventions for PCOS in anonbiased and systematic manner.We reported our findings fol-lowingthePRISMAguidelinesutilizingrigorousmethodologywithduplication in all study tasks.However,we note study limitationsincludingthediverseAMSTARqualityoftheincludedreviewsandthe lackof clear interpretationof thequalityof individual studieswithintheincludedsystematicreviews.However,performingaddi-tionalqualityassessmentofmorethan350includedstudieswouldbeunfeasible.Wealsoexcludedpublicationsbeforeyear2009asanattempttofilteroutreviewsthatdidnotfollowthePRISMAguide-lines.AssomeinterventionsforPCOShavebeenusedfordecades,wemayhaveexcludedsignificantearlierstudies,albeitpotentiallyoflowerquality.Inourstudy,wefoundthatonlyanti-androgenswereaffectedbythislimitation.66,67
Lastly, quality of future systematic reviews may be strength-enedbyaddressingreportingconflictofinterestofincludedstudies,registering for an apriori protocol andprovides a list of excludedstudies.Wealsoidentifiedsignificantgapsinknowledgeregardingthelackofdataonpsychologicaloutcomesintreatmentofwomenwith PCOS.We retrieved included psychological outcomes as anoutcomeofinterestonlyin2reviews39,47despitethewidelyknownincreasedprevalenceofdepression,anxietyandlowerqualityoflifeinwomenwithPCOSwhichfuturestudiesshouldaddress.72
5 | CONCLUSIONS
This overview of systematic reviews consolidates the evidence oftreatmentoptionsfornonreproductiverelatedoutcomesinwomenwith PCOS.We call attention to the lack of studies investigating
psychological outcomes in any intervention in womenwith PCOSwarrantingfurtherexamination.Overall,wenoteevidenceformet-forminandCOCPuseinnonreproductiveoutcomesinPCOS,cautionagainstthiazolidinedionesandhighlightthatfurtherresearchiswar-rantedinanumberofinterventionssuchasstatins,bariatricsurgery,vitaminDorinositoltoclarifyoutstandingclinicalgaps.
ACKNOWLEDG MENT
ChauTTayissupportedbyaCREinPCOSentrylevelscholarship,HelenaJTeedeissupportedbyanNHMRCPractitionerFellowship,AnjuEJohamissupportedbyaNHMRCEarlyCareerFellowshipandLisa JMoran is supportedbyaNationalHeartFoundationFutureLeaderFellowship.
CONFLIC T OF INTERE S T
Nothingtodeclare.
ORCID
Chau T. Tay http://orcid.org/0000-0001-6228-2654
Helena J. Teede http://orcid.org/0000-0001-7609-577X
Anju E. Joham http://orcid.org/0000-0002-6307-2568
Lisa J. Moran http://orcid.org/0000-0001-5772-6484
R E FE R E N C E S
1. BozdagG,MumusogluS,ZenginD,KarabulutE,YildizBO.Theprev-alenceandphenotypicfeaturesofpolycysticovarysyndrome:asys-tematicreviewandmeta-analysis.Hum Reprod.2016;31:2841-2855.
2. ConwayG,DewaillyD,Diamanti-KandarakisE,etal.Thepolycysticovarysyndrome:apositionstatementfromtheEuropeanSocietyofEndocrinology.Eur J Endocrinol.2014;171:P1-P29.
3. Fauser BC, Tarlatzis BC, Rebar RW, et al. Consensus on wom-en’s health aspects of polycystic ovary syndrome (PCOS): theAmsterdam ESHRE/ASRM-Sponsored 3rd PCOS ConsensusWorkshopGroup.Fertil Steril.2012;97:28-38.e25.
4. TeedeH,MichelmoreJ,McCallisterV,NormanRJ.Evidence-basedguidelinefortheassessmentandmanagementofpolycysticovarysyndrome.PCOSAustralianAlliance2011.
5. LegroRS,ArslanianSA,EhrmannDA,etal.Diagnosisandtreatmentofpolycysticovarysyndrome:anEndocrineSocietyclinicalprac-ticeguideline.J Clin Endocrinol Metab.2013;98:4565-4592.
6. ShorakaeS,BoyleJ,TeedeH.Polycysticovarysyndrome:acom-monhormonalconditionwithmajormetabolicsequelaethatphysi-ciansshouldknowabout.Intern Med J.2014;44:720-726.
7. GoodmanNF,CobinRH,FutterweitW,etal.AmericanAssociationof Clinical Endocrinologists, American College of Endocrinology,and Androgen Excess and Pcos Society Disease State ClinicalReview: Guide to the Best Practices in the Evaluation andTreatment of PolycysticOvary Syndrome – Part 2.Endocr Pract. 2015;21:1415-1426.
8. TeedeH,DeeksA,MoranL.Polycysticovarysyndrome:acomplexcondition with psychological, reproductive and metabolic man-ifestations that impacts on health across the lifespan.BMC Med. 2010;8:41.

552 | TAY eT Al.
9. MoranLJ,MissoML,WildRA,NormanRJ.Impairedglucosetoler-ance,type2diabetesandmetabolicsyndromeinpolycysticovarysyndrome: a systematic review and meta-analysis. Hum Reprod Update.2010;16:347-363.
10. SetjiTL,HollandND,SandersLL,PereiraKC,DiehlAM,BrownAJ.Nonalcoholic steatohepatitis and nonalcoholic fatty liver diseaseinyoungwomenwithpolycysticovarysyndrome.J Clin Endocrinol Metab.2006;91:1741-1747.
11. Lim SS, Davies MJ, Norman RJ, Moran LJ. Overweight, obesityand central obesity in women with polycystic ovary syndrome:a systematic review and meta-analysis. Hum Reprod Update. 2012;18:618-637.
12. deGroot PC,DekkersOM, Romijn JA,Dieben SW,HelmerhorstFM.PCOS,coronaryheartdisease,strokeandtheinfluenceofobe-sity: a systematic review andmeta-analysis.Hum Reprod Update. 2011;17:495-500.
13. DokrasA,Clifton S, FutterweitW,WildR. Increased prevalenceof anxiety symptoms inwomenwith polycystic ovary syndrome:systematicreviewandmeta-analysis.Fertil Steril.2012;97:225-230.e2.
14. BarryJA,KuczmierczykAR,HardimanPJ.Anxietyanddepressioninpolycysticovarysyndrome:asystematicreviewandmeta-analysis.Hum Reprod.2011;26:2442-2451.
15. BazarganipourF,Taghavi SA,MontazeriA,AhmadiF,ChamanR,KhosraviA.Theimpactofpolycysticovarysyndromeonthehealth-relatedqualityoflife:asystematicreviewandmeta-analysis.Iran J Reprod Med.2015;13:61-70.
16. Boomsma CM, Eijkemans MJ, Hughes EG, Visser GH, FauserBC, Macklon NS. A meta-analysis of pregnancy outcomes inwomen with polycystic ovary syndrome. Hum Reprod Update. 2006;12:673-683.
17. HaoulaZ,SalmanM,AtiomoW.Evaluatingtheassociationbetweenendometrial cancer and polycystic ovary syndrome.Hum Reprod. 2012;27:1327-1331.
18. Azziz R, Marin C, Hoq L, Badamgarav E, Song P. Health care-relatedeconomicburdenofthepolycysticovarysyndromeduringthe reproductive life span. J Clin Endocrinol Metab. 2005;90: 4650-4658.
19. LimSS,NormanRJ,DaviesMJ,MoranLJ.Theeffectofobesityonpolycysticovarysyndrome:asystematicreviewandmeta-analysis.Obes Rev.2013;14:95-109.
20. MoranLJ,PasqualiR,TeedeHJ,HoegerKM,NormanRJ.Treatmentof obesity in polycystic ovary syndrome: a position statementoftheAndrogenExcessandPolycysticOvarySyndromeSociety.Fertil Steril.2009;92:1966-1982.
21. Escobar-MorrealeHF,CarminaE,DewaillyD,etal.Epidemiology,diagnosisandmanagementofhirsutism:aconsensusstatementbytheAndrogenExcessandPolycysticOvarySyndromeSociety.Hum Reprod Update.2012;18:146-170.
22. Wild RA, Carmina E, Diamanti-Kandarakis E, et al. Assessmentofcardiovascularriskandpreventionofcardiovasculardiseaseinwomenwith the polycystic ovary syndrome: a consensus state-ment by the Androgen Excess and Polycystic Ovary Syndrome(AE-PCOS)Society.J Clin Endocrinol Metab.2010;95:2038-2049.
23. Escobar-Morreale HF, Botella-Carretero JI, Alvarez-Blasco F,Sancho J. San Millan JL. The polycystic ovary syndrome as-sociatedwithmorbid obesitymay resolve afterweight loss in-duced by bariatric surgery. J Clin Endocrinol Metab. 2005;90: 6364-6369.
24. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group.Preferred reporting items for systematic reviews and meta-analyses:thePRISMAstatement.BMJ. 2009;339:b2535.
25. SheaBJ,BouterLM,PetersonJ,etal.Externalvalidationofamea-surementtooltoassesssystematicreviews(AMSTAR).PLoS ONE. 2007;2:e1350.
26. SheaBJ,GrimshawJM,WellsGA,etal.DevelopmentofAMSTAR:ameasurementtooltoassessthemethodologicalqualityofsystem-aticreviews.BMC Med Res Methodol. 2007;7:10.
27. TangT,LordJM,NormanRJ,YasminE,BalenAH.Insulin-sensitisingdrugs (metformin, rosiglitazone,pioglitazone,D-chiro-inositol) forwomenwith polycystic ovary syndrome, oligo amenorrhoea andsubfertility.Cochrane Database Syst Rev.2009:CD003053.
28. TangT,LordJM,NormanRJ,YasminE,BalenAH.Insulin-sensitisingdrugs (metformin, rosiglitazone,pioglitazone,D-chiro-inositol) forwomenwith polycystic ovary syndrome, oligo amenorrhoea andsubfertility.Cochrane Database Syst Rev.2010:CD003053.
29. Du Q, Wang YJ. Comparative efficacy of thiazolidinedionesand metformin for polycystic ovary syndrome. Saudi Med J. 2012;33:954-961.
30. DuQ,WangYJ,YangS,WuB,HanP,ZhaoYY.Asystematic re-viewandmeta-analysisofrandomizedcontrolledtrialscomparingpioglitazoneversusmetformininthetreatmentofpolycysticovarysyndrome.Curr Med Res Opin.2012;28:723-730.
31. DuQ,YangS,WangY-J,WuB,ZhaoY-Y,FanB.Effectsofthiazoli-dinedionesonpolycysticovarysyndrome:ameta-analysisofran-domizedplacebo-controlledtrials.Adv Ther.2012;29:763-774.
32. FangF,NiK,CaiY,ShangJ,ZhangX,XiongC.EffectofvitaminDsupplementationonpolycysticovarysyndrome:asystematicre-viewandmeta-analysisofrandomizedcontrolledtrials.Complement Ther Clin Pract.2017;26:53-60.
33. JiaX-Z,WangY-M,ZhangN,etal.EffectofvitaminDonclinicalandbiochemicalparametersinpolycysticovarysyndromewomen:ameta-analysis.J Obstet Gynaecol Res.2015;41:1791-1802.
34. Li XJ, Yu YX, Liu CQ, et al. Metformin vs thiazolidinediones fortreatment of clinical, hormonal and metabolic characteristics ofpolycystic ovary syndrome: ameta-analysis.Clin Endocrinol (Oxf). 2011;74:332-339.
35. MengY,ChenX,PengZ,LiuX,SunY,DaiS.Associationbetweenhighserumhomocysteinelevelsandbiochemicalcharacteristicsinwomenwithpolycysticovariansyndrome:asystematicreviewandmeta-analysis.PLoS ONE. 2016;11:e0157389.
36. Sun J, YuanY, Cai R, et al. An investigation into the therapeuticeffects of statinswithmetformin on polycystic ovary syndrome:a meta-analysis of randomised controlled trials. BMJ Open. 2015;5:e007280.
37. XueY,XuP,XueK,etal.EffectofvitaminDonbiochemicalparam-eters inpolycysticovarysyndromewomen:ameta-analysis.Arch Gynecol Obstet.2017;295:487-496.
38. Zhang YY, Hou LQ, Zhao TY. Effects of acarbose on polycysticovary syndrome: a meta-analysis. Exp Clin Endocrinol Diabetes. 2014;122:373-378.
39. ZhuangJ,WangX,XuL,WuT,KangD.Antidepressantsforpolycys-ticovarysyndrome.Cochrane Database Syst Rev.2013:CD008575.
40. Azadi-Yazdi M, Nadjarzadeh A, Khosravi-Boroujeni H, Salehi-Abargouei A. The effect of vitamin D supplementation on theandrogenic profile in patientswith polycystic ovary syndrome: asystematicreviewandmeta-analysisofclinicaltrials.Horm Metab Res.2017;49:174-179.
41. Bordewijk EM, Nahuis M, Costello MF, et al. Metformin duringovulation induction with gonadotrophins followed by timed in-tercourse or intrauterine insemination for subfertility associatedwith polycystic ovary syndrome. Cochrane Database Syst Rev. 2017;1:CD009090.
42. Gao L, Zhao FL, Li SC. Statin is a reasonable treatment optionfor patients with Polycystic Ovary Syndrome: a meta-analysisof randomized controlled trials. Exp Clin Endocrinol Diabetes. 2012;120:367-375.
43. PundirJ,PsaroudakisD,SavnurP,etal.Inositoltreatmentofanovu-lationinwomenwithpolycysticovarysyndrome:ameta-analysisofrandomisedtrials.BJOG.2018;125(3):299-308

| 553TAY eT Al.
44. RavalAD,Hunter T, StuckeyB,Hart RJ. Statins forwomenwithpolycysticovarysyndromenotactivelytryingtoconceive.Cochrane Database Syst Rev.2011:CD008565.
45. TangT,LordJM,NormanRJ,YasminE,BalenAH.Insulin-sensitisingdrugs (metformin, rosiglitazone,pioglitazone,D-chiro-inositol) forwomen with polycystic ovary syndrome, oligo amenorrhoea andsubfertility.Cochrane Database Syst Rev.2012:CD003053.
46. Al Khalifah RA, Florez ID, Dennis B, Thabane L, Bassilious E.Metforminororal contraceptives foradolescentswithpolycysticovariansyndrome:ameta-analysis.Pediatrics. 2016;137:e20154089.
47. ButterworthJ,DeguaraJ,BorgC-M.Bariatricsurgery,polycysticovarysyndrome,andinfertility.J Obes.2016;2016:1-6.
48. Galazis N, Galazi M, Atiomo W. D-Chiro-inositol and its signifi-cance inpolycysticovarysyndrome:asystematicreview.Gynecol Endocrinol.2011;27:256-262.
49. DomecqJP,PrutskyG,MullanRJ,etal.Adverseeffectsofthecom-montreatmentsforpolycysticovarysyndrome:asystematicreviewandmeta-analysis.J Clin Endocrinol Metab.2013;98:4646-4654.
50. Halperin IJ,KumarSS,StroupDF,LaredoSE.Theassociationbe-tweenthecombinedoralcontraceptivepillandinsulinresistance,dysglycemiaanddyslipidemiainwomenwithpolycysticovarysyn-drome: a systematic review and meta-analysis of observationalstudies.Hum Reprod.2011;26:191-201.
51. HeC,LinZ,RobbSW,EzeamamaAE.SerumvitaminDlevelsandpolycysticovarysyndrome:asystematicreviewandmeta-analysis.Nutrients.2015;7:4555-4577.
52. ThakkerD,RavalA,PatelI,WaliaR.N-acetylcysteineforpolycysticovarysyndrome:asystematicreviewandmeta-analysisofrandom-izedcontrolledclinicaltrials.Obstet Gynecol Int. 2015;2015:817849.
53. Patel R, Shah G. Effect of metformin on clinical, metabolic andendocrineoutcomesinwomenwithpolycysticovarysyndrome:ameta-analysis of randomized controlled trials.Curr Med Res Opin. 2017;33:1545-1557.
54. Amini L, Tehranian N, MovahedinM, Ramezani Tehrani F, ZiaeeS.AntioxidantsandmanagementofpolycysticovarysyndromeinIran:asystematicreviewofclinicaltrials.Iran.2015;13:1-8.
55. SkublenyD,SwitzerNJ,GillRS,etal.Theimpactofbariatricsur-geryonpolycysticovarysyndrome:asystematicreviewandmeta-analysis.Obes Surg.2016;26:169-176.
56. GraffSK,MarioFM,ZiegelmannP,SpritzerPM.Effectsoforlistatvs. metformin onweight loss-related clinical variables in womenwithPCOS: systematic review andmeta-analysis. Int J Clin Pract. 2016;70:450-461.
57. Pergialiotis V, Karampetsou N, Panagopoulos P, Trakakis E,PapantoniouN.TheeffectofVitaminDsupplementationonhor-monalandglycaemicprofileofpatientswithPCOS:ameta-analysisofrandomisedtrials.Int J Clin Pract. 2017;71:e12957.
58. Mendoza N, Simoncini T, Genazzani AD. Hormonal contracep-tive choice for women with PCOS: a systematic review of ran-domized trials and observational studies. Gynecol Endocrinol. 2014;30:850-860.
59. Gill S, Gemmell A, Colleran R, ZanuriN,O’BrienH, PoobalanA.Doesmetformincombinedwithclomiphenecitrateimprovefertil-ityrelatedoutcomesinclomipheneresistantwomenwithPCOS:asystematicreview.Middle East Fertil Soc J.2014;19:81-88.
60. GoodmanNF,CobinRH,FutterweitW,etal.AmericanAssociationofClinicalEndocrinologists,AmericanCollegeofEndocrinology,andAndrogen Excess and Pcos SocietyDisease State Clinical Review:Guide to the Best Practices in the Evaluation and Treatment ofPolycysticOvarySyndrome-Part1.Endocr Pract.2015;21:1291-1300.
61. Berberoglu Z, Yazici AC, Demirag NG. Effects of rosiglita-zone on bone mineral density and remodelling parameters inPostmenopausal diabetic women: a 2-year follow-up study. Clin Endocrinol (Oxf).2010;73:305-312.
62. Turner RM, Kwok CS, Chen-Turner C, Maduakor CA, Singh S,Loke YK. Thiazolidinediones and associated risk of bladder can-cer: a systematic review and meta-analysis. Br J Clin Pharmacol. 2014;78:258-273.
63. CostelloMF,ShresthaB,EdenJ,JohnsonNP,SjoblomP.Metforminversus oral contraceptive pill in polycystic ovary syndrome: aCochranereview.Hum Reprod.2007;22:1200-1209.
64. AmiriM,RamezaniTehraniF,NahidiF,KabirA,AziziF,CarminaE.Effectsoforalcontraceptivesonmetabolicprofileinwomenwithpolycystic ovary syndrome: a meta-analysis comparing productscontaining cyproterone acetatewith third generation progestins.Metabolism.2017;73:22-35.
65. KorytkowskiMT,MokanM,HorwitzMJ,BergaSL.Metabolicef-fectsoforalcontraceptives inwomenwithpolycysticovarysyn-drome. J Clin Endocrinol Metab.1995;80:3327-3334.
66. SwigloBA,CosmaM,FlynnDN,etal.Clinical review:antiandro-gensforthetreatmentofhirsutism:asystematicreviewandmeta-analyses of randomized controlled trials. J Clin Endocrinol Metab. 2008;93:1153-1160.
67. BrownJ,FarquharC,LeeO,ToomathR,JepsonRG.Spironolactoneversusplaceboorincombinationwithsteroidsforhirsutismand/oracne. Cochrane Database Syst Rev.2009:CD000194.
68. ColquittJL,PickettK,LovemanE,FramptonGK.Surgeryforweightlossinadults.Cochrane Database Syst Rev.2014:CD003641.
69. QiL,GuoY,LiuCQ,HuangZP,ShengY,ZouDJ.Effectsofbariatricsurgeryonglycemicandlipidmetabolism,surgicalcomplicationandqualityoflifeinadolescentswithobesity:asystematicreviewandmeta-analysis.Surg Obes Relat Dis.2017;13:2037-2055.
70. RicciC,GaetaM,RausaE,AstiE,BanderaF,BonavinaL.Long-termeffectsofbariatric surgeryon type IIdiabetes,hypertensionandhyperlipidemia:ameta-analysisandmeta-regressionstudywith5-yearfollow-up.Obes Surg.2015;25:397-405.
71. PreissD,SeshasaiSR,WelshP,etal.Riskofincidentdiabeteswithintensive-dose compared with moderate-dose statin therapy: ameta-analysis.JAMA.2011;305:2556-2564.
72. ChingHL,BurkeV,StuckeyBG.Qualityof lifeandpsychologicalmorbidity inwomenwith polycystic ovary syndrome: bodymassindex,ageandtheprovisionofpatientinformationaresignificantmodifiers.Clin Endocrinol (Oxf).2007;66:373-379.
SUPPORTING INFORMATION
Additional supporting information may be found online in theSupportingInformationsectionattheendofthearticle.
How to cite this article:TayCT,JohamAE,HiamDS,etal.Pharmacologicalandsurgicaltreatmentofnonreproductiveoutcomesinpolycysticovarysyndrome:Anoverviewofsystematicreviews.Clin Endocrinol (Oxf). 2018;89:535–553. https://doi.org/10.1111/cen.13753
Top Related