







Languages
Pages
Legal


Patient’s Profile
GEW
49
Male
Chinese
150kg (obese)
15/7/09
Name
Age
Gender
Race
BW
DOA

C/O : Transferred from Damansara Specialist
Center Admitted due to fever, sore throat, cough,
headache
HPI : ILI for 3/7

PMH: Hypertension
Throat swab done : H1N1 +ve S/FH :
accountant Single MSM
PMHx : none
Diagnosis : Severe ARDS 2˚ to H1N1 pneumonitis Septic shock 2˚ to severe ARDS 2˚ to H1N1
pneumonitis ARF Juntional bradycardia VAP – MRSA and Acinetobacter Sacral bedsore Pressure sore on both feet

H1N1 introduction

Swine flu – new influenza virus Causing illness in people First detected in US in April 2009

Why called swine flu?
Lab testing showed that many of the genes in this new virus were very similar to influenza viruses that normally occur in pigs (swine) in North America
But further study has shown that this new virus is very different from what normally circulates in North American pigs.
It has two genes from flu viruses that normally circulate in pigs in Europe and Asia and bird (avian) genes and human genes.
Scientists call this a "quadruple reassortant" virus.
CDC, Antiviral Drugs and H1N1 Flu (Swine Flu). http://www.cdc.gov/h1n1flu/antiviral.htm, (accessed May 2009).

H1N1 Flu in Humans
Contagious Spreading from human to human
Through coughing/sneezing Touching something – surface/object with
flu viruses on it and then touching their mouth/nose

Signs and Symptoms
Fever Cough Sore throat Runny / stuffy nose Body aches Headache Chills and fatigue Diarrhea and vomiting

Current Treatments
Oseltamivir (Tamiflu) Zanamir (Relenza) Given 1st to those people who have been
hospitalized or are at high risk of severe illness from flu
Work best if given within 2 days of becoming ill but may be given later if illness is severe or for those at high risk complications

High-risk Groups
Children younger than 5 years old. The risk for severe complications from seasonal influenza is highest among children younger than 2 years old.
Adults 65 years of age and older. Persons with the following conditions:
Chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, hematological (including sickle cell disease), neurologic, neuromuscular, or metabolic disorders (including diabetes mellitus)
Immunosuppression, including that caused by medications or by HIV
Pregnant women Persons younger than 19 years of age who are receiving
long-term aspirin therapy Residents of nursing homes and other chronic-care
facilities.
Centers for Disease Control and Prevention, USA. Interim Guidance on Antiviral Recommendations for Patients with Novel Influenza A (H1N1) Virus
Infection and Their Close Contacts, May 6,2009.

Centers for Disease Control and Prevention, USA. Interim Guidance on Antiviral Recommendations for Patients with Novel Influenza A (H1N1) Virus
Infection and Their Close Contacts, May 6,2009.
ChildrenChildren
AdultAdult
Side Effects
Oseltamivir Nausea (10%) Vomiting (9%) Self-injury and delirium
Less severe if taken with food
Centers for Disease Control and Prevention, USA. Antiviral Agents for Seasonal Influenza: Side Effects and Adverse Reactions

Zanamivir Use in persons w/o underlying respiratory or
cardiac disease
Not recommended for tx for pt with underlying airway disease
Others SE (<5%) : allergic reaction, diarrhea, nausea, sinusitis, bronchitis, cough, headache, dizziness, ear, nose and throat infections
Asthma/COPD + ILI 20% decline in forced expiratory volume 1 second (FEV1)
Mild/moderate asthma w/o ILI BronchospasmRespiratory fx deterioration
Centers for Disease Control and Prevention, USA. Antiviral Agents for Seasonal Influenza: Side Effects and Adverse Reactions

Complications from H1N1
Pulmonary complications are the most common and include : Primary influenza pneumonia 2◦ bacterial pneumonia
Streptococcus pneumonia, Staphylococcus aureus, MRSA, Haemophilus influenza and occasionally other gram-negative bacilli
Micheal B. Rothberg, MD, MPH et al. Complication of viral Influenza,. The American Journal of Medicines, Vol 121, No4, 256-263, April 2008.

Pneumonia due to unusual pathogens/ immunocompromised hosts Aspergillus sp, Chlamydia pneumoniae, B-
hemolytic streptococci, Legionella pneumophila Exacerbation of chronic pulmonary
diseases 25% induce by virus influenza
Micheal B. Rothberg, MD, MPH et al. Complication of viral Influenza,. The American Journal of Medicines, Vol 121, No4, 256-263, April 2008.

Miscellaneous complications [3]
Myositis, rhabdomyolisis (rare)
Renal failure (resolve in 4-6 weeks)
Neurologic – encephalophaty, meningitis, focal neurologic disorder [1] (CNS involvement usually occurred in children)
Psychiatric complication – schizophrenia in offspring of women developed influenza during 2nd trimester [2]
CHF, ischemic heart disease, direct cardiac complications (uncommon)
[1] Studahl M. Influenza virus and CNS manifestations. J Clin Virol. 2003;28:225-232.[2] Barr CE, Mednick SA, Munk-Jorgensen P. Exposure to nfluenza epidemics during gestation and adult schizophrenia. A 40-year study.Arch Gen Psychiatry. 1990;47:869-874 .[3] Micheal B. Rothberg, MD, MPH et al. Complication of viral Influenza,. The American Journal of Medicines, Vol 121, No4, 256-263, April 2008.
During 24 days admission
Clinical Progression

H1N1 positive
D1
H1N1 positive
D1
ARDSARDS
Septic shock
D2
Septic shock
D2
VAPD6 C+S : MRSAD15 C+S : Acinetobacter spp
VAPD6 C+S : MRSAD15 C+S : Acinetobacter spp
Throat swab
Cap. Oseltamivir 150mg bd x 5/7
Hypoxeamia : ventilation support
IV Noradrenaline 2ml/h
IV Vancomycin 1.5g tdsIV Vancomycin 2g tds
Neb Polymyxin E 2mu bd

Juntional bradycardiaECG finding
Juntional bradycardiaECG finding
ARFD1-D3 : oliguria
ARFD1-D3 : oliguria
Sacral bedsoreSacral bedsore Pressure sore on both feetPressure sore on both feet
Prolonged hospitalization
Thrombophebilitis
D16
Thrombophebilitis
D16
IV Unasyn 1.5g tds
IV Dobutamine 1.5ml/h
IV Cloxacillin 1g qid
IV Aminolasix

Medications chart
Medications Date started
Date stopped
Durations (days)
Indication
Cap. Tamiflu 150mg bd 15/7 19/7 5 H1N1
IV Azithromycin 500mg od 15/7 20/7 6 Empirical - CAP
IV Augmentin 1.2g tds 15/7 16/7 2 Empirical - CAP
IV Ampicillin 2g qid 16/7 22/7 7 Empiric
IV Meropenem 2g bd 16/7 22/7 7 Empiric
IV Vancomycin 1.5g stat and tds
24/7 28/7 6 MRSA
IV Vancomycin 2g tds 28/7 30/7 3 MRSA
Cap. Rifampicin 600mg od 28/7 30/7 3 MRSA
IV Cloxacillin 1g qid 30/7 3/8 5 Thrombophebilitis
Neb Polymycin 2mu bd 31/7 6/8 7 Acinetobacter MRO
IV Unasyn 1.5g tds 5/8 Sacral bedsore


Days Findings Indications Managements
D1 – D5 H1N1Cyanotic, HypoxaemiaBradycardiaSeptic ShockHypoK
Throat swab : +vePaO2 40mmHg60/minK : 3.3
Start Cap. Oseltamivir 150mg bdVentilatied with high settingsIV Dobutamin 1.5ml/hIV Noradrenaline 2ml/hAdd 1g KCl in IVDAdd mist KCl 1g tds
D6-D10 MRSA infectionHyperbilirubinemia Hypernatremia
WBC : 13->20->18->19T.Bil : 27->25->60Na : 154 -> 156
Start IV Vancomycin 1.5g tdsOn meropenem and ampicillin
D11-D16 MRSA infectionRed man syndrome
WBC : 17->15->15Skin Rashes
IV Vancomycin 2g tds + Rifampicin 600mg odStop IV Vancomycin
D17-D24 Acinetobacter spp infectionBedsore
C+S BAL : acinetobeacter Neb Polymyxin 2mu bdIV Unasyn 1.5g tds
Pharmaceutical Care Issues
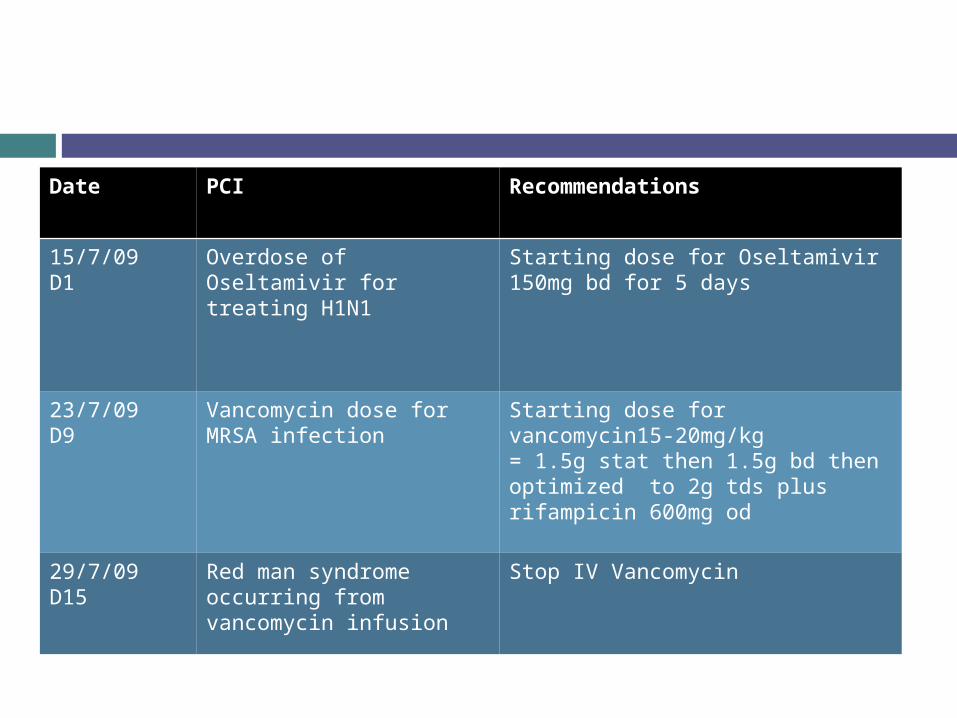
Date PCI Recommendations
15/7/09D1
Overdose of Oseltamivir for treating H1N1
Starting dose for Oseltamivir 150mg bd for 5 days
23/7/09D9
Vancomycin dose for MRSA infection
Starting dose for vancomycin15-20mg/kg= 1.5g stat then 1.5g bd then optimized to 2g tds plus rifampicin 600mg od
29/7/09D15
Red man syndrome occurring from vancomycin infusion
Stop IV Vancomycin

Does double dose 150mg bd is appropriate for treating this patient??
Current dose for H1N1 treatment is 75mg bd
1. Antiviral therapy
controversial
Centers for Disease Control and Prevention, USA. Interim Guidance on Antiviral Recommendations for Patients with Novel Influenza A (H1N1) Virus Infection and Their Close Contacts, May 6,2009.
Obese??Resistance ??
The conventional oseltamivir dose is 75mg bd (5 days).
Some centres are administering 150mg bd for up to 10 days in the critically ill to attempt to limit the duration of viral
shedding, ensure aggressive antiviral treatment and
therapeutic levels. This is an unlicensed use but there are
no reported safety concerns so far.Pandemic H1N1 2009 Clinical Practice Note – Managing critically ill cases. Royal College of Anaesthetists, Health Proctection Agency, The intensice care Society, 28 July 2009

Obesity vs dose No clinical data yet
Obesity vs severe complications Obese have a higher prevalence of comorbid
conditions Prolonged duration of mechanical ventilation
and longer ICU length of stay, but not mortality, are associated with moderate obesity
Extremely obese ICU patients had higher rates mortality, nursing home admission and ICU complications compared with moderate obese patientIntensive-Care Patients with Severe Novel Influenza A (H1N1) Virus Infection – Michigan, June 2009

It was noted in the CDC study that carrying extra weight can compromise the lungs and therefore may make people more vulnerable to complications from the novel flu virus.
Moreover, impaired breathing due to pressure on the chest and abdomen can restrict a person’s ability to breathe, cough and aerate the lungs.
Obese people possible high risk of complications from Pandemic (H1N1)2009, Manila, July 30, 2009

Drug-resistance vs dose No clinical data yet Few reports of drug resistant
August 09 : 2 reports from MMWR in immunocompromised patients [1]
Washington – both leukemia patients received immunosuppresive chemotherapy
July 09 : 3 reports of oseltamivir-resistant [2]
Hong Kong Japan Denmark
Became ill after receiving oseltamivir for chemoprophylaxis
[1] Oseltamivir-Resistant Novel Influenza A (H1N1) Virus Infection in Two Immunosuppressed Patients --- Seattle, Washington, 2009[2] Three Reports of Oseltamivir Resistant Novel Influenza A (H1N1) Viruses, CDC
The benefits of antiviral treatment with oseltamivir are unknown in patients with influenza presenting later than 2 days after illness onset.
Higher dose (hypothesis) : more rapidly decrease viral replication, reduce the duration and severity of illness, reduce complications, and improve outcomes after infection
with either human or avian influenza. Risk of higher dose :
unlikely worsen the disease caused by the influenza infection related to side effects and toxicities of the drug predictable risk - is primarily an increase in nausea and
vomiting High-Dose versus Standard-Dose Oseltamivir for the Treatment of Severe Influenza and Avian Influenza: A Phase II Double-Blind, Randomized Clinical Trial, Feb 27, 2008

Data to inform clinical guidance are needed on viral shedding pharmacokinetics clinical effectiveness of standard versus higher-dose
oseltamivir treatment on optimal duration of therapy for patients, including obese
persons, with severe or progressive H1N1virus infection. Until additional data are available, higher oseltamivir
dosage (150 mg bd for adults) or extending the duration of treatment can be considered for severely ill hospitalized patients with H1N1 if the patient is well-tolerated.
Intensive-Care Patients With Severe Novel Influenza A (H1N1) Virus Infection --- Michigan, June 2009. www.cdc.gov.mmwr

Patient’s outcomes :
Monitoring Parameters
D1 D2 D3 D4 D5
WBC 7.46 6.85 5.93 9.04 9.98
Temp 36 38 34.8
SpO2 80-85%
95% 96%
Lung Clear CXR - New patch – tracheal secretion creamy and yellowish VAP infection

2. MRSA infection
2º Bacterial infection one of the complications for prolonged hospitalization and with ventilator support.
Started dose with 1.5g tds and then optimized to 2g tds plus rifampicin 600mg od
Date Source Pathogen Sensitivity
S :20/7R: 23/7
BAL MRSACandida Albican
Vancomycin
S: 23/7R: 24/7
Trac Asp MRSA Vancomycin
S: 23/7R: 24/7
NSW MRSA Vancomycin
S: 24/7R: 26/7
Trac Asp MRSA Vancomycin
S: 27/7R: 30/7
Trac Asp MRSA Vancomycin
S: 29/7R: 31/7
BAL Acinetobacter MRO
Polymyxin B
Patient’s outcomes :

BAL C+S : MRSAStart IV Vanco 1.5g tds
IV Vanco 2g tds + Rifampicin 600mg od
Oseltamivir 150mg bd

Addition of rifampicin is often used, perhaps owing to better intraosseous and intracellular penetration, despite a lack of evidence for synergy.
Antoine Hamel et al Efficacy of quinupristin/dalfopristin versus vancomycin, alone or in combination with rifampicin, against methicillin-resistant Staphylococcus aureus in a rabbit arthritis model, sept 2007
Vancomycin + Rifampicin
Working??? Or not working??
Is not recommended combination treatment for MRSA if Vancomycin alone is not working
Consider to change to Linezolid

Therapy Subjects Microbiological response within 72 hours
Success rate
Mortality rate
Linezolid +/- carbapenem
n=35 75% 88% 13%
Vancomycin + rifampicin / aminoglycosides
n=35 17% 0% 53%
Jang HC et al, Salvage treatment for persistent methicillin-resistant Staphylococcus aureus bacteremia: efficacy of linezolid with or without carbapenem. Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea. Aug 2009.
Conclusion : Linezolid-based salvage therapy effectively eradicated S. aureus from the blood for patients with persistent MRSA bacteremia.

On D15 patient developed red man syndrome due to concentrated dilution
Vancomycin was diluted 2g in150cc which makes the final concentration 13.33 mg/ml
Run for 4 hoursMax conc < 5mg/ml
Fluid restriction, max conc
10mg/ml
Infusion rate 10mg / minDose Infusion time Dilution
500-1000mg 1 hour 100-200ml
1250-2000mg 1.5-2 hour 250-500ml
Complication Managements
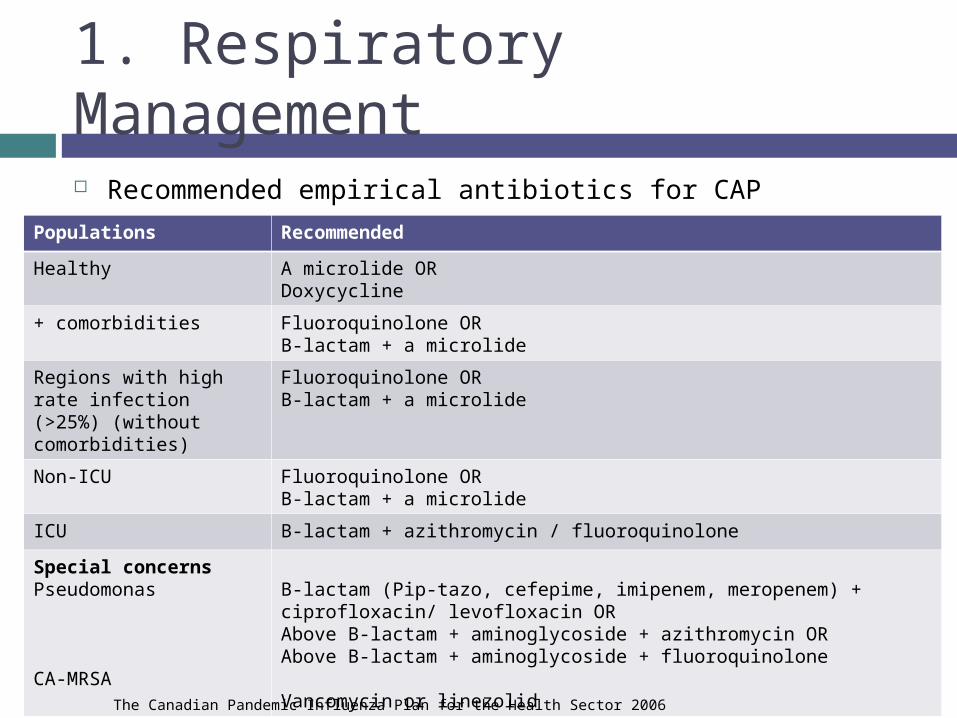
Recommended empirical antibiotics for CAP
1. Respiratory Management
Populations Recommended
Healthy A microlide ORDoxycycline
+ comorbidities Fluoroquinolone ORB-lactam + a microlide
Regions with high rate infection (>25%) (without comorbidities)
Fluoroquinolone ORB-lactam + a microlide
Non-ICU Fluoroquinolone ORB-lactam + a microlide
ICU B-lactam + azithromycin / fluoroquinolone
Special concernsPseudomonas
CA-MRSA
B-lactam (Pip-tazo, cefepime, imipenem, meropenem) + ciprofloxacin/ levofloxacin ORAbove B-lactam + aminoglycoside + azithromycin ORAbove B-lactam + aminoglycoside + fluoroquinolone
Vancomycin or linezolid
The Canadian Pandemic Influenza Plan for the Health Sector 2006

1. Respiratory Management (cont) Rapidly progressive respiratory failure is
relatively common preceding ICU admission Monitoring must include respiratory rate and SpO2
Hypoxaemia is also common Standard management by starting ventilation
High PEEP / high frequency oscillation may cause alveolar over-distension or worsen
oxygenation/haemodynamics. refractory hypoxaemia may persist for 48–72 hours
on antivirals before improving. prone positioning and nitric oxide have also been
used the outcomes are unclear
Pandemic H1N1 2009 Clinical Practice Note – Managing critically ill cases. Royal College of Anaesthetists, Health Proctection Agency, The intensice care Society, 28 July 2009

2. Cardiovascular Management Moderate hypotension is relatively common with
predictable increases in cardiac output and decreases in systemic vascular resistance. [1]
Most patients respond to fluid therapy +/- vasopressor therapy
volume expansion should be undertaken with caution as over-hydration seems to worsen outcome and as a result a conservative fluid strategy is recommended.
Patient receiving clopidogrel [2]
Inhibit hydrolysis of oseltamivir by 90% making this drug therapeutically in active.
[1] Pandemic H1N1 2009 Clinical Practice Note – Managing critically ill cases. Royal College of Anaesthetists, Health Proctection Agency, The intensice care Society, 28 July 2009[2] Deshi Shi et al. Anti-Influenza Prodrug Oseltamivir is activcated bye Carboxylesterase Human Carboxylesterase1, and the Activation is Inhibited by Antiplatelet Agent Clopidogrel, Sept 1, 2006

3. Renal Management
Impairment of renal function is common Continuous renal replacement therapy
(CRRT) maybe required in 10-50% Negative fluid balance by either diuretics
or continuous ultraflitration improves oxygenation
Pandemic H1N1 2009 Clinical Practice Note – Managing critically ill cases. Royal College of Anaesthetists, Health Proctection Agency, The intensice care Society, 28 July 2009
The dose for oseltamivir also need to be adjusted according to CrCl. >30ml/min : no dose adjustment – 75mg bd <30ml/min : 75mg once daily
Oseltamivir is not recommended for patients undergoing routine HD and PD with end stage renal disease
Tamiflu® PI, June 4 2009

Thank you~~
Top Related