







Languages
Pages
Legal


Great state. Great opportunity.
Torres and Cape Hospital and Health Service
PC12 Child Health CheckPart 2 - Physical Assessment workbook
Preventative Care


Participant Details
PC122 Physical Assessment - Child Health Check
Name
Community
Site
Position
Date Completed
PaRROT Program - Child Health Check: Part 2 | A primary health care approach


PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Contents
PC122 Child Health Check - Part 2: Physical Assessment 5
PC122 Pre-Session Survey 7
PC1221-1 Introduction to Skin 8
PC1221-1 Learning Activity 16
PC1221-2 Rashes 17
PC1221-2 Learning Activity 21
PC1221-3 Infections 22
PC1221-3 Learning Activity 26
PC1221 Quiz 27
PC1222-1 Introducing Ears and Hearing 29
PC1222-1 Learning Activity 40
PC1222-2 Otoscopy 41
PC1222-2 Learning Activity 48
PC1222-3 Tympanometry 49
PC1222-3 Learning Activity 52
PC1222-4 Audiometry 53
PC1222-4 Learning Activity 56
PC1222 Quiz 57
PC1223-1 Introducing Eyes and Vision 60
PC1223-1 Learning Activity 66
PC1223-2 Eye Checks 67
PC1223-2 Learning Activity 73
PC1223-3 Abnormal Findings 74
PC1223-3 Learning Activity 81
PC1223-3 Quiz 82
PC1224-1 Oral Health Introduction 84
PC1224-1 Learning Activity 87
PC1224-2 Screening 88
PC1224-2 Learning Activity 100
PC1224-3 Prevention 101
PC1224-3 Learning Activity 104
PC1224-3 Quiz 105
PC122 Theory to Practice Activity 107
PC1221-1 Learning Activity Feedback 117
PC1221-2 Learning Activity Feedback 118
PC1221-3 Learning Activity Feedback 119
PC1221 Quiz Feedback 120

PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-1 Learning Activity Feedback 122
PC1222-2 Learning Activity Feedback 123
PC1222-3 Learning Activity Feedback 124
PC1222-4 Learning Activity Feedback 125
PC1222 Quiz Feedback 126
PC1223-1 Learning Activity Feedback 129
PC1223-2 Learning Activity Feedback 130
PC1223-3 Learning Activity Feedback 130
PC1223-3 Quiz Feedback 131
PC1224-1 Learning Activity Feedback 133
PC1224-2 Learning Activity Feedback 133
PC1224-3 Learning Activity Feedback 134
PC1224-3 Quiz Feedback 135
PC122 Theory to Practice Activity Feedback 143
PC122 Post-Session Survey 146
PC122 References 147

5PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC122 Child Health Check - Part 2: Physical Assessment
Introduction
A comprehensive child health check includes conducting routine physical assessment which will assist in the identification of risk factors for poor health outcomes.
A physical check includes inspecting the skin for rashes and infections, viewing the physical components of the ears and eyes and evaluating vision and hearing and examining and assessing oral health.
This course considers the various elements of a physical check, identifies potential issues with the skin, ears, eyes and oral environment and discusses interventions that may be taken to prevent further issues.
Learning Objectives
On completion of this course participants will be able to:
• Discuss the structure, physiology and function of the skin, ears, eyes and mouth• Describe the differences between normal healthy and unhealthy skin, ears, eyes and mouth• Provide simple prevention and treatment interventions for problems of the skin, ears, eyes and mouth• Clearly and accurately document findings on screening of the skin, ears, eyes and mouth
Topics
• The first topic introduces and explores the basic anatomy and physiology of skin, its function and somecommon skin problems we may see as part of the child health check. It reviews rashes including allergies,eczema and those associated with infectious diseases and discusses skin infections including fungal,impetigo and infected scabies.
• Topic two introduces the child health ears and hearing check and provides some information on the ear andthe reasons for checking ears and hearing routinely. It provides information on otoscopy, tympanometry andaudiometry, discusses normal and abnormal findings and provides information on intervention and followup should it be needed.
• Topic three introduces the eye, reviews the structures within the eye and discusses how the eye works. Itprovides information on screening the eyes and explains the different tests that are included in the eyecheck. The topic identifies and explains potential normal and abnormal findings and discusses sometreatment and management options.
• The final topic introduces and discusses factors that contribute to the healthy and unhealthy oralenvironment. It reviews the screening process for infants and children from 0 to 14 and strategies forensuring a healthy oral environment.
Pre and Post Session Surveys
Before you commence, we ask you to complete a quick survey to identify current knowledge base. This will provide a baseline you can refer to once you have completed this topic.
When you have completed this session, we ask you to complete another quick survey to determine if we have met your learning needs.

6 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Learning activities / Quiz
An ungraded, interactive learning activity and graded quiz is included in each module and an ungraded theory to practice activity for the course is included and must be completed in order to receive your certificate.
Certificate
Once the quiz is completed you are eligible to receive a personalised certificate which provides evidence of your training. Included on this is the average time the course takes which can be used for professional development points.
If this course is completed using the workbook it will need to be forwarded to the PaRROT team who will issue the certificate.

7PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC122 Pre-Session Survey
Before you commence this session we ask you to take a few moments to complete the pre-session survey for this topic. This will give us some indication what your learning needs might be.
At the end of this session we will also ask you to complete another survey to see how well we have met your needs.
Please indicate the degree to which you agree to the following, by ticking the box most relevant.
I am able to discuss the structure, physiology and function of the skin, ears, eyes and mouth
I can describe the differences between normal healthy and unhealthy skin, ears, eyes and mouth
I am able to provide simple prevention and treatment interventions for problems of the skin, ears, eyes and mouthI can clearly and accurately document findings on screening of the skin, ears, eyes and mouth
Stro
ngly
Agr
ee
Agre
e
Neu
tral
Dis
agre
e
Stro
ngly
Dis
agre
e

8 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-1 Introduction to Skin
Learning Objectives
On completion of this module learners will be able to:
• Describe the structure of the skin• Discuss the physiology of the skin • Describe the function of the skin• Define normal healthy and unhealthy skin
Skin
Skin is our largest organ – this diagram shows a cross section of skin. Within the structure there are various components which all work together to ensure the skin functions as it should. The outer layer is waterproof, and if intact protects the body from microscopic organisms and foreign bodies.
When the skin surface is broken, these microorganisms can enter the body and create infections within the skin, bloodstream and other structures.
The skin has three layers - the epidermis, dermis, and fat layer (also called the subcutaneous layer).
Each layer performs specific tasks.

9PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Cross section of Skin
Structure Purpose
Hair Shaft • Temperature regulation, protection, sensation
Pores • Waterproof and when undamaged prevents bacteria, viruses and foreign bodies from entering the body
• Drains oils and other impuritiesSkin surface / Sweat Pore • Drains sweat
Capillaries • Blood Flow
Pilo Erectile Muscle • Moves hair follicle if cold or frightened
Sweat Gland • Cools body
Venule / Arteriole • Blood Flow
Adipose Tissue (fat) • Cushioning and insulation
Nerve Ending • Sensitive to pain, temperature and itch
Matrix • Tissue regeneration and healing
Connective Tissue • Binds the structures together
Sebaceous Gland • Produce oil to moisturise
Epidermis • Pigmentation (colour) protection and immune response
Dermis or True Skin • Skin elasticity and body temperature regulation
Subcutaneous Tissue • Cushioning and insulation
10 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Skin Epidermis
The epidermis is the thin, tough, outer layer of the skin.
The outermost portion of the epidermis is relatively waterproof and, when undamaged, prevents most bacteria, viruses, and other foreign substances from entering the body.
The epidermis (along with other layers of the skin) also protects the internal organs, muscles, nerves, and blood vessels against trauma.
Scattered throughout the basal layer of the epidermis are cells called melanocytes, which produce the pigment melanin, one of the main contributors to skin colour.
Melanin’s primary function, however, is to filter out ultraviolet radiation from sunlight which can damage DNA, resulting in numerous harmful effects, including skin cancer.
The epidermis also contains Langerhans’ cells, which are part of the skin’s immune system.
Although these cells help detect foreign substances and defend the body against infection, they also play a role in the development of skin allergies.
Skin - Dermis
The dermis, the skin’s next layer, is a thick layer of fibrous and elastic tissue that gives the skin its flexibility and strength. The dermis contains nerve endings, sweat glands and oil glands, hair follicles, and blood vessels.
The nerve endings sense pain, touch, pressure, and temperature. Some areas of the skin contain more nerve endings than others. For example, the fingertips and toes contain many nerves and are extremely sensitive to touch.
The sweat glands produce sweat in response to heat and stress. Sweat is composed of water, salt, and other chemicals. As sweat evaporates off the skin, it helps cool the body.
The sebaceous (oil) glands secrete sebum into hair follicles. Sebum is an oil, that keeps the skin moist and soft and acts as a barrier against foreign substances.
Hair follicles provide a layer of protection and help in regulation of body temperature and facilitation of evaporation of perspiration.
Blood vessels – carry blood to the extremities.

11PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Skin – Subcutaneous
Below the dermis lies a layer of fat that helps insulate the body from heat and cold, provides protective padding, and serves as an energy storage area.
The fat is contained in living cells, called fat cells, held together by fibrous tissue.
The fat layer varies in thickness, from a fraction of an inch on the eyelids to several inches on the abdomen and buttocks in some people.
Skin
• These layers all come together to form the skin, which weighs about 11 kg and is the largest human organ.
• It protects the body from harm by preventing germs and chemicals entering the body and causing problems with the internal systems.
• Skin regulates body temperature by sweating to cool the body down and shivering to warm it up. • It assists with fluid balance and provides a means to feel the environment through the sense of touch and
feeling.
Normal healthy skin is smooth, clean, slightly oily and free from sores or wounds. Rashes, infections and lesions are all signs of skin problems.
An inflammatory response (inflammation) occurs when tissues are injured by bacteria, trauma, toxins, heat, or any other cause.
The damaged cells release chemicals which cause blood vessels to leak fluid into the tissues, resulting in swelling and redness.
If the skin is infected there is pain, swelling, redness, fever, throbbing and discharge which may be malodorous and purulent.

12 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Problems of the Skin
An important component of the child health check is to observe, report and manage problems of the skin.
Skin infections need to be treated as soon as possible to prevent further ongoing health problems from the microorganism entering into the bloodstream and causing more infection in the internal body structures.
With skin infections, one of the greatest risk is glomerulonephritis which will be discussed later in this session.
Other issues include:
• Excess oil production• Histamine responses• Injury• Viral infections• Birth marks• Metabolic issues
The following pages provide information on potential findings of a skin check.
Cradle CapCradle cap is common in small babies and is the result of excessive oil production that dries causing a scaly, crusty mass.
It is treated using oil or moisturiser. Regular gentle massaging of the baby’s head is a good way to prevent the development of cradle cap, as it disperses the oil.

13PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Nappy Rash
Nappy rash is found in the perineum region.
It is an inflammatory response to acid burns from urine (and sometimes faeces).
Nappy rash is red, raw and swollen and can be very painful and itchy.
Nappy rash can be prevented by more regular nappy changes, leaving the nappy off and using treatments such a pawpaw ointment or lanolin.
If left untreated, it can become infected or develop into a fungal rash which is very painful and itchy and will need prescription medication for treatment.
Sunburn
Sunburn is caused by overexposure to ultraviolet (UV) radiation from the sun.
This burns the skin, causing an inflammatory response that includes redness, swelling, pain and in severe cases, blistering. Injury can start within 30 minutes of exposure.
Sunburn is a common problem for young children that can be easily prevented by using UV protective shirts, sunscreens and hats when the baby or child is in the sun.
The best treatment is cool water and moisturisers and it will heal fully within 1 to 2 weeks

14 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Bruises
Bruises are common in young children and generally appear when they first start moving.
Bruises are caused when tiny blood vessels are damaged or bro-ken as the result of a blow to the skin from falling or knocking into things, and usually appear over hard surfaces like shins, knees or foreheads.
The raised area of a bump or bruise results from blood leaking from these injured blood vessels into the tissues or into the top layers of skin and as part of the body’s response to the injury.
Bruises can be black, blue, yellow or green, depending on the age of the injury. Bruises will often disappear after a couple of weeks.
When observing bruises be mindful of where they are and the story behind how they occurred as they can be the result of child abuse.
Birthmarks
Birthmarks are quite common in babies and children.
They include: • Mongolian Blue Spot which looks like a large bruise
usually over the back and buttocks of darker skinned children
• Strawberry mark which is a small raised and rough red mark
• Port wine stain which is a flatter, larger red mark often on the face and upper body
• Café au lait spot or stork marks which are a small brown spot on the forehead or neck
• Most birth marks will fade or disappear over time.

15PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Jaundice
Jaundice develops when the liver is unable to rid the body of bilirubin which is a brownish yellow substance found in bile.
When bilirubin levels are high, the skin and whites of the eyes may appear yellow (jaundice).
Jaundice may be caused by liver disease, blood disorders, or blockage of the bile ducts that allow bile to pass from the liver to the small intestine.
Too much bilirubin (hyperbilirubinaemia) in a newborn occurs when the baby’s immature liver has not started to function fully.
It can cause brain damage, hearing loss, problems with the eye muscles, physical abnormalities, and even death.
Some babies who develop jaundice may need be treated with special lights (phototherapy) which breaks down the bilirubin, or a blood transfusion to lower their bilirubin levels.
If it hasn’t cleared after 2 weeks, the baby should be reviewed by a medical officer.

16 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-1 Learning Activity
1. Which of the following statements about normal healthy skin are true?
Tick Answer
Dry
Smooth
Scaly
Lesion free
Slightly oily
2. Arrange the layers of skin in order from inner to outer
1. Epidermis 2. Subcutaneous 3. Dermis
Answer

17PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-2 Rashes
Learning Objectives
On completion of this module learners will be able to:
• Describe the various types of rashes that may be found on screening• Identify rashes associated with infectious diseases• Discuss simple prevention and treatment of rashes
Rashes - Allergies
The most common rash on children is an allergy, which is the result of an overactive immune response generated in the Langerhans’ cells in the epidermis.
These rashes are often large raised welts, wheals or hives.
They are itchy, red and swollen and are caused by contacting an allergen, an insect bite or a food allergy.
They are usually of short duration, but can be severe and may need treatment.
Rashes - Eczema
Atopic dermatitis, or eczema, is a skin condition that usually appears in early childhood and affects people with a genetic susceptibility.
Damage to the skin barrier allows moisture to escape and allergens and infection to enter, causing an inflammatory response including redness and itchiness.
Once the skin barrier is disrupted, moisture leaves the skin and it becomes dry and scaly.
Treatment for eczema includes:
• Moisturisers • Anti-inflammatory ointments – either topical corticosteroids or non-steroidal anti-inflammatory ointment • Coal tar – to reduce the itch • Dietary changes• Ultraviolet radiation therapy (phototherapy)

18 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Slapped cheek / fifths disease
Slapped cheek or fifths disease is a harmless viral infection. The rash starts on the cheeks, but quickly appears on the body and arms and legs.
A child usually presents with a defined red rash on the cheeks, abdomen or limbs, which forms after the infectious period of the virus.
Children with this rash do not need to be isolated as the infectious period passes before the rash appears.
The rash is bright red and slightly raised. It gives the characteristic look of slapped cheeks on the face, followed by a lacy appearance which gives a blotchy look to the rash.
The rash is not usually itchy.
Hand, foot and mouth disease
Hand, foot and mouth disease is a mild viral infection that begins with a slight fever, tiredness, no appetite, and sorethroat.
It develops into flat or raised red spots, which may form blisters. It affects the palms of the hands and soles of the feet.
Small red mouth sores form painful blisters, and may turn into ulcers which need to be treated.
The virus is highly contagious and is spread by coughing and sneezing and close contact that gets better in a few days without treatment.

19PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Molluscum
Molluscum is commonly found on young children.
It is a round lesion with a dimple in the middle and is filled with watery white fluid.
It can last for months and although harmless, it is highly infectious, with gross infection related to bathing.
Treatment varies but may include removal of heads, agitation of lesion etc.
Chicken Pox
Chicken pox is a viral infection that is spread through coughing, sneezing, and direct contact.
It is not a mild infection as it can cause meningitis and death – it is recommended that children are immunised against the disease when they are babies.
The rash starts with small, flat red spots which become raised and form multiple small watery filled blisters (vesicles) form over the entire body after exposure to virus.
Chicken pox is contagious for 1-2 days before the rash begins up until blisters have become scabs.
Chickenpox rash evolves through 3 stages, and a person may have examples of each type of spot at any one time. New crops of spots appear over a period of 2 to 4 days.
The rash starts with small, flat red spots. These flat red spots then become raised and very itchy and form round, fluid-filled blisters (called vesicles) against a red background.
The vesicles crust over forming dry crusty lesions that are intensely itchy.
The rash starts on the trunk (body) and then later appears on the face, arms and legs. It is unusual for the rash to affect the palms and soles.
Chickenpox spots (lesions) can sometimes be found on the eyelids and inside the mouth and the vagina.

20 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Measles
Measles is a dangerous viral disease that is spread through coughing and sneezing.
Severe cases of measles can cause brain inflammation and pneumonia which can result in brain damage and death.
The measles virus can remain latent following infection and represent as Subacfe Sclerosing Pan Encephalitis (SSPE) in adolescence which causes rapid neurological deterioration and eventually death.
It causes a high fever, cough and rash and is diagnosed usually through the Koplik (white scaly) spots found in the throat, a spreading rash and bilateral conjunctivitis.
The measles rash starts around the ears and hairline after the Koplik’s spots disappear.
After 1-2 days the rash may spread to the trunk, arms and legs and start to fade on the face.
The ‘spots’ are separate flat red areas to start with, they become raised and join together as rash spreads.
Measles rash may be slightly itchy. Measles can be prevented through child hood immunisation.
Rubella
Rubella, which is commonly known as German measles, is caused by the rubella virus.
It is caught in the same way as measles.
An infected person coughs or sneezes and so spreads droplets containing the virus, which other people breathe in and, if they are not immune, become infected with rubella.
The incubation period for Rubella is 12 to 23 days — that is the time lag between being exposed to the virus and developing a rash.
The rash is pink and flat. The spots are very small, giving the rash a fine appearance. It is similar to the measles rash but less extensive and fades more quickly. The rash starts around the hairline and affects the face and neck first. It will then spread to the body and the arms and legs.

21PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-2 Learning Activity
1. Which of the following are signs of an allergic rash? (More than one possible answer)
Risk Answer
Welts
Crusty lesions
Lesions in the mouth
Lesions with fluid filled centre
Itchy lesions
2. Which of the following can be used to manage eczema? (More than one possible answer)
Risk Answer
Moisturisers
Antibiotics
Ultraviolet radiation
Antifungal creams
Dietary changes

22 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-3 Infections
Learning Objective
On completion of this module learners will be able to:
• Describe some of the common skin infections found on screening• Discuss the importance of treating skin infections• Define impetigo• Discuss potential outcomes of untreated skin infections
Fungal Infections
Skin infections are common, but not normal in the tropics.
Fungal infections such as tinea, ring worm and ‘double skin’ can be found on most skin surfaces.
They are dry, scaly and itchy and are usually defined to a specific area.
The infections develop in hot moist environments.
Treatment options include creams such as Miconazole or Clotromazole, ointments, lotions including Selenium Sulphide (Selsun Gold) or tablets which are prescribed by Medical Officers if all else fails .
If fungal conditions are not treated they will spread and can become infected.
Scabies
Scabies is a parasitic infection that thrives in warm temperatures, where there is poor water supply,overcrowding and issues with accessing good hygiene.
They usually present as pus filled itchy blisters and sores and are found in skin folds.
Scabies is caused by a mite that burrows into the skin.An allergic reaction to the presence of the mite is responsible for the signs and symptoms.
It is usually spread by skin to skin contact, although clothing and bedding can be a source of infestation.
The mite can live away from the skin for 1-2 days or, if near a host (e.g. in bed linen) for up to 4 days.

23PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Scabies - continued
Multiple family members / householders tend to be affected and need to be treated if someone in the home has a scabies infection.
Scabies is treated with scabies cream and requires the washing of clothes and linen with hot soapy water and drying them in the sun.
All contacts of a person, especially family sharing the house will need to be treated or it will continue to spread.
If left untreated, scabies can develop into bacterial skin infections which may also infect the heart and kidneys.
Dog scabies is a different species to human scabies, and it is very unlikely that dogs play any significant role in maintaining scabies transmission in humans.
Impetigo
One of the most common infections of the skin is Impetigo also
known as school sores. They are yellow crusty lesions commonly found around the mouth and on the limbs.
Impetigo is a highly infectious bacterial skin infection that occurs in children 2 years and over. They are spread by close contact.
Impetigo needs to be treated with soap and water and antibiotics if they become infected.
Impetigo may also be found with other skin conditions such as Infected scabies; eczema; infected fungal infections; insect bites and minor abrasions.
Impetigo begin as a tiny blister (vesicle ) which is sometimes surrounded by a red, hot area that becomes filled with pus. The blisters pop easily and when they dry they form a golden crust.
Each blister is no bigger than 1-2cm but sometimes they join to form larger blisters.
It is not uncommon for infected sores to form after the blister has burst.
These sores become red, hot and painful and if left unattended can cause infections that spread to the internal structures.

24 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Streptococcus Aureus
The bacteria that causes impetigo is called Streptococcus.
Streptococci are a normal part of the environment of the mouth, skin, intestine, and upper respiratory tract of healthy people.
When a person’s health is compromised, streptococci multiply and invade body structures that do not usually contain streptococci.
Most common and most dangerous is Streptococcus Aureus or Strep A.
Strep A can cause severe infections and has high incidence in Aboriginal and Torres Strait Islander communities of Australia.
Streptococcus is known to cause infections of the brain, heart, lungs, upper respiratory tract, joints, throat, skin and kidneys.
Streptococcal infections are a major concern in some communities, and need to be treated immediately with antibiotics.
Untreated streptococci infections cause major health problems in some communities in Australia.
Acute Post Streptococcal Glomerulonephritis (APSGN) is one of themajor causes of ill health in children which leads to severe chronic disease in adults.
APSGN
Acute Post Streptococcus Glomerulonephritis (APSGN) is a common side affect of untreated skin infections. When broken down into its components it means a severe infection of the kidney which occurs following a streptococcus infection.
Acute Severe
Post After
Streptococcus Streptococcus bacteria
Glomerular Structure within the kidney
Nephritis Kidney infection
APSGN is the result of recurrent untreated streptococcal skin or throat infections.

25PaRROT Program - Child Health Check: Part 2 | A primary health care approach
APSGN – Infection Progress
The bacteria travels with blood to kidney for filtering and the Glomeruli become infected and stop working properly.
If left untreated, kidney function may become compromised and chronic kidney disease may occur.
Chronic disease causes kidneys to fail which may lead to dialysis for filtering.
Untreated Infection
Streptococcus bacteria travels in the blood
Blood reaches kidney for cleaning
Kidneys function becomes compromised
Kidney Disease Infected glomeruli stop working
Prevention
An effective way of preventing APSGN is the check the skin folds, mouth and throat carefully when doing a child health check.
If a skin problem is identified it needs to be treated appropriately and not just recorded as being checked.
The adoption of consistent screening helps identify skin problems and by taking action when problems are identified our children will have a better chance of a healthy future.
Skin Describe skin: Healthy Intact Jaundice Sores Rash
Bites Scars Bruises Itchy
Prevention is also possible if health professionals encourage personal hygiene.
Clothes and bed sheets (for whole family) should be washed in the hottest water possible and dried in sunlight.
Finger nails need to be kept cut and clean and everyone taught good hand washing techniques.
If a child has impetigo they need to avoid contact with other children until pustules cease and dry up.
The use of penicillin to treat the infection should be included in the care of the child.

26 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-3 Learning Activity
1. Which of the following skin conditions need to be treated as soon as possible?
Tick Answer
Scabies
Fungal infections
Insect bites
Sores
Impetigo

27PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221 Quiz
1. Match the type of rash with its most likely cause (5 marks)
1. Allergy 2. Hand, Foot and Mouth Disease 3. Chicken Pox 4. Eczema 5. Fifth’s Disease
Rash Cause
Hives
Dry scaly skin
Lacy rash
Lesions around mouth
Fluid filled blisters
2. Which of the following statements are incorrect? (1 marks)
Tick Answer
The family of a person with scabies needs to be treated
Streptococcus is usually a harmless natural occurring bacteria
Scabies can be found in conjunction with impetigo
Fungal infections will clear up on their own
Impetigo is a bacterial infection

28 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. APSGN could be the consequence of which of the following conditions (5 marks)
Tick Answer
Scabies
Impetigo
Eczema
Insect bites
Minor abrasions
4. Strep A is the most common and dangerous of the streptococcal infections (1 mark)
Tick Answer
True
False
5. Fungal infections are normal in the tropics so do not need to be treated (1 mark)
Tick Answer
True
False

29PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-1 Introducing Ears and Hearing
On completion of this module learners will:
• Describe the function of the ear• List 5 causes of ear problems• Discuss the importance of checking ears and hearing• Accurately document child health ear and hearing checks
The Ear
The ear is a complex organ made up of many complementary parts. It is used for both hearing and balance. The pinna is made up of cartilage which is the outer section of the ear which catches and funnels sound (which is in fact a vibration).
The sound travels into the auditory canal and hits the tympanic membrane (ear drum), which vibrates onto the three ear bones known as the incus (anvil), malleous (hammer) and stapes (stirrup) or ossicular chain.
This vibration causes fluid to move in the cochlea which sends a message to the auditory nerve to interpret the sound.
The semi-circular canals hold fluid which helps with balance and knowing where the body is in relation to gravity – the vestibular nerve carries the balance message to the brain.
The eustachian tube allows for ventilation and drainage of the middle ear. The eustachian tube is connected from the middle cavity to the back of the nose.

30 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
If the eustachian tube is free of fluid, the tympanic and ear bones are able to vibrate and hearing and balance function correctly. If it is full of fluid, hearing and balance are impaired.
It is important to check ears and hearing from birth.
Hearing loss is a common but preventable problem for children so abnormal results need to be documented and the child referred for specialist assessment. Brief intervention education on ear health is an essential com-ponent of the all hearing checks.
Rationale for assessment
Regular assessment is recommended because:
• Ear disease is a common illness in all populations • The Aboriginal and Torres Strait Islander population have the highest rates of severe and persistent ear
disease as described in medical literature, generally in rural and remote Indigenous communities.
The high rate of ear disease affects a child’s communication, speech and language development and play and learning.
If hearing loss is left undetected and untreated, it can impact heavily on social and emotional wellbeing, education, unemployment outcomes.
Causes of Ear Problems
Causes of ear and hearing problems are many. Some of these are:
• Frequent upper respiratory tract infections causing recurrent ear infections• Foreign objects in the ear canal including wax• Swimming in dirty water• Loud noises• Prop bottle feeding to sleep

31PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Ear Assessment
Otoscopy from 2 months
Audiometry from 5 years
Tympanometry from 6 months
Ear checks are included for all ages of children.
Otoscopy (Visual checks ) are conducted on all children from birth.
Tympanometry (describes normal and abnormal middle function) from 6 months and at specific ages.
Audiometry (hearing tests) are conducted from 5 years.
At ages where there are no specific checks, parents or children should be asked questions about ears and hearing.
Any concerns should be followed up and a full check conducted.
Referral
A child is referred for further review if:
• They report pain or discomfort• There is visible discharge• The tympanic membrane is perforated or bulging• The ear canal is blocked by wax or foreign body• They complain of sudden hearing loss with tinnitus and/or dizziness (urgent)• They fail the audiometry test • There are any abnormal tympanometry results

32 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Questions birth to 4 months
Questions Procedure
1 - 6 weeks
Is your baby startled by loud noises such as a loud clap?Has your baby been free of ear infections or discharge?
2 months
Do you think your baby can hear you?Has your baby been free of ear infections or discharge?
Otoscopy
4 months
Are you happy about your baby’s hearing?Does your baby turn towards sound or voices?Does your baby settle with familiar sounds or voices?Has your baby been free of ear infections or dischage?
Otoscopy
All ear and hearing checks should be proceeded with questions appropriate to the child’s age.
At 1 to 6 weeks questions include a baby’s response to loud noises. At 2 months parents and carers are asked if they think their baby can hear them.
At 4 months questions are around the parent or carers perception of their baby’s ability to hear and if the baby is responding to sounds and voices.
A history of ear infections is asked at all ages.

33PaRROT Program - Child Health Check: Part 2 | A primary health care approach
1 to 6 weeks
Startled by loud noises such as a clap?
Eye appearance
*Red eye reflex
Yes No
Normal Abnormal
Present Not present
Hearing and visionPrint name: Signature: Date:
At 1 to 6 weeks very basic checking begins.
Parents are asked if their baby jumps or wakes at a loud noise.
If answer is no, baby is referred.
2 months
• Ask the questions• Perform the otoscopy
Do you think your baby can hear you?
Otoscopy
Yes No
Normal Refer
Present Refer
Ears and hearingPrint name: Signature: Date:
Left ear:
Right ear:
Comments:
At 2 months all parents and family will know if their baby jumps or wakes at a loud noise and will have an idea if the baby can hear.
Parents are asked if they have any concerns. Otoscopy (viewing ears ) commences at 2 months of age.
The baby is referred if there are any concerns.

34 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
4 months
• Ask the questions• Perform the otoscopy
Are you concerned about your child’s hearing?
Does the baby settle with familiar sounds or voices?
Does the child look towards sound?
Otoscopy
Yes No
Healthy Refer
Healthy Refer
Ears and hearingPrint name: Signature: Date:
Left ear:
Right ear:
Comments:
Yes No
Yes No
6 and 12 months
Questions Procedure
6 months
Are you happy about your baby’s hearing?Does your baby turn towards sound or voices?Has your baby been free of ear infections or discharge?
Otoscopy andtympanometry
12 months, 18 months and 2 years
Has your child been free of ear infections or discharge in the last 6 months?Are you happy about your child’s ears and hearing?Are you happy with your child’s speech and language development?
Otoscopy andtympanometry
At 6 months questions are asked about a child’s hearing and their response to sound or voices.
From 12 months to 2 years, parents are asked about their child’s speech and language development.
Questions continue to be asked about ear infections.

35PaRROT Program - Child Health Check: Part 2 | A primary health care approach
6 months
• Ask the questions• Perform otoscopy and tympanometry
Has your child had any ear infections or ear discharge in the last 6 months?
Are you concerned about your child’s ears or hearing?
Otoscopy
Tympanometry
Yes No
Healthy Refer
Healthy Refer
Ears and hearingPrint name: Signature: Date:
Left ear:
Right ear:
Comments:
Yes No
Healthy (Type A) Refer (Type B or C)
Healthy (Type A) Refer (Type B or C)
Left ear:
Right ear:
At 6 months otoscopy and tympanometry are performed.
If a child has normal otoscopy in both ears they are reviewed at their next regular check.
From 6 months tympanometry, which measures ear canal size, if the ear drum moves, and if the middle ear is working is included in hearing checks.
If the result is abnormal in one or both ears they are referred to a Medical Officer.

36 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
12 months to 4 years
Questions Procedure
12 months, 18 months and 2 years
Has your child been free of ear infections or discharge in the last 6 months?Are you happy about your child’s ears and hearing?Are you happy with your child’s speech and language development?
Otoscopy andtympanometry
3 and 4 years
Has your child been free of ear infections or discharge in the last 12 months?Are you happy about your child’s ears and hearing?Are you happy with your child’s speech and language development?
Otoscopy andtympanometry plus audiometry for 4 year olds
From 12 months to 4 years parents and carers are asked if they are happy about their child’s ears and hearing and it their speech and language development appears to be normal.
Questions continue to be asked about ear infections in the last 6 or 12 months – depending on how frequently the child is being reviewed.
37PaRROT Program - Child Health Check: Part 2 | A primary health care approach
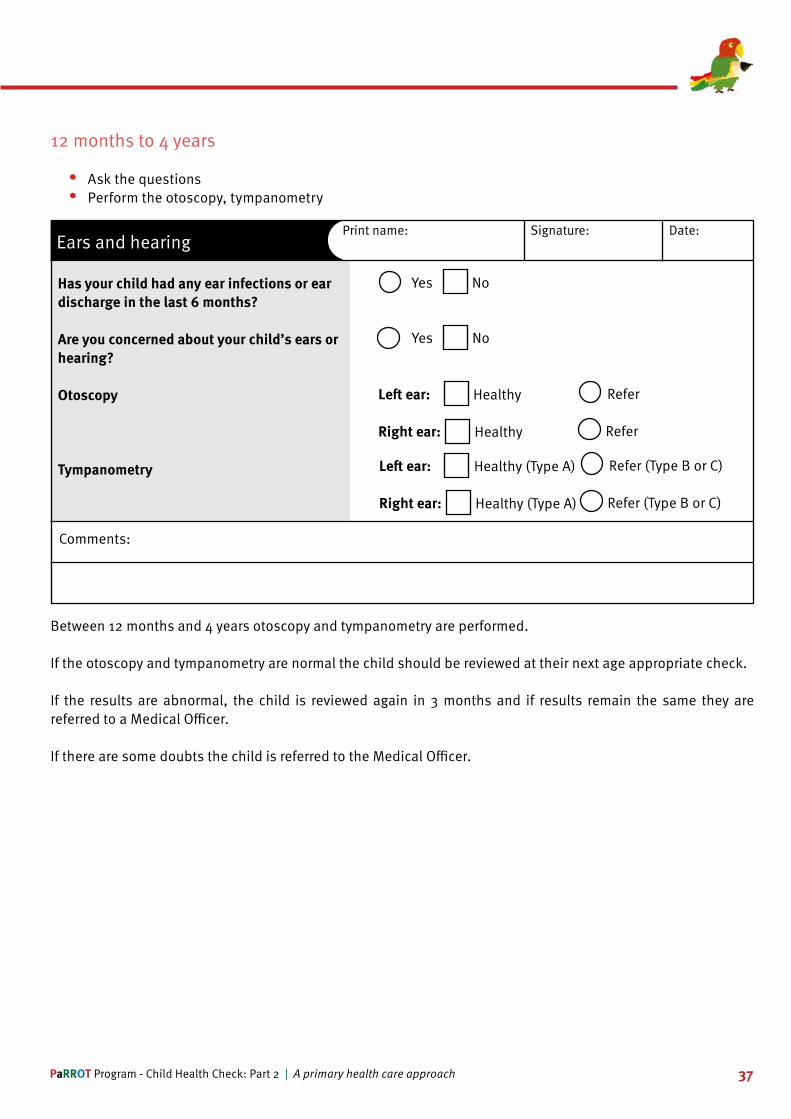
12 months to 4 years
• Ask the questions• Perform the otoscopy, tympanometry
Has your child had any ear infections or ear discharge in the last 6 months?
Are you concerned about your child’s ears or hearing?
Otoscopy
Tympanometry
Yes No
Healthy Refer
Healthy Refer
Ears and hearingPrint name: Signature: Date:
Left ear:
Right ear:
Comments:
Yes No
Healthy (Type A) Refer (Type B or C)
Healthy (Type A) Refer (Type B or C)
Left ear:
Right ear:
Between 12 months and 4 years otoscopy and tympanometry are performed.
If the otoscopy and tympanometry are normal the child should be reviewed at their next age appropriate check.
If the results are abnormal, the child is reviewed again in 3 months and if results remain the same they are referred to a Medical Officer.
If there are some doubts the child is referred to the Medical Officer.

38 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Age appropriate questions
Questions Procedure
5 and 12 years
Otoscopy, tympanometry and audiometry
6, 7, 8, 9,10, 11, 13 and 14 year olds
Family history of genetic hearing loss?History of frequent ear, nose and throat infections?Speaks in loud or monotone voice?Does not respond to name?Watches others continuously?Asks for statements to be repeated?Withdraws from group?Has learning problems in class?Has disruptive and impulsive behaviour?Teacher reports hearing difficulty?Parent / carer reports hearing difficulty?
If yes to any questions or Aboriginal or Torres Strait Islander descent then perform otoscopy, tympanometry and audiometry
From 5 years onwards, children have audiometry testing as well as otoscopy and tympanometry.
If there are no evident issues with the child’s ears or hearing, the checks only need to be done at 5 and 12 years of age.
However, if parents, carers and teachers report hearing difficulties, tests should be conducted at that time.
Although official testing may not need to be conducted, whenever a child presents for a health check a number of questions are asked.
These include:
• Family history of hearing loss and a history of ear, nose and throat infections in the child.• If the child speaks in a loud or monotone voice, if they respond to their name or asks for statements to be
repeated.• Questions about behaviour including watching others closely, withdrawing in a group, having learning
problems and displaying disruptive and impulsive behaviour are also asked.
39PaRROT Program - Child Health Check: Part 2 | A primary health care approach
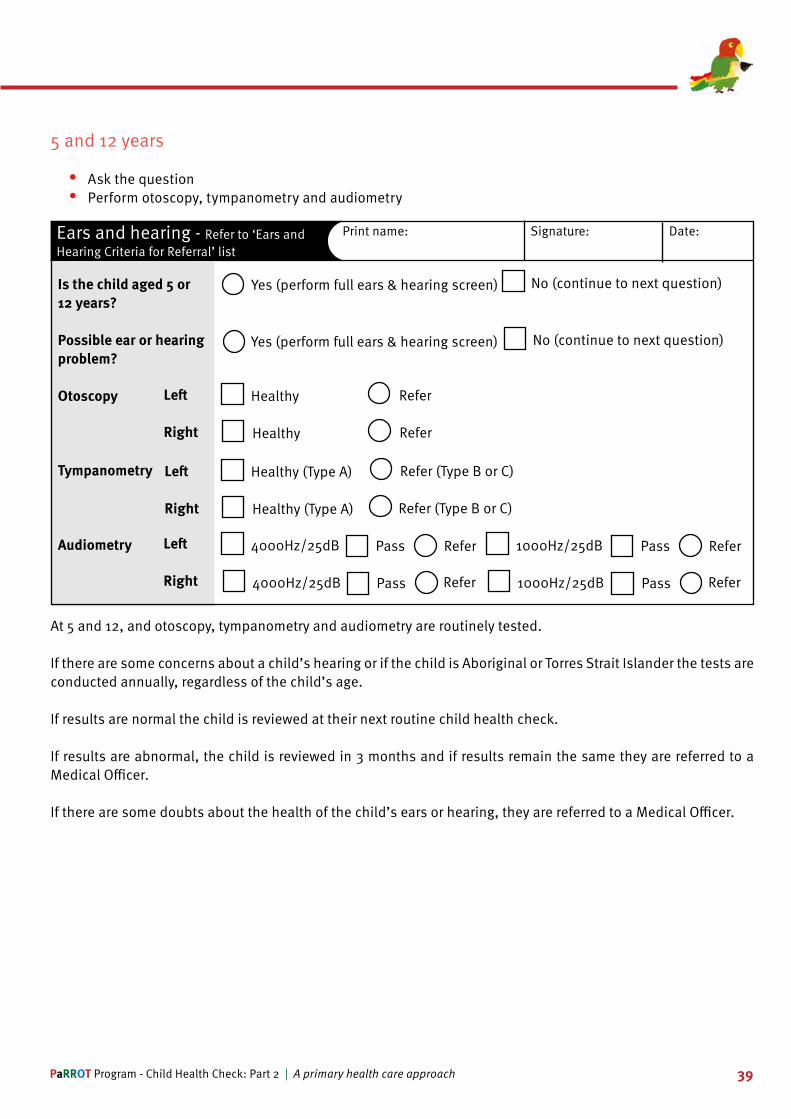
5 and 12 years
• Ask the question • Perform otoscopy, tympanometry and audiometry
Is the child aged 5 or 12 years?
Possible ear or hearing problem?
Otoscopy
Tympanometry
Audiometry
Yes (perform full ears & hearing screen) No (continue to next question)
Healthy Refer
Healthy Refer
Ears and hearing - Refer to ‘Ears and Hearing Criteria for Referral’ list
Print name: Signature: Date:
Left
Right
Yes (perform full ears & hearing screen) No (continue to next question)
Healthy (Type A) Refer (Type B or C)
Healthy (Type A) Refer (Type B or C)
Left
Right
Left
Right
4000Hz/25dB Refer
4000Hz/25dB Refer
Pass
Pass
1000Hz/25dB Refer
1000Hz/25dB Refer
Pass
Pass
At 5 and 12, and otoscopy, tympanometry and audiometry are routinely tested.
If there are some concerns about a child’s hearing or if the child is Aboriginal or Torres Strait Islander the tests are conducted annually, regardless of the child’s age.
If results are normal the child is reviewed at their next routine child health check.
If results are abnormal, the child is reviewed in 3 months and if results remain the same they are referred to a Medical Officer.
If there are some doubts about the health of the child’s ears or hearing, they are referred to a Medical Officer.

40 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-1 Learning Activity
1. Match the procedure with what it is checking for
1. Otoscopy 2. Tympanometry 3. Audiometry
Procedure Checking for
Measure canal volume
Visualise ear canal and tympanic
Test hearing

41PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-2 Otoscopy
On completion of this module learners will be able to:
• Define otoscopy• Discuss the rationale for otoscopy• Identify a normal ear canal and ear drum using Otoscopy• Recognise an abnormal ear canal and ear drum and refer for treatment• List 8 abnormalities of the ear drum and ear canal
Definition
Otoscopy is a visual examination that involves looking into the ear with an otoscope (or auriscope).
This is performed in order to examine the external auditory canal and inspection of the eardrum which provides information about what’s happening within the middle ear and other anatomical structures associated with ears, nose and throat.
Otoscopy Procedure
The Chronic Disease Guidelines outlines the procedure to perform and otoscopy. It is important to check that the battery is charged and the light works.
The correct sized ear piece for the child is chosen. Pull the child’s ear up and backwards and slowly insert the otoscope.
Always brace the hand against the child’s head to prevent the otoscope tip perforating the ear drum if any sudden movement.
The clinician must brace the otoscope before otoscopy is commenced. The two styles of holding the otoscope are pencil grip and pistol grip.
Note the colour of the canal and tympanic membrane, observe for foreign bodies, fungus, infection and discharge.
Look for bulges and holes in the tympanic membrane and debris in the canal.
Record findings.
Otoscopy is performed on all children to 5 years of age and at 12 years unless there is pain or notable discharge.
If there are problems the child should be referred to the Medical Officer or Nurse Practitioner.
The Primary Clinical Care Manual (PCCM) – Ear problems provides more information.

42 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Referral process for Otoscopy
YES Refer to MO, NP or PCCM - Ear Problems
Review in 3 months
Otoscopy result abnormalStructural defect of ear
was occlusion of ear canalforeign body
blood or dischargeinflammation or perforationfluid or pus behind ear drum
bulging eardrum
NO Proceed to Otoscopy
Otoscopy result normal Eardrum intact and free of bulgingear canal clean and free of debris
PASS
Proceed with tympanometry and audiometry
Does the child have ear pain or discharge?
Diagram 1: Referral and review process for otoscopy
Performing Otoscopy
All health professionals should perform otoscopy on children presenting to clinics.
Otoscopy is part of a comprehensive physical assessment.
The more ears are looked at, the more health professionals will see a normal ear, making it easier to identify abnormal findings.
The rest of this module provides images that may be seen when performing otoscopy.

43PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Normal Tympanic Membrane
These are normal, healthy tympanic membrane. Look for the land marks – cone of light and handle of the malleus.
Retracted Tympanic Membrane
Retracted tympanic membrane usually associated with a problem of pressure and drainage of the Eustachian tube.

44 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Foreign Body
These pictures clearly show a foreign body in the canal.
Otitis Media
These two pictures indicate otitis media also known as glue ear which is an infection of the inner ear.
45PaRROT Program - Child Health Check: Part 2 | A primary health care approach
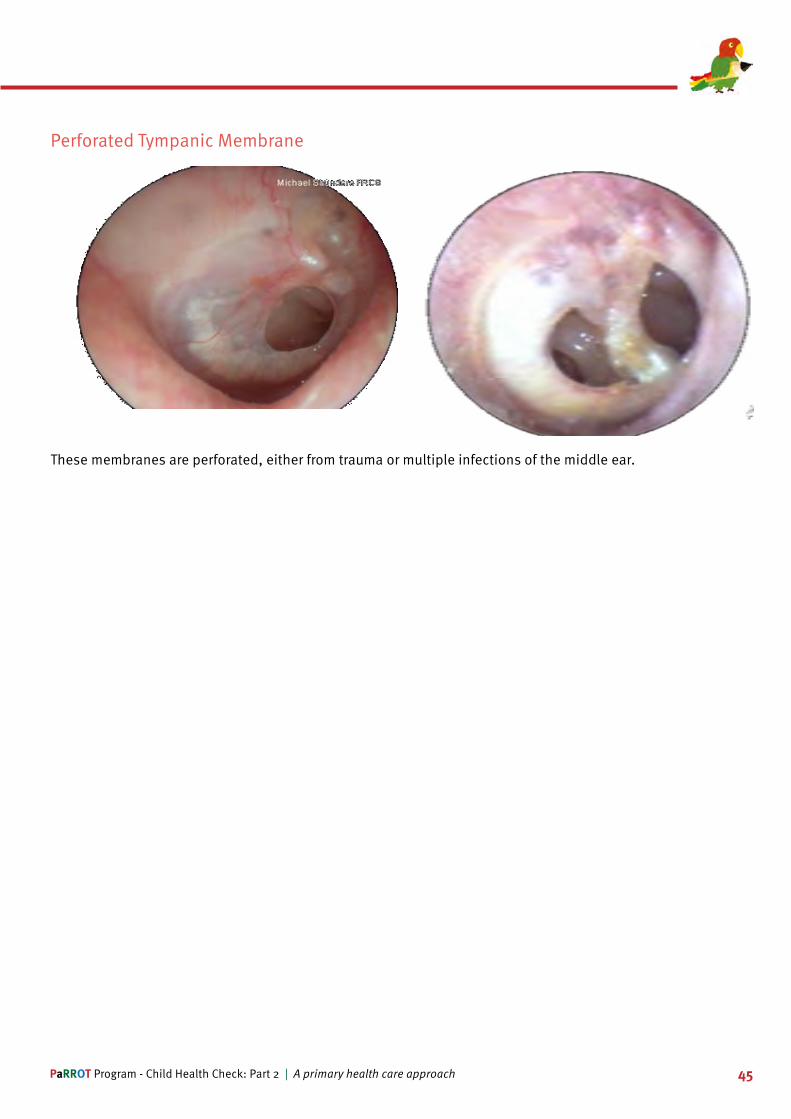
Perforated Tympanic Membrane
These membranes are perforated, either from trauma or multiple infections of the middle ear.

46 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Otitis Externa
These two illustrations are of an infection in the canal also known as Otitis Externa which is the result of excessive moisture in the canal.
Further examples of otitis externa.

47PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Bulging Tympanic
These are examples of a bulging tympanic membrane caused by a build up of fluid and pressure behind the ear drum.
Grommets
These are grommets which are inserted to assist in the drainage of pus to allow drum movement which is
essential for hearing.

48 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-2 Learning Activity
1. Match the type of problem you may see with the part of the ear anatomy it affects.
1. Ear canal 2. Ear Drum 3. Pinna 4. Middle Ear 5. Eustachian Tube
Problem Anatomy
Fungal infection
Perforation
Red, itchy and dry skin
Bulge in the ear drum
Retracted eardrum

49PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-3 Tympanometry
On completion of this module learners will be able to:
• Define tympanometry• Discuss the rationale for tympanometry• Read and interpret tympanometry graphs• Recognise abnormal results and refer for treatment• Clearly document results
Definition
• Tympanometry is not a hearing test but it is used in addition with the results of otoscopy and audiometry to assess the ear function.
• Tympanometry measures any obstruction of sound through the middle ear. • Tympanometer calculates
» The size of the ear canal. » Movement of the ear drum. » If the eustachian tube is open
Tympanometry measurements
Tympanometry measures:
• Ear canal volume (ECV) (normal between 0.2 and 2.0cm)• Middle ear pressure (normal between -150 and +100 daPa) and• Middle ear compliance or movement (normal between 0.2 and 1.4 cm)
Conducting Tympanometry
Tympanometry is performed on children from 6 months of age. It should not be performed if child has had recent surgery, pain, a perforation or if there is discharge from ears.
If there is ear discharge the child needs to be referred to the Medical Officer or Nurse Practitioner.
The Primary Clinical Care Manual (PCCM) provides information under the heading Chronic suppurative otitis media.

50 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Conducting Tympanomety
Before commencing a tympanometry, it is important to check to see if the battery is charged and the correct sized ear piece is available.
Before proceeding it is important to view the canal and ensure there is no discharge in the child’s ear.
To proceed, pull the child’s ear up and backwards, insert the Tympanometer ensuring there is a good seal.
Press the button corresponding to the ear that is being checked.
Record results and refer if needed.
There are a number of potential results from tympanometry.
These are identified as curves with peaks. The most common curves are:
• Type A – normal peak• Type B – flat line• Type C – left peak
The following pages demonstrates these peaks
Type A

51PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Type B
This type B flat line shows a low ear canal and no middle ear movement or pressure.
Otitis Media is the most common cause for this result, however, other causes may include:
Otosclerosis (stiff middle earbones due to bony growths); Badly scarred eardrum; Eardrum perforation (hole); Grommet; Ear canal blockage; Wax
Type C
This is a type C peak. It shows normal ear canal volume and middle ear movement. However it also shows a negative middle ear pressure which may be the result of a eustachian tube not draining properly.
An upper respiratory tract infection causing excessive fluid production in the sinuses.
Fluid not moving into the middle ear.

52 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-3 Learning Activity
1. Match the image to its definition
Type A Type B Type C
Type - A, B or C Definition
• Normal ear canal volume• Normal middle ear movement• Negative middle ear pressure
• No middle ear movement• No middle ear pressure
• Normal ear canal volume• Normal middle ear movement • Normal middle ear pressure

53PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-4 Audiometry
Learning Objectives
On completion of this module learners will be able to:
• Define audiometry• Discuss the rationale for conducting audiometry• Explain the findings on Audiometry• Discuss abnormal results and refer for treatment• Clearly document hearing assessment results
Definitions
• Audiometry tests a child’s ability to hear sound.• Sounds vary based on loudness (intensity) and speed of sound wave vibrations (tone).• Hearing occurs when sound waves stimulates the nerve of the inner ear and travels along nerve pathways
to the brain.• Sound intensity is measured in decibels – a whisper is 20 decibels, loud music is 80 to 120 decibels and
a jet engine is 140-180 decibels.• Tone is measured in cycles per second (cps) or hertz. Low based tones are around 50 to 60 hertz and
shrill, high pitched tones range around 10,000 hertz or higher.• Normal range of human hearing is from 20 to 20,000 hertz. Human speech is between 500 and 3,00
hertz.
Audiometry Test
• Audiometry checking follows a set sequence• The right then the left ear is tested at set and
decreasing levels of intensity (dB) and tone (Hz)• Results at each level are recorded as a pass or
fail before moving to the next level• An overall pass or fail is recorded on completion
of the test.

54 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Audiometry Test - continued
Before an audiology is performed, the procedure needs to be explained to the child.
Advise the child to raise a finger or drop a rock in a cup when they hear a noise.
Put the ear phones on, ensuring the red side is on the right ear.
Set the hertz dial to 4000Hz and the decibel level to 50dB.
Before the test begins do a sound test and practice – when the child demonstrated understanding begin the test.
Once the child indicates they are ready to do the test it commences on the right ear first.
The hertz is set to 4000Hz and the decibels to 50dB then press the sound button. Reduce the decibels to 35dB then 25dB. If the child hears the sounds down to 25dB they pass the test. If they do not hear a sound, increase the decibels by 5dB until they do.
Record this as their result on the child health check form.
Set Hertz to 2000Hz and follow the above procedure with 50dB, 35dB, then 25dB.
Set Hertz to 1000Hz and follow the same procedure with 50dB, 35dB and 25dB.
If child indicates they can hear the sounds at 4000Hz, 2000Hz and 1000Hz then they pass the test.
If they do not pass then increase by 5dB stages until the child responds.
Record the results on the Hearing Health form.
Repeat the same procedure for the left ear.
Once the right ear is tested, change over and test the left ear. Repeat the test on both ears starting at 4000Hz and 55dB.
A child passes the test if they hear 25dB in both ears and respond at 1000Hz, 2000Hz and 4000Hz for both ears.
If the child does not pass the test they need to be referred to the medical officer/audiologist for follow up.

55PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Audiometry Flow Chart
FAILaudiometry in one or both ears or B and
C type tympanometry
MO, NP or Audiologist
No further action Review next
scheduled as-sessment or in 6 months if Hx of
OM
PASSaudiometry in both ears and
A type tympanometry
Audiometry > 40dB?
Review in 3 months
PASSaudiometry in both ears and
A type tympanometry
FAILaudiometry in one or both ears or B
and C type tympanometry
Things to remember
Clinicians need to be aware that a child may pre-empt the sound if the intervals are regular. They should ensure the sound button is pressed irregularly to prevent this.
If a child doesn’t appear to hear, the positioning and sealing of the ear phones should be checked.
Children need to understand what is required of them.
The test should be conducted in a quiet (preferably sound proof) room and the child encouraged using praise. The audiometer must never go above 80dB.
Brief Intervention
Brief interventions for children for ears and hearing include ensuring the child understands the need to:
• Blow their nose• Wash their hands• Stay away from loud noises• Stay away from smoke• Swim in running water or swimming pools• Eat healthy foods• Don’t put anything in their ears

56 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-4 Learning Activity
1. What is the minimum sound intensity a child has to respond to in both ears to pass a hearing test?
Tick Answer
25 dB
10dB
30 dB
45 dB
50 dB
2. Which of the following measurements returning a positive response indicates a child is hearing tone correctly?
Tick Answer
1000 Hz
6000 Hz
4000 Hz
2000 Hz
5000 Hz

57PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222 Quiz
Please complete the gradable quiz for this session. You can complete this quiz as many times as you like until you are happy with your results.
1. Otoscopy checks canal volume
Tick Answer
True
False
2. Which of the following indicates a child may require follow up?
Tick Answer
Bulging tympanic membrane
Perforated tympanic
Canal volume between 0.2 and 2.0
Failed Audiometry at 55dB and 1000 Hz
Type A peak on Typanometry
Middle ear pressure above 100 daPa
Middle ear movement between 0.2 and 1.4

58 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. Which of the following requires urgent referral?
Tick Answer
Visible perforation
Ear canal blocked by wax
Sudden hearing loss or dizziness
Abnormal Typanometry results
Visible discharge
Failed Audiometry

59PaRROT Program - Child Health Check: Part 2 | A primary health care approach
4. Which of the following requires urgent referral?
1 2
3 4
Tick Answer
Which image shows a fungal infection?
Which image shows a retracted drum?
Which image shows a bulging tympanic?
Which image shows a perforation?

60 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-1 Introducing Eyes and Vision
On completion of this module participants will be able to:
• Identify the normal eye• Identify the different structures of the eye• Describe how the eye works
Function of the Eye
The main function of the eye is sight which includes near, far and peripheral vision. It helps to differentiate colours and receives and sends images to the brain for interpretation.
Structure of the Eye
Lacrimal GlandDucts
Pupil
ScleraIris
Lacrimal puncta Inferior Lacrimal Canal
Lacrimal Duct
Lacrimal Sac
Superior Lacrimal Canal
EyelidLacrimal Gland
The eye is made up of a number of structures that work together to produces images which help us to interpret our environment
• Eyelid – protects eye from injury and distributes lubrication over eye• Eyelashes – protect eyes from foreign bodies• Lacrimal glands – produce tears to moisturize and wash away foreign substances• Cornea – outermost layer of eye sensitive to pain• Sclera – white of the eye which gives eye its shape• Pupil – located in centre of iris which controls the amount of light entering retina• Lens – the disc that lies behind pupil, through which light and images pass. It changes shape for near and
far vision• Retina – contains rods and cones that transform light and colour impulses to brain• Iris – coloured part of the eye

61PaRROT Program - Child Health Check: Part 2 | A primary health care approach
How the Eye works
The eye works similar to a camera. Each part plays a vital role in providing clear vision.
As with the camera, if the “film” is bad in the eye (i.e. the retina), no matter how good the rest of the eye is, you will not get a good picture.
The human eye accommodates to changing lighting conditions and focuses light rays originating from various distances from the eye.

62 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Light Entry
The cornea, behaves much like a lens cover.
As the eye’s main focusing element, the cornea takes widely diverging rays of light and bends them through the pupil, the dark, round opening in the centre of the coloured iris.
The iris and pupil act like the aperture of a camera. The lens acts like the lens in a camera, helping to focus light to the back of the eye.
63PaRROT Program - Child Health Check: Part 2 | A primary health care approach
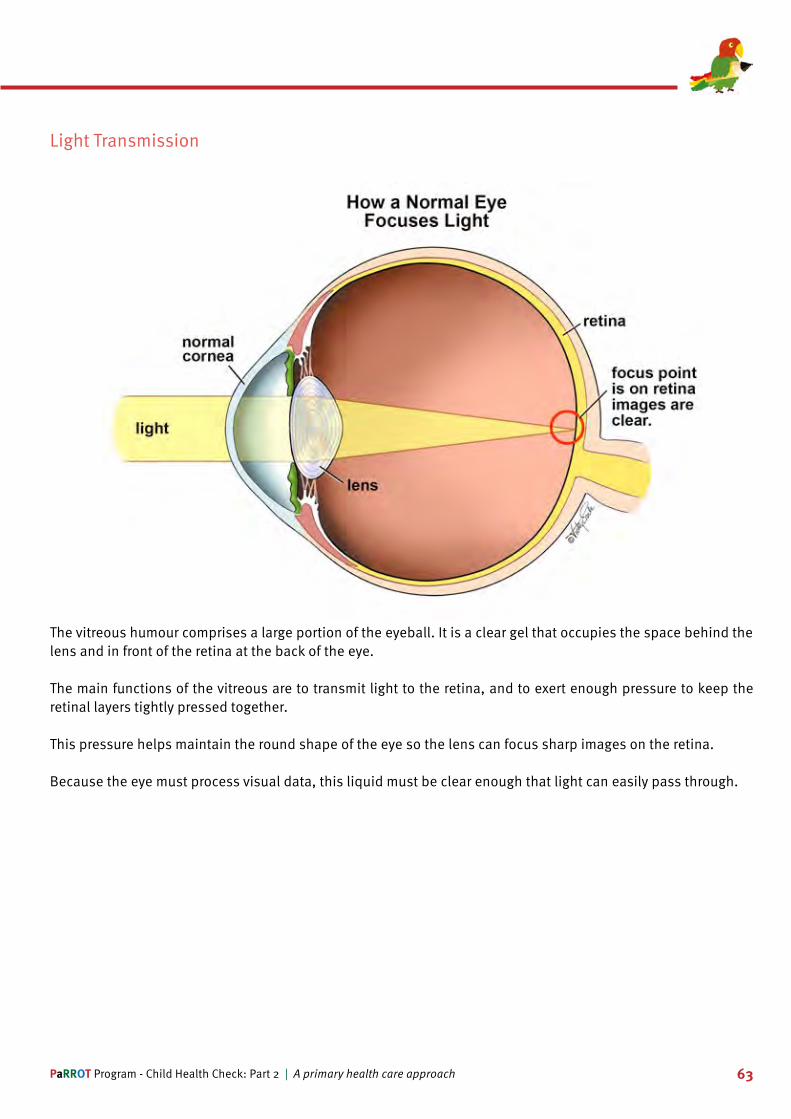
Light Transmission
The vitreous humour comprises a large portion of the eyeball. It is a clear gel that occupies the space behind the lens and in front of the retina at the back of the eye.
The main functions of the vitreous are to transmit light to the retina, and to exert enough pressure to keep the retinal layers tightly pressed together.
This pressure helps maintain the round shape of the eye so the lens can focus sharp images on the retina.
Because the eye must process visual data, this liquid must be clear enough that light can easily pass through.

64 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Light Receptors
The very back of the eye is lined with a layer called the retina which acts like the film of the camera.
The retina is a membrane containing photoreceptor nerve cells that change the light rays into electrical impulses.
These impulses are sent to the optic nerve (which is tested as part of the red eye reflex).
The centre 10% of the retina is called the macula. This is responsible for sharp and reading vision.
The peripheral retina is responsible for the peripheral vision.

65PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Light to Image
The electrical impulses formed by the light rays travel through the optic nerve to the brain.
The lateral geniculate nucleus (LGN) is the primary relay centre for visual information received from the retina.
The neurons of the LGN send the stimuli through to the visual cortex of the brain where where visual information is processed and turned into an image.
Both hemispheres of the brain contain a visual cortex and a LGN.
The left visual cortex receives signals from the right visual field and the right visual cortex from the left visual field.

66 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-1 Learning Activity
1. List in order the structures of the eye in which light travels to produce an image.
Cornea | Lens | Vitreous | Pupil | Optic Nerve | Retina
Order Answer
1
2
3
4
5
6
2. Now match the structure of the eye with its role in the process of creating an image from light rays.
Cornea | Lens | Vitreous | Pupil | Optic Nerve | Retina
Structure Function
Controls the amount of light going through the eye
Takes wide diverging rays and bends them
Transmits light to the retina
Focuses light to the back of the eye
Transfers electrical impulses to the brain
Changes light rays into electrical impulses

67PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-2 Eye Checks
On completion of this module participants will be able to:
• Undertake a reliable eye assessment at relevant ages and stages of development• List the types of eye tests and describe the procedure• Describe near and far sightedness• Define visual acuity
Eyes and Vision
Checking a child’s eyes and vision commences at birth and continues until they are 14 years old.
Checks include observing the eye, red eye reflex, corneal light reflex, cover tests and visual acuity.
Parents, teachers and children should always be asked if there are any concerns before routine checks are conducted.
If concerns are reported, extra checks should be conducted, recorded and the child referred as needed.
Screening 6 weeks, 2 and 4 months
Eye and vision checks at 6 weeks, 2 and 4 months involve inspecting the eye for symmetry, the presence of infection or lesions, conjunctiva colour and movement and a red eye reflex.
Print Name: Signature: Date:Eyes and Vision
Eye Appearance
*Red Eye reflex
Normal Abnormal
Present Not present

68 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Appearance
The eye is checked for evidence of deformity and disease.
Both eyes should move evenly and freely with symmetrical pupils (shape and size) which constrict and dilate when light is shone in the eyes.
The conjunctiva should be white and free of discharge, lids and lashes clear of lesions and discharge and the iris uniformly shaped and free of lesions.

69PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Red eye reflex
Normal Response Problem
Problem Problem
The red eye reflex test is usually performed by a medical officer or trained child health nurse.
While the child is looking at a distant object, the light of an ophthalmoscope is directed at the pupil from 30 centimetres away.
A red reflex from the retina should be observed.
An uneven response is cause for concern and the child needs to be referred to a specialist.
Screening 6 months
At 6 months the corneal light reflex is added to the well child health eye check.
Parents are asked parents if they have any concerns and test the child to see whether they fixate and follow an object with their eyes.
Red eye and corneal light reflex should be equal in both eyes.
Print Name: Signature: Date:Eyes and vision
Child fixates and follows an object with eyes at the following distance
*Red eye reflex
Corneal light reflex equal
30cm (near) Yes No
6m (distant) Yes No
Present Not present Yes No

70 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Corneal Light Reflex
To check the corneal light reflex a bright light is held centrally but level with the eyes at about 30 cm from the eyes. Light will reflect in both eyes. If both eyes are properly fixing, the reflection should fall centrally on each cornea. If there is a squint, the light will not fall centrally on the corneas.
This test is a preliminary step to the cover test which better identifies squints and other eye problems.
Screening 12 to 18 months
At 12 months, Parents are still asked questions about any concerns and the red eye and corneal light reflex is still checked.
The fixation (focus) and following of eyes are tested for near and distant objects.
Print Name: Signature: Date:Eyes and vision
Child fixates and follows an object with eyes at the following distance
*Red eye reflex
Corneal light reflex equal
30cm (near) Yes No
6m (distant) Yes No
Present Not present Yes No

71PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Following near and distant objects
To check if a child is following near and distant objects an object is held at arms length then moved away from
them (other side of room).
The child is observed to see if they follow the object.
Parents can also be asked if they noticed if their child focuses on things in the distance and nearby - children who do not focus close or distant objects may have vision problems.
Far and Short sightedness
Children who are far sighted have trouble focusing on objects that are close by as the image falls be-yond the optic nerve.
Those who are short sighted have problems seeing things in the distance as the image falls short of the optic nerve.
Screening 5 - 14 years
From 5 to 14 years, vision is only checked if problems are reported EXCEPT at 6 and 12 years when a child has a full check including cover tests and visual acuity.
Print Name: Signature: Date:Eyes and vision - Refer to ‘Vision Criteria for Referral’ list
Is the child aged 6 or 12 years?
Possibly eye or vision problem?
Cover test Left: Right:
Visual acuity (with prescription glasses if worn)
Yes (perform full eye and vision screen) No (continue to next question)
Yes (perform full eye and vision screen) No (continue to next question)
Near Movement No movement Distant Movement No movement Near Movement No movement Distant Movement No movement Left / Right /

72 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Near and Far Cover Tests
Near and far cover tests are conducted by asking a child to focus on a near (30 cm away) object and on a distant (more than 6 metres away).
The tests are always started on the right eye first.
The child is asked to fixate on the distant object first and encouraged to keep the eye still. The right eye is covered and the left observed for movement.
Any corrective movement of the left eye may suggest a squint.
The right eye is then uncovered and observed for movement as well – any movement of either eye when the right eye is uncovered may also suggest a squint.
The test is repeated on the left eye using the distant object then a near object.
Visual Acuity
Vision is dependent on how sharp the retina can focus an image and how well the brain can interpret the information. Visual acuity is the most common clinical measurement for assessing clarity of vision which is checked using a Snellen or Tumbling E chart.
It determines how clearly a child can identify black symbols on a white background at a certain distance.
Visual acuity is checked at 6 and 12 years only, unless a teacher, parent or child expresses concerns about vision.
To check visual acuity the child stands 6 metres (3 metres if using mirror and reverse chart) away from the eye chart.
The left eye is fully occluded and the child asked to read the letters or indicate the way the E is facing using 3 fingers, with their right eye.
The check is then repeated by occluding the right eye and reading using the left eye.
Each line has a number that refers to the distance in metres from which the child can clearly see the row of letters.
The results are recorded as ‘the line number the child can read clearly’ /6 (the distance to the chart).
The second number is the distance from which most children with normal vision would be able to see the letters clearly.
By 7 years old all children should be 6/6 in both eyes. If a child’s result is not 6/6 they should be referred for follow up.

73PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-2 Learning Activity
1. Which of the following are included in the 12 month old eye check? (More than one answer)
Tick Answer
Visual acuity
Red eye reflex
Corneal light reflex
Near cover test
Far cover test

74 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-3 Abnormal Findings
On completion of this module participants will be able to:
• Recognise and describe potential problems and appearance of the eye• Define Strabismus and amblyopia• Recognise abnormal results and refer for treatment
Appearance of the Eye
Children’s eyes that are of no concern move evenly and freely with symmetrical pupils (shape and size) which constrict and dilate when light is shone in the eyes. The conjunctiva should be white and free of discharge, lids and lashes clear of lesions and discharge and the iris uniformly shaped and free of lesions.
Ptosis or drooping eyelid is caused by weakness of the muscles that raise the eyes, damage to the nerves that control the muscles or looseness of the skin on the upper eyelid.
In children this is usually caused by a congenital abnormality, injury or disease.

75PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Infections of the Eye
Herpes simplex causes ocular herpes and cold sores. Usually the cornea is infected and in most cases just in the superficial layer (epithelial keratitis).
Infection of the deeper layers (stromal keratitis) is more serious as it may cause scarring of the cornea.
A minor and temporary inflammation of the conjunctiva (conjunctivitis), eyelids (blepharitis) and deeper structures such as the retina or iris may also occur with active infection, often at the same time as the cornea is infected.
Blepharitis is usually caused by seborrhoeic dermatitis, a bacterial or viral infection or allergies.
The eyelids become red, swollen, itchy, burning and may be dry and crusty.
Treatment involves bathing the eyes daily and applying ointments and creams to treat infection.
Conjunctivitis
Viral conjunctivitis Bacterial conjunctivitis
Conjunctivitis could be either a viral or bacterial infection or the result of allergies affecting the conjunctiva. It causes redness in the sclera, stickiness, discomfort and light sensitivity.
Viral Conjunctivitis is very contagious, so children should be avoid close contact with others while they have an infection.
Bacterial conjunctivitis may require antibiotic treatment so a medical officer should be consulted and allergic conjunctivitis can be treated by anti-histamines.

76 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Infections of the Eye - continued
A stye is a small lump that occurs on the eyelid. It develops when an oil gland becomes blocked.
Styes can become infected and quite painful. They can be treated using warm compresses, gentle massage and antibiotic drops, ointment or tablets if it becomes infected.
A nasolacrimal duct cyst occurs when the tear duct becomes blocked - usually the result of a congenital abnormality.
Treatment includes gentle daily massages and in some cases surgicalintervention to open the duct.

77PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Conditions of the Eye
Trachoma is caused by a bacterial infection (Chlamydia trachomatis) of the eye.
It is spread through direct contact with infected eye, nose or throat secretions or contact with contaminated objects like towels and clothes.
In Australian remote communities the infection is carried by flies.
Trachoma starts out as an infection that causes a cloudy cornea, discharge, swelling of the lymph nodes, swollen eyelids and turned-in eyelashes.
Treatment with antibiotics is essential if complications such as scarring, permanent eyelid damage and blindness are to be prevented.
Glaucoma is the result of increased pressure in the eye which damages the optic nerve.
Childhood glaucoma is the result of abnormal development of the eye drainage system or disorders of the body of the eye that may or may not be genetic.
Paediatric glaucoma usually requires surgery early in the baby’s life – if left untreated permanent vision loss will occur.

78 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Strabismus
Strabismus is a condition in which the eyes are not properly aligned with each other.
It typically involves a lack of coordination between the extra ocular muscles that prevents bringing the gaze of each eye to the same point in space.
This prevents proper binocular vision, which may affect depth perception.
Strabismus can be either a disorder of the brain coordinating the eyes or a disorder of one or more muscles of the eye.
Strabismus is most commonly described by the direction of the eye misalignment; common types of strabismus are esotropia, exotropia, hypotropia, and hypertropia.
Esotropia is inward turning of the eyes (crossed eyes). Types of esotropia include infantile esotropia, accommodative esotropia, and sixth nerve palsy.
Exotropia is the term used to describe outward turning of the eyes (wall-eyed)
Esotropia – abnormal eye turned in Exotropia – abnormal eye turned out
The terms hypertropia and hypotropia are used to describe vertical misalignment. Hypertropia is an abnormal eye higher than the normal eye.
Hypotropia is when the abnormal eye is lower than the normal eye.
Hypertropia - abnormal eye higher than the normal one
Hypotropia – abnormal eye is lower than normal eye

79PaRROT Program - Child Health Check: Part 2 | A primary health care approach
False / Psuedo Squint
A false or pseudo squint can be mistaken for strabismus. The eye appears turned because of a broad bridge of the nose. In this picture strabismus can be ruled out as the corneal light reflexes fall evenly on the eye.
Sometimes young babies may appear to have a squint as a result of immature eye muscles.
This usually disappears by 6 months.
Broad bridge of nose Immature eye muscles
Latent Squint
A latent squint is not a true strabismus. It occurs in some children who squint when they are tired.
The only way to determine this is to conduct a cover test when the child is not tired to exclude strabismus.
Occurs if child is tired Can be excluded with a cover test

80 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Amblyopia
Amblyopia also known as a lazy eye is a vision development disorder that may be the result of
• An undiagnosed or poorly treated strabismus (squint).• Deprivation of visual experience caused by a blockage on the visual pathway e.g. child hood cataracts.• Refractive problems (poor eyesight due to poor focusing of light through the lens) e.g. one eye is more
near or farsighted than the other.
Amblyopia occurs when the brain stops forming an image from one eye to maximise the vision in the other.
This may lead to a perceptive “blindness” (blindness not caused by structural problems) and poor depth perception.
Amblyopia is diagnosed by conducting a cover test, if a child fails a cover test, it is essential they are referred for specialist follow up, in order to prevent long term vision problems.
Lazy eye May lead to poor depth perception
Treating Squints
Early detection and treatment of squints impacts on the chances of successful intervention and prevention of long term complications including amblyopia.
Treatment of squints involves patching, glasses, exercises, eye drops, or surgery.
Success of the treatment depends on the child’s compliance.

81PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-3 Learning Activity
1. Match the eye abnormality with its definition
1. Conjunctivitis 2. Blepharitis 3. Stye 4. Amblyopia 5. Strabismus
Abnormality Definition
Vision development disorder
Eyes not properly aligned
Small infected lump on eyelid
Infection of the conjunctiva
Swollen, red, itchy eyelid

82 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-3 Quiz
1. Amblyopia and Strabismus are the same thing (1 mark)
Tick Choice
True
False
2. Match the test with what it is checking for (5 Marks)
1. Cover test 2. Corneal light reflex 3. Visual acuity 4. Red eye reflex 5. Eye inspection
Abnormality Definition
Amblyopia
Strabismus
Retinal function
Ability to see from certain distances
Conjunctivitis

83PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. Which of the following requires follow up by a specialist? (More than one answer) (4 marks)
Tick Choice
Stye
Amblyopia
Strabismus
Blepharitis
Conjunctivitis
4. Which of the following conditions has the potential to lead to vision loss or blindness in one or both eyes? (More than one answer) (4 marks)
Tick Choice
Nasolacrimal duct cyst
Glaucoma
Trachoma
Untreated Strabismus
Amblyopia

84 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-1 Oral Health Introduction
Learning Objectives
On completion of this module learners will be able to:
• Discuss the importance of oral health• Define plaque and causes of tooth decay • Discuss influences of diet on oral health• Identify the foods that are most likely to harm the oral environment.
Oral Environment
The health of teeth is dependent on the environment of the mouth.
Teeth will remain healthy as long as they are in contact with fluoride from toothpaste or water, are flushed by a good flow and quantity of saliva and there is sufficient calcium in the diet to ensure they remain strong.
Teeth become weaker when they are not exposed to fluoride, the quality and amount of saliva is reduced, there is insufficient calcium and water and a high sugar content in diet, there is poor or no dental care.
Plaque is made up of germs (bacteria) and food debris. Everyone has plaque but some people have “worse” bacteria than others.
Plaque bacteria is only found in the mouth – brushing teeth reduces the build up of plaque, but it continues to develop again soon after.
It takes 12-24hrs for the full plaque amount to return.
When a baby is born there is no bacteria in their mouth, a baby gets their bacteria from the mouths of their parents.
If the parents have poor oral health they will pass on bad bacteria to their child.
Sucking dummies or milk bottle teats to “clean” them is a common root of bacteria transfer so this practice needs to be strongly discouraged.

85PaRROT Program - Child Health Check: Part 2 | A primary health care approach
A poor oral environment is the culmination of a high sugar diet and plaque bacteria in the mouth building up over time and affecting a susceptible tooth.
Plaque Bacteria
Susceptible tooth
Time
High sugary diet
Plaque Bacteria
Susceptible tooth
Time
High sugary diet
Plaque Bacteria
Susceptible tooth
Time
High sugary diet
The combination of sugary drinks and food, if not cleaned from the teeth results in the development of plaque bacteria. This produces acid which attacks the teeth causing tooth decay.
Sugary drinks and food
Plaque bacteria
Makes acid which attacks the teeth
Influences of Diet
Plaque bacteria reproduces in sugar that’s left on your teeth after food or drinks are consumed.
Sugar can come from fruit, milk, lollies, biscuits and bread – in fact any food group could have a sugar content.
The more these foods are eaten, without cleaning the teeth after, the more the bacteria produces the acid which causes decay.

86 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Liquid Sugar
The worst sugars are liquid and sticky sugars which get into all the small places where its harder to clean.
Fluids containing sugar include: soft drink; cordial; fruit juice; sports drinks; Ribena; sweetened tea/coffee; flavoured milk.
Sticky Sugar
Sticky sugars which come from confectionary like roll-ups, muesli bars, chewing gum, lollies and toffee all adhere to the tooth surface and are harder to clean off.
If left on the tooth surface they will begin to damage the enamel which results in tooth decay.
Soft Drinks
Soft drinks also cause tooth decay.
• Full sugar soft drink contains sugar and acid which leads to tooth decay.• Diet soft drink contains acid which leads to tooth decay.
Plain water has no sugar or acid which leads to healthy intact teeth.
It is recommended that water instead of soft drink is consumed.

87PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-1 Learning Activity
1. Which of the following factors contribute to a healthy oral environment?
Tick Answer
Good water supply
Access to fluoride
High sugar diet
Dental check-ups every 2 years
Good oral hygiene

88 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-2 Screening
Learning Objectives
On completion of this module learners will be able to:
• Discuss the oral health screening process • Conduct oral health screening • Identify degrees of tooth decay• Make recommendations to reverse tooth decay
Introduction
Checking oral health on every child health check is essential.
Poor dental health is an extremely common problem amongst children.
There is an association between periodontal disease and the risk of heart disease, coronary artery disease, inadequate nutrition and otitis media.
There is also an association between periodontal disease and diabetes, obesity and diets high in sugar and fatInfections and decay may result in the loss of teeth which impacts on nutrition, psycho-social health and life outcomes.
If poor oral health practices are present, parents and carers should to be educated and supported to make good choices.

89PaRROT Program - Child Health Check: Part 2 | A primary health care approach
0-12 months
Prior to commencing an oral health check, parents, carers are asked a series of questions.
At 6 months the parents are asked if the child has any teeth and if they are cleaning the teeth and gums.
The baby’s teeth, gums, cheeks and tongue are visually checked.
Questions Intervention
6 months
Does the child have any teeth?Does the parent clean the child’s teeth and gums?
Brief Intervention
Are teeth present?
Do you clean your child’s teeth and gums?
Yes No
Oral HealthPrint name: Signature: Date:
Yes No

90 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
12 months - 4 years
Questions Intervention
12 months, 18 months, 2,3 and 4 years
Does the child have any teeth?Does the parent clean the child’s teeth and gums using a small soft toothbrush with a pea sized amount of low fluoride toothpaste twice a day?
Brief InterventionVisual Oral Check
Are teeth present?
Do you clean the child’s teeth and gums using a small soft toothbrush with a pea sized amount of low fluoride toothpastetwice a day?
Oral examination of teeth
Oral examination of gums
Yes No
Oral HealthPrint name: Signature: Date:
Yes No
Healthy Decay Malalignment No exam
Healthy Bleeding Swelling No exam
Between 12 months and 4 years parents are asked if they are cleaning their child’s teeth with a toothbrush and toothpaste.
The child’s teeth, gums, cheeks and tongue are checked. If there are any concerns the child should be referred to a medical officer or dentist.

91PaRROT Program - Child Health Check: Part 2 | A primary health care approach
5 to 14 years
Questions Intervention
5 to 14 years
How often do you brush your teeth?Have you had any toothache or bleeding gums in the last 4 weeks?Have you had a dental checkup in the last 12 months?
Brief InterventionVisual Oral Check
How often do you brush your teeth?
Have you had any toothache or bleeding gums in the last 4 weeks?
Have you had a dental checkup in the last 12 months?
Oral examination of teeth
Oral examination of gums
Twice daily Once daily
Oral HealthPrint name: Signature: Date:
Yes No
Healthy Decay Malalignment No exam
Healthy Bleeding Swelling No exam
Occasionally Never
Yes No
Children aged between 5 and 14 are asked if they brush their teeth, if so how often, if they have any pain or bleeding and if they have had a dental check in the past year.
The child’s teeth, gums, cheeks and tongue are checked. If there are any concerns the child should be referred to a medical officer or dentist.
Screening
Parents/carers or children should be asked questions about their dental hygiene and nutrition practices prior to examining the teeth and gums.
Oral health checks involve a full mouth check including:
• Cheeks for grazes, ulcers and infections• Teeth for plaque and decay • Gums for boils and gingivitis• Tongue for ridges, ulcers and other abnormalities
Education about healthy habits, brushing and flossing daily is an integral part of the check.

92 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Checking the mouth
To check the mouth good lighting or a torch is essential. A gloved hand and tongue depressor makes the process easier.
The child is asked to open their mouth, and with teeth clenched and lips parted, the outside of the front teeth is checked.
The child is then asked to open mouth fully so the molars, gums, cheeks and gum can be checked.
Tooth Decay
Tooth decay is one of the most common problems with oral health.
It is a consequence of bottle feeding that continues into toddlerhood, excessive juice intake especially with pop-top bottles and excessive consumption of soft drinks – full sugar and diet.
Poor dental hygiene and a poor diet with high sweet and sugar intake causes plaque build up which may result in decay.
Healthy Teeth
Healthy teeth are clean, unstained and have no holes or cavities.

93PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Early Decay - Frosting
Early decay or frosting is indicated by discolouration and spots on the tooth enamel.
It is reversible with improved oral health and decreasing exposure to sugars.
Without change decay will continue, holes will form and teeth will need fillings or, if the decay is bad enough, require extraction.
Small hole already formed
Active Decay
Early decay or frosting is indicated by discolouration and spots on the tooth enamel.
It is reversible with improved oral health and decreasing exposure to sugars.
Without change decay will continue, holes will form and teeth will need fillings or, if the decay is bad enough, require extraction.

94 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Severe Active Decay
Severe active decay leads to loss of tooth structure and is not reversible.
All teeth may need to be extracted which will cause difficulty with speech and eating.
If habits do not change NOW this child will have severe dental problems into adult life.
Less Active Decay
If oral health habits change early enough, the damage to the tooth can be halted. In this image damage has occurred but is now less active.
The darker (black) colour is inactive decay and the lighter brown areas are more active meaning decay has recommenced.

95PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Misaligned Teeth
Misaligned teeth have both cosmetic and health impacts.
Cross bite is when the upper front teeth should be in-front of the lower teeth – usually caused by lower jaw anat-omy which can be corrected by orthodontic intervention.
Crowding occurs when there is insufficient space in the jaw- resulting in overlapping or crooked teeth.
Misaligned teeth can impact on a child’s ability to chew and if very crowded can cause problems with teeth cleaning and potential decay.

96 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Misaligned Teeth - continued
The above images show misalignment as a result of thumb sucking.
This space is caused from thumb sucking which is quite normal for young children.
It should be stopped by the time the child begins to lose their baby teeth.
Healthy Gums
When checking for oral health it is important to take note of the gums.
Healthy gums are pink or coral coloured and have ridges above the teeth.
The top of the tooth is clean and free of plaque and the gums are not puffy or red.
The attachment to the tooth is firm and the gum is clean.

97PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Unhealthy Gums
This image shows unhealthy gums. There is plaque at the top of the teeth.
Between the teeth are red puffy sections which will build easily when cleaned with a toothbrush.
There are no clear ridges above each tooth and the teeth are likely to be loose.
It is very easy to return these gums to good health by cleaning teeth and gums with a soft toothbrush, using a mouthwash and rinsing after eating or drinking.
Floss should also be used daily.
Causes of Unhealthy Gums
Gums become unhealthy if a person is brushing too roughly or they are using a hard or medium toothbrush.
They may not be brushing near the gums which results in build-up of plaque which causes gum infections.
When infected gums are touched with a toothbrush bleeding occurs.
This can be fixed by regularly brushing the gums gently to remove the plaque and reversing the infection.

98 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Inflamed Gums
Inflamed gums indicate infection.
They become inflamed at the base of the teeth as a result of plaque build up – if the infection is not managed, it spreads to the whole gum.
Gums will be sensitive and will bleed when brushing teeth. Correcting brushing technique, flossing and using mouthwash are all good ways to manage gum infections.
Gum Boils and Abscesses
Gum boils and abscesses occur as a result of poor oral hygiene – the decay moves beyond the tooth into the gum causing infection.
Gum boils can be very painful and may need antibiotic treatment.
Tooth decay needs to be halted by practising good hygiene, if this is not possible teeth may need to be extracted.

99PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Ulcers and Lumps
Ulcers and lumps which can be found on gums, cheeks and lips may be caused by a number of different conditions including:
Herpes; warts; biting; burns; poor nutrition; hand foot and mouth and other diseases.
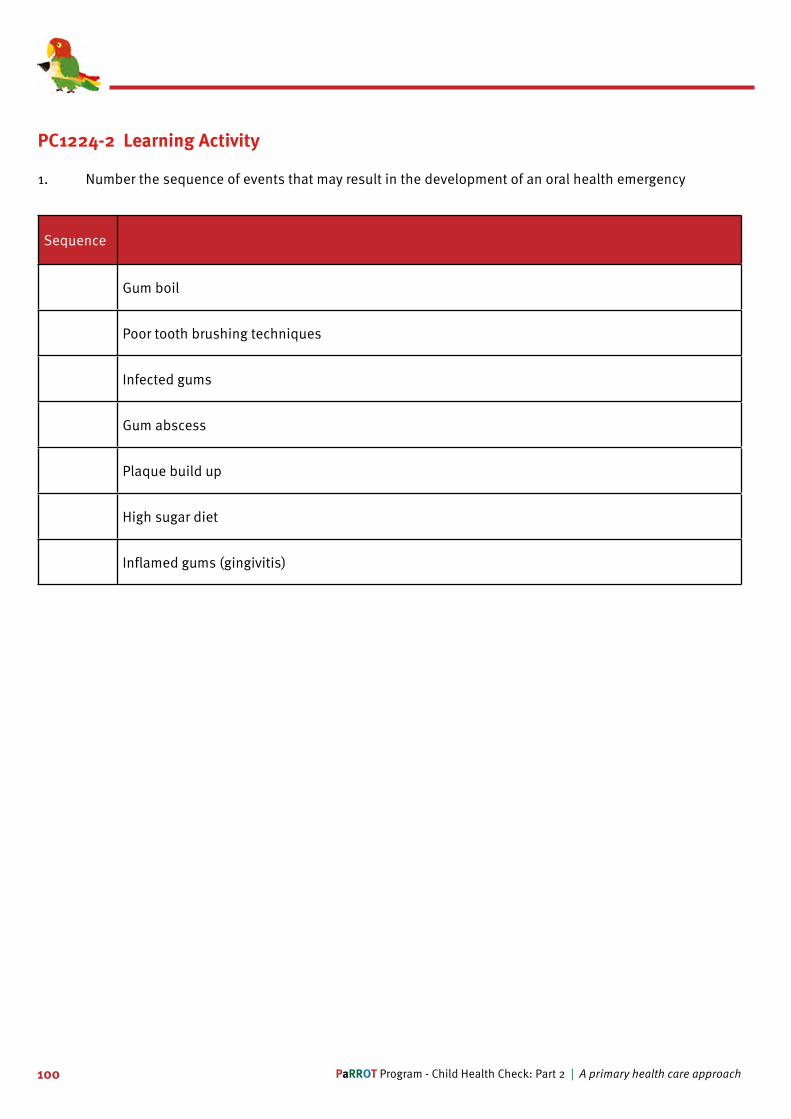
100 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-2 Learning Activity
1. Number the sequence of events that may result in the development of an oral health emergency
Sequence
Gum boil
Poor tooth brushing techniques
Infected gums
Gum abscess
Plaque build up
High sugar diet
Inflamed gums (gingivitis)

101PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-3 Prevention
Learning Objectives
On completion of this module learners will be able to:
• Describe good oral health habits• Discuss ways to maintain a healthy oral health environment• Explain process of teeth brushing and flossing for adults and children• Discuss the benefits of regular dental checks• Identify what issues require referral and to whom.
Good Oral Health Habits
Good oral health is the result of drinking plenty of water and milk and eating fruit and vegetables. Brushing teeth twice daily with a soft, well maintained toothbrush, daily flossing and regular visits to the dentist will ensure oral hygiene is maintained.
Teeth Cleaning
Good oral hygiene includes regular teeth cleaning starting in infancy.
Up to 12 months of age teeth should be wiped with a clean, soft cloth after eating or drinking.
From 12 months of age children’s teeth need to be cleaned twice a day.
Parents should clean and floss children’s teeth up until they are 8 years old. Flossing needs to be done daily, preferably at night.
Brushing Teeth
The best way to keep the mouth healthy is for adults and children to brush their teeth twice a day.
Children under 8 need adult help with teeth brushing as it is difficult for them to do it correctly.
Children over 8 are able to brush their teeth but need to be supervised to ensure they do it correctly.
A thorough brushing should take two to three minutes to complete, less than that is less then optimal.
Toothbrushes
Teeth should be brushed with a soft toothbrush – not medium or hard as they do not clean as well as they are not flexible and they can cause damage to the teeth enamel and gums. Toothbrushes with smaller heads are more able to reach the back of the mouth.

102 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Replacing Toothbrushes
Toothbrushes should be changed regularly – they begin to look scraggy after about three months so should be replaced. Toothbrushes should not be shared as this will transfer germs.
Toothpaste
Toothpaste must contain fluoride which helps strengthen teeth to resist, reverse or slow down decay.
It is preferable to use a toothpaste that suits taste.
Children’s Toothpaste
Children between 2 and under 6 should use a child’s toothpaste which has less fluoride that adult toothpaste.
Toothpaste should no be swallowed and needs to be spat out of the mouth.
Mouths, however do not need to be rinsed following teeth cleaning because leaving the teeth in contact with the fluoride longer is good for the teeth.
Using Toothpaste for Children
Toothpaste is not required for children under 2 years of age. For children between 2 and 6 a smear is sufficient and for children over 6 a pea sized amount of adult toothpaste is recommended.
Flossing
Flossing is the only way to clean between the teeth. Flossing should be done daily - preferably at night time and before brushing.
There are a number of different types of floss available, some are like string and others similar to small plastic toothpicks.
All styles are effective and preferences are based on personal choice and budget.
Effective flossing takes practice but should be part of the daily routine.
Dental Checks
All children should have an annual check up with the dentist.
Dentists are trained to diagnosis and treat dental disease.
Problems with teeth and gums could be painless, making it more important for the annual check up.
If problems are left untreated, ongoing issues with oral health will occur.

103PaRROT Program - Child Health Check: Part 2 | A primary health care approach
Dental Visits
Once a child starts to feel pain, the dental problem has escalated.
The longer it takes for the problem to be treated the worse it will become.
If pain stops, it is still important to see a dentist, as this does not necessarily mean the problem has gone away.
Medical Referral
A child requires a medical referral if they complain of moderate to severe pain, and have abscesses, unusual lumps, swelling or ulcers.
Abscesses with associated facial swelling requires urgent follow up.
Young children with severe dental decay should also be referred to a medical officer for a more thorough check and treatment.
Dental Referrals
Children with dental pain, tooth trauma, swollen bleeding gums, crooked teeth, tooth decay and lumps, swelling and ulcers should be referred to a dentist.

104 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-3 Learning Activity
1. Which of the following statements are true?
Tick Answer
Flossing is best way to clean between teeth
Flossing needs to be done twice daily
Flossing is an optional element of oral hygiene
The best product for flossing is the string
A variety of flossing products can be used

105PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-3 Quiz
1. Which of the following statements are true? (More than one answer) 2 marks
Tick Answer
Gingivitis is inflamed or infected gums
Teeth should be cleaned with a hard toothbrush
A tooth abscess is a dental emergency
Babies teeth should be cleaned with a soft toothbrush and fluoride toothpaste
White discolouration of the tooth indicates active decay
2. Which of the following occurs when the lower teeth protrude over the upper teeth? (1 mark)
Tick Answer
Cross bite
Crowding
Crooked teeth
Gum boil
Gingivitis

106 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. Match the problem with its best definition (5 marks)
1. Gingivitis 2. Ulcer 3. Plaque 4. Active Decay 5. Non-active Decay
Problem Definition
Cement like structures between teeth
Black discolouration on tooth
Inflamed or infected gums
Small open lesion on the gums or cheek
Brown discolouration on tooth
4. It is best to use a medium toothbrush for teeth cleaning (1 mark)
Tick Answer
True
False
5. With appropriate intervention, active decay is reversible (1 mark)
Tick Answer
True
False

107PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC122 Theory to Practice Activity
Tommy who is 4 ½ years old has been brought to the clinic for a check. His mother says he has been unwell over the last week and she is worried about his health in general. When you talk to Mum she tells you:
• Tommy is often unwell. • He seems to always have a cold and runny nose and complained recently of a very sore throat. • He is having trouble weight bearing on his right ankle.• This is the second time in 6 months that he has had joint pain, although the last time it was in his left
knee which she thought was growing pains.• He has also had many ear infections in the past and she is worried he may have some hearing loss. • He has not had his four (4) year old immunisations yet, as each time Mum was going to bring him in he
had a cold.• Tommy is a fussy eater; he refuses to eat meat and all vegetables but loves mashed potato, fish and fruit.
He drinks juice and soft drink but refuses milk and water.• He is very clumsy and is having problems with his speech and playing with other children at preschool.• Mum is very worried as Tommy seems to be ‘just not right’ – he was very premature and had had health
problems as a baby.
You complete a child health check on Tommy and find:
• He weighs 13.5 kg and is 100 cm tall.• He has a bulging tympanic and a fungal infection in his right ear. • He is also lethargic and has a slight fever.• He has active caries on his 4 front teeth. • He has infected lesions on his elbows and hands with signs he has been scratching.
Please complete Tommy’s Child Health Check form, his growth chart and his BMI chart, then complete the following quiz.

HE
ALTH
CH
EC
K - 4 Y
EA
RS
Legend: Indicates a health risk that requires brief intervention, follow up or action.
Patient’s actual age:
Indigenous status: Aboriginal but not Torres Strait Islander origin Torres Strait Islander but not Aboriginal origin Both Aboriginal and Torres Strait Islander origin Neither Aboriginal or Torres Strait Islander origin Not stated / unknown
Parent / carer’s name: Relationship: Signature (consent for health check): Date:
Has the carer / parent been advised of the process and benefits of health check? Yes No
Medical historyAllergies:
Family history:
Medical history:
Current problems / concerns:
Examination (*MO’s note: examination requirements on following pages):
Medications:
Immunisations due at 4 years of age:
Immunisations current: Yes No (proceed to consent and immunise child)
Evidence of 4 year old immunisation sighted? Yes No (child must be vaccinated to claim ‘Healthy Kid’ check)
Evidence of immunisation sighted by (print name): Signature: Date:
© S
tate
of Q
ueen
slan
d (Q
ueen
slan
d H
ealth
) 201
2Li
cens
ed u
nder
: http
://cr
eativ
ecom
mon
s.or
g/lic
ense
s/by
-nd/
3.0/
au/d
eed.
enC
onta
ct: C
IM@
heal
th.q
ld.g
ov.a
u
DO
NO
T WR
ITE IN
THIS
BIN
DIN
G M
AR
GIN
DO
NO
T W
RIT
E IN
TH
IS B
IND
ING
MA
RG
IN
Page 1 of 4
Health Check4 Years
Medicare Item No. 715 or ‘Healthy Kid’ check
(Affix identification label here)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F IFacility: .........................................................................................................
ÌSW
058"
Îv3
.00
- 0
6/20
12M
at. N
o.: 1
0219
443
SW
058
Tommy
Sarah Mother
Nil known
Nil significant
Nil currently

Body measurements Print name: Signature: Date:
Weight kg ( ..................................... %le) Healthy Abnormal
Height cm ( ..................................... %le) Healthy Abnormal
Body Mass Index (BMI) Underweight Healthy Overweight Obese
Clinical measurements Print name: Signature: Date:
Breathing
*Heart sounds
Normal Noisy Coughing Wheeze Breathless
Normal Abnormal
General appearance Print name: Signature: Date:
Movement
Limbs
Joints
Normal Abnormal
Normal Abnormal
Normal Abnormal
Skin Describe skin: Healthy Intact Jaundice Sores Rash
Bites Scars Bruises Itchy
Developmental milestones Print name: Signature: Date:
Hops on one foot
Catches and throws ball
Runs and turns corners without over balancing
Draws a person with 2 or more parts (e.g. eyes, arms)
Is able to name drawing (e.g. drawing of dog, parent)
Uses a pencil grip
Plays with other children
Able to have a conversation
Is fluent in conversation
Is easily understood
Asks questions
Understands opposites
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Achieved Not Achieved
Ears and hearing Print name: Signature: Date:
Has your child had any ear infections or ear discharge in the last 12 months?
Are you concerned about your child’s ears or hearing?
Otoscopy
Tympanometry
Yes No
Yes No
Left ear: Healthy Refer
Right ear: Healthy Refer
Left ear: Healthy (Type A) Refer (Type B or C)
Right ear: Healthy (Type A) Refer (Type B or C)
Comments:
DO
NO
T WR
ITE IN
THIS
BIN
DIN
G M
AR
GIN
DO
NO
T W
RIT
E IN
TH
IS B
IND
ING
MA
RG
IN
Page 2 of 4
Health Check4 Years
Medicare Item No. 715 or ‘Healthy Kid’ check
(Affix identification label here)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
Tommy

Nutrition Print name: Signature: Date:
Healthy food
Unhealthy food
If your child was hungry are you always able to provide food?
Cereal with iron Vegetables Meat Fruit Fish
Water Milk
Coke / soft drink Junk food Juice Tea Cordial
Yes No
Continence / elimination Print name: Signature: Date:
Is the child independent in toileting?
Is the child incontinent of urine or faeces?
Does the child wet the bed?
Yes No
Yes No
Yes No
Oral health Print name: Signature: Date:
Are teeth present
Do you clean your child’s teeth and gums using a soft toothbrush with a low fluoride toothpaste, twice per day?
Oral examination of teeth
Oral examination of gums
Yes No
Yes No
Healthy Decay Malalignment No exam
Healthy Bleeding Swelling No exam
Social emotional well-being Print name: Signature: Date:
Does the parent / carer have concerns about any of the following
Observe: is interaction between mother / carer and child positive?
Coping: Yes No
Relationships (family and social): Yes No
Support available: Yes No
Violence: Yes No
Child’s behaviour: Yes No
Yes No
Environment Print name: Signature: Date:
Is the child exposed to cigarette smoke?
How many people live in the house?
Yes No
Topics for discussion / education Cross infection Injury prevention
Comments:
DO
NO
T WR
ITE IN
THIS
BIN
DIN
G M
AR
GIN
DO
NO
T W
RIT
E IN
TH
IS B
IND
ING
MA
RG
IN
Page 3 of 4
Health Check4 Years
Medicare Item No. 715 or ‘Healthy Kid’ check
(Affix identification label here)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
■
■
■
■
■
●
■
■
8
Tommy
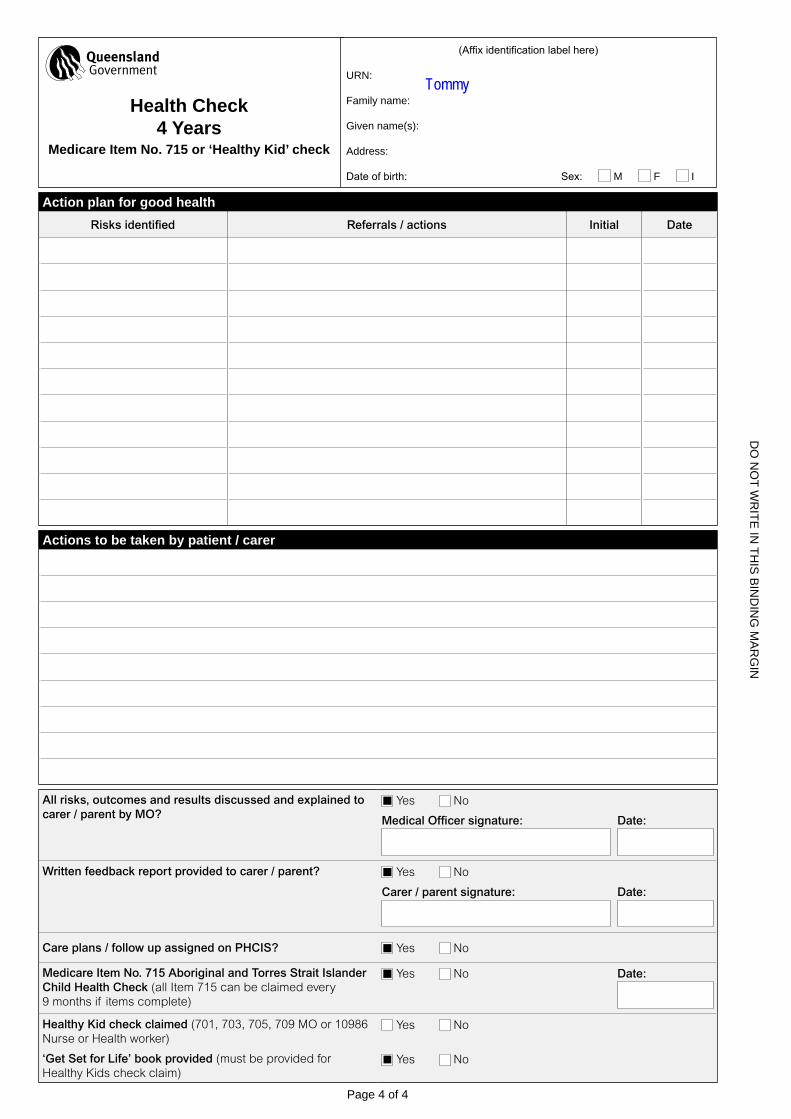
Action plan for good healthRisks identified Referrals / actions Initial Date
Actions to be taken by patient / carer
All risks, outcomes and results discussed and explained to carer / parent by MO?
Yes No
Medical Officer signature: Date:
Written feedback report provided to carer / parent? Yes No
Carer / parent signature: Date:
Care plans / follow up assigned on PHCIS? Yes No
Medicare Item No. 715 Aboriginal and Torres Strait Islander Child Health Check (all Item 715 can be claimed every 9 months if items complete)
Yes No Date:
Healthy Kid check claimed (701, 703, 705, 709 MO or 10986 Nurse or Health worker)
‘Get Set for Life’ book provided (must be provided for Healthy Kids check claim)
Yes No
Yes No
DO
NO
T WR
ITE IN
THIS
BIN
DIN
G M
AR
GIN
DO
NO
T W
RIT
E IN
TH
IS B
IND
ING
MA
RG
IN
Page 4 of 4
Health Check4 Years
Medicare Item No. 715 or ‘Healthy Kid’ check
(Affix identification label here)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
Tommy
■

WH
O C
hild
Gro
wth
Sta
nd
ard
s
Weig
ht-
for-
ag
e B
OY
S2
to 5
yea
rs (
per
cen
tile
s)
Ag
e (c
om
ple
ted
mo
nth
s an
d y
ears
)
Weight (kg)
5 ye
ars
4 ye
ars
3 ye
ars
2 ye
ars
9101112131415161718192021222324
9101112131415161718192021222324
24
68
102
46
810
24
68
10M
onth
s
15th
3rd
97th
50th
85th
Tomm
y

WH
O C
hild
Gro
wth
Sta
nd
ard
s
BM
I-fo
r-ag
e B
OY
SB
irth
to
5 y
ears
(p
erce
nti
les)
Mon
ths
Ag
e (c
om
ple
ted
mo
nth
s an
d y
ears
)
BMI (kg/m2)
1 ye
arBi
rth
2 ye
ars
3 ye
ars
4 ye
ars
5 ye
ars
101112131415161718192021
101112131415161718192021
24
68
102
46
810
24
68
102
46
810
24
68
10
15th
3rd
97th
50th
85th
BMI =
Wei
ght
(kg)
/ (H
eigh
t (m
) x H
eigh
t (m
))
Name
:To
mmy
View
Ans
wer
s

114 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC122 Theory to Practice Activity
1. There are a number of health concerns and Tommy needs to be reviewed as soon as possiblet
Tick Answer
True
False
2. What immediate follow up does Tommy require
Answer

115PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. Tommy’s weight is on which centile curve?
Tick Answer
20th centile
Between 95th and 98th centile
98th centile
Below the 3rd centile
5th centile
4. Tommy’s BMI is on which centile curve?
Tick Answer
20th centile
Between 95th and 98th centile
98th centile
Between the 3rd and 15th centile
5th centile
5. Are there any concerns with Tommy’s weight? If so, what are they?
Answer

116 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
6. What longer term follow- up does Tommy require?
Answer

117PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-1 Learning Activity Feedback
1. Which of the following statements about normal healthy skin are true?
Tick Answer
Dry
Smooth
Scaly
Lesion free
Slightly oily
2. Arrange the layers of skin in order from inner to outer
1: Epidermis 2. Subcutaneous 3. Dermis
Answer
1 Subcutaneous
2 Dermis
3 Epidermis

118 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-2 Learning Activity Feedback
1. Which of the following are signs of an allergic rash? (More than one possible answer)
Tick Choices
Welts
Crusty lesions
Lesions in the mouth
Lesions with fluid filled centre
Itchy lesions
2. Which of the following can be used to manage eczema? (More than one possible answer)
Tick Choices
Moisturisers
Antibiotics
Ultraviolet radiation
Antifungal creams
Dietary changes

119PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221-3 Learning Activity Feedback
1. Which of the following skin conditions need to be treated as soon as possible?
Tick Choices
Scabies
Fungal infections
Insect bites
Sores
Impetigo
All skin conditions should be treated as soon as possible to prevent complications such as systemic infection e.g.
Acute Post Streptococcal Glomerulo Nephritis.

120 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1221 Quiz Feedback
1. Match the type of rash with its most likely cause (5 marks)
1. Allergy 2. Hand, Foot and Mouth Disease 3. Chicken Pox 4. Eczema 5. Fifth’s Disease
Rash Cause
Hives Allergy
Dry scaly skin Eczema
Lacy rash Fifth’s Disease
Lesions around mouth Hand, Foot and Mouth Disease
Fluid filled blisters Chicken Pox
2. Which of the following statements are incorrect? (1 marks)
Tick Answer
The family of a person with scabies needs to be treated
Streptococcus is usually a harmless natural occurring bacteria
Scabies can be found in conjunction with impetigo
Fungal infections will clear up on their own
Impetigo is a bacterial infection

121PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. APSGN could be the consequence of which of the following conditions (5 marks)
Tick Answer
Scabies
Impetigo
Eczema
Insect bites
Minor abrasions
4. Strep A is the most common and dangerous of the streptococcal infections (1 mark)
Tick Answer
True
False
5. Fungal infections are normal in the tropics so do not need to be treated (1 mark)
Tick Answer
True
False

122 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-1 Learning Activity Feedback
1. Match the procedure with what it is checking for
1. Otoscopy 2. Tympanometry 3. Audiometry
Procedure Checking for
Otoscopy Visualise ear canal and tympanic
Tympanometry Measure canal volume
Audiometry Test hearing

123PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-2 Learning Activity Feedback
1. Match the type of problem you may see with the part of the ear anatomy it affects.
1. Ear canal 2. Ear Drum 3. Pinna 4. Middle Ear 5. Eustachian Tube
Problem Anatomy
Fungal infection Ear canal
Perforation Ear drum
Red, itchy and dry skin Pinna
Bulge in the ear drum Middle ear
Retracted eardrum Eustachian tube

124 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-3 Learning Activity Feedback
1. Match the image to its definition
Type A Type B Type C
Type - A, B or C Definition
Type A• Normal ear canal volume• Normal middle ear movement• Negative middle ear pressure
Type B• No middle ear movement• No middle ear pressure
Type C• Normal ear canal volume• Normal middle ear movement • Normal middle ear pressure

125PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222-4 Learning Activity Feedback
1. What is the minimum sound intensity a child has to respond to in both ears to pass a hearing test?
Tick Answer
25 dB
10dB
30 dB
45 dB
50 dB
2. Which of the following measurements returning a positive response indicates a child is hearing tone correctly?
Tick Answer
1000 Hz
6000 Hz
4000 Hz
2000 Hz
5000 Hz

126 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1222 Quiz Feedback
Please complete the gradable quiz for this session. You can complete this quiz as many times as you like until you are happy with your results.
1. Otoscopy checks canal volume
Tick Answer
True
False
2. Which of the following indicates a child may require follow up?
Tick Answer
Bulging tympanic membrane
Perforated tympanic
Canal volume between 0.2 and 2.0
Failed Audiometry at 55dB and 1000 Hz
Type A peak on Typanometry
Middle ear pressure above 100 daPa
Middle ear movement between 0.2 and 1.4

127PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. Which of the following requires urgent referral?
Tick Answer
Visible perforation
Ear canal blocked by wax
Sudden hearing loss or dizziness
Abnormal Typanometry results
Visible discharge
Failed Audiometry

128 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
4.
1 2
3 4
Tick Answer
2 Which image shows a fungal infection?
4 Which image shows a retracted drum?
1 Which image shows a bulging tympanic?
3 Which image shows a perforation?

129PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-1 Learning Activity Feedback
1. List in order the structures of the eye in which light travels to produce an image.
Cornea | Lens | Vitreous | Pupil | Optic Nerve | Retina
Order Answer
1 Cornea
2 Pupil
3 Lens
4 Vitreous
5 Retina
6 Optic nerve
2. Now match the structure of the eye with its role in the process of creating an image from light rays.
Cornea | Lens | Vitreous | Pupil | Optic Nerve | Retina
Structure Function
Pupil Controls the amount of light going through the eye
Cornea Takes wide diverging rays and bends them
Vitreous Transmits light to the retina
Lens Focuses light to the back of the eye
Optic nerve Transfers electrical impulses to the brain
Retina Changes light rays into electrical impulses

130 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-2 Learning Activity Feedback
1. Which of the following are included in the 12 month old eye check? (More than one answer)
Tick Answer
Visual acuity
Red eye reflex
Corneal light reflex
Near cover test
Far cover test
PC1223-3 Learning Activity Feedback
1. Match the eye abnormality with its definition
1. Conjunctivitis 2. Blepharitis 3. Stye 4. Amblyopia 5. Strabismus
Abnormality Definition
Amblyopia Vision development disorder
Strabismus Eyes not properly aligned
Stye Small infected lump on eyelid
Conjunctivitis Infection of the conjunctiva
Blepharitis Swollen, red, itchy eyelid

131PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1223-3 Quiz Feedback
1. Amblyopia and Strabismus are the same thing (1 mark)
Tick Choice
True
False
2. Match the test with what it is checking for (5 Marks)
1. Cover test 2. Corneal light reflex 3. Visual acuity 4. Red eye reflex 5. Eye inspection
Abnormality Definition
Corneal light reflex Amblyopia
Cover test Strabismus
Red eye reflex Retinal function
Visual acuity Ability to see from certain distances
Eye inspection Conjunctivitis
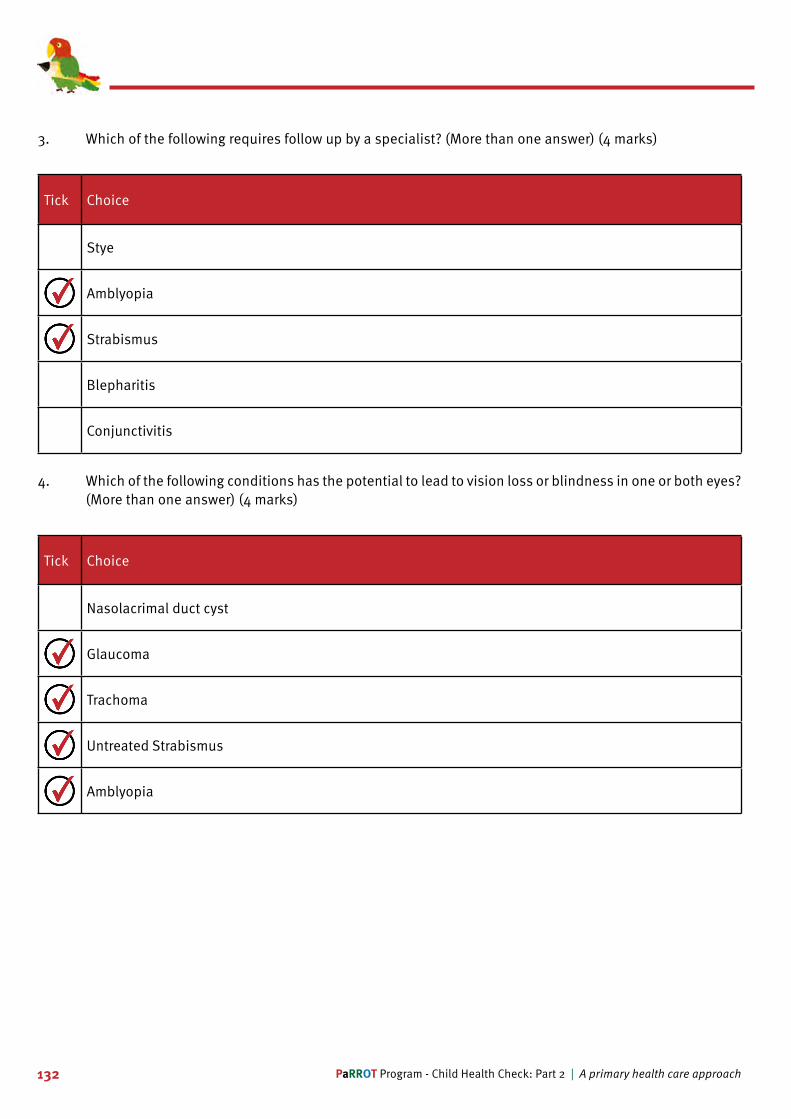
132 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. Which of the following requires follow up by a specialist? (More than one answer) (4 marks)
Tick Choice
Stye
Amblyopia
Strabismus
Blepharitis
Conjunctivitis
4. Which of the following conditions has the potential to lead to vision loss or blindness in one or both eyes? (More than one answer) (4 marks)
Tick Choice
Nasolacrimal duct cyst
Glaucoma
Trachoma
Untreated Strabismus
Amblyopia

133PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-1 Learning Activity Feedback
1. Which of the following factors contribute to a healthy oral environment?
Tick Answer
Good water supply
Access to fluoride
High sugar diet
Dental check-ups every 2 years
Good oral hygiene
PC1224-2 Learning Activity Feedback
1. Number the sequence of events that may result in the development of an oral health emergency
Sequence
6 Gum boil
2 Poor tooth brushing techniques
5 Infected gums
7 Gum abscess
3 Plaque build up
1 High sugar diet
4 Inflamed gums (gingivitis)

134 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-3 Learning Activity Feedback
1. Which of the following statements are true?
Tick Answer
Flossing is best way to clean between teeth
Flossing needs to be done twice daily
Flossing is an optional element of oral hygiene
The best product for flossing is the string
A variety of flossing products can be used

135PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC1224-3 Quiz Feedback
1. Which of the following statements are true? (More than one answer) 2 marks
Tick Answer
Gingivitis is inflamed or infected gums
Teeth should be cleaned with a hard toothbrush
A tooth abscess is a dental emergency
Babies teeth should be cleaned with a soft toothbrush and fluoride toothpaste
White discolouration of the tooth indicates active decay
2. Which of the following occurs when the lower teeth protrude over the upper teeth? (1 mark)
Tick Answer
Cross bite
Crowding
Crooked teeth
Gum boil
Gingivitis

136 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. Match the problem with its best definition (5 marks)
1. Gingivitis 2. Ulcer 3. Plaque 4. Active Decay 5. Non-active Decay
Problem Definition
Plaque Cement like structures between teeth
Non-active Decay Black discolouration on tooth
Gingivitis Inflamed or infected gums
Ulcer Small open lesion on the gums or cheek
Active Decay Brown discolouration on tooth
4. It is best to use a medium toothbrush for teeth cleaning (1 mark)
Tick Answer
True
False
5. With appropriate intervention, active decay is reversible (1 mark)
Tick Answer
True
False







143PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC122 Theory to Practice Activity Feedback
1. There are a number of health concerns and Tommy needs to be reviewed as soon as possiblet
Tick Answer
True
False
2. What immediate follow up does Tommy require
Answer
Tommy needs an urgent medical referral to exclude Acute Rheumatic Fever (See PCCM Paediatric Section - Immune Complications).
The Medical Officer should also conduct a thorough clinical assessment to determine Tommy’s general state of health.
Tommy needs to have his 4 year old immunisations as soon as possible and to be seen by a dentist.
His ear and skin infections need to be treated. It is possible he has infected scabies so the whole family and house hold needs to also be treated.
Tommy needs to continue to be monitored closely.

144 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
3. Tommy’s weight is on which centile curve?
Tick Answer
20th centile
Between 95th and 98th centile
98th centile
Below the 3rd centile
5th centile
4. Tommy’s BMI is on which centile curve?
Tick Answer
20th centile
Between 95th and 98th centile
98th centile
Between the 3rd and 15th centile
5th centile

145PaRROT Program - Child Health Check: Part 2 | A primary health care approach
5. Are there any concerns with Tommy’s weight? If so, what are they?
Answer
Tommy’s weight is below the third centile and his BMI is between the 3rd and 15th centile.
It is important to remember that a single, stand-alone measurement cannot be viewed in isolation; it needs to be reviewed over a period of time.
When viewed over time, Tommy’s weight and BMI centile have steadily dropped.
This is a concern, particularly because Tommy has had several bouts of poor health recently.
Tommy is at risk of ongoing poor health including failure to thrive which, if left untreated, may result in serious longer term complications.
6. What longer term follow- up does Tommy require?
Answer
Tommy’ growth is of concern and he has some developmental delays.
He requires specialist review and follow up and needs to continue to be monitored closely including:
• Regular child health checks• Paediatric follow up• Hearing health follow up. • Medical care if he has had Acute Rheumatic Fever.
Tommy’s food intake is also of a poor quality with little variety. This will further impact on his growth and development.
Mum would benefit from some education on good nutrition and some hints on how to get Tommy to eat foods that are healthy and nutritious.

146 PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC122 Post-Session Survey
Now that you have completed this session we ask you to take a few moments to complete the post-session survey for this topic. This will give us some indication about how well we have met your learning needs. Once submitted you will be eligible to receive your certificate.
Please indicate the degree to which you agree to the following, by ticking the box most relevant.
Stro
ngly
Agr
ee
Agre
e
Neu
tral
Dis
agre
e
Stro
ngly
Dis
agre
e
I am able to discuss the structure, physiology and function of the skin, ears, eyes and mouth
I can describe the differences between normal healthy and unhealthy skin, ears, eyes and mouth
I am able to provide simple prevention and treatment interventions for problems of the skin, ears, eyes and mouthI can clearly and accurately document findings on screening of the skin, ears, eyes and mouth
What, if anything could have been added to this session?

147PaRROT Program - Child Health Check: Part 2 | A primary health care approach
PC122 References
1. Queensland Health, Child and Youth Health Practice Manual. 2007, Queensland Health.
2. Queensland Health, The Royal Flying Doctor Service (Queensland Section), Apunipima Cape York Health Service. Chronic Disease Guidelines. 3rd ed. 2010. Cairns.
3. Queensland Health and the Royal Flying Doctor Service (Queensland Section), Primary Clinical Care Manual 8th Edition 2013. Cairns.
4. Western Australian Health (2013) Community Health Manual Procedure- 6.3.1 Otoscopic examination 5. Western Australia Health (2013) Community Health Manual Procedure – 6.3.2 Screening Audiometry
6. Western Australia Health (2013) Community Health Manual Procedure – 6.3.3 Tympanometry
7. Queensland Health - Deadly Ears Program
Top Related