






Languages
Pages
Legal


Pediatric Brain Tumors
S. Ndoro, J. Caird, and D. Crimmins
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Classification of Tumors of the Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Clinical Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Diagnostic Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Immunohistochemistry in Brain Tumor Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Molecular markers in Pediatric Neuro-Oncology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
General Operative Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Posterior Fossa Tumors: Tumors of the Cerebellum and Fourth Ventricle . . . . . . . . 10Medulloblastoma WHO Grade IV . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Ependymal Tumors WHO Grade II-III . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Cerebellar Pilocytic Astrocytomas WHO Grade I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Tumors of the Mid-Brain and Cervico-Medullary Region . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Brain Stem Gliomas (DIPG: Diffuse Intrinsic Pontine Gliomas, Focal, Dorsal,
Exophytic, Cervicomedullary Tumors) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Tumors of the Sellar/Suprasellar Region . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Craniopharyngioma WHO Grade I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Optic Pathway Gliomas (OPGs) WHO Grade I, II . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Pituitary Adenomas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Tumors of the Pineal Region . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Pineoblastoma (PB) WHO Grade IV . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Germ Cell Tumors (Germinoma, Embryonal Carcinoma, Yolk Sac Tumor,
Choriocarcinoma, and Teratomas) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Tumors of the Choroid Plexus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Choroid Plexus Papilloma and Choroid Plexus Carcinoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
S. Ndoro · J. Caird · D. Crimmins (*)Temple St. Children’s University Hospital, Dublin, Irelande-mail: [email protected]; [email protected]
© Springer-Verlag GmbH Germany, part of Springer Nature 2020P. Puri (ed.), Pediatric Surgery,https://doi.org/10.1007/978-3-642-38482-0_156-1
1

Neurocutaneous Syndromes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Conclusion and Future Directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
AbstractTumors of the central nervous system are themost common type of solid neoplasm found inchildren and are second only to leukemia inoverall cancer frequency. Incidence is 2–5 in100,000 with primary brain tumors accountingfor 20% of deaths from cancer in children. Sixtypercent of children who survive a brain tumorare left with a life-altering disability. The ratio ofsupratentorial to infratentorial tumors is age-specific. Many tumors remain undetected untilthey are relatively large in size due in part to theelasticity of the infant skull, compensation bythe developing nervous system for deficits, andthe difficulty in many instances of the child’sinability to cooperate in physical examinations.The WHO classification comprises a histologi-cal grading according to a four-tiered schemeranging from WHO grade I (benign) to WHOgrade IV (the most malignant). Immunohisto-chemical markers play an important role in thediagnosis of different tumor entities. The con-tribution of molecular genetics to brain tumordiagnostics is an ever-expanding field that haspotential to significantly impact classification,prognosis, and therapeutic management of mostCNS tumors. Different treatment modalitiessuch as surgery, radiotherapy, and chemother-apy are widely used management entities; how-ever, morbidity and mortality in pediatric braintumors remains high. Novel targeted therapiesand approaches to multidisciplinary treatmentstrategies are required if progress is to beachieved to cure most pediatric brain tumors.
KeywordsPediatric brain tumors · Radiotherapy ·Chemotherapy · WHO classification of CNStumors
Introduction
Tumors of the central nervous system are the mostcommon type of solid neoplasm found in childrenand are second only to leukemia in overall cancerfrequency. In the pediatric population, incidence is2–5 in 100,000. Primary brain tumors account for20% of deaths from cancer in children and 60% ofchildren who survive a brain tumor are left with alife-altering disability. The highest incidence rate ofchildhood brain tumors is in children below the ageof 5 years, who are particularly vulnerable to theeffects of treatment (Limond et al. 2019). Exclud-ing epidemiological differences, the feature thatdistinguishes pediatric brain tumors from adultbrain tumors is the relative incidence by histolog-ical type. The common pediatric brain tumors aregliomas (cerebellum, brain stem, and optic nerve),pineal tumors, craniopharyngiomas, teratomas, andprimitive neuroectodermal tumors (PNETs, pri-marily medulloblastoma). Fortunately, the mostmalignant astrocytic tumor, glioblastoma multi-forme, is less common in children. Anotherdistinguishing feature is the site of origin. Theratio of supratentorial to infratentorial tumors isdependent on the specific age group as illustratedin Table 2. Most supratentorial tumors are astrocy-tomas (13%). Ependymomas, choroid plexustumors, and PNETs also occur. Infratentorialtumors include medulloblastoma (14%) and cere-bellar astrocytomas (15%) and ependymomas(9%). There is however a significant pre-ponderence of posterior fossa (infratentorial)tumours in children. Conversely, posterior fossatumors only account for 10% of brain tumors inthe adult population.
2 S. Ndoro et al.

Classification of Tumors of theNervous System
The World Health Organization (WHO) classifi-cation is the most commonly used method forclassifying brain tumors. It is based on histologicand immunohistochemical differences and thepresumption that these tumors arise from specificcategories of normal cells. The WHO classifica-tion comprises a histological grading according toa four-tiered scheme ranging from WHO grade I(benign) to WHO grade IV (highly malignant).Generally, WHO grade I lesions include tumorswith a minimal proliferative potential and thelikelihood of cure following surgical resectionalone (e.g., pilocytic astrocytomas). WHO gradeII tumors are more infiltrative with low mitoticactivity but with a tendency to recur after treat-ment (e.g., diffuse astrocytomas, oligoden-drogliomas, and ependymomas). WHO grade IIIis reserved for neoplasms with histological evi-dence of anaplasia, in the form of increasedmitotic activity, increased cellularity, nuclearpleomorphism, and cellular anaplasia. WHOgrade IV is assigned to mitotically active andnecrosis prone, highly malignant neoplasms thatare typically associated with rapid pre and post-operative evolution of disease (e.g., glioblastomaand various forms of embryonal tumors) (Figs. 1and 2; Tables 1, and 2).
Clinical Presentation
Many tumors remain undetected until they arerelatively large in size due in part to the elasticityof the infant skull, compensation by the develop-ing nervous system for deficits, and the difficultyin many instances of the child’s inability to coop-erate in physical examinations. As a consequence,this frequently leads to a prolonged symptominterval, with associated cognitive impairmentand significant brain distortion. Common pre-senting complaints of pediatric brain tumors aredependent on location of the tumor, tumor
biology, and age of the child. In general, pre-senting symptoms fall into five categories: raisedintracranial pressure, focal neurological deficits,endocrine abnormalities, seizures or occasionallypediatric brain tumors can be found incidentally.
Raised intracranial pressure will manifest aspersistent/recurrent headaches, persistent/recur-rent vomiting (especially without obvious gastro-intestinal complaints), abnormal balance/walking/coordination, and somnolence. This may be due tothe mass effect itself, although in children it isoften due to the development of hydrocephalus.Headache may occur from direct mass effect anddural stretch in the posterior fossa but also fromobstruction of the cerebrospinal fluid (CSF) path-ways leading to hydrocephalus; this is due topediatric brain tumors commonly being in themidline, therefore hydrocephalus is common.The severity of hydrocephalus will range fromthat causing mild headaches to, severe hydroceph-alus with changes in level of consciousness andoccasionally rapid deterioration leading to comaand death from brain herniation.
Focal symptoms and signs are due to involve-ment or compression of adjacent eloquent braintissue or due to a mass adjacent to or within thebrainstem. Focal neurological deficits are com-monly seen with hemispheric lesions. In veryyoung children, focal motor deficits may be mis-sed due to compensation, as young children will“mask” a deficit by compensating with anotherextremity or unconsciously changing theirbehavior.
Seizures/fits generally arise from benigntumors that involve the cortex. These are usuallyintrinsic tumors such as low grade astrocytomasand neuronal tumours.
Additional signs seen in pediatric brain tumorsinclude blurred/ double vision, abnormal eyemovement, dysarthria, head tilt, and long tractsigns (hyperreflexia and sensory changes). Pedi-atric brain tumors can distort, damage, anddestroy portions of the brain involved in bothafferent and efferent visual pathways (Peragallo2019). Children with a brain tumor therefore have
Pediatric Brain Tumors 3

a high risk of impaired vision. Children in the12–18 age group may present with delayed/arrested puberty. While in the under 5 age group,failure to thrive, irritability, or developmentaldelay may be the only presenting finding ininfants with hypothalamic lesions, the so called‘diencephalic syndrome’. Sellar-region lesionscan also present with visual disturbances andvisual loss. Hypopituitarism is a rare presentingsymptom but does occur following surgical inter-vention for sellar lesions (Table 3).
Diagnostic Studies
Assessment of an infant’s acquisition of develop-mental milestones provides insight into a child’smotor and cognitive function. Initial evaluationshould include a complete physical examination.This is particularly important in infants and tod-dlers where an objective history is not available.Increasing head circumference over a short dura-tion and a bulging anterior fontanelle indicate
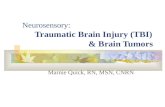
Recognizing sensations,and body positions, recognizing objects,spatial judgments and understanding time
Parietal Lobe
Integrating and processing visual information,(colour, shape, distance)
Occipital Lobe
Controls balance andMuscle coordination
Cerebellum
Regulates breathing,breathing,Body temperature,heart activity, etc
Brain stemUnderstanding language,Processing auditoryinformation,organizing information,
Temporal Lobe
Planning/reasoning, problem solving,recognizing and regulating emotion,social skills
Frontal Lobe
Fig. 1 Areas of the brain (lateral view)
Germ cell tumours/Pineal parenchymaltumours
Medulloblastoma
Cerebellarastrocytoma
InfratentorialEpendymomaBrain stem glioma
Craniopharyngioma
Opticglioma
Astrocytoma/PNET/Ependymoma
Fig. 2 Location of mostcommon pediatric braintumors (medial view)
4 S. Ndoro et al.

raised intracranial pressure. Although difficult tovisualize in many cases, a glimpse of the opticdisk can sometimes exclude significant raised
intracranial pressure when it may be suspectedbased on the child’s symptoms. Skin and extrem-ity examinations for manifestation of syndromic
Table 1 WHO grading of tumors of the central nervous system
Tumor group Tumor entityGradeI
GradeII
GradeIII
GradeIV
Astrocytic tumors Pilocyctic astrocytoma x
Pilomyxoid astrocytoma x
Pleomorphic xanthoastrocytoma x
Diffuse astrocytoma x
Anaplastic astrocytoma x
Glioblastoma x
Oligodendroglial tumors Oligodendroglioma x
Anaplastic oligodendroglioma x
Mixed gliomas Oligoastrocytoma x
Anaplastic oligoastrocytoma x
Ependymal tumors Ependymoma x
Anaplastic ependymoma x
Choroid plexus tumors Choroid plexus papilloma x
Choroid plexus carcinoma x
Neuronal and mixedglioneuronal tumors
Gangliocytoma x
Ganglioglioma x x
Anaplastic ganglioglioma x
Desmoplastic infantile ganglioma x
Dysembryoplastic Neuroepithelialtumor (DNET)
x
Central/extraventricular neurocytoma x
Pineal parenchymal tumors Pineocytoma x
Pineoblastoma x
Papillary tumor of the pineal region x x
Embryonal tumors Medulloblastoma x
Medulloepithelioma x
CNS-PNET x
Atypical teratoid/rhabdoid tumor x
Tumors of peripheral nerves Schwannoma x
Neurofibroma x
Tumors of the meninges Meningioma x
Atypical meningioma x
Clear cell meningioma x
Chordoid meningioma x
Anaplastic meningioma x
Papillary meningioma x
Rhabdoid meningioma x
Tumors of the sellar region Craniopharyngioma x
Pediatric Brain Tumors 5

conditions such as café au lait spots and axillaryfreckling is useful. A neurological examination toassess mental status, cranial nerves I-XII, andmotor function – bulk, tone, strength, sensation,and deep tendon reflexes.
A child presenting with intractable headaches,especially associated with persistent vomiting or aneurological deficit, should receive a screeningimaging study, usually a computed tomography(CT) scan. While CT may not provide the requireddetail, a perfectly normal study will exclude thepresence of hydrocephalus or a significant masslesion. An abnormality on the CT study shouldprompt a more detailed magnetic resonance imag-ing (MRI) scan. It should be noted that vomiting andirritability and/or headaches are exceedingly com-mon in children, and it is impractical for all childrento undergo imaging studies. In general, if there is asuspicion of an intracranial mass or if the childcannot be evaluated properly due to lack of cooper-ation or other circumstances, then a CT should beobtained. A child in whomCNS imaging is requiredto exclude a brain tumor (potential diagnosis butlow index of suspicion) should be imaged within4 weeks. MRI is the imaging modality of choice fora child who may have a brain tumor as it revealshigher definition of anatomy. If MRI is not avail-able, a contrast enhanced CT should be performed.Imaging results should be interpreted by a profes-sional with expertise and training in central nervoussystemMRandCTimaging in children. The need tosedate or anaesthetize a child for imaging should notdelay imaging by more than 1 week. To determinethe extent of a brain tumor or spinal cord dropmetastases before treatment, an MRI study of thebrain and spine, both before and after gadoliniuminfusion, is mandatory. Metastases outside theCNS are very rare in children, and for this reasonroutine imaging of the chest, abdomen, and pelvis isnot indicated (unless there is suspicion based on theclinical setting).
For suspected midline supratentorial tumors,serum and CSF alpha feto-protein (AFP), betahuman chorionic gonadotropin (βhCG), and pla-cental alkaline phosphatase (PLP) values shouldbe obtained to rule out secretory germ cell tumors.Sellar region masses also may produce endocrineand visual dysfunction. In the setting of an irrita-ble child with a suspected infectious process, thequestion of doing a lumbar puncture (LP) toexclude meningitis is sometimes raised. Lumbarpuncture is contraindicated where risk of a braintumor is a differential diagnosis (Table 4).
Immunohistochemistry in Brain TumorClassification
Immunohistochemical staining for the expressionof specific differential markers as well as prolifer-ation – associated antigens has enormously facil-itated the morphologic classification of braintumors. It will continue to play an even moreimportant role in brain tumor diagnostics asnovel cell and /or tumor type specific markersare developed. With the introduction of targetedtherapies directed against certain proteins that areactivated or overexpressed by tumor cells, immu-nohistochemical analyses plays an important rolein demonstrating expression of the target proteinsbefore therapy is initiated (Table 5).
Molecular markers in Pediatric Neuro-Oncology
Pediatric molecular neuro-oncology is a fast, devel-oping field. With ever-expanding knowledge ofpathogenesis of primary brain tumors, numerousgenetic and epigenetic alterations have been identi-fied in different tumor types. Impressive technolog-ical advances have beenmade inmolecular analyses
Table 2 Location ofpediatric brain tumorsby age
Age % infratentorial
0–6 months 27%
6–12 months 53%
12–24 months 74%
2–15 years 42%
6 S. Ndoro et al.

and hopefully soon these advances will be used inconjunction with established morphological braintumor diagnosis. These molecular markers may beused for diagnosis and/or predicating therapyresponse or prognosis in the brain tumors that com-monly occur in children (Tables 6 and 7).
General Operative Considerations
The principles of pediatric brain tumor surgery areto treat symptoms, treat raised intracranial pressureif present, and to avoid deficits. Surgery establishesa histological diagnosis, resection or reductiontumor bulk, and to reestablishes normal CSF path-ways. Cerebral hemispheric tumors are approachedby craniotomy.With the aid of functionalMRI, it ispossible to localize the speech and motor cortex inrelation to the tumor and aid in selecting the safestsite for excision. Tumors of the brain stem may be
debulked if they are dorsally exophytic (lowgrade); however, MRI is sufficient to establish thediagnosis of most intrinsic pontine gliomas.Tumors of the pineal region may be approachedthrough a posterior fossa route, by retracting thecerebellum from the underside of the tentorium, bya supratentorial route between the hemispheres andthrough the posterior corpus callosum or throughthe tentorium itself. Tumors of the cerebellum andlower brainstem are approached by a posteriorsuboccipital craniotomy. Midline tumors of thefourth ventricle usually present with obstructivehydrocephalus, 20–40% of patients ultimatelyrequire a CSF diversion procedure with the optionof placing a ventriculoperitoneal drain orventriculostomy. Postoperative problems includeacute hydrocephalus, pseudomeningoceles, asepticmeningitis, mutism, and cranial nerve or brainstemdysfunction.
Table 3 Symptoms of pediatric brain tumors by age group
Adopted from www.headsmart.org.co.uk
Pediatric Brain Tumors 7

Table 4 Radiological features of pediatric brain tumors
Mass Location Imaging appearance Other features
Choroid plexustumors
Intraventricular Lobulated mass Feeding vessels often visible
Along choroid plexus Intense enhancement On postcontrast sequences
Papilloma: Iso-or hyperdense,and T1 isotense and #T2 SI
Hydrocephalus
Teratoma Pineal region Heterogenous mass Most are benign, but few can behighly malignant3rd ventrile Heterogeneous T1 and T2 SI;
Midline post fossa "T1 SI due to fat
Astrocytoma Cerebellum, 40% JPA: Cyst with enhancingmural nodes or solidenhancing mass
Most cerebellar astrocytomas
Cerebrum, 40% Are JPA
Brainstem, 20% High grade astrocytomas are> heterogenous and mixed indensity and enhancement
Intra-axial mass, #T17 "T2 SI
AT/RT Cerebellum Mimics medulloblastomamixed ependymoma, variablepattern of enhancement
Earlier age of presentation<2 years, poor prognosis
Brainstemglioma, focal
Medulla, tectum Medullary tumors enhanceuniformly
Focal: <50% brainsteminvolvement, margins
Tectal gliomas are discrete, donot
Medullary tumors are usually
enhance, present withhydrocephalus
JPA, tectal gliomas are grade IUsually well defined
Brainstemglioma, diffuse
Pons, diffuse: >50% maxinvolvement of brainstem intransaxial plane
Hypodense mass Differential diagnosis:abscess,encephalitis, demyelination#T1 and "T2 SI
Heterogenous enhancement
Hydrocephalus
Ependymoma Infrantentorial, 70% Iso- or hyperdense mass Commonly involve floor of thefourth ventricle and extend intoforamina of Luschka andMagendie
#T1 and heterogeneous T2 SI
Frequent calcification andcysts
Hydrocephalus
Medulloblastoma Vermis and roof of 4thventricle, vermis in children
Hyperdense, hetergenousmass #T1 and iso- or #T2 SIHydrocephalus
Most common pediatric postfossa tumor spread through thesubarachnoid space
Germinoma Involve stalk and extendinto hypothalamus
Well defined heterogenousmass Iso- or hyperdense #T1and mixed T2 SI
Diabetes insipidus
Pituitaryadenoma
Pituitary gland (intrasellar) Well-defined mass Headaches
Large adenomas can extendinto suprasellarcompartment, andcompress optic chiasm
#T1 SI Visual deficits
Endocrine dysfunction
8 S. Ndoro et al.

Posterior Fossa Tumors: Tumors of theCerebellum and Fourth Ventricle
Medulloblastoma WHO Grade IV
This is a malignant invasive embryonal tumor ofthe cerebellum with preferential manifestation inchildren, and an inherent tendency to metastasizevia CSF pathways. The annual incidence isapproximately 0.5 per 100,000 children<15 years. The peak age at presentation is5–7 years, with 70% of medulloblastomas occur-ring in children <16 years. Approximately 65%are male. At least 75% of childhood medulloblas-tomas arise in the cerebellar vermis and projectinto the fourth ventricle. Involvement of cerebel-lar hemispheres increases with the age of thepatient.
Pathology: Common genetic losses involve17p, 16q, 8p, 10q, and 11q. Chromosomal gainsof the MYC have been found. There are fouridentifiable principal subgroups of medulloblas-toma: WNT, SHH (Sonic Hedgehog), Group 3and Group 4. Medulloblastoma can occur in thefollowing histological variants (i) classic, (ii)desmoblastic/nodular, (iii) medulloblastoma with
extensive nodularity (iv) anaplastic and (v) largecell.
Treatment: Surgical resection with a goal ofgross total resection, radiotherapy, and chemo-therapy are indicated as treatment. Thirty to fortypercent of children require permanent VP shuntsfollowing posterior fossa resection.
Prognosis: Progression free survival rates of86% at 3 years and 79% at 5 years. Prognosis isbest in older children (as they can receive radio-therapy), children without metastases who havehad a complete resection and children in theWNT/SHH subgroups (Figs. 3 and 4).
Ependymal Tumors WHO Grade II-III
Ependymomas are slow growing tumors of chil-dren and young adults, originating from the wallof the ventricles or the spinal canal and are com-posed of neoplastic ependymal cells. They havean incidence of 0.2–0.3 per 100,000 per year.They account for 2–9% of all neuro-epithelialtumors, 6–12% of all intracranial tumors, and upto 30% of those occur in children <3 years. Sixtypercent of ependymomas are infratentorial with anaverage presenting age of 6.4 years. They can
Table 5 Immunohistochemical stains commonly used in neuropathology
Stain Cell type or structure stained Examples of tumors
MAP-2 Cell bodies and dendrites in mature andimmature neurons
Glial and neuronal tumors
Cytokeratins Epithelial cells Metastatic: carcinoma
Epithelial membrane antigen Meninges, epithelial cells Meningioma, carcinoma
S-100 Neural-crest-derived cells Melanoma, schwannoma,astrocytes
Synaptophysin Synapses Neuronal and neuroendocrinetumors
Ki67 (MIB-1) Mitotic activity All malignant tumours
GFAP (glial fibrillary acidicprotein)
Nucleus of proliferating cells Low in benign, high in malignanttumors
Table 6 Molecular diagnostic tests
Genetic variable Tumor type/indication
IN11 mutation Atypical teratoid/rhabdoid tumor: confirmation of diagnosis
MYCN/MYCC amplification Medulloblastoma: indicator of poor prognosis
1p/19q loss & EGFR amplification Anaplastic oligodendroglioma/ small cell glioblastoma: differential diagnosis
Pediatric Brain Tumors 9

Table 7 Molecular markers of pediatric brain tumors. (Adapted from Ichimura et al. 2012)
Tumortypes
Histologicaldiagnosis Subgroup
WHOgrades Genes Chromosomes Immunohistochemistry
Astrocytictumor
Pilocyticastrocytoma
Cerebellar/ I KIAA1549-BRAFfusion
7q34 gain
Optic/brainstem
Cerebral / I BRAF mut
Diencephalic
Diffuseastrocytoma
Pediatric II BRAF mut
Glioblastoma Pediatric,DIPG
IV H3F3Amut,ATRX mut
ATRX
DAXX mut,ADAM3AHD
DAXX
PDGFRAamp/mut
Neuronaltumor
Ganglioglioma I BRAF mut Trisomy 7
Ependymaltumor
Ependymoma Post Fossagroup A
II-III 1q gain LAMA2
Ependymoma Post Fossagroup B
II 6q loss, 22qloss,
NELL2
9q gain, 15qgain,
18q gain
Embryonaltumor
Medulloblastoma Wnt IV CTNNB1mut, MLL2
Monosomy 6 CTNNB1
MLL3 mut,SMARCA4mut,
DKK1
DDX3Xmut
Shh IV PTCH1mut, SUFUmut,
9q del,chromothripsis
SFRP1, GAB1
GLI amp,MYCN amp
(TP53germline mut)
GLI1
Group 3 IV SMARCA4mut, MYCamp
i17q, 5q loss,10q loss
NPR3
1q gain
Group 4 IV KDM6Amut
i17q KCNA1
AR/RT IV SMARCB1mut,SMARCA4mut
22q loss SMARCB1 loss
Germinalcell tumor
Germinoma KIT mut i12p, TrisomyX
KIT
Provides an overview of the most typical findings of each tumor type listedAT/RT atypical teratoid/rhabdoid tumor, DIPG diffuse intrinsic pontine glioma, mut mutation, HD homozygous deletion,amp amplification
10 S. Ndoro et al.

occur at any site along the ventricular system andspinal canal. Ependymomas are classified under therevised WHO schema as subependymoma andmyxopapillary ependymoma (grade 1),ependymoma (grade 2), malignant ependymoma(grade 3), and ependymoblastoma (grade 4).
Pathology: 30% of ependymomas show aber-rations involving chromosome 22, 6q and 9q. TheMF2 gene is involved in ependymoma tumorgenesis. They show a pattern of perivascularpseudo-rosettes and ependymal rosettes. Subtypesinclude, (i) cellular, (ii) papillary, (iii) clear cell,and (iv) tanycytic.
Treatment: The goal of treatment is gross totalresection where feasible. Radiotherapy 45-54Gyfor low-grade (Grade II) and 54-60Gy for high-grade ependymomas (grade III). Chemotherapywith the use of vincristine and cyclophosphamidewith or without etoposide is the favored treatmentin children <3 years.
Prognosis: Presence of residual disease on post-operative imaging is the most important negativeprognostic factor, 5 year survival 20–30% (Fig. 5).
Fig. 3 (a, b) T1 axial and T 1 sagittal with contrast views of Medulloblastoma
Fig. 4 T1 axial view post resection of Medulloblastoma
Pediatric Brain Tumors 11

Cerebellar Pilocytic Astrocytomas WHOGrade I
Pilocytic astrocytoma is a slow growing, predomi-nately cystic, and generally well-circumscribedastrocytoma. It is the most common primary braintumor in children. It represents 85% of cerebellarand 10% of cerebral astrocytomas. Pilocytic astro-cytomas can also arise in the optic nerve (optic nerveglioma) or chiasm, hypothalamus, thalamus,brainstem, and spinal cord. Approximately 15% ofpatients with NF1 develop pilocytic astrocytoma.Peak incidence is between 5 and 15 years of age.
Pathology: Pilocytic astrocytomas display lowcellularity, with a typical biphasic pattern:compacted bipolar cells with Rosenthal fibersand loose-textured multipolar cells with granularbodies and microcysts. They are positive forGFAP and protein�100.MIB1 labeling is usuallylow (<5%). They carry duplications of the BRAFoncogene at 7q34 that result in increased mitogen-activated kinase signaling.
Treatment: Definitive treatment for pilocyticastrocytomas is complete surgical resection of thetumor. Radiotherapy is indicated for nonresectablerecurrence or recurrence with malignant histology.Chemotherapy is preferable in younger
patients where surgery is not feasible and thetumour is progressive. Pilocytic astrocytomas ofthe optic pathways (common in NF1) are not usu-ally resectable and are managed withchemotherapy.
Prognosis: Completely resected PAs haveexcellent prognosis, 10 year survival ofalmost 100%, and when residual tumor is present,there is a 10 year survival of 50%. Malignanttransformation is possible but rare (Fig. 6).
Tumors of the Mid-Brain andCervico-Medullary Region
Brain Stem Gliomas (DIPG: DiffuseIntrinsic Pontine Gliomas, Focal,Dorsal, Exophytic, CervicomedullaryTumors)
Brain Stem tumors account for 10–15% of allprimary childhood CNS tumors, the majoritybeing gliomas. Sixty to eighty percent of pediatricbrainstem tumors are DIPGs and occur in the pons.
In the UK, the incidence of brain stem tumorsis ~3.8 per million, with sex incidence equal andthe mean presenting age is 5–10 years.
Fig. 5 (a, b) T1 axial with contrast view pre and post op views of Ependymoma
12 S. Ndoro et al.

Pathology: Dorsally exophytic gliomas areshown to be predominately pilocytic astrocyto-mas. Diffuse intrinsic pontine gliomas demon-strate malignant histology, astrocytoma WHOgrades III, IV. Cervicomedullary has various his-topathologies including, pilocytic astrocytoma,fibrillary astrocytoma, oligodendroglioma, andganglioglioma.
Treatment: Classically, DIPGs arise from theventral pons and can extend into the medulla andmidbrain. Surgical debulking carries great risk ofmorbidity/mortality and has no effect on outcome.Patients with gliomas located outside the pons –including focal cystic, exophytic, andcervicomedullary tumors – frequently benefit fromdebulking. These milder forms of brain stem glio-mas have a better prognosis and prolonged survival.
Prognosis: If a brainstem glioma has a malig-nant pathological picture on biopsy, survival willbe zero percent at 12 months, despite therapy. Thelow grade brain stem gliomas have a better out-come with 5 year progression free survival at60–72% and at 5 years 89–95% of patients sur-vive (Figs. 7 and 8).
Tumors of the Sellar/SuprasellarRegion
Craniopharyngioma WHO Grade I
Craniopharyngiomas are benign partly cystic epi-thelial tumors of the sellar region presumablyderived from Rathke’s pouch epithelium. It cangrow to enormous sizes and extend into the thirdventricle and laterally into the temporal lobes.There is a peak in children (5–15 years) foradamantinomatous craniopharyngiomas. Theyare accompanied by a triad of symptoms, visualproblems, endocrine or metabolic problems, andsymptoms of raised intracranial pressure second-ary to hydrocephalus.
Pathology: Two histological types aredescribed: (a) adamantinomatous, consisting ofsheets of epithelial cells with a tendency towhorl, a palisade of columnar cells at the periph-ery, and containing “wet” keratin; and, (b) papil-lary, consisting of epithelial tissue resting on afibrous stroma, without wet keratin.
Fig. 6 (a, b) T1 axial views with contrast of a cerebellar pilocytic astrocytoma
Pediatric Brain Tumors 13

Fig. 7 (a, b) T2 saggital and axial views of DIPG
Midbrain:Tend to beGrade 1(Tectal glioma)
Pons:DIPGs are60-80%of Brain stemGliomas:Tend to be High grade
Cerebellum
Medulla:Tend to be Exophytic Low grade(Pilocytic astrocytoma)
Midbrain: Involved in vision, hearing, eye movement and bodymovementPons: Involved in motor control and sensory analysisMedulla: Maintains vital body functions, such as breathing andheart rate
Fig. 8 Saggital view of brain stem and cerebellum
14 S. Ndoro et al.

Treatment: Craniopharyngiomas are appro-ached via three routes (i) transnasal transphenodialapproach (if completely located within the sella), (ii)pterional approach and splitting of the Sylvian fis-sure and (iii) subfrontal approach through the laminaterminalis. Subtotal resection is usually achievedand no tumor should be forcibly pulled away fromthe optic nerve, vascular structures, or hypothalamusto avoid hypothalamic damage. Diabetes insipidusmay develop. Radiotherapy aids in preventingregrowth when residual tumor is left behind. Recur-rence rates are comparable to complete resection at10 years with less hypothalamic morbidity thanradical surgery. In younger children it may be bestto postpone radiotherapy to minimize deleteriouseffect on IQ, recognizing that reoperation may benecessary for recurrence.
Prognosis: Survival rate at 5 years is 94% butlong-term follow up is required given the recur-rence rate approaches 40% when excision is neartotal or subtotal (Fig. 9; Table 8).
Optic Pathway Gliomas (OPGs) WHOGrade I, II
OPGs are a subset of low-grade gliomas that occurin the optic pathway (optic nerve, chiasm, tract/
radiations). They grow as infiltrative lesions or aslarge expansive masses. They account for 4–6%of all pediatric brain tumors. OPG is the mostfrequent central nervous system tumor in childrenwith Type 1 neurofibromatosis (NF1), affectingapproximately 15–20% of patients (Cassina et al.2019). Mode of inheritance is autosomal domi-nant, from mutations in a gene on chromosome17q11.2. Owing to their location, 35–50% ofaffected children present with reduced visual acu-ity (Campen and Gutmann 2018).
Pathology: The majority are low-grade glio-mas, mostly juvenile pilocytic astrocytomas,fibrillary astrocytomas, and pilomyxoidastrocytomas.
Fig. 9 (a, b) T2 sagittal view and T1 coronal view of a craniopharyngioma
Table 8 Complications of transphenodial surgery
Complications of transphenodial surgery
CSF leak
Meningitis
SIADH: DI (usually transient)
New visual deficits
Palsy of CNII, VI
Vascular injury (carotid a.), stroke
Hypopituitarism
Hypothalamic injury
Death
Pediatric Brain Tumors 15

Treatment: Surgery is controversial due tohigh morbidity and the high correlation withNF1. Surgery is offered in cases where the OPGis clearly unilateral, in whom proptosis and severevisual loss are apparent, or to relieve mass effect.Radiotherapy provides excellent results in termsof stabilization and tumor regression, withimprovement in visual function if visual loss isnot long-standing; it is contraindicated in childrenless than 8 years of age and with NF 1. Chemo-therapy is increasingly used in children under10 years of age.
Prognosis: Gliomas restricted to the opticnerves rarely prove fatal but can lead to progressivevisual loss. Four year progression free survival is~50% for patients with chiasmatic-hypothalamicgliomas, with 4 year overall survival of 90%.
Pituitary Adenomas
Pituitary adenoma is a rare benign neoplasmderived from parenchymal cells of adenohypoph-ysis. Micro-adenomas are <10 mm and macro-adenomas are 20 mm in size. Pituitary adenomaswith endocrine activity or of sufficient size toproduce symptoms make up to 10–12% of allintracranial neoplasms. These are classicallydivided into functional [secreting: prolactin(PRL), adrenocorticotropic hormone (ACTH),growth hormone (GH), thyrotropin (TSH), gonad-otropins (LH & FSH)], and nonfunctional. Thereis a female predominance in PRL and ACTHsecreting tumors and a male predominance inGH secreting tumors.
Treatment: Requires a multidisciplinary teamof neurosurgeons, endocrinologists, and radiationoncologists. Surgical approaches include: (i)Endoscopic transphenoidal (commonly used),(ii) trans cranial (for laterally extending macro-adenomas after failed transphenodial surgery).
Prognosis: This is dependent upon patient sta-tus, comorbidity, tumor size and extension, andfunctional status of the patient. Thirty percent ofmales that present with macroadenomas in puber-tal years normalize their prolactin levels. Femaleswho present with secondary amenorrhea andgalactorrhea secondary to microadenomas over
75% will achieve biochemical remission. Patientswith Cushing’s disease can achieve remissionwith trans-sphenodial surgery in the majority ofinstances 70–90% (Fig. 10).
Tumors of the Pineal Region
Pineoblastoma (PB) WHO Grade IV
PB is a rare highly malignant primitive embryonaltumor of the pineal gland, preferentially affectingchildren. They comprise ~40% of all pineal paren-chymal tumors which represent <0.3% of allintracranial neoplasms. They most often presentin the first decade of life.
Pathology: Chromosomal abnormality is seenon chromosome 22. Highly pattern-less sheets ofdensely packed small cells, with the possible pres-ence of rosettes are seen. They also show reactiv-ity for neuronal, glial, and photoreceptor markers.
Treatment: Extensive resection is thought toimprove prognosis. Surgery is followed by radio-therapy and chemotherapy.
Prognosis: 5 year survival rate ~50% (Fig. 11).
Fig. 10 Pituitary adenoma filling the sella and extendinginto the suprasellar space (coronal and sagittal TI-WI withcontrast)
16 S. Ndoro et al.

Germ Cell Tumors (Germinoma,Embryonal Carcinoma, Yolk Sac Tumor,Choriocarcinoma, and Teratomas)
This is a rare group of morphological andimmune-phenotypically similar tumors, originat-ing from midline regions (gonads, mediastinum,and retroperitoneal area) and affecting childrenand young adults. Far East Asia has the highestprevalence. They account for 2–3% of primaryintracranial neoplasms and 8–15% of pediatricseries. Eighty to ninety percent of CNS germ celltumors affect patients <25 years.
Pathology: Elevated circulating gonadotropinlevels are thought to be a factor in the pathogen-esis of germ cell tumors. Mitotic activity isincreased, and T-cell infiltration is a typical fea-ture; there is also strong cytoplasmic labeling forc-Kit and nuclear reactivity for OCT4, and othermarkers are B-hCG and cytokeratins. Mature ter-atomas are composed exclusively of fully differ-entiated tissue elements, comprising skin, brain,
cartilage, fat, and muscle. Immature teratomascontain incompletely differentiated componentsresembling fetal tissue. Yolk sac tumor is com-posed of primitive appearing epithelial cells, puta-tively representing yolk cell endoderm, set inloose variably cellular and often myxoid matrix.Embryonal carcinoma is composed of large cells,forming abortive papillae and gland-like spacesand may replicate the structure of the earlyembryo. Choriocarcinoma is characterized byextra-embryonal differentiation along trophoblas-tic lines. Identification of cytophoblastic elementsis required for diagnosis.
Treatment: Germ cell tumors are amenable toradiotherapy. Surgery is also indicated. Chemo-therapy with the use of platinum-based regimensis also used in secreting germ cell tumours(BHCG and AFP).
Prognosis:Germinomas have 10-year survivalrates of ~90%. Embryonal carcinomas 1-year sur-vival rates are ~80%. Yolk sac tumors 1-yearsurvival rates are 33%. Malignant teratomas 10-year survival rate are 70% (Fig. 12; Table 9).
Fig. 11 Pineoblastoma causing noncommunicating hydrocephalus (Transaxial T1-WI, without and with contrast)
Pediatric Brain Tumors 17

Tumors of the Choroid Plexus
Choroid Plexus Papilloma and ChoroidPlexus Carcinoma
Choroid plexus papilloma is an intraventricular pap-illary neoplasm derived from choroid plexus epithe-lium. They account for 0.3–0.6% of all brain tumorsbut 2–4% of those occur in children <15 years and10–20% of those manifesting in the 1st year of life.The average annual incidence is approximately 0.3per million population per year. They are located inthe lateral (50%), third (5%), and fourth ventricles(40%). Ectopic locations are rare.
Choroid plexus carcinomas: incidence is 20%of choroid plexus tumors.
Pathology: Choroid plexus papillomas arecircumscribed cauliflower like masses that adhereto the ventricular wall but are usuallywell delineated
from brain tissue. They express cytokeratin,vimentin, and many tumors express S100 and GFA.
Choroid plexus carcinomas show frank signsof malignancy; this includes at least four of thefollowing five features: frequent mitosis (usually>5 mitoses/10HPF), increased cellular density,nuclear pleomorphism, blurring of the papillarypattern with poorly structured sheets of tumorcells, and necrotic areas.
Treatment: Total surgical resection is curativeif achievable. Choroid plexus papillomas canmetastasize along the CSF pathway and patientsshould undergo CNS staging.
Prognosis: Gross total resection has 10-yearsurvival rate of 85%, while those with subtotalresection has survival rate of 56%.
The overall 5-year survival rate for patients withchoroid plexus carcinomas is ~50% (Fig. 13).
Neurocutaneous Syndromes
See Table 10.
Table 9 Common markers in pineal region tumors
Pineocytoma B-HCG AFP
Pineoblastoma Negative Negative
Germinoma Negative Negative
Teratoma Negative/positive Negative
Embryonal carcinoma Positive Positive
Choriocarcinoma Positive Negative
Yolk sac tumor Negative Positive
Fig. 12 Germinoma. Slightly heterogeneous, mildlyenhancing T1-hypointense, T2-hyperintense mass in thepineal region (Transaxial T1-WI with contrast) Fig. 13 Choroid plexus papilloma in the fourth ventricle.
Noncommunicating hydrocephalus with dilation of the tem-poral horns of the lateral ventricles (Transaxial T1-WI withcontrast)
18 S. Ndoro et al.

Table 10 Neurocutaneous syndromes
NF 1 VonRecklinghausen’sdisease NF2
Tuberous sclerosis(Bourneville’sdisease)
Von Hippel-Lindausyndrome
Incidence 1:4000 1:50000 1:30000 1:40000
Inheritance Autosomaldominantchromosome 17
Autosomal dominantchromosome 22
Autosomaldominantchromosome 9and 11
Autosomal dominantchromosome 3
Pathology Overgrowth ofmesoderm andectoderm
“Tuber” growtharound ventricleswhich can transformmalignant
Multiplehemangioblastomas
Skin Café-au-lait spots Adenomasebaceum
Cutaneousneurofibromas
Vitiligo
Plexiformneurofibroma
Fibromas
Mollusca fibrosa Café-au-lait
Shagreen spots
Ungual fibrosis
Eyes Lisch nodules Post capsular cataractat a young age
Retinal hamartomas Retinal hemangiomas(50%)Microphthalmia
Retinal phakomas
Skeletal Scoliosis Cystic metacarpals
Subperiostealneurofibromas
Widened spinalcanal
CNS Dural ectasia Microgyria
Meningocele Hydrocephalus
Aquaduct stenosis Moya-moya
Moya-moya
AVMs, aneurysms
Mentalretardation
40% 60%
Epilepsy 10–15% 100% ‘Salaam’spasms
CNS neoplasia Cranial: Cranial: Astrocytomas(from tubers)
60%
Optic nerve glioma Bilateral acousticneuromas
Subependymalgiant cellastrocytoma (at f. ofMunro)
Cranial:
Acoustic neuroma Meningiomas Cerebellarhemangiblastoma (65%)
Multiplemeningiomas
Astrocytomas Brain stemhemangioblastoma (20%)
Low grade astros Hamartomas Spine:
Ependymomas Spine: Hemangioblastoma(15%)Hamartomas Ependymomas
Spine: Nerve rootschwannomasMeningioma
Neurofibroma
Glioma
(continued)
Pediatric Brain Tumors 19

Conclusion and Future Directions
Optimal management of pediatric patients withbrain tumors requires a multidisciplinary approachthat involves in general: surgery, radiotherapy,chemotherapy, and rehabilitation. That is, Neurosur-geons, neurologists, neuroradiologists, neuropathol-ogists, radiation oncologists, medical oncologists,pediatricians, specialists in rehabilitation medicine,nurses, and social workers are all actively involvedin management. However, patient outcomes remainlow for the vast majority of patients with malignantneoplasms of the CNS. Novel therapies andapproaches are required if progress is to be achievedon this frontier. The use of clinical trials with focuson targeted therapies and their delivery should bemore aggressively pursued. Special consideration isrequired in cases where a palliative approach is
taken. Continued care with occupational therapists,physiotherapists, and speech and language thera-pists is paramount for improving quality of life forthese patients and their families. Patients progres-sively lose independence, cognitive ability, developbehavioral dysfunction, increase frequency of sei-zures, develop venous embolism, and develop dys-phagia due to cranial nerve or bulbar palsy. Theseterminal issues place extraordinary psychologicaland physical burdens on patients and their families.Tangible strides need to be made in curing thesemalignancies, with emphasis on pediatric neuro-oncology as a gateway to individualized treatment.A concentrated effort on patient’s quality of lifethrough support from psychologists and providingbetter patient awareness of outcome and prognosisis needed to improving overall survival and qualityof life.
Table 10 (continued)
NF 1 VonRecklinghausen’sdisease NF2
Tuberous sclerosis(Bourneville’sdisease)
Von Hippel-Lindausyndrome
Otherneoplasia
Leukemia Bilateral acousticneuromas
Cardiacrhabdomyoma(30%)
Renal cell carcinoma(30%), angiomatosis
Neuroblastoma Renalangiomyolipoma(60%)
Pheochromocytoma(10%)
Medullary thyroidcarcinoma
Cysts in lung, liver,spleen
Cysts (60%) liver,pancreas & kidney
MEN Pancreatic adenoma Epidydimal cystadenoma
Other Hypertension frompheochromocytomaor renal arterystenosis
Thoraco-abdominalaortic aneurysm
Diagnosis 6 CAL spots Relative with NF2and 1 acoustic
Facialangiofibroma
Multiple CNShemangioblastomas
2 neurofibromas 2 of neurofibroma,meningioma, glioma,schwannoma,cataract at young age
Periungualsubungual fibroma
One CNShemangioblastoma andone visceral lesion with afirst degree relative withVHL
1 plexiformneurofibroma
Fibrous plaque offorehead and scalp
Axillary freckling Triad of mentalretardation,seizures andadenoma sebaceum(<50%)
Osseus lesion
Optic glioma
2 Lisch nodules
Relative with NF1
20 S. Ndoro et al.

References
Campen CJ, Gutmann DH. Optic pathway gliomas inNeurofibromatosis type 1. J Child Neurol. 2018;33(1):73–81.
Cassina M, Frizziero L, Opocher E, et al. Optic pathwayglioma in type 1 neurofibromatosis: review of its path-ogenesis, diagnostic assessment, and treatment recom-mendations. Cancers (Basel). 2019;11(11):pii: E1790.
Ichimura K, Nishikawa R, Matsutani M. Molecularmarkers in pediatric neuro-oncology. Neuro Oncol.2012;14:iv90–9.
Limond J, Thomas S, Bull KS et al. Quality of survivalassessment in European childhood brain tumour trials,for children below the age of 5 years. Eur J PaediatrNeurol. 2019;19(2):202–10, 2015 Mar.
Peragallo JH. Visual function in children with primarybrain tumors. Curr Opin Neurol. 2019;32(1):75–81.
Pediatric Brain Tumors 21
Top Related