







Languages
Pages
Legal


PELVIC FLOOR
DYSFUNCTION
AND SRU
Reza Ansari
Associate professor of Medicine
DDRC
TUMS
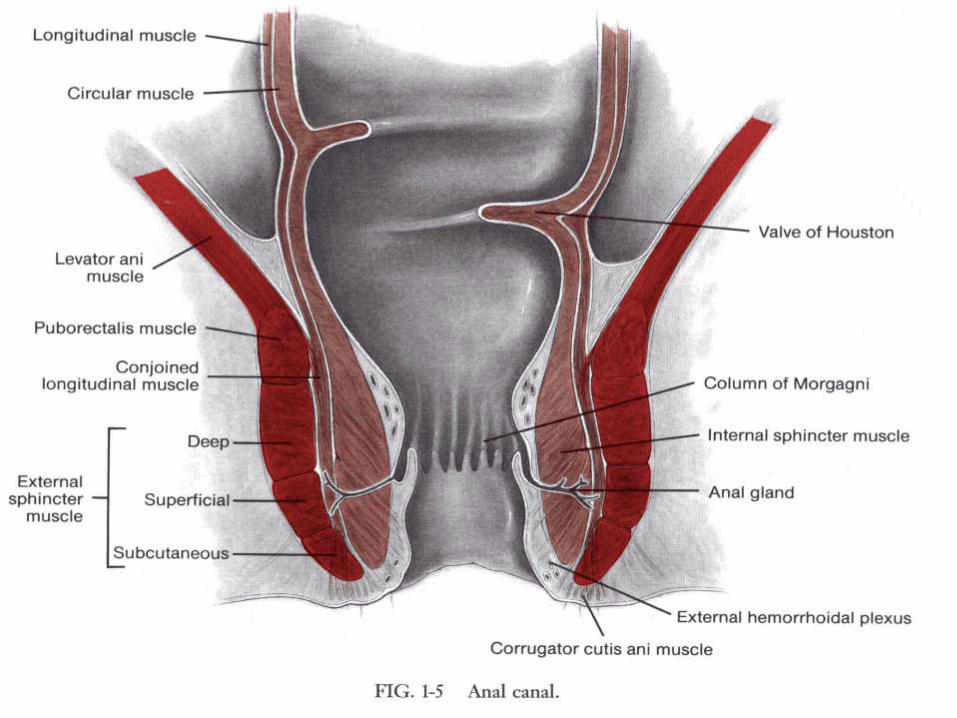
PELVIC FLOOR ANATOMY The pelvic floor has superficial and deep muscle
The superficial layers include the internal anal
sphincter (IAS) and external anal sphincter (EAS),
perineal body, and transverse perinei muscles
The puborectalis maintains anorectal angulation and
creates a mechanical barrier for stool flow and
maintains pelvic floor integrity
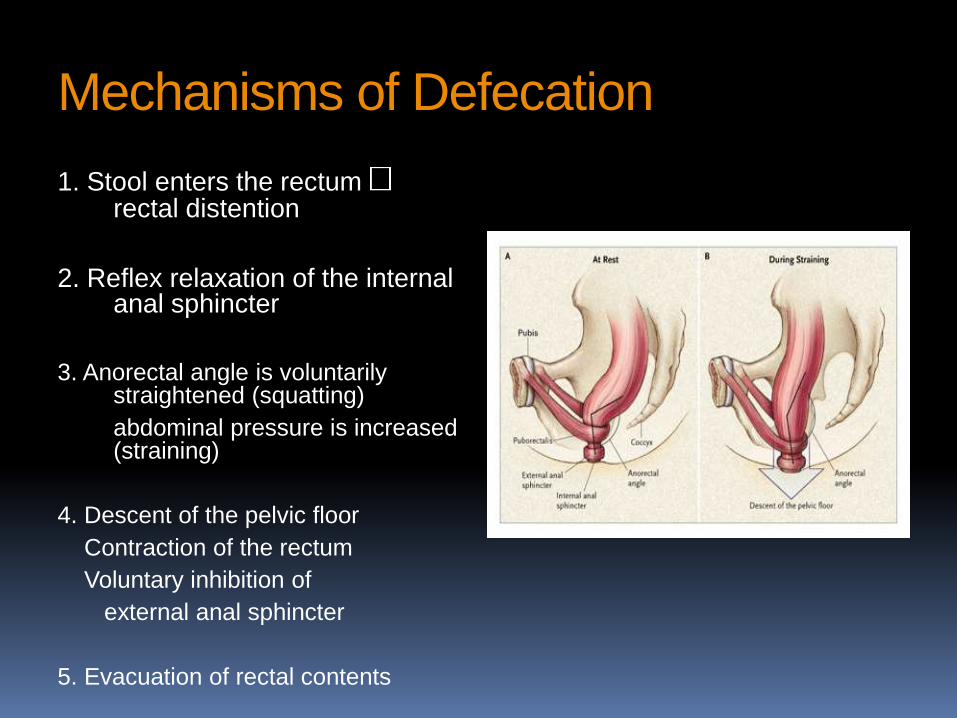
Mechanisms of Defecation
1. Stool enters the rectum rectal distention
2. Reflex relaxation of the internal anal sphincter
3. Anorectal angle is voluntarily straightened (squatting)
abdominal pressure is increased (straining)
4. Descent of the pelvic floor
Contraction of the rectum
Voluntary inhibition of
external anal sphincter
5. Evacuation of rectal contents

Physiology of defecation

Functional Defecation Disorder Symptoms:
Prolonged excessive straining (85%)
Feeling of incomplete evacuation (75%)
May have soft stool
Require digital evacuation (66%)
Do not respond well to standard laxatives

Pelvic floor dyssynergia
It is multifactorial and thought to be an acquired, learned dysfunction rather than an organic disease and 31% begins during childhood, 29% after a specific event (pregnancy,trauma),40% the precipitating event is unknown

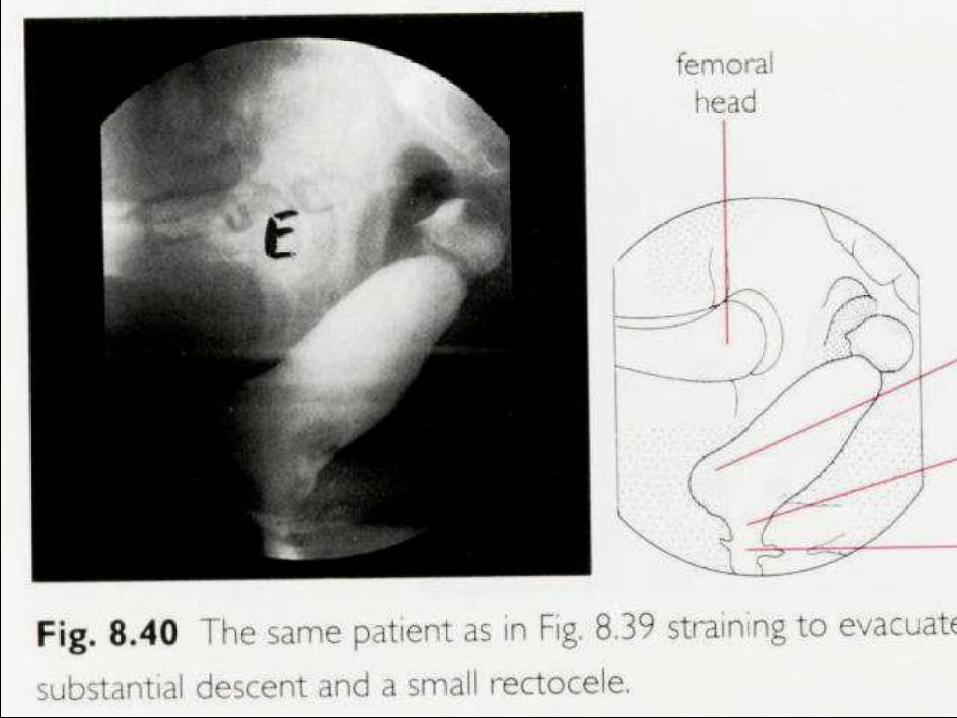
Structure and function Barium defcography MR (magnetic resonance) defecography
Functional only :
- Balloon expulsion - Manometry (HRM) - Colonic transit time - Anal sphincter EMG

DX Balloon expulsion test
This provides information regarding the ability to
expel a 50-ml water-filled balloon placed in the
rectum. Normal expulsion time is 1 min
It has 80– 90% specificity and 97 % negative
predictive value for identifying dyssynergia
Sensitivity 50 %

Colonic transit study Slow transit constipation can coexist in two-thirds of
patients with DD, and it is imperative to differentiate
between patients with isolated DD or mixed with
slow transit constipation.

Anorectal manometry Type I : adequate push effort with paradoxical anal
contraction
type II : impaired push effort with paradoxical anal
contraction,
type III : impaired anal relaxation with adequate
push
Effort
type IV : impaired push effort with impaired anal
relaxation.

Defecation normally involves the coordinated relaxation of the puborectalis and external anal sphincter muscles as pressure is building in the rectum (control panel, left). However, in patients with dyssynergic defecation (patient panel, right), ineffective defecation is associated with a failure to relax, or inappropriate contraction of, the puborectalis and external anal sphincter muscles as pressure increases in the rectu

MR (magnetic resonance) defecography
It is not widely available and can be performed with a
closed or open system:
Open magnetic resonance imaging (MRI) acquires
images in a sitting position, simulating true
defecation
Closed-configuration MRI system, images are
acquired in the supine position




SRU The annual incidence is 1– 3.6/ 100,000
80% of patients are < 50 years of age ,with slightly
higher prevalence in females
Rectal intussusception is often present and
evacuation is delayed
SRU Patients present with rectal bleeding and / or pain,
mucus discharge, straining and tenesmus, and a
feeling of incomplete evacuation
A majority of these patients use digital maneuvers
but rarely admit
In some patients, an underlying psychologic
disorder, such as obsessive – compulsive disorder,
may be present


SRU
Approximately 55 %with constipation
20– 40% with diarrhea
25% of the patients, asymptomatic
25 % are treated as IBD
Histology of solitary rectal ulcer Thickened mucosal layer with distortion of the crypt
architecture
The lamina propria is replaced with smooth muscle
and collagen (fibromuscular obliteration)
Collagen infiltration of the lamina propria can be
helpful for distinguishing solitary rectal ulcer
syndrome from IBD and chronic ischemic colitis

DX Defecography may show other abnormalities such as
rectal mucosal intussusception in 45– 80% of subjects
Barium enema is unreliable
Anorectal manometry does not help in establishing the diagnosis or predicting therapeutic response
Ultrasonography may show marked thickening of the IAS, submucosa, and EAS, as well as rectal wall and muscularis propria
SRU, DX Sigmoidoscopy may reveal a small, shallow ulcer
with a white slough or hyperemic mucosa on the
anterior wall of the rectum
Th e lesions can be multiple (30 % ), ulcerated
(57 % ), polypoid (25 % ), or with patches of
hyperemic mucosa (18 % )
It is usually found on the anterior or anterolateral
wall of the rectum, over a rectal fold, ~ 5 – 10 cm
from anus






Management
Reminding patients that :
The levatory is not the
Library

Management Behavioral therapy remains the mainstay of
treatment
Reducing excessive straining, spending < 5 min during evacuation, and discontinuing the use of digital maneuvers
These recommendations, together with biofeedback therapy, improved symptoms in 67 % of patients
A high-fiber diet showed a variable response rate of 19 – 70 % , suggesting that although diet helps by itself, it is insufficient.


Management Local treatment with topical steroids and
sulphasalazine is generally ineffective
There are limited data for sucralfate
A recent study suggests that Argon plasma
coagulation may be useful in controlling bleeding
and improving healing of ulcers, but controlled
studies are lacking

Botulinum toxin
An open label trial reported that injections of 60 to
100 units of type A botulinum toxin into both sides of
the puborectalis muscle under ultrasound guidance
was effective in patients with defecatory dysfunction
Repeat injections may be necessary to maintain
benefits
Biofeedback therapy
A prospective study of 11 patients with refractory
SRUS showed that biofeedback therapy improved
straining effort and stool frequency, digital
maneuvers were discontinued in 45 % , and bleeding
ceased in 56 % of patients
Ulcer healing was reported in 10 patients: 4 had
complete healing, 2 had > 50% healing, and 4 had <
50% healing

Surgery Appropriate for patients with full-thickness or mucosal rectal
prolapse, or with symptoms unresponsive to conservative management
Surgical options include local excision, diversion, or rectopexy
Outcomes of surgery are often disappointing, because of either persistent symptoms, postoperative bleeding, or sexual dysfunction
New methode laparoscopic mesh rectopexy a minimally invasive option for selected patients

Classification of Constipation:
Slow Transit Constipation (STC): “colonic inertia”; characterized by prolonged delay in the transit of stool through the colon due to neuromuscular dysfunction of the colon
Constipation-predominant irritable bowel syndrome:
subtype of constipation associated with abdominal discomfort
Functional Defecation Disorder (Pelvic Floor
Dysfunction): difficulty or inability to expel stool from the anorectum due to neuromuscular dysfunction of the defecation unit
3.


Colectomy in constipation ? At least five criteria should be met prior to consideration of surgery:
The patient has chronic, severe, and disabling symptoms from constipation that are unresponsive to medical therapy
The patient has slow colonic transit of the inertia pattern
The patient does not have intestinal pseudoobstruction, as demonstrated by radiologic or manometric studies
The patient does not have pelvic floor dysfunction based on anorectal manometry
The patient does not have abdominal pain as a prominent symptom.
Misoprostol A prostaglandin analog which has been used
successfully to treat some patients with severe constipation
Anecdotal experience suggests that misoprostol (200 mcg every other day and increased by 200 mcg every other day and can be increased as tolerated
Act more better when use with PEG
Misoprostol should not be used in women who could become pregnant since it induces labor and can lead to loss of the fetus. It can also increase menstrual bleeding

Linaclotide Agonist of the guanylate cyclase-C receptor that
stimulates intestinal fluid secretion and transit
Linaclotide has been approved by FDA for the
treatment of chronic idiopathic constipation at a dose
of 145 micrograms daily
However, the role of linaclotide in treating chronic
constipation and the long-term risks and benefits
remain to be determined

Lubiprostone A locally acting chloride channel activator
Its approval was based upon two placebo-controlled
trials that included a total of 479 patients (either 24 or
48 mcg daily)
Its long-term safety is not yet established
Reserved for patients with severe constipation in
whom other approaches have been unsuccessful

Prucalopride this 5HT4 prokinetic agent in a dose of 1 to 4 mg
once daily has been shown to be superior to placebo
in 4 to 12-week trials, and safe and well tolerated in
patients age 65 or older
The improvement in quality of life scores seen at the
end of the 12-week trials was maintained for up to 18
months

Colchicine May be effective for the treatment of chronic
constipation
It is effective with 1 mg daily
It should not be used in patients with renal
insufficiency
The drug can induce a myopathy

Top Related