






Languages
Pages
Legal

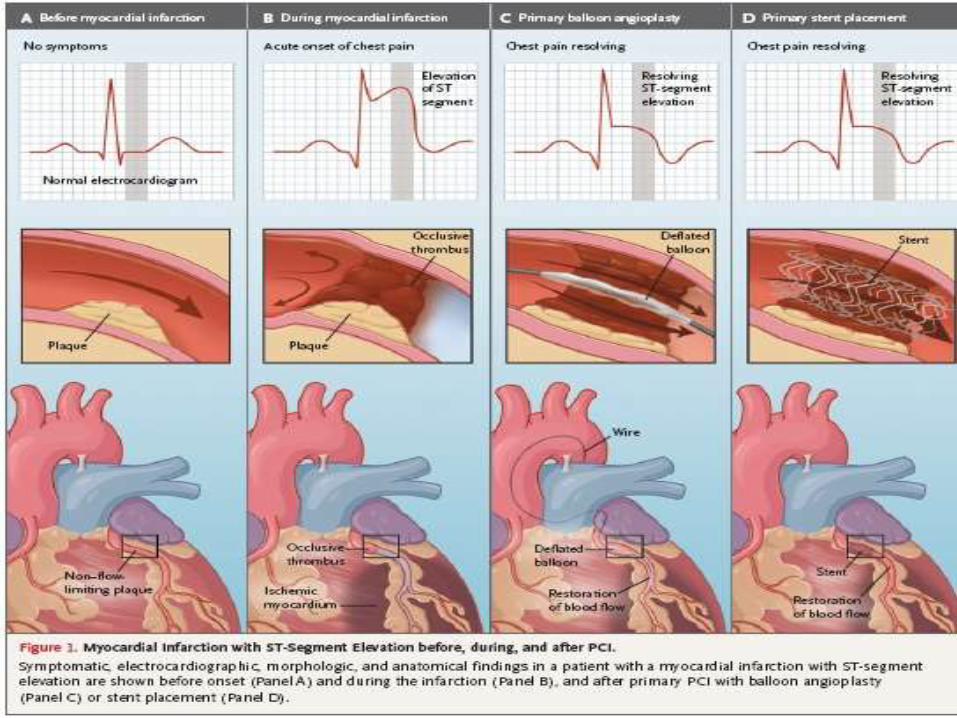
Primary PCI vs. thrombolysis
Dr. Ameel Toma
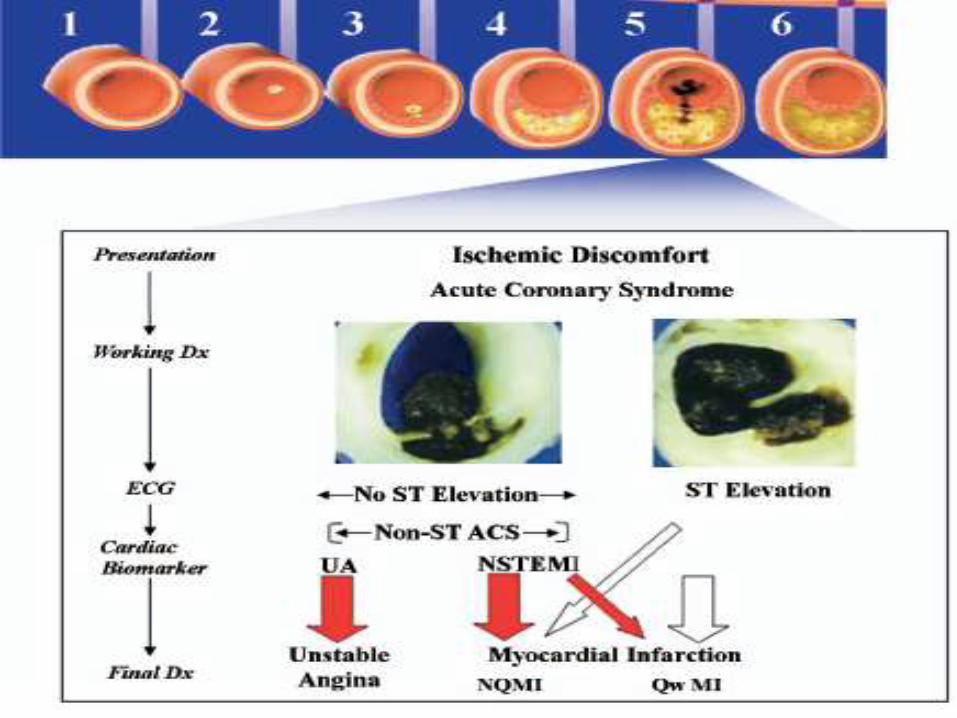
Acute coronary syndrome
1- ST- elevation myocardial infarction (STEMI).
2- Non St- elevation – ACS (NSTE-ACS):
include
- Non ST-elevation myocardial infarction
(NSTEMI).
- Unstable angina.
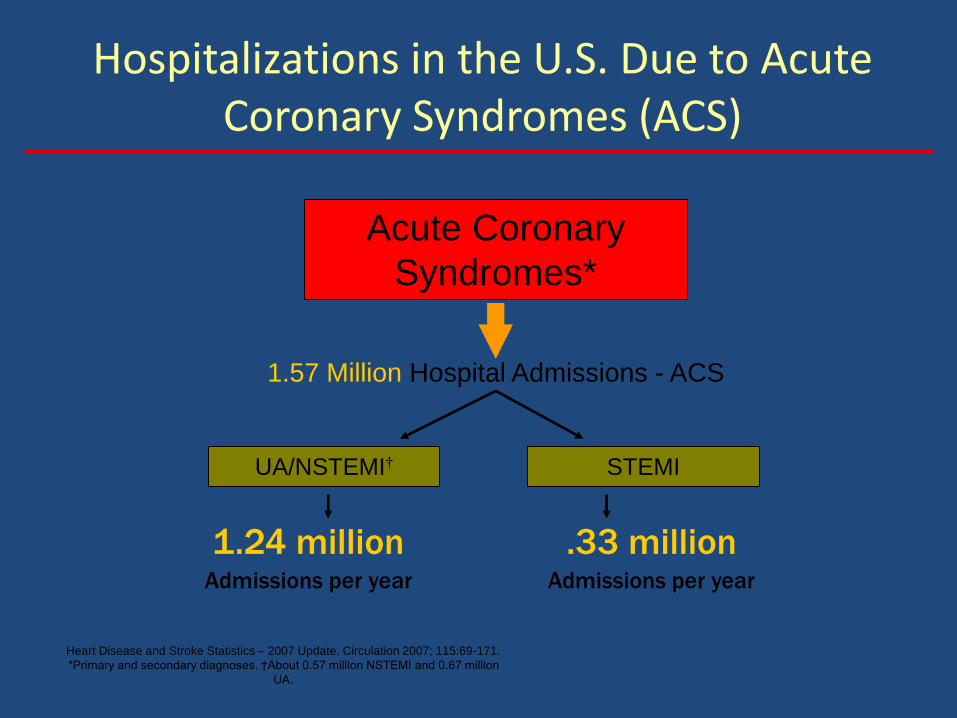
Hospitalizations in the U.S. Due to Acute Coronary Syndromes (ACS)
Acute Coronary
Syndromes*
1.57 Million Hospital Admissions - ACS
UA/NSTEMI† STEMI
1.24 millionAdmissions per year
.33 millionAdmissions per year
Heart Disease and Stroke Statistics – 2007 Update. Circulation 2007; 115:69-171.
*Primary and secondary diagnoses. †About 0.57 million NSTEMI and 0.67 million
UA.
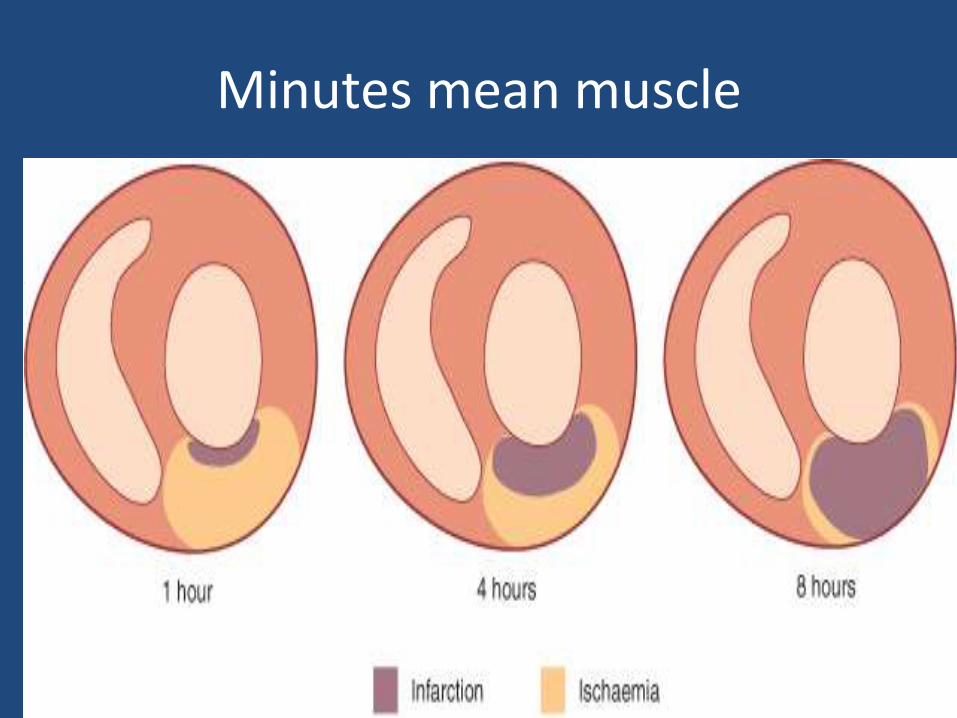
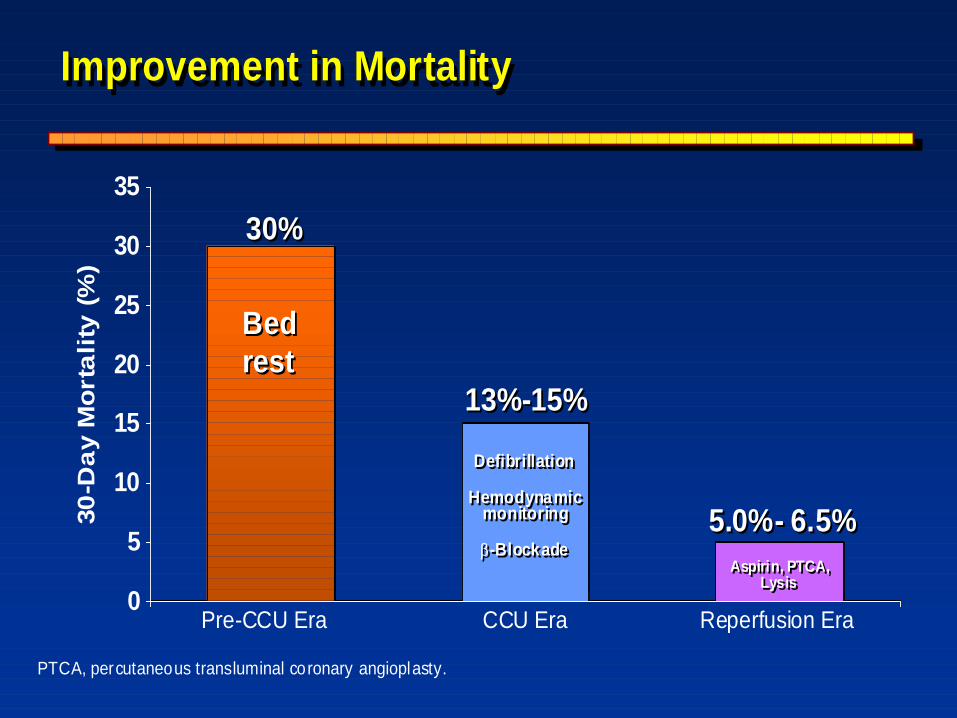
Minutes mean muscle
Chest Pain
• Rapid Dx &Tx = saved muscle = improved outcome
Danger:
acute-- arrhythmia(VF)—death ---- CCU
Late - muscle loss--- heart failure
(increase morbidity, mortality, cost)
PTCA, percutaneous transluminal coronary angioplasty.
0
5
10
15
20
25
30
35
30
-Da
y M
orta
lity
(%
)
5.0%- 6.5%5.0%- 6.5%
13%-15%13%-15%
30%30%
Defibrillation
Hemodynamicmonitoring
b-Blockade
Defibrillation
Hemodynamicmonitoring
b-BlockadeAspirin, PTCA,
Lysis
Aspirin, PTCA,Lysis
Bed
rest
Bed
rest
Pre-CCU Era CCU Era Reperfusion Era
Improvement in MortalityImprovement in MortalityImprovement in Mortality
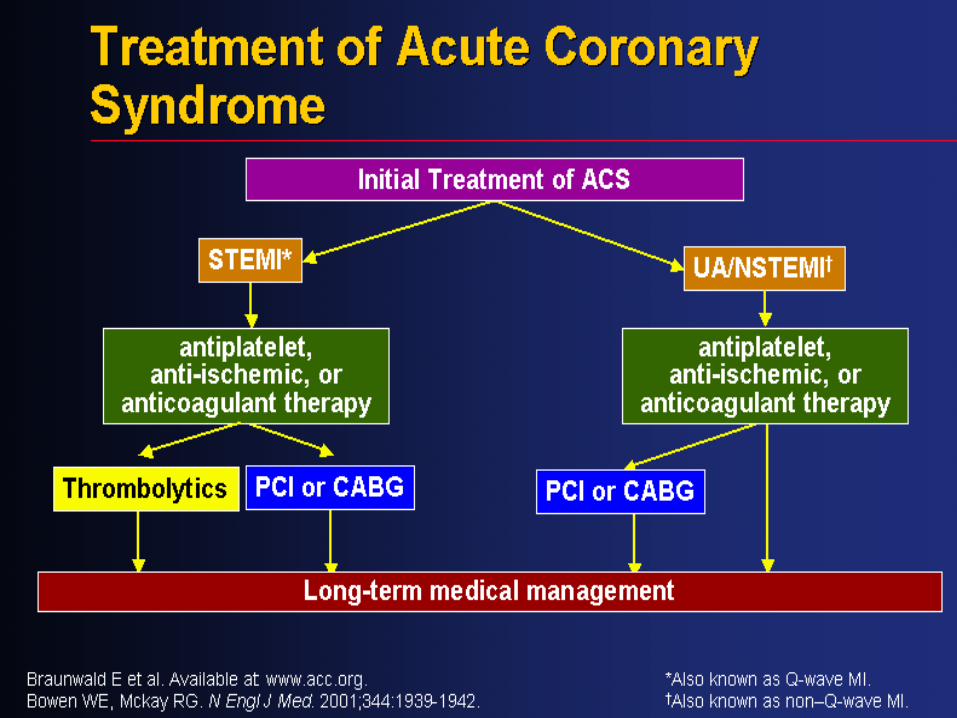
STEMI:
1-Early management.
2-Early reperfusion therapy as much as possible.
3- Optimal long-term treatment & secondary prevention.
Early management of acute MI:
A- Provide facility for defibrilation.
B- Immediate measures:
- high flow oxygen. - IV analgesia,Nitrate
- IV access. - aspirin 300 mg
- 12 leads ECG - clopidogrel 600mg
- continous ECG montor - B-blockers
C- Detect & manage complication:
- recurrent ischemia - arrhythmia
- heart failure
Revascularization (REPERFUSION):
1. Thrombolytic(fibrinolytic):
used to lyses the clot
- streptokinase, tPA, tenectiplase.
2. Percutaneouse coronary intervention (PCI)
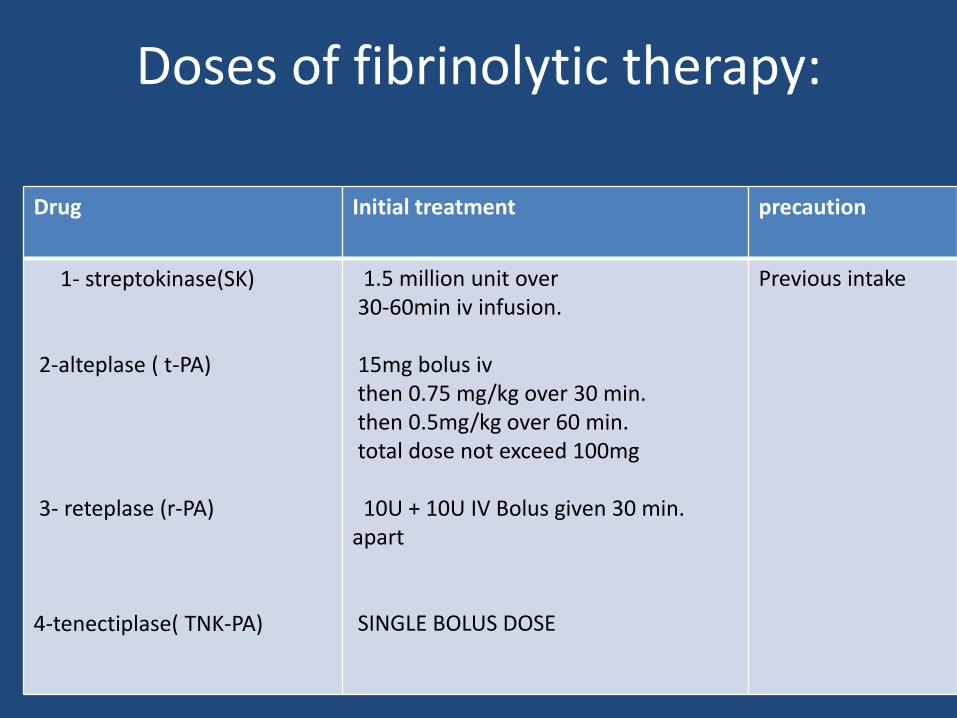
Doses of fibrinolytic therapy:
precautionInitial treatmentDrug
Previous intake1.5 million unit over30-60min iv infusion.
15mg bolus ivthen 0.75 mg/kg over 30 min.then 0.5mg/kg over 60 min.total dose not exceed 100mg
10U + 10U IV Bolus given 30 min. apart
SINGLE BOLUS DOSE
1- streptokinase(SK)
2-alteplase ( t-PA)
3- reteplase (r-PA)
4-tenectiplase( TNK-PA)
Time, time
Door to Needle Time
< 30 min
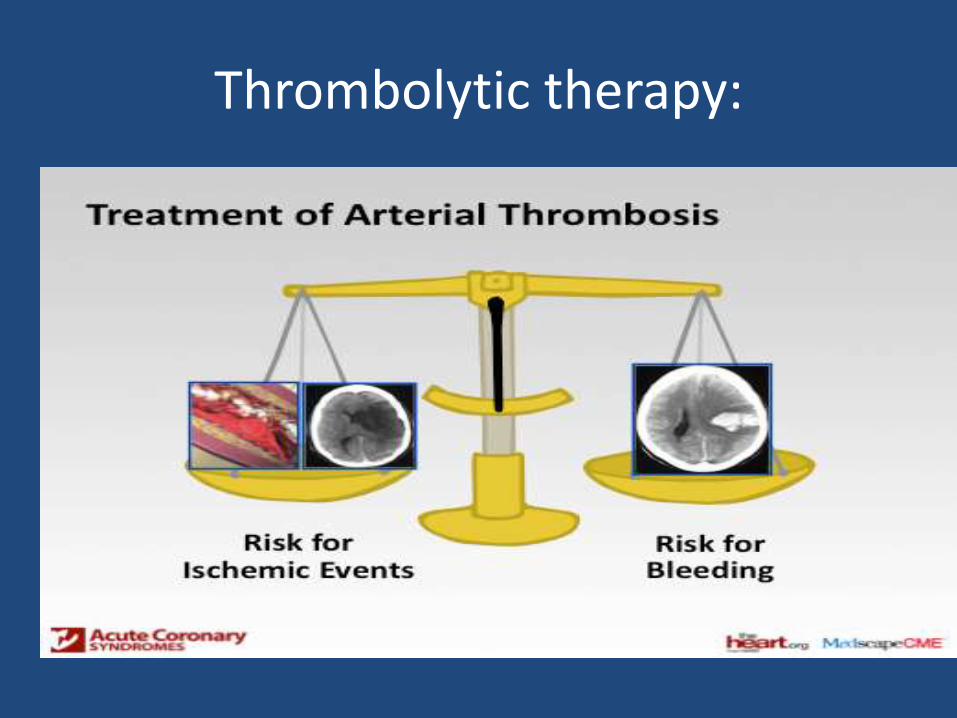
Thrombolytic therapy:
Fibrinolytic therapy:
Risk of intra cerebral therapy:
1-age >65 y.
2- low body weight(<70 Kg).
3- initial hypertension(>180/110).
4- use of tPA.
Absolute contraindication for fibrinolytic therapy:
• Previous intracerebral bleeding.
• Ischemic stroke within 3 months.
• Brain structural lesion( tumor, malformation).
• Dissecting aortic aneurysm.
• Active bleeding
Thrombolytic therapy:
Pitfalls:
• Contraindication
• Complication
• Effectiveness:
• After successful thrombolysis:
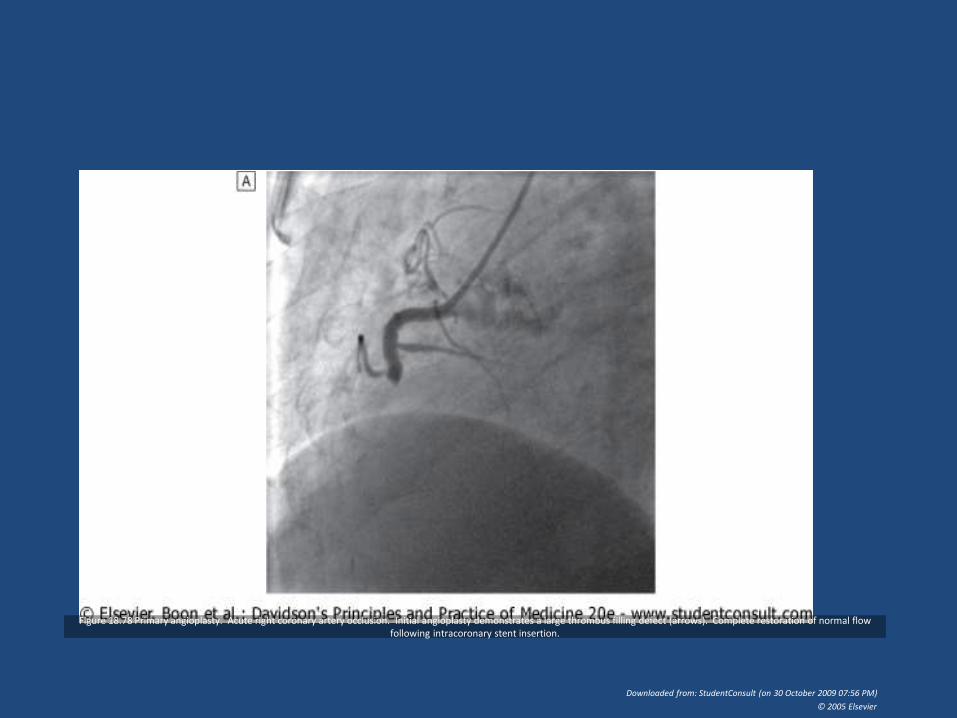
Figure 18.78 Primary angioplasty. Acute right coronary artery occlusion. Initial angioplasty demonstrates a large thrombus filling defect (arrows). Complete restoration of normal flow following intracoronary stent insertion.
Downloaded from: StudentConsult (on 30 October 2009 07:56 PM)
© 2005 Elsevier
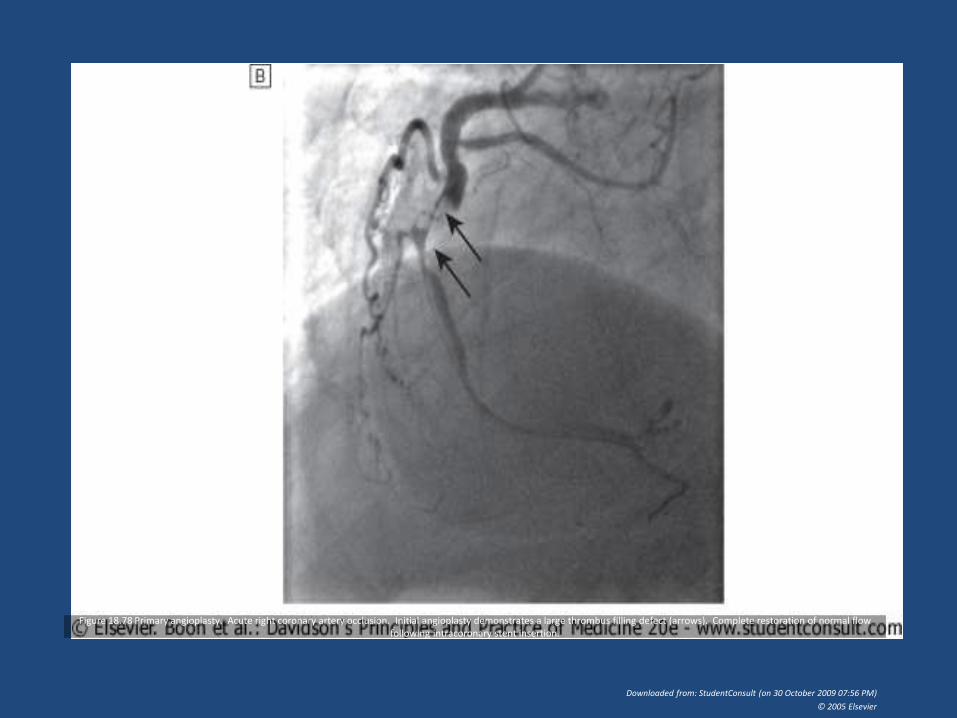
Figure 18.78 Primary angioplasty. Acute right coronary artery occlusion. Initial angioplasty demonstrates a large thrombus filling defect (arrows). Complete restoration of normal flow following intracoronary stent insertion.
Downloaded from: StudentConsult (on 30 October 2009 07:56 PM)
© 2005 Elsevier
PCI (Percutaneous Coronary intervention)
• Primary PCI (PPCI):
• Rescue PCI: failed thrombolysis
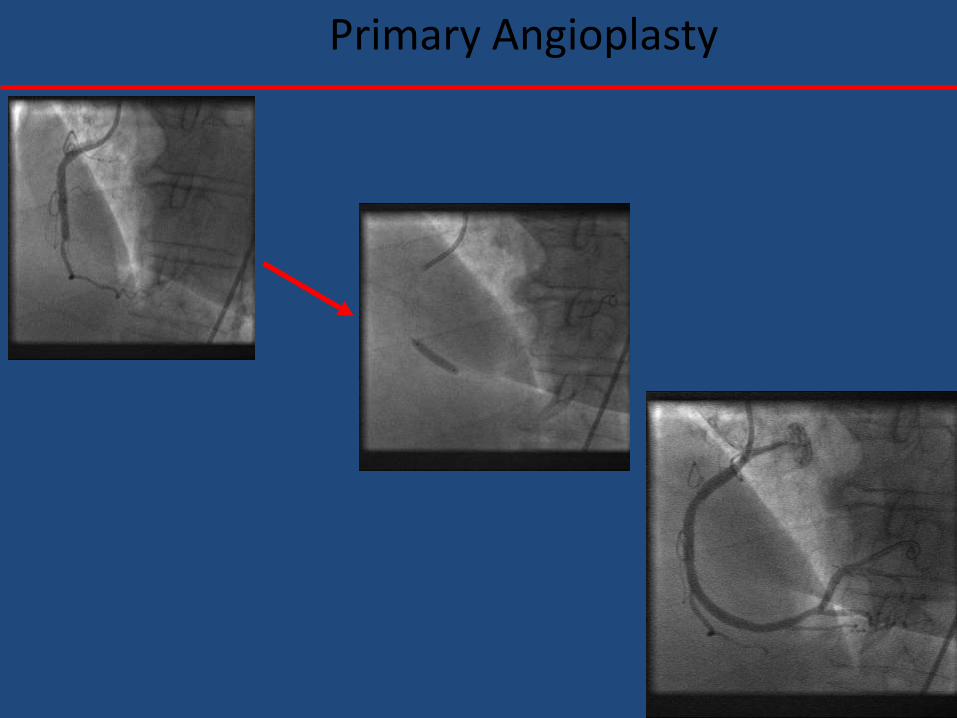
Primary Angioplasty
PCI:
• Invasive procedure.
• More effective.
• Less recurrent ischemia.
• Less hospital stay.
• Need experienced person.
• Expensive.
Direct from ambulance to cath.
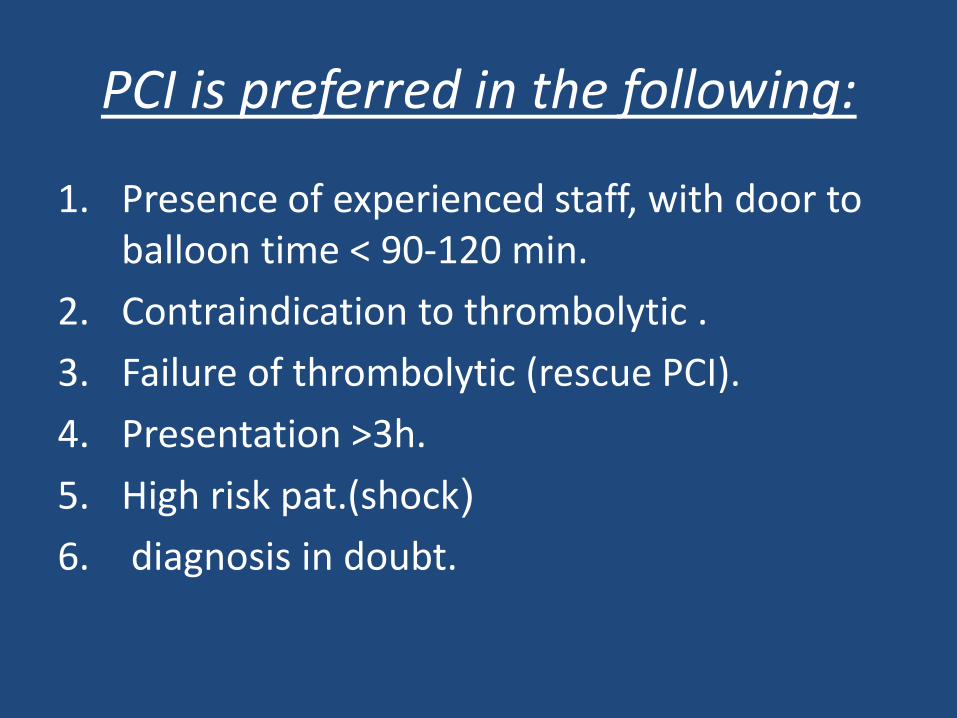
PCI is preferred in the following:
1. Presence of experienced staff, with door to balloon time < 90-120 min.
2. Contraindication to thrombolytic .
3. Failure of thrombolytic (rescue PCI).
4. Presentation >3h.
5. High risk pat.(shock(
6. diagnosis in doubt.
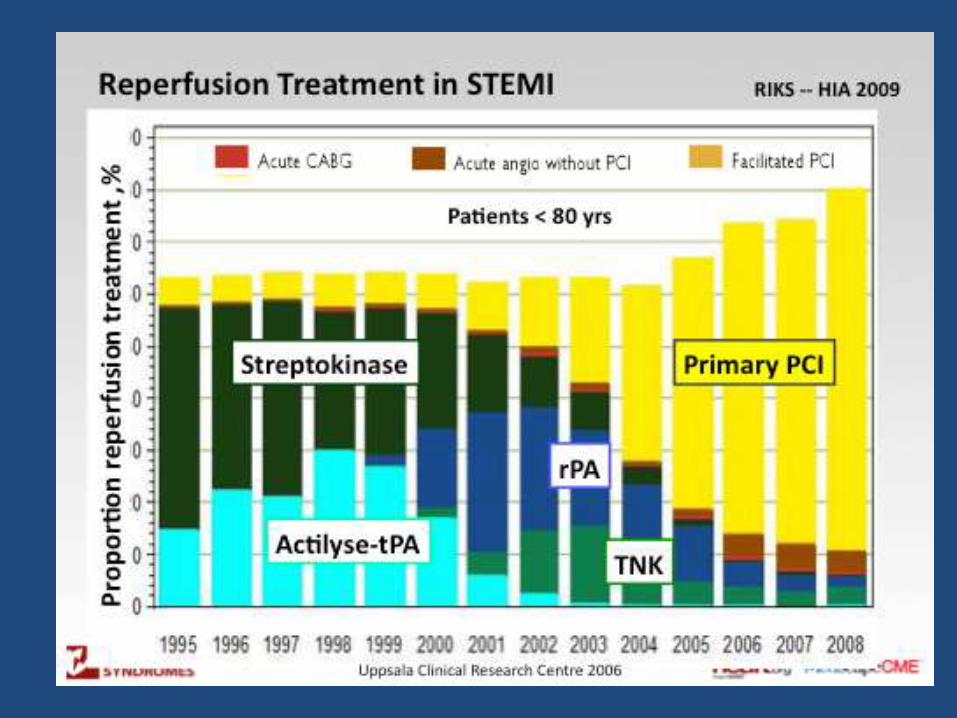
Reperfusion: ??
Thrombolytic
VS
PCI

THANK YOU
Top Related