







Languages
Pages
Legal


Occupational Therapy Section Meeting May 11, 2017
Page 1 of 2
Ohio Occupational Therapy, Physical Therapy, and Athletic Trainers Board Occupational Therapy Section Meeting
May 11, 2017 9:00 am. Roll Call
77 South High Street, 31st Floor, East B Columbus, Ohio 43215
Occupational Therapy Section Vision Statement:
The Occupational Therapy Section is committed to proactively:
Provide Education to the Consumers of Occupational Therapy Services; Enforce Practice Standards for the Protection of the Consumer of Occupational Therapy Services; Regulate the Profession of Occupational Therapy in an Ever-Changing Environment; Regulate Ethical and Multicultural Competency in the Practice of Occupational Therapy; Regulate the Practice of Occupational Therapy in all Current and Emerging Areas of Service Delivery.
1. Administrative Matters
1.1 Agenda Review
1.2 Approval of Minutes
Action Required
1.3 Executive Director’s Report
1.4 Executive Session
1.4.1 To discuss pending and imminent court action (ORC 121.22 (G)(3))
1.4.2 To discuss personnel matters related to:
Appointment; Employment; Dismissal; Discipline; Promotion; Demotion; Compensation (ORC 121.22 (G)(1)) (see Item 8.1)
Investigation of charges/complaints against a public employee, licensee, or regulated individual in lieu of a public hearing (ORC 121.22 (G)(1))
1.4.3 To discuss matters required to be kept confidential by federal law, federal rules, or state statutes (ORC 121.22 (G)(5))
1.5 Discussion of Law and Rule Changes
2. Licensure Applications (50 Minutes)
2.1 Application Review Liaison Report (5 Minutes)
Action Required
2.2 Releases from Limited License Agreement(s)
2.3 License Application Waiver Requests
2.4 Occupational Therapist/Occupational Therapy Assistant Examination Applications
Action Required
2.5 Occupational Therapist/Occupational Therapy Assistant Endorsement Applications
Action Required
2.6 Occupational Therapist/Occupational Therapy Assistant Reinstatement Applications
Action Required
2.7 Occupational Therapist/Occupational Therapy Assistant Restoration Applications
Action Required

Occupational Therapy Section Meeting May 11, 2017
Page 2 of 2
2.8 CE Request(s) for Approval
Action Required
2.8.1 CE Denial Appeal
Action Required
2.9 Licensure Renewal Report
3. Enforcement Division (50 Minutes)
3.1 Assistant Attorney General Report (5 Minutes)
3.2 Case Review Liaison Report (10 Minutes)
3.3 Releases from Consent Agreement(s)
3.4 Notice(s) of Opportunity for Hearing
3.5 Consent Agreement(s)
3.6 Affidavit Consideration(s)
3.7 Hearing Officer Report(s)
3.8 Summary Suspension(s)
3.9 To discuss proposed disciplinary action against a licensee pursuant to ORC 121.22 (G)(1) and pursuant to 121.22 (G)(5) that involve matters required to be kept confidential under ORC sections 149.43 (A)(2) and 4755.02 (E)(1)
4. Correspondence (30 Minutes)
5. OOTA Report (5Minutes)
6. Open Forum (5 Minutes)
7. Old Business (10 Minutes)
7.1 Limited License Rules
7.2 Section Retreat Planning
8. New Business (20 Minutes)
8.1 Medicaid School Program Requirements
8.2 BWC Proposed Rules
9. Next Meeting Preparation
9.1 Agenda Items
9.2 Executive Director Assignments
10. Adjournment
Occupational Therapy Section March 9, 2017
Page 1
Ohio Occupational Therapy, Physical Therapy, and Athletic Trainers Board
Occupational Therapy Section
March 9, 2017 9:00 a.m.
Members Present Beth Ann Ball, OTR/L, Chair Mary Beth Lavey, COTA/L, Secretary Jean Halpin, OTR/L Anissa Seifert, OTR/L Legal Counsel Melissa Wilburn, AAG
Staff Jennifer Adams, Investigator Diane Moore, Executive Assistant Lisa Ratinaud, Enforcement Division Supervisor Tony Tanner, Executive Director Guests Jacquelyn Chamberlin, OOTA
Call to Order Beth Ann Ball, Section Chair, called the meeting to order at 9:00 a.m. The Section began the meeting by reading the vision statement. The Occupational Therapy Section is committed to proactively:
Provide Education to the Consumers of Occupational Therapy Services; Enforce Practice Standards for the Protection of the Consumer of Occupational Therapy Services; Regulate the Profession of Occupational Therapy in an Ever-Changing Environment; Regulate Ethical and Multicultural Competency in the Practice of Occupational Therapy; Regulate the Practice of Occupational Therapy in all Current and Emerging Areas of Service Delivery.
Approval of Minutes Action: Jena Halpin all moved that the minutes from the January 12, 2017, meeting be approved as amended. Mary Beth Lavey seconded the motion. The motion carried. Administrative Reports Licensure Liaisons Reassignments CE Liaisons: Mary Beth Lavey and Anissa Siefert Enforcement Liaison: Jean Halpin Licensure Liaison: Jean Halpin Licensure Report Action: Jean Halpin moved that the Occupational Therapy Section ratify, as submitted, the occupational therapist and occupational therapy assistant licenses issued by examination, endorsement, reinstatement, and restoration by the Ohio Occupational Therapy, Physical Therapy, and Athletic Trainers Board from January 12, 2017 through March 9, 2017, taking into account those licenses subject to discipline, surrender, or non-renewal. Anissa Siefert seconded the motion. The motion carried. Occupational Therapist – Examination
Brittney Nicole Ali Nicholas Ryan Bell Emily Kathryn Blessing Kelsey Marie Bobek Stephanie Elizabeth Bombrys Amy R Botos Matthew Ryan Branden Kayleigh Buckner Krista Burchett Kelly Burdick Alice Marie Byrne Kelly Elizabeth Cassidy
DRAFT

Occupational Therapy Section March 9, 2017
Page 2
Alyssa Donceel Chandler Tracy Chappell Maria Kathleen Chiurazzi Colleen Louise Colvin Kelsie Ann Day Kelsey Douglas Jasmin Nicole Durig Erica Blake Ekvall Kristin Marie Elliott Julie Marie Faieta Amanda Diane Fitzgerald Megan Flower Lauren Elizabeth Frantz Elise Frein Hillary Suzanne Fritz Gabrielle Chastain Gabrosek Kirsten L Gaerke Chelsea Ann Geiger Brian Joseph Goedde Caroline Goldman Esther Graber Keri Michelle Greene Anthony Curtis Guinn Clasey Elaine Hahn Stephanie Lynn Hamm Justin David Hammer Marisa Hammond Patrick Haws Katie Helus Tiffany Ann Herzog Dana L. Hinebaugh Kristin Hopkins Megan Hostetler Alyssa Dree Iden Kara Beth Jordan Kari Kahle Veronica Mary Kennedy Jessica Lauren Klonk Molly Anne Laibe Allison Marie Larison Irene Lee Andrew James Leemaster Keri Ann Litmer Andrew Richard Lonneman Mary Lynn Mack Katharine Mailleue Caitlyn Malorni Melanie Rae Margraf Lindsey A Martindale Katherine Antoinette Maxwell Laura Adell McCready Caitlin Sighle Medley Britney Teanne Millfelt Rebecca Neff Samantha Jeane Nieman Allison Michelle Noss Erin Novak Hilary Obringer Amanda Oress Corinne Marie Piepmeyer Janell Lynn Pisegna Gayle Ann Rayman Emily Jane Riepenhoff Lauren Ashley Robinson Lauren Roy Brent R Sager Robin Phyllis Schnell Alison Kathryn Sehringer Gina Marie Seitz Niraj Anil Shah Julia Catherine Shaw Olivia LePontois Sherck Karena Olivia Skibinski Katherine Elizabeth Slavik Madonna Marie Smith Jillian Dyan Smith Gina Marie Solitro Hannah Storar Peter Attila Tapolyai Kylie Shannon Tayerle Olivia Thiemann Gabrielle Lynn Valco Kathryn Elizabeth Walsh Kirsten Nicole Wengerd Julianne Michelle Werner Jennifer Werring Stephanie Renee Williams Brooke Lynn Willis Michelle Kathleen Wirth Rachel Grace Wise Cortney Julianne Wisniewski Karlie Ann Wurm Anne Yanosko Kathryn Rose Zimmerly
Occupational Therapy Assistant – Examination
Kimberly Ann Bieri Abby Elaine Brenoel Hannah Lynn Burgess Cara Nichole Consiglio Connie Ann Diglaw Stephanie Sue Frase Christina Marie Garner Andrew Tyler Gulley Brittney Marree Hager Jonathan Drew Haislop Kelly L Hicks Amanda Michelle Johnson Heather Natasha Jones Mindi Michelle Jones-Quito Jenna Kate-Lynn Kassinger Julie Dawn Lachowyn Holly Leonard Aaron McClue Deborah Ann Moskalsky Brandy Marie Oates Maura O'Brien Jonah Lee Scott Parsons Jennifer Noel Ridgway Dwann Sade Robinson Carly Jade Ann Roush Shena Bulgado Simmons Kelli Lynn Tucker Lauren Nicole Whiting Jessica Elizabeth Wilt
Occupational Therapist – Endorsement
Michael Kwaku Agyemang Kerry Marie Allen Nicolas Christopher Beckas Traci Ann DeGrow Jennifer Lynn Hitzel Kristopher Allen Nelson Hannah Pilarski Lacey Anne Rae Kara Michelle Romano Nicole Sarmiento Brittany Renee Stasik Sridevi Peyyeti Surampudi Alison Atwood White Rondalyn Varney Whitney Molly Kathleen Wiberg Gina Wiley Kathryn Marie Wolfe
Occupational Therapy Assistant – Endorsement
Victoria Lynn Anderson Karissa Jo Greenhill Ashley Nichole Lohr Kelly Megan McConnell Sharilynn McGarey Teresa Anne Murphy
DRAFT

Occupational Therapy Section March 9, 2017
Page 3
Michelle M Newton Occupational Therapist – Reinstatement
Lindsey Lee Dean Barbara Joyce Verrusio Occupational Therapy Assistant – Reinstatement None Limited License Agreements Jean Halpin reported that Jean Aronoff complied with all terms and conditions and was released from her limited license agreement. Jean Halpin informed the Section that the nontraditional work setting was approved for limited license agreement OT restoration file #348216based on the documentation provided. Jean Halpin recommended that the Section grant a limited license agreement to occupational therapist restoration file # 3488669 based on the documentation provided. Action: Mary Beth Lavey moved that the Section grant a limited license agreement to occupational therapist restoration file # 3488669 based on the documentation provided. Beth Ann Ball seconded the motion. Jean Halpin abstained from voting. The motion carried. Jean Halpin recommended that the Section grant a limited license agreement to occupational therapist restoration file # 3347 based on the documentation provided. Action: Mary Beth Lavey moved that the Section grant a limited license agreement to occupational therapist restoration file # 3347 based on the documentation provided. Anissa Siefert seconded the motion. Jean Halpin abstained from voting. The motion carried. Continuing Education Report Action: Mary Beth Lavey moved that the Section approve 90 applications for contact hour approval. Jean Halpin seconded the motion. The motion carried. Assistant Attorney General’s Report Melissa Wilburn, AAG informed the Section that she will prepare the practice pointers overview at the Section Retreat. Enforcement Report Jean Halpin reported that the Enforcement Division opened two cases and closed eleven cases since the January 12, 2017, meeting. There are currently eight cases open. There are zero consent agreements and two adjudication orders being monitored. Jean Halpin notified the Board that the subject of case number OT-FY15-035 is indefinitely suspended and this case is now closed due to non-fulfillment of the requirements to reinstate their license per the consent agreement requirements. Enforcement Actions: Jean Halpin recommended that the Section accept the consent agreement for case OT FY17-013 in lieu of going to hearing. Action: Beth Ann Ball moved that the Section accept the consent agreement for case OT FY17-013 in lieu of going to hearing. Anissa Siefert seconded the motion. Jean Halpin abstained from voting. The motion carried. Jean Halpin recommended that the Section issue a notice of opportunity for a hearing for case number OT FY16-010 for falsification of patient records. Action: Beth Ann Ball moved that the Section issue a notice of opportunity for a hearing for case number OT FY16-010 for falsification of patient records. Mary Beth Lavey seconded the motion. Jean Halpin abstained from voting. The motion carried. Jean Halpin recommended that the Section issue a notice of opportunity for a hearing for case number OT FY17-012 for admission of poor record keeping. Action: Mary Beth Lavey moved that the Section issue a notice of opportunity for a hearing for case number OT FY17-012 for admission of poor record keeping. Beth Ann Ball seconded the motion. Jean Halpin abstained from voting. The motion carried.
DRAFT
Occupational Therapy Section March 9, 2017
Page 4
Jean Halpin recommended that the Section rescind the notice of opportunity for a hearing for case number OT FY17-002 as the licensee provided proof of continuing education. Action: Beth Ann Ball moved that the Section rescind the notice of opportunity for a hearing for case number OT FY17-002 as the licensee provided proof of continuing education. Anissa Siefert seconded the motion. Jean Halpin abstained from voting. The motion carried. Correspondence The Section reviewed the correspondence and provided feedback to the Correspondence Liaison. Old Business The Executive Director will make updates to the Board website. The Board Presentation at Owens community College was rescheduled for March 21, 2017. New Business The Section discussed the School- Based Practice issues. Beth Ann Ball will draft a response. Open Forum The Section will select date for summer retreat. Doodle a meeting request for the June and August date availability. Ohio Occupational Therapy Association (OOTA) Report Jacquelyn Chamberlin informed the Board that OOTA testified at the Finance sub-committee regarding the consolidation bill. Items for Next Meeting Retreat Planning - Doodle a meeting date Next Meeting Date The next regular meeting date of the Occupational Therapy Section is scheduled for Thursday, May 11, 2017. Action: There being no further business and no objections, Beth Ann Ball adjourned the meeting at 2:16 p.m. Respectfully submitted, Diane Moore
Beth Ann Ball, OTR/L, Chair Mary Beth Lavey, COTA/L, Secretary Ohio Occupational Therapy, Physical Therapy, Ohio Occupational Therapy, Physical Therapy, and Athletic Trainers Board, OT Section and Athletic Trainers Board, OT Section Tony Tanner, Executive Director Ohio Occupational Therapy, Physical Therapy, and Athletic Trainers Board MBL:dm
DRAFT

Type Applicant Full Name Licensed By
Occupational Therapist (OT) Shayna Back Endorsement
Occupational Therapist (OT) Jacqueline Barto Endorsement
Occupational Therapist (OT) Caroline Brandel Carroll Endorsement
Occupational Therapist (OT) Hannah Michelle Conn Endorsement
Occupational Therapist (OT) Shannon McDyer Daily Endorsement
Occupational Therapist (OT) Kailey DaLonzo Endorsement
Occupational Therapist (OT) Heather Marie Duyck Endorsement
Occupational Therapist (OT) Alan Terrell Freeman Endorsement
Occupational Therapist (OT) Susanna L. Graham Endorsement
Occupational Therapist (OT) Alyssa Kaylynn Gruhn Endorsement
Occupational Therapist (OT) Krista Lynn Hehemann Endorsement
Occupational Therapist (OT) Therese Ann Henry Endorsement
Occupational Therapist (OT) Teresa Carol King Endorsement
Occupational Therapist (OT) Kayla Kroninger Endorsement
Occupational Therapist (OT) Gar W Lee Endorsement
Occupational Therapist (OT) Ashley Marie Liberatore Endorsement
Occupational Therapist (OT) Katelyn M Martig Endorsement
Occupational Therapist (OT) Christina Needham Endorsement
Occupational Therapist (OT) Andrew Tyler Paulus Endorsement
Occupational Therapist (OT) Jason Adam Suda Endorsement
Occupational Therapist (OT) Shannon Marie Thomas Endorsement
Occupational Therapist (OT) York McFerran Thomas Endorsement
Endorsement Count 22
Occupational Therapist (OT) Susan Emily Arendt Examination
Occupational Therapist (OT) Kayla Elizabeth Beebe Examination
Occupational Therapist (OT) Kristina Dawn Blauser Examination
Occupational Therapist (OT) Alexis Nicole Bober Examination
Occupational Therapist (OT) Steffenie Nicole Camarata Examination
Occupational Therapist (OT) Meaghan Michelle Campbell Examination
Occupational Therapist (OT) Anita Marie Casto Examination
Occupational Therapist (OT) Emily Jacqueline Chaloux Examination
Occupational Therapist (OT) Kara Cicuto Examination
Occupational Therapist (OT) Kelly Joanne Cornachione Examination
Occupational Therapist (OT) Allexandra Marie Cox Examination
Occupational Therapist (OT) Erica M Ellerbrock Examination
Occupational Therapist (OT) Nicole Farrar Examination
Occupational Therapist (OT) Felicia Bianca Foci Examination
Occupational Therapist (OT) Kelly Garman Examination
Occupational Therapist (OT) Susan Elaine Gaskill Examination
Occupational Therapist (OT) Douglas Joseph Gentile Examination
Occupational Therapist (OT) Alexandra Gillen Examination
OT/OTA Licensure Applications May 11, 2017

Occupational Therapist (OT) Corey Allen Glanzer Examination
Occupational Therapist (OT) Claire Elizabeth Graupmann Examination
Occupational Therapist (OT) Taylour Hoyt Examination
Occupational Therapist (OT) Patricia Marie King Examination
Occupational Therapist (OT) Emily Rae Kingrey Examination
Occupational Therapist (OT) Olivia Kolomiyets Examination
Occupational Therapist (OT) Ivah Kurzhals Examination
Occupational Therapist (OT) Nicole Marie Luthman Examination
Occupational Therapist (OT) Amanda E McCoy Examination
Occupational Therapist (OT) Tyler McDaniels Examination
Occupational Therapist (OT) Kelly Marie O'Dell Examination
Occupational Therapist (OT) Megan Grace Placko Examination
Occupational Therapist (OT) Danielle Nicole Rasey Examination
Occupational Therapist (OT) Erica Jean Ream Examination
Occupational Therapist (OT) Elizabeth Anne Reilly Examination
Occupational Therapist (OT) Sarah Elizabeth Rhoad Examination
Occupational Therapist (OT) Julie Elizabeth Rolik Examination
Occupational Therapist (OT) Anthony J. Roscoe Examination
Occupational Therapist (OT) Jennifer Lynn Sabo Examination
Occupational Therapist (OT) Geoffrey A. Shafto Examination
Occupational Therapist (OT) Ashleigh Elizabeth Spires Examination
Occupational Therapist (OT) Emily Jane Stout Examination
Occupational Therapist (OT) Sarah Elizabeth Thomas Examination
Occupational Therapist (OT) Jonathan Conrad Upholz Examination
Occupational Therapist (OT) Alicia Lou Valle Examination
Occupational Therapist (OT) Eryn Clarissa Weber Examination
Occupational Therapist (OT) Chelsea Rae Wischmeyer Examination
Examination Count 45
Occupational Therapist (OT) Elizabeth Ann Buddelmeyer Reinstatement
Occupational Therapist (OT) Brenda L. Fisher Reinstatement
Reinstatement Count 2
Occupational Therapist (OT) Carla Ann Qazi Restoration
Occupational Therapist (OT) Tracy Ann Zinser‐Bourne Restoration
Restoration Count 2
Occupational Therapy Assistant (OTA) Elizabeth Arwen Boldt Endorsement
Occupational Therapy Assistant (OTA) Brittany Nicole Boso Endorsement
Occupational Therapy Assistant (OTA) Sherri Amanda Hurt Endorsement
Occupational Therapy Assistant (OTA) Kyle Huth Endorsement
Occupational Therapy Assistant (OTA) Alyssa Marie Jones Endorsement
Occupational Therapy Assistant (OTA) Kimberly Ann Krause Endorsement
Occupational Therapy Assistant (OTA) Christie Lynn Mielke Endorsement
Occupational Therapy Assistant (OTA) Kathleen Elaine Rill Endorsement
Occupational Therapy Assistant (OTA) Tina Hood Tafur Endorsement
Occupational Therapy Assistant (OTA) Hailee Raeanne Temple Endorsement

Occupational Therapy Assistant (OTA) Ellen Jane Violand Endorsement
Occupational Therapy Assistant (OTA) Karen Waldern Endorsement
Occupational Therapy Assistant (OTA) Brooke Beatrice Wilson Endorsement
Endorsement Count 13
Occupational Therapy Assistant (OTA) Shanice R. Abrams Examination
Occupational Therapy Assistant (OTA) Alicia Marciana Amador Examination
Occupational Therapy Assistant (OTA) Elizabeth Erin Antal Examination
Occupational Therapy Assistant (OTA) Kylah Danielle Arnwine Examination
Occupational Therapy Assistant (OTA) Laurence Zachary Barden Examination
Occupational Therapy Assistant (OTA) Rebecca Marie Barker Examination
Occupational Therapy Assistant (OTA) Kayle Kathleen Becht Examination
Occupational Therapy Assistant (OTA) Katey Jo Bentley Examination
Occupational Therapy Assistant (OTA) Douglas John Bernard Examination
Occupational Therapy Assistant (OTA) Teraina C Cargile Examination
Occupational Therapy Assistant (OTA) Ashley Nicole Chase Examination
Occupational Therapy Assistant (OTA) Chanell Coleman Examination
Occupational Therapy Assistant (OTA) Kelly Christine Collins Examination
Occupational Therapy Assistant (OTA) Amy J Eberly Examination
Occupational Therapy Assistant (OTA) Catherine Enciso‐McCoy Examination
Occupational Therapy Assistant (OTA) Erica Lee Ettinger Examination
Occupational Therapy Assistant (OTA) Lea Friend Examination
Occupational Therapy Assistant (OTA) Raimonda Garjonyte Examination
Occupational Therapy Assistant (OTA) Jamie Lee Garwood Examination
Occupational Therapy Assistant (OTA) Lisa Gingerich Examination
Occupational Therapy Assistant (OTA) Ashley Nicole Grove Examination
Occupational Therapy Assistant (OTA) Jennifer Guyton Examination
Occupational Therapy Assistant (OTA) Britni Gene Hall Examination
Occupational Therapy Assistant (OTA) Katelynn Hamilton Examination
Occupational Therapy Assistant (OTA) Christina Jacqueline Harber Examination
Occupational Therapy Assistant (OTA) Bryan James Holtsclaw Examination
Occupational Therapy Assistant (OTA) Celeste Noel Kapitan Examination
Occupational Therapy Assistant (OTA) Jennifer Dianne Keltner Examination
Occupational Therapy Assistant (OTA) Julie Knallay Examination
Occupational Therapy Assistant (OTA) Morgan Koepfle Examination
Occupational Therapy Assistant (OTA) Lisa Marie Kurcsak Examination
Occupational Therapy Assistant (OTA) Amanda Kay Lasko Examination
Occupational Therapy Assistant (OTA) Emily Ann Lentz Examination
Occupational Therapy Assistant (OTA) Rhonda Luce Examination
Occupational Therapy Assistant (OTA) Lisa Ann Martin Examination
Occupational Therapy Assistant (OTA) Hannah Mathis Examination
Occupational Therapy Assistant (OTA) Audrey Anna Miller Examination
Occupational Therapy Assistant (OTA) Danielle Nicole Morgan Examination
Occupational Therapy Assistant (OTA) Amanda Marie Murphy Examination
Occupational Therapy Assistant (OTA) Chloe Netro Examination

Occupational Therapy Assistant (OTA) Paige Elise Northeim Examination
Occupational Therapy Assistant (OTA) Kenneth E ONeill Examination
Occupational Therapy Assistant (OTA) Alycia Kay Perry Examination
Occupational Therapy Assistant (OTA) Samantha Jo Pucci Examination
Occupational Therapy Assistant (OTA) Chelsea Marie Pyle Examination
Occupational Therapy Assistant (OTA) Kayla Nanette Lee Schlund Examination
Occupational Therapy Assistant (OTA) Rachel Lynne Scribben Examination
Occupational Therapy Assistant (OTA) Frances Anne Sicking Examination
Occupational Therapy Assistant (OTA) Elizabeth Ann Smith Examination
Occupational Therapy Assistant (OTA) Monica Ashley Smith Examination
Occupational Therapy Assistant (OTA) Alexandria Nicole Stark Examination
Occupational Therapy Assistant (OTA) Ronald Glenn Swartz Examination
Occupational Therapy Assistant (OTA) Leo Sean Talikka Examination
Occupational Therapy Assistant (OTA) Archanna Corinna Walcott Examination
Occupational Therapy Assistant (OTA) Morgan Christine Williams Examination
Occupational Therapy Assistant (OTA) Samantha Lee Woodburn Examination
Occupational Therapy Assistant (OTA) Aubrey Leigh Wright Examination
Examination Count 57
Occupational Therapy Assistant (OTA) Diana Lynn Bishop‐Haney Reinstatement
Reinstatement Count 1
Grand Count 142
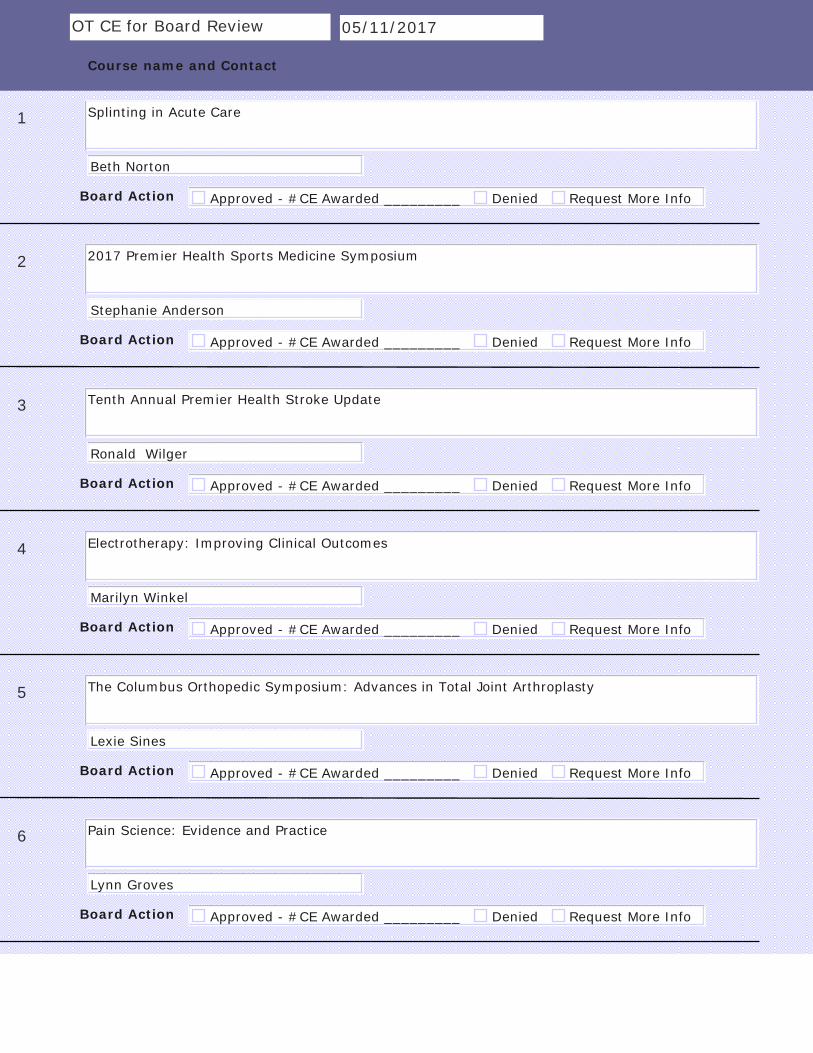
Course name and Contact
OT CE for Board Review 05/11/2017
Splinting in Acute Care
Beth Norton
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
1
2017 Premier Health Sports Medicine Symposium
Stephanie Anderson
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
2
Tenth Annual Premier Health Stroke Update
Ronald Wilger
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
3
Electrotherapy: Improving Clinical Outcomes
Marilyn Winkel
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
4
The Columbus Orthopedic Symposium: Advances in Total Joint Arthroplasty
Lexie Sines
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
5
Pain Science: Evidence and Practice
Lynn Groves
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
6

Course name and Contact
OT CE for Board Review 05/11/2017
19th Annual OhioHealth Orthopedic Education Day
Lynn Groves
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
7
Managing Behavioral Health Issues in Rehabilitation Patients
Lynn Groves
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
8
Dizziness ad Balance Symposium
Becky Roberts
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
9
Aaron W. Perlman Memorial Symposium, Cerebral Palsy 2017
Lisa Zimmermann
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
10
Post Secondary TransitionL How Occupational Therapy and Physical Therapy Can Help
Pamela Cotrell
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
11
Advanced Therasuit Method Training
Amanda Stohrer
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
12
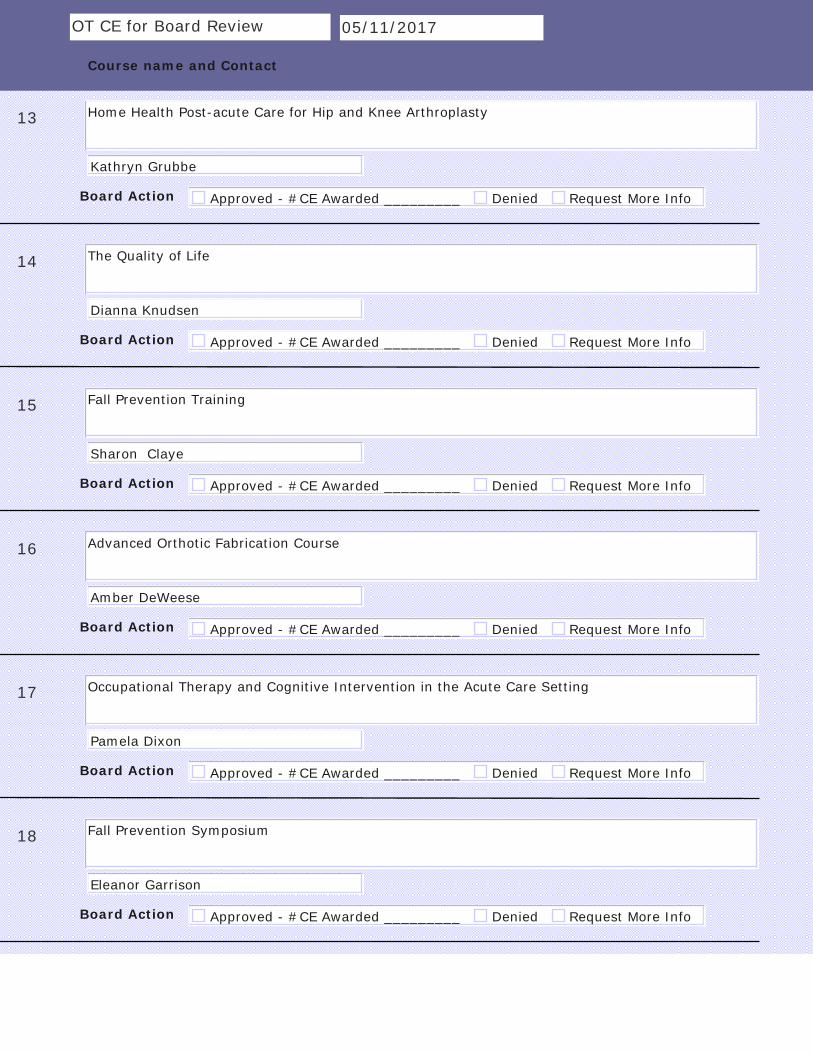
Course name and Contact
OT CE for Board Review 05/11/2017
Home Health Post-acute Care for Hip and Knee Arthroplasty
Kathryn Grubbe
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
13
The Quality of Life
Dianna Knudsen
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
14
Fall Prevention Training
Sharon Claye
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
15
Advanced Orthotic Fabrication Course
Amber DeWeese
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
16
Occupational Therapy and Cognitive Intervention in the Acute Care Setting
Pamela Dixon
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
17
Fall Prevention Symposium
Eleanor Garrison
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
18
Course name and Contact
OT CE for Board Review 05/11/2017
25th Annual Ohio Institute for OT/PT School-Based Practice
Holly Cartholomew Bartholomew
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
19
Successful Collaboration for Management of Dysphagia
Kim Downing
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
20
The Orthopedic Shoulder: Fundamentals for the Occupational Therapy Practitioner
Christine Griffin
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
21
The University of Toledo Orthopaedic Symposia Series, Symposium 4-Foot and Ankle Conditions
Cassandra Kaiser
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
22
Advanced Clinical Summit(for Neuro feeback)
Amie Crunelle
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
23
CIMT Presentation
Sue Gara
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
24

Course name and Contact
OT CE for Board Review 05/11/2017
Stroke 201: Introduction to Stroke Rehabilitation: Creating Recovery After Stroke
Lindsay Scott
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
25
Physical Work Performance Evaluation
Jacque Brown
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
26
Ethics and Rehab in 2017-Why Should I Care?
Lynn Groves
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
27
Lab Values and Importance to Therapy
Lynn Groves
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
28
Stroke Education Series
Courtney Petrone
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
29
Assessment and Treatment of Imbalance to Reduce Fall Risk
Karen Lance
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
30

Course name and Contact
OT CE for Board Review 05/11/2017
An Overview of: Cultural Considerations When Working with Diverse Patients
Michelle Graf
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
31
An Overview of ENT Procedures & Diagnosis Related to Rehab Services
Michelle Graf
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
32
2017 MS Symposium
Lynn Groves
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
33
An Overview of: Early Mobilization/Intervention in the ICU Setting
Michelle Graf
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
34
Orthosis Options for DRUjt and CMCjt Conditions
Lori DeMott
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
35
Level 1 Instrument Assisted Soft Tissue Mobilization (IASTM)
Nick Colosi
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
36

Course name and Contact
OT CE for Board Review 05/11/2017
Upper Extremity Cadaver Course for DeQuervain’s Release and Flexor Tendon Repair
Amber DeWeese
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
37
Best Practices in Pediatric Therapy
Amy Johnson
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
38
Milestones 15th Annual Autism Spectrum Disorder Conference
Leslie Rotsky
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
39
Milestones 15th Annual Autism Spectrum Disorder Conference
Leslie Rotsky
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
40
Milestones 15th Annual Autism Spectrum Disorder Conference
Leslie Rotsky
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
41
25th Annual Virginia Miller Educational Seminar
Julie Houston
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
42
Course name and Contact
OT CE for Board Review 05/11/2017
Mellen Center Update in Multiple Sclerosis
Brigid Ring
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
43
Effective Daily Treatment Notes to Support CPT Codes
Kim Downing
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
44
Strain Counterstrain-for the Upper Quarter for PTs & OTs
Rachel Walton
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
45
Encouraging Clients to Become Solution Focused
Rebecca Balmert
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
46
Aging Eye Summit: Vision for the Future
Laura Schwartz
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
47
Extensor Tendon Injury, Repair and Rehabilitation
Karen Bitzer
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
48

Course name and Contact
OT CE for Board Review 05/11/2017
The Concussion Health Summit
Bridgett Wallace
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
49
Expanding Patient Engagement in Critical Care: Practice Pattern Changes from the ICU Pilot Project
Lynn Groves
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
50
Prosthetic Joint Infections: Current Concepts and Implications for Rehabilitation
Lynn Groves
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
51
Pharmacology for Health Sciences
Keeley Shaw
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
52
The Plagiocephaly/Torticollis Connection: Assessment and Treatment Options for the PediatricTherapist
Alexandria Haigh
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
53
Evidence Based Management of the Throwing Athlete
Jason Dundr
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
54

Course name and Contact
OT CE for Board Review 05/11/2017
The University of Toledo Orthopaedic Symposia Series, Symposium 5-Arthritis & Joint Arthroplasty
Cassandra Kaiser
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
55
IASTM: A Brief Overview
Angie Strong
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
56
Issues in Acute Care Journal Club
Andrew Morris
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
57
Essentials of Neurocritical Care: Translating Research to Clinical Practice
Michelle Graf
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
58
Essentials of Neurocritical Care: Translating Research to Clinical Practice
Michelle Graf
Approved - #CE Awarded _________ Denied Request More InfoBoard Action
59
OCCUPATIONAL THERAPY SECTION ENFORCEMENT REVIEW PANEL MEETING
Date: April 26, 2017 Meeting Time: 9:30 am
Board Office Conference Room-16th Floor
“New” cases opened since the March meeting: 7
Cases “closed” at the March meeting: 5
Cases “currently open”: 10
Active consent agreements: 1
Adjudication orders being monitored: 2
Physical Therapy Section New cases opened since the March meeting: TBD
Cases closed at the March meeting: TBD Cases currently open: TBD
Active consent agreements: TBD Adjudication orders being monitored: TBD
Athletic Trainers Section New cases opened since the March meeting: TBD
Cases closed at the March meeting: TBD Cases currently open: TBD
Active consent agreements: TBD Adjudication orders being monitored: TBD
*Statistics as of 4/19/17
McKenzie Abigail
008651
Occupational Therapy
Can you bill for in home services for a child that is older than 3 in the state of Ohio? I have a lot of parents who have asked about help setting up TEACCH structure in their homes and I cannot find information on the legality of that.
It is not within the jurisdiction of the Occupational Therapy Section to render billing and reimbursement advice. The Section recommends that you refer to payer policies for any specific billing and reimbursement requirements in your setting. You might also contact the Ohio Occupational Therapy Association, or the Reimbursement Department of the American Occupational Therapy Association.
The requirements for provision of occupational therapy services are consistent across practice settings. If you are representing yourself as an occupational therapist and/or your services as related to your skills as an occupational therapist (regardless of payer source), each client would require an evaluation and plan of care.
According to rule 4755-7-02 (A) of the Administrative Code, occupational therapists shall assume professional roles and responsibility for the following activities, which shall not be wholly delegated, regardless of the setting in which the services are provided:
(1) Interpretation of referrals or prescriptions for occupational therapy services;
(2) Interpretation and analysis for evaluation purposes;
(3) Development, interpretation, and modification of the treatment/intervention plan and the discharge plan.
Additionally, rules 4755-7-08 (C)(13) and (15)(a) of the Ohio Administrative Code require a licensee to advocate for clients to obtain needed services through available means, and that licensees shall obtain informed consent from clients.
If you decide to bill for your services through a third party payer, the Section recommends that you refer to Medicare, Medicaid, and/or payer policies for any specific billing and
DRAFT

reimbursement requirements in your setting. You might also contact the Ohio Occupational Therapy Association, or the Reimbursement Department of the American Occupational Therapy Association.
DRAFT

Misko Alexis
OT008097
Occupational Therapy
As an OT in the state of Ohio, am I permitted to sign a form stating that a person needs modified equipment for their job for musculoskeletal reasons? This person is not my patient and is not someone I have encountered through my job. In this example, the individual is a police officer seeking a lighter weight, more ergonomic duty belt as opposed to the standard issue one in order to prevent future low back problems. Other officers have obtained the lighter weight belts with signatures from their chiropractors. Furthermore, if an OT is not permitted to sign this form, is a PT? Thank you for any information.
The requirements for provision of occupational therapy services are consistent across practice settings.
If you are representing yourself as an occupational therapist and/or your services as related to your skills
as an occupational therapist (regardless of payer source), each client would require an evaluation and
plan of care.
According to rule 4755‐7‐02 (A) of the Administrative Code, occupational therapists shall assume
professional roles and responsibility for the following activities, which shall not be wholly delegated,
regardless of the setting in which the services are provided:
(1) Interpretation of referrals or prescriptions for occupational therapy services;
(2) Interpretation and analysis for evaluation purposes;
(3) Development, interpretation, and modification of the treatment/intervention plan and the
discharge plan.
Additionally, rules 4755‐7‐08 (C)(13) and (15)(a) of the Ohio Administrative Code require a licensee to
advocate for clients to obtain needed services through available means, and that licensees shall obtain
informed consent from clients.
If you decide to bill for your services through a third party payer, the Section recommends that you refer
to Medicare, Medicaid, and/or payer policies for any specific billing and reimbursement requirements in
your setting. You might also contact the Ohio Occupational Therapy Association, or the Reimbursement
Department of the American Occupational Therapy Association.
DRAFT

Christian Andrea
OT2279
What is the correct way to document continued OT services (school based) when an IEP has expired, and I have not yet received the new IEP. I do not write on the IEP, I make recommendations only, therefore, I am unsure what the new IEP document states until I receive a copy. I work in a charter school, and the district of residence is the one who writes the IEP. I did contact the SST in my area, and was referred to my licensure board for direction. Thank you for your time
DRAFT

Heilman Ashley
008040
Occupational Therapy
Hello, I have a question regarding using kinesiology tape in home health setting. Do I need a physician's order to apply the tape to the left shoulder to decrease subluxation following a CVA? I reviewed the laws and rules but did not see anything regarding phyicians orders. Thank you for the information, Ashley Heilman
DRAFT

Heilman Ashley
008040
Occupational Therapy
Hello, I have a question regarding using kinesiology tape in home health setting. Do I need a physician's order to apply the tape to the left shoulder to decrease subluxation following a CVA? I reviewed the laws and rules but did not see anything regarding phyicians orders. Thank you for the information, Ashley Heilman
DRAFT

Boling Daniella
OT009396
Occupational Therapy, Occupational Therapy Assistant
I work in skilled nursing and I and an OTA completed a home assessment for one of our patients, the home was in horrible condition, with no running water, no gas, no electricity. The ceiling was caving in, there were light fixtures hanging from the ceiling due to animals chewing the electrical ceiling. The patient wants to discharge to this home and is likely to go AMA. This home is absolutely not safe and we ended our evaluation as soon as we entered and were able to convince the patient to come back with us to the SNF. We have reported this to our rehab director and our social worker, we would like to ensure that we follow the proper procedures for reporting the home and to whom.
DRAFT
Norton Dinah Beth
OT 02577
Occupational Therapy
With the increase in Occupational Therapy's involvement in the intensive care units and early mobility, it has been suggested that OTs be trained in suctioning for ventilator patients. I am writing on behalf of our OT department to get some advice on if suctioning falls under of scope of practice. Thanks for your assistance, Beth Norton
in accordance with section 4755.04 (A)(3) of the Ohio Revised Code, it is the position of the Occupational Therapy Section that occupational therapy practitioners may use physical agent modalities in the provision of occupational therapy services provided that the occupational therapy practitioner demonstrates and documents competency in the modality, in accordance with rule 4755‐7‐08 of the Administrative Code, and is practicing within the occupational therapy scope of practice. If the modality will be administered by an occupational therapy assistant both the supervising occupational therapist and occupational therapy assistant must document and demonstrate competency in the techniques or modality.
DRAFT

Parrott Emily
OT.008217
Occupational Therapy
Is there an official standpoint on an occupational therapist practicing dry needling? I feel like I have seen previously that it was only allowed for PTs due to the fact that the skin is punctured and now I cannot find one way or another for OT, I can only find information for PT. I would appreciate any clarification. Thank you!
DRAFT

Newhart Heather
006319
Occupational Therapy
The school district myself and my OTR / COTA employees contract with is requiring all of us to obtain an ORP (ordering, referring, prescribing) # for the purposes of continuing to bill the Medicaid Schools program, and also for continuing to be contracted with the district. We all currently have NPI #'s and follow the district requirements for documentation for the purposes of the district currently billing Medicaid for our OT services. My question is: Do the requirements of being an ORP provider through the Medicaid program fall within the scope of practice for OTRs and COTAs? If so, what additional liabilities are we potentially responsible for by being the ORP provider? Should we feel comfortable obtaining this ORP# and continuing to follow the districts requirements for documenting on HPC for purposes of the district billing Medicaid?
In response to your question regarding Medicaid billing in the schools, our practice act is silent on
billing. It is not within the jurisdiction of the Occupational Therapy Section to render billing and
reimbursement advice. The Section recommends that you follow the Medicaid payer policies for any
specific billing and reimbursement requirements. The Section also recommends that you contact the
Ohio Occupational Therapy Association’s pediatrics member support group coordinator concerning
questions regarding this school‐based issue at www.oota.org as they are closely monitoring this matter.
According to the Ohio Practice Act for Occupational Therapy, 4755‐7‐08 Code of ethical conduct, A
licensee shall not use or participate in the use of any form of communication that contains false,
fraudulent, deceptive, or unfair statements or claims. Regardless of practice setting, the occupational
therapy practitioner shall maintain the ability to make independent judgments. A licensee shall strive
to effect changes that benefit the client. (10) A licensee shall accurately represent the qualifications,
views, contributions, and findings of colleagues and students. (11) A licensee shall not misrepresent the
credential, title, qualifications, education, experience, training, and/or specialty certifications held by
the licensee. (12) An individual licensed by the occupational therapy section has a responsibility to
report any organization or entity that holds itself out to deliver occupational therapy services that
places the licensee in a position of compromise with this code of ethical conduct
DRAFT

Boylen James
0000
Occupational Therapy Assistant
Is it within the scope of practice of an OTA or PTA to elect to co treat if that is not part of the care plan?
DRAFT

Wendland Porter PT Jean
2029
Occupational Therapy Assistant
PTAs are permitted to accept and transcribe physicians' orders. There is nothing in the Laws and Rules for Occupational Therapy that say that OTAs can or can't. Please clarify.
DRAFT
Heyob Jennifer
PTA07034
Occupational Therapy, Physical Therapy
I need clarification on procedures for verbal orders taken by both PT and OT, as well as COTA and PTA My setting is a SNF where evaluating therapists feel that verbal orders received from an ortho CNP making his rounds for status changes like weight bearing or dc of sling stand alone and can be passed word of mouth. Or simply written in a soft chart communication log, not given to nursing or even in our computer documentation. My understanding is all verbal orders are quickly followed up with a signed written order and put in the medical record or nursing chart. Thanks for your assistance
DRAFT
Schmidt Jeri
Occupational Therapy Assistant
I am interested in taking an online OT AIDE course program from Penn Foster Career School. Upon completing this program I will receive an undergraduate OT AIDE diploma..Are there any special requirements in OHIO I should know about before completing this program? Thank you!
DRAFT

Donovan Jessica
PT013465
Occupational Therapy Assistant, Physical Therapy Assistant
Can a PTA or a COTA perform a environmental/home safety screen? For example, can they utilize the Home FAST to identify potential fall risk related to their environment?
DRAFT
Carraher Jill
OT005260
Occupational Therapy
I started a PRN job and completed a few evals. I was not yet CARE tool certified so my evals are marked incomplete. But I billed for eval and tx. Now I got my certification and need to finalize and complete the evals. Is the start date last week when I first did the eval? Or the date I finalize it? And will insurance pay for the treatment last week? Were they considered to be on caseload?
It is not within the jurisdiction of the Occupational Therapy Section to render billing and reimbursement
advice. The Section recommends that you refer to payer policies for any specific billing and
reimbursement requirements in your setting. You might also contact the Ohio Occupational Therapy
Association, or the Reimbursement Department of the American Occupational Therapy Association.
DRAFT

Eckel Jillian
10974
Physical Therapy
I have recently joined the rehabilitation team with the new Mount Carmel Rehabilitation Hospital in partnership with HealthSouth in Westerville, OH. We are reviewing our policies and want to confirm the timeframe in which notes written by a PTA or a COTA need to be cosigned by the primary PT or OT. I could not locate this specific information in the laws. Are you able to assist me with this information?
Rule 4755‐7‐04(H) of the Ohio Administrative Code states that “Any documentation written by an occupational therapy assistant, student occupational therapist, or student occupational therapy assistant for inclusion in the client’s official record shall be co‐signed by the supervising occupational therapist” but does not specify time requirements for co‐signing the occupational therapy assistant’s notes. It is the position of the occupational therapy section that the urgency of reviewing and co‐signing notes may vary with the patient population and with the acuity of the patient’s condition. The physical therapist should be able to demonstrate that effective supervision was provided for the particular patient care delegated to the physical therapist assistant.
DRAFT

Gallick Joanne
1342
Occupational Therapy
I have started a new job that has 4 full time COTAs and several prn COTAs. Is there a limit as to how many I can supervise? Thanks.
No, it is up to your professional judgement how many OTA/L's you can supervise. 4755-7-04 Supervision. (B) The following factors must be considered by the supervising occupational therapist when determining the appropriate frequency, methods, and content of supervision: (1) Complexity of the client needs; (2) Number and diversity of clients; (3) Skills of the occupational therapist and occupational therapy assistant; (4) Type and number of practice settings; (5) Requirements of the practice setting; and (6) Any other regulatory or administrative requirements. (C) Occupational therapist assistant. Supervision of the occupational therapy assistant, as defined in division (C) of section 4755.04 of the Revised Code, requires initial direction and periodic inspection of the service delivery and relevant in-service training. The supervising occupational therapist need not be on-site, but must be available for consultation with the occupational therapy assistant at all times. (1) The supervising occupational therapist must provide supervision at least one time per week for all occupational therapy assistants who are in their first year of practice. (2) The supervising occupational therapist must provide supervision at least one time per month for all occupational therapy assistants beyond their first year of practice. (3) Supervision requires an interactive process between the supervising occupational therapist and the occupational therapy assistant. The interactive process must include, but is not limited to, review of the following: (a) Client assessment; (b) Client reassessment; (c) Treatment/intervention plan; (d) Intervention; and (e) Discontinuation of treatment/intervention plan. (4) Co-signing client documentation alone does not meet the minimum level of supervision. (5) It is the responsibility of the occupational therapist and occupational therapy assistant to establish evidence that the supervision occurred in accordance with the requirements of this rule. This evidence may include documentation in the client record, or it may exist as a separate document, such as a collaboration log DRAFT
Hi Tony, I am a licensed occupational therapist in Ohio in private practice. I am considering adding a blog to my practice that will include education information, primarily on health, wellness, occupation, and ergonomics. Does the state of Ohio have parameters in our scope of practice regarding blogging? If so, where can I find these? Also, are there any stipulations from the State of Ohio for generating revenue for an occupational therapist via an educational blog? I wanted to make sure this was not a conflict of interest somehow or viewed as unethical. I have seen other OT blogs where things are sold. I wanted to check before creating so I do not do something outside of the practice act or ethics. Thank you, Julie Julie Zeigler Wood, OTR/L, LMT, CFCE, CEAS, CEIM Occupational Therapist Registered and Licensed, Licensed Massage Therapist, Certified Functional Capacity Evaluator, Certified Ergonomics Assessment Specialist Certified Educator Infant Massage Mobile: 614‐581‐8780 Fax: 614‐853‐2686 The OT Practice Act is silent on this matter. The requirements for provision of occupational therapy services are consistent across practice settings. If you are representing yourself as an occupational therapist and/or your services as related to your skills as an occupational therapist (regardless of payer source), each client would require an evaluation and plan of care. According to rule 4755‐7‐02 (A) of the Administrative Code, occupational therapists shall assume professional roles and responsibility for the following activities, which shall not be wholly delegated, regardless of the setting in which the services are provided: (1) Interpretation of referrals or prescriptions for occupational therapy services; (2) Interpretation and analysis for evaluation purposes; (3) Development, interpretation, and modification of the treatment/intervention plan and the discharge plan. Additionally, rules 4755‐7‐08 (C)(13) and (15)(a) of the Ohio Administrative Code require a licensee to advocate for clients to obtain needed services through available means, and that licensees shall obtain informed consent from clients. If you decide to bill for your services through a third party payer, the Section recommends that you refer to Medicare, Medicaid, and/or payer policies for any specific billing and reimbursement requirements in your setting. You might also contact the Ohio Occupational Therapy Association, or the Reimbursement Department of the American Occupational Therapy Association. It is also advisable to seek consultation from your legal representation.
DRAFT
Alex Karen
2144
Has it ever been legal, in the stated of Ohio, for and OTA to do an initial evaluation on a patient and then have the OT see the patient for 15 minutes and sign off on the evaluation. I currently work with someone who says she did this in either the 1980's or 1990's.
DRAFT

Birkhimer Virginia
5354
1. What does 'direct access mean'? 2. In Ohio, is it legal to evaluate and treat a patient without a prescription from a Physician? 3. If so, is an individual able to refer him/her self- verbally? 4. Any other info you can provide would be appreciated.
DRAFT

Constable Kay
991
I already submitted this question under scope of practice when perhaps it should have been categorized as "other". I am very concerned that as a district employee I am being told to fill out 1099 and W-9 tax forms in order to be able to "refer" for the school medicaid program. I am not self-employed nor am I a sole proprietor. I also question the ethics of "referring" students/patients to ourselves. Do you have any input on this situation? Thanks
Constable Kay
991
Occupational Therapy
Our district OTs and PTs are being instructed to fill out 1099 and W-9 forms in order to be able to "refer" students to therapy that is funded by the school medicaid program and that is included in the IEP. This is a result of House bill 89. Is this legal and ethical? Are we referring patients to ourselves? Should we have to submit our personal tax information to Medicaid when we are not personally billing Medicaid? The district is billing medicaid and we are not contractors-we are district employees. Thanks!
DRAFT
Miller Kim
OT-02668
Occupational Therapy
I was curious if the Board has a stance on the new Medicaid changes from House Bill 89 (that permit school district providers to begin serving as the ordering/referring providers in the Ohio Medicaid School Program for next school year)? The emails I have received from our Medicaid billing agency and my district come off as no big deal to submit the requested tax forms. I am not getting much of an explanation on anything yet. It worries me that it will cause a significant increase in workload, as well as, personal liability. Thank you for your time, Kim Miller OT OT-02668
DRAFT

Hill Lauren
OT. 007591
Occupational Therapy
Hello, I wanted to gain a better understanding of OT's scope of practice in visual assessment and visual therapy (neuro-visual in particular). I want to provide an in-service to fellow OT's on proper vision screening during our evaluation (acute and inpatient rehab) and ways to incorporate visual re-training in our practice. For example, demonstrating treatment ideas for homonymous hemianopsia or left visual field cut. Please advise at what point do we need to contact an ophthalmologist or visual specialist if the patient is in the acute stroke stage? Thank you, Lauren Hill, OTR/L, CSRS
DRAFT

March Lisa
8381
Occupational Therapy
Hello, I am looking for clarification regarding if medication reconciliation including medication eduation in the home is within the scope of practice for Occupational Therapists and Occupational Therapy Assistants. Thank you for your assistance.
DRAFT

Good afternoon, I wanted to see if there is any information that states an Occupational Therapist cannot directly supervise a COTA that is a relative? Any assistance would be greatly appreciated. Thank you, Lori Summers
Lori Summers Compliance Manager Alternate Solutions Health Network
Office: 937-298-1111,1217 Mobile: 937-572-8746
1251 East Dorothy Lane Kettering, OH 45419 [email protected] www.ashomecare.com
DRAFT
Zeiger Marcia
OT-02463
Occupational Therapy, Occupational Therapy Assistant
Are there any regulations or restrictions in Ohio OT practice related to a sibling being the supervising OT to a COTA? I have looked through the practice acts and FAQ's and did not see anything regarding this, but wanted to check for sure. Thank you, Marcia Zeiger, OTR/L
The OT Practice Act is silent on this matter.
DRAFT

Winkel Marilyn
Occupational Therapy, Occupational Therapy Assistant
We have a question pertaining to therapists/assistants completing one-time home assessments. For a therapist/assistant that is licensed in and working in a SNF in KY, IN, MI (and the SNF bills the claims out of those states) --- In order to complete a home assessment (in preparation for discharge to home) for a resident of the SNF whose home is in Ohio, does the therapist/assistant need an Ohio license? Thank you! Marilyn Winkel, MS, OTR Director of Clinical Support Paragon Rehabilitation
Yes, a therapist would need an Ohio OT license if they are coming into the State to complete a home
assessment.
It is the position of the Ohio Occupational Therapy Section that an occupational therapy practitioner is required to hold a valid, current license in the State of Ohio to serve any clients residing in Ohio. Therefore, out of state occupational therapy personnel must hold a valid Ohio license to treat clients in Ohio.
DRAFT

From: Mary Renick [mailto:[email protected]]
Sent: Tuesday, May 09, 2017 11:46 AM
To: Adams, Jennifer [email protected]
Subject: Re: OT Section
Hi Jennifer,
Can an OT evaluate for Sensory Processing issues? Or, does that diagnosis need to be determined by an
MD?
Thank you!
DRAFT

Williams Michelle
005178
Occupational Therapy Assistant
I have two questions Does a co treatment need to be in a POC to cotreat? Does a assistant need to ask permission from a therapist to co treat?
DRAFT
Henry Pam
3526
Occupational Therapy
I had mailed an question ~ 6 weeks ago re: ethical practice. I originally thought I would be able to attend the board meeting tomorrow, however I am not. Could the board e-mail me their response on the decision to expand the law on professional behavior (Please call 513-505-9258 if clarification needed for my letter)? Thanks! Pam Henry, MHS, OTR/L
DRAFT

Ferguson Ruby
5527
Occupational Therapy, Physical Therapy, Physical Therapy Assistant
I am currently a DOR at a long term care facility. I am trying to find information regarding how many COTA's an OT can supervise at a time. The OT currently travels between 3 facilities. Also, I need information regarding the amount of PTA's a PT can supervise as he travels 3 facilities as well. Thank you for your time. Ruby Ferguson, DOR/PTA
DRAFT

Heisman S E
000315
Occupational Therapy
If a PRN OT forgets a TX note, but has billed, must she return to write the note, or may fulltime OT indicate she has "received written info from PRN OT and she completed the following Rx......"
DRAFT

Poffenbarger Sheri
PT008828
Can an OT cosign notes for dates prior to them physically starting employment
DRAFT
Mullen Sharlene
OTA 02240
Occupational Therapy Assistant
I was told by the my supervising occupational therapist that I am not permitted to use the word "splint" referring to resting hand splints or any type of splint in my documentation. I now have to use the word orthotic. Is this accurate. Thank you. Sharlene Mullen COTA/L
It is not within the jurisdiction of the Occupational Therapy Section to render billing and reimbursement
advice. The Section recommends that you refer to payer policies for any specific billing and
reimbursement requirements in your setting. You might also contact the Ohio Occupational Therapy
Association, or the Reimbursement Department of the American Occupational Therapy Association.
In accordance with section 4755.04 (A)(5) of the Ohio Revised Code, it is the position of the Occupational Therapy Section that occupational therapy practitioners Designing, fabricating, applying, recommending, and instructing in the use of selected orthotic or prosthetic devices and other equipment which assists the individual to adapt to the individual’s potential or actual impairment; in the provision of occupational therapy services provided that the occupational therapy practitioner demonstrates and documents competency in the modality, in accordance with rule 4755-7-08 of the Administrative Code, and is practicing within the occupational therapy scope of practice. If the modality will be administered by an occupational therapy assistant both the supervising occupational therapist and occupational therapy assistant must document and demonstrate competency in the techniques or modality.
DRAFT

Wolke Sophia
007493
Occupational Therapy, Occupational Therapy Assistant
If a site has a specific OT assessment (initial/annual), are COTA's able to meet with clients/patients to complete some of the assessment (background information, education, health, family history/support, ADL's, and self-care)? The OTR then collaborates with COTA and completes the summary, recommendations (including objective and interventions), and any other final items. Would this be in compliance with our laws? Thanks! Sophy Wolke
DRAFT
fleckenstein susan
n/a
Good afternoon My colleagues and I are starting a new home health agency and would like to know the process for informing you of our intentions.We intend to offer PT and OT services. Thank you for your time. Susan Fleckenstein RN, MS [email protected] or [email protected]
DRAFT

Barrington Tammy
Occupational Therapy, Occupational Therapy Assistant, Athletic Trainer
Can you please clarify the education requirements for OT? The application seems to state that an Associates Degree, Certification, B.S., and higher education are all acceptable forms to take the board exam. I understand that the AT is still a B.S. or Master's degree, and that the CAATE is changing the format by 2022. Thank you for your time and assistance in answering these questions as they will help determine which route to take. Sincerely, Tammy
OT: Master Degree or Doctorate Degree OTA: Associates Degree
DRAFT

From: Brenda George, MS, OTR/L [mailto:[email protected]] Sent: Thursday, May 04, 2017 12:36 PM To: Ball Beth <[email protected]>; Tanner, Tony <[email protected]> Cc: [email protected]; Finni Becky <[email protected]>; Stephens Angie <[email protected]>; Kessler Rachel <[email protected]>; [email protected]; dhurley@capitol‐consulting.net; djones@capitol‐consulting.net Subject: Fw: MSP enrolment requirements and code of ethical conduct
TO THE ATTENTION OF THE OT SECTION OF THE OTPTAT LICENSURE BOARD;
I am in receipt of the most recent attempts by Ohio Department of Medicaid (ODM) to modify their Independent Medicaid Provider application to “fit “ for the school based OT Practitioner. Please attached.
Our concern, specific to the Independent Medicaid Provider Enrollment, is that school based practitioners are being required by ODM/ODE as part of the Medicaid School Program (MSP) to complete an application that places the OT practitioner’s ethics at risk.
To provide service to students in schools settings, in compliance with IDEA federal regulation and Ohio Operating Standards, an OT has an additional license from the Ohio Department of Education and does not have to have a prescription.
Please realize that the Independent Medicaid Provider Enrollment application is only needed so that the school district (who is the Medicaid provider) may participate in the MSP program and so that the billing agent may submit billing to ODM. This Independent Medicaid Provider Enrollment is one of two options the school district has in order to participate in the MSP. The other option is to obtain an Rx from a doctor, nurse practitioner, physician assistant, etc. who is an outside ORP only provider.
My question to the Section: Is the content and response requirements of the attached Independent Medicaid Provider Enrollment application compliant with the code of ethical conduct( 4755‐7‐08)?
Thank you for your prompt reply, as ODM is wanting to post this on their portal immediately.
Brenda M. George, MS, OTR/L Ohio Occupational Therapy Association Pediatric Coordinator Legislative Committee
From: LESLEY.SCOTT‐[email protected] Sent: Thursday, May 04, 2017 10:38 AM To: Brenda George, MS, OTR/L ; [email protected] Cc: [email protected] ; [email protected] ; [email protected] ; [email protected] Subject: RE: MSP questions‐‐one more please
Hey Ladies, we want to get this out today, but wanted to make sure that we captured what is needed based on the feedback that you gave.
Can you let me know your thoughts, ASAP?
Thanks!
Agenda 8.1

How to enroll as a provider in the Ohio Medicaid program Guidance for Physical Therapists (PT), Occupational Therapists (OT), Speech Language Pathologists (SLP), and Audiologists working under a
Medicaid School Program (MSP) May 2016
House Bill 89 (HB89), authorized PT/OT/SLP and Audiology practitioners to make referrals for certain services
under the Medicaid School Program (MSP). In order to make a referral for a service, such practitioners are
required to enroll with the Ohio Department of Medicaid (ODM) and have an active provider agreement. This
guide includes step‐by‐step instructions for completing the provider enrollment application and offers specific
guidance for the practitioners impacted by HB89.
For dates of service July 1, 2017 and after, the National Provider Identifier (NPI) of the practitioner who
referred a therapy service under MSP will be required on claims submitted to ODM for reimbursement.
Practitioners impacted by HB89 are encouraged to start the provider enrollment application as soon as
possible to ensure claim payment is not disrupted. To ensure no delays in processing, provide all required
information at the time of application. When an incomplete application is submitted to ODM, it will be
returned to the applicant to provide the missing information.
To complete the enrollment application, you must provide the following identifying information:
‐ Your Social Security Number (SSN)
‐ Your National Provider Identifier (NPI)
‐ Your Medicare Provider ID (If applicable)
Formatted: Font: 12 pt

Ohio Department of Medicaid 2
Figure 1: ENROLL AS A PROVIDER
Access the Provider Enrollment Portal:
https://portal.ohmits.com/Public/Providers/Enrollment/tabId/44/Default.aspx
Select “I need to enroll as a provider to bill Ohio Medicaid”
o PT/OT/ST and Audiology practitioners are not eligible to enroll with Ohio Medicaid as
“ORP Providers” because they cannot order or prescribe services. The “ORP Provider”
designation is only for physicians and other prescribers who have the full professional
scope to order, refer, and prescribe services for Medicaid covered individuals.
Click on “new application” button and proceed to next screen

Ohio Department of Medicaid 3

Ohio Department of Medicaid 4
Figure 2: “REQUEST TYPE” Panel
Select “Individual Practitioner” from the “enrollment Type” drop down Menu
Select “Initial Enrollment” from the “Action Request” drop down Menu

Ohio Department of Medicaid 5
Figure 3: “REQUEST TYPE” Panel
Select appropriate provider type from the drop‐down menu:
o Physical Therapist: 39 – Physical Therapist, Individual
o Speech Therapist: 40 – Speech and Language Pathologist Individual
o Occupational Therapist: 41 – Occupational Therapist, Individual
o Audiologist: 43 – Audiologist Individual
Select the “Yes” radial button for the question “Are you a provider new to Ohio Medicaid?”
Click “Next”
IMPORTANT NOTE: Record your Application Tracking Number (ATN)! If you do not complete and submit
the application within 72 hours, the application will be purged from the system and you will need to start a
new application.
Ohio Department of Medicaid 6
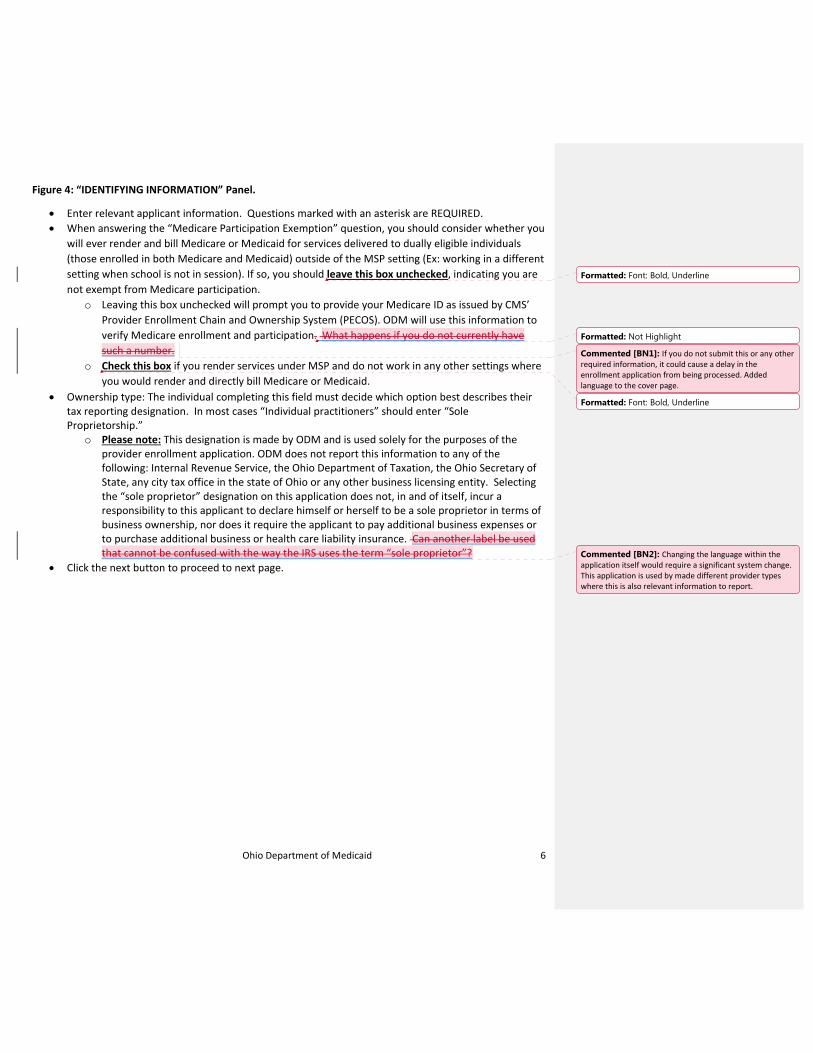
Figure 4: “IDENTIFYING INFORMATION” Panel.
Enter relevant applicant information. Questions marked with an asterisk are REQUIRED.
When answering the “Medicare Participation Exemption” question, you should consider whether you
will ever render and bill Medicare or Medicaid for services delivered to dually eligible individuals
(those enrolled in both Medicare and Medicaid) outside of the MSP setting (Ex: working in a different
setting when school is not in session). If so, you should leave this box unchecked, indicating you are
not exempt from Medicare participation.
o Leaving this box unchecked will prompt you to provide your Medicare ID as issued by CMS’
Provider Enrollment Chain and Ownership System (PECOS). ODM will use this information to
verify Medicare enrollment and participation. What happens if you do not currently have
such a number.
o Check this box if you render services under MSP and do not work in any other settings where
you would render and directly bill Medicare or Medicaid.
Ownership type: The individual completing this field must decide which option best describes their tax reporting designation. In most cases “Individual practitioners” should enter “Sole Proprietorship.”
o Please note: This designation is made by ODM and is used solely for the purposes of the provider enrollment application. ODM does not report this information to any of the following: Internal Revenue Service, the Ohio Department of Taxation, the Ohio Secretary of State, any city tax office in the state of Ohio or any other business licensing entity. Selecting the “sole proprietor” designation on this application does not, in and of itself, incur a responsibility to this applicant to declare himself or herself to be a sole proprietor in terms of business ownership, nor does it require the applicant to pay additional business expenses or to purchase additional business or health care liability insurance. Can another label be used that cannot be confused with the way the IRS uses the term “sole proprietor”?
Click the next button to proceed to next page.
Formatted: Font: Bold, Underline
Formatted: Not Highlight
Commented [BN1]: If you do not submit this or any other required information, it could cause a delay in the enrollment application from being processed. Added language to the cover page.
Formatted: Font: Bold, Underline
Commented [BN2]: Changing the language within the application itself would require a significant system change. This application is used by made different provider types where this is also relevant information to report.

Ohio Department of Medicaid 7
Figure 4:
Formatted: Font: 12 pt, Bold
Formatted: Font: 12 pt, Bold

Ohio Department of Medicaid 8
Figure 5: “TAX ID – 1099 INFORMATION” Panel
Please enter all required fields.
Under State and Federal law, all applicants are required to provide their individual social security
number, complete the 1099 information and submit a completed W‐9 form. All information is kept
confidential within MITS and is not part of any publicly available provider lists.
Ohio Medicaid requires the completion of the 1099 Tax ID Information for all applicants. If you never
bill to Medicaid directly, you will not receive a 1099. Medicaid is required to send a 1099 only if the
individual practitioner submits claims and is paid more than $600 in a given tax year.
Figure 6: “DEA” Panel
This does not apply to PT/OT/SLP or Audiologists
Click “next”
Figure 7: “DEA” Panel, continued
This does not apply to PT/OT/SLP or Audiologists
Click “next”

Ohio Department of Medicaid 9
Figure 8: “DEA” Panel error message
OOPS! I added a line on the DEA page by mistake, how do I remove it?
Figure 9: Now it won’t let me continue without putting in DEA information
Figure 10: Select the empty line and click “delete button to remove”
Ohio Department of Medicaid 10
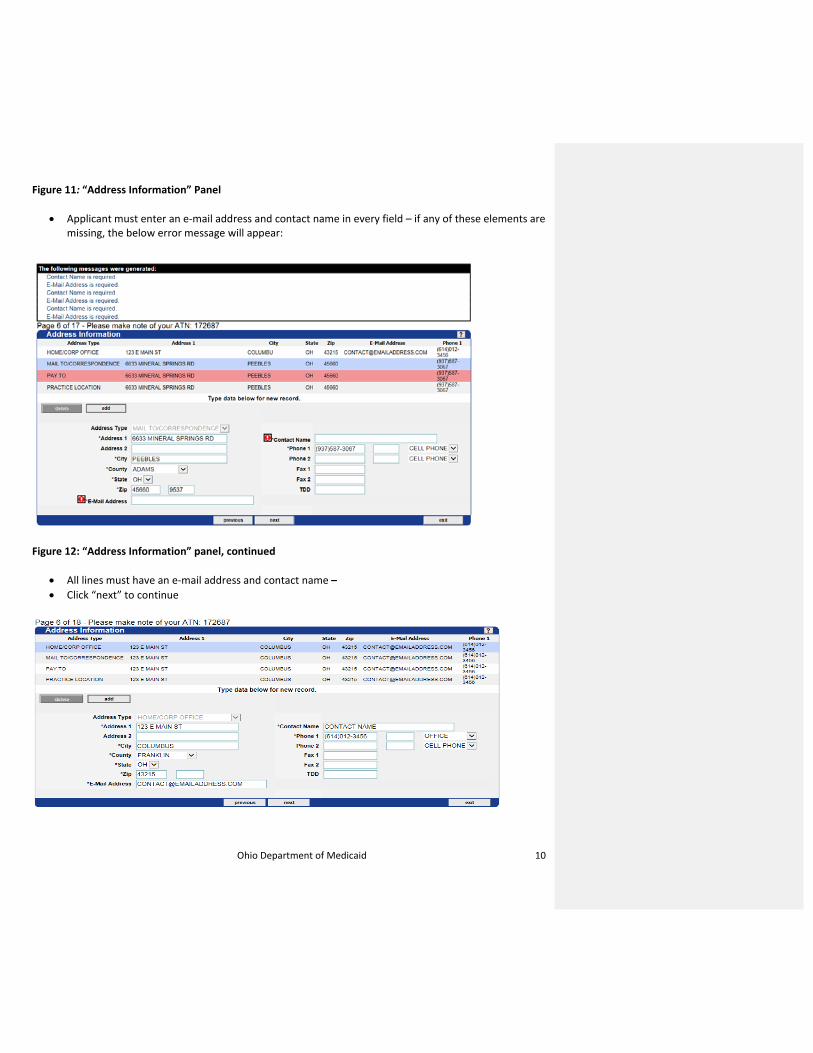
Figure 11: “Address Information” Panel
Applicant must enter an e‐mail address and contact name in every field – if any of these elements are missing, the below error message will appear:
Figure 12: “Address Information” panel, continued
All lines must have an e‐mail address and contact name –
Click “next” to continue

Ohio Department of Medicaid 11
Figure 13: “TYPE AND SPECIALTY” Panel
Select a specialty from the drop‐down menu and check the “primary specialty” box.
NOTE: Select a primary specialty that corresponds with your provider type: ‐ Physical Therapist: 391 – Physical Therapy. ‐ Occupational Therapist: 410 – Occupational Therapy ‐ Speech Therapist: 400 – Speech and Language Pathology ‐ Audiologist: 430 ‐ Audiology
Formatted: Font: 12 pt

Ohio Department of Medicaid 12
Figure 14: “LANGUAGE PANEL”
SELECT LANGUAGE
Figure 15: “GROUP AFFILIATIONS” Panel
NOTE: Do not complete this panel. Physical Therapists, Occupational Therapists, Speech Language
Pathologists, and Audiologists who are employed by a school and provide services under the
Medicaid Schools Program (MSP) are not required to affiliate with the MSP provider. are not
required to affiliate. Affiliation needs to be explained
Formatted: Font: Bold, Underline
Formatted: Font: Bold, Underline
Commented [BN3]: These practitioners are not required to affiliate at this time.
Formatted: Font: Bold, Underline
Formatted: Font: Bold, Underline
Formatted: Highlight
Ohio Department of Medicaid 13
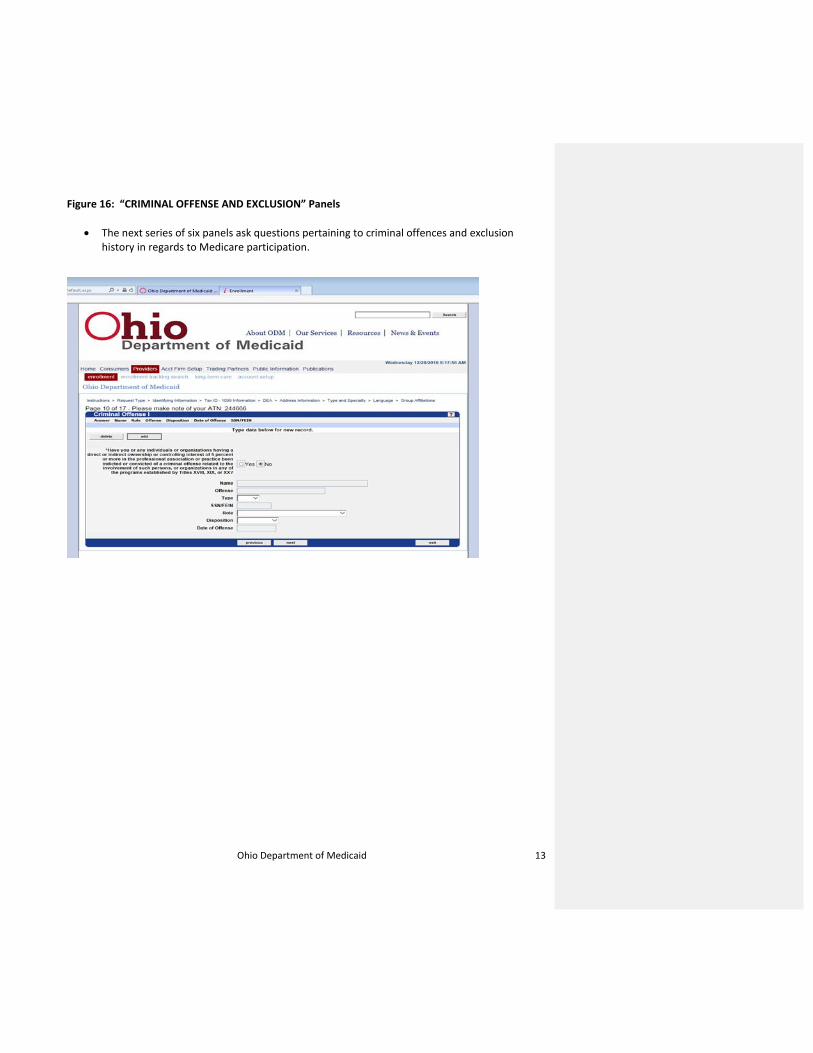
Figure 16: “CRIMINAL OFFENSE AND EXCLUSION” Panels
The next series of six panels ask questions pertaining to criminal offences and exclusion history in regards to Medicare participation.

Ohio Department of Medicaid 14
Figure 17: “CERTIFICATION’ Panel
Applicant must accept the terms and conditions
Email address is required if “Email” was selected as preferred contact method
“Legal Entity Name” should be the individual practitioner’s name

Ohio Department of Medicaid 15
Figure 18: “Terms and Conditions” panel
Initially only 3 terms are visible
Applicant must drag the scroll bar down to the bottom and indicate they have read all 16 terms
Figure 19: “Terms and Conditions” panel, continued
Applicant must accept/attest that the application is true and complete
IMPORTANT – ELECTRONIC SIGNATURE MUST BE THAT OF THE APPLICANT

Ohio Department of Medicaid 16
Figure 20: Provision Check box for retroactive billing.
Please read instructions for eligibility

Ohio Department of Medicaid 17
Figure 21: “Document Submission Type and Notes” Panel.
Select the method of how you would like to submit required documents
Figure 22: “Document Submission Type and Notes” panel
Document upload may take 1‐2 minutes to complete
Ohio Department of Medicaid 18
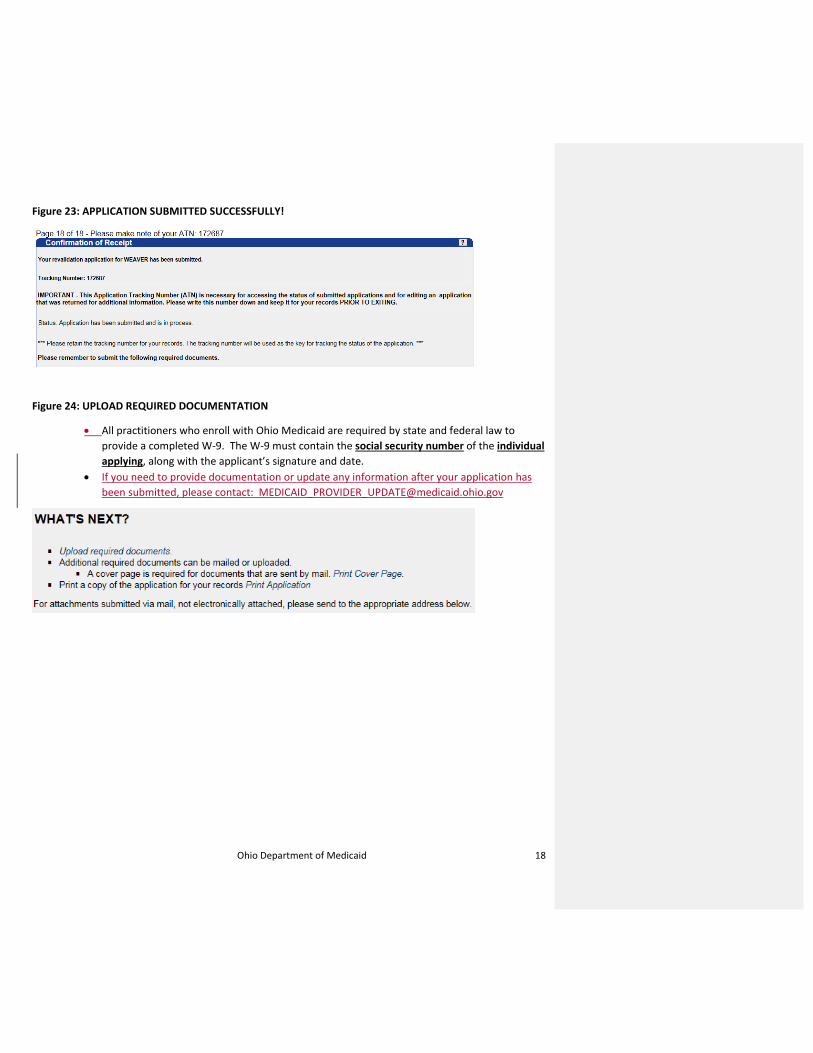
Figure 23: APPLICATION SUBMITTED SUCCESSFULLY!
Figure 24: UPLOAD REQUIRED DOCUMENTATION
All practitioners who enroll with Ohio Medicaid are required by state and federal law to
provide a completed W‐9. The W‐9 must contain the social security number of the individual
applying, along with the applicant’s signature and date.
If you need to provide documentation or update any information after your application has
been submitted, please contact: [email protected]
1
Moore, Diane
From: Delaserda, JenniferSent: Monday, May 08, 2017 11:13 AMTo: Delaserda, Jennifer; Johnson, FreddieSubject: BWC Medical Rules for feedbackAttachments: OAC 4123-6-32 Payment for lumbar fusion surgery.pdf; OAC 4123-6-02.3 certification
criteria.pdf; OAC 4123-6-01.2 pilot program rule revised.pdf
Dear Stakeholders: BWC seeks your comments and feedback on three proposed rules.
We have completed a review of the attached Ohio Administrative Code (OAC) 4123‐6‐32, lumbar fusion surgery rule; OAC 4123‐6‐02.3, provider application and certification criteria rule; and OAC 4123‐6‐01.2, provisional treatment pilot program rule. Per the review, we propose changes to these rules. How to submit your feedback
We have created an email box for you to provide your feedback. Please submit your comments to: [email protected]. Please include contact information with your name, phone number, email address and practice and/or specialty, if applicable.
We will accept comments through May 26, 2017.
Thank you for providing quality services to Ohio’s injured workers. We look forward to hearing from you.
1
OAC 4123-6-32 Payment for lumbar fusion surgery
Effective November 1, 2017, reimbursement for lumbar fusion surgery for treatment of allowed conditions in a claim resulting from an allowed industrial injury or occupational disease shall be limited to claims in which current best medical practices as implemented by this rule are followed.
This rule governs the bureau's reimbursement of lumbar fusion surgery to treat a work related injury or occupational disease. It is not meant to preclude, or substitute for, the surgeon's responsibility to exercise sound clinical judgment in light of current best medical practices when treating injured workers.
A provider's failure to comply with the requirements of this rule may constitute endangerment to the health and safety of injured workers, and claims involving lumbar fusion surgery not in compliance with this rule may be subject to peer review by the bureau of workers' compensation stakeholders' health care quality assurance advisory committee (HCQAAC) pursuant to rule 4123-6-22 of the Administrative Code or other peer review committee established by the bureau.
(A) Prerequisites to consideration of lumbar fusion surgery.
Authorization for lumbar fusion shall be considered only in cases in which the following criteria are met:
(1) Conservative care.
(a) Except as otherwise provided in paragraph (A)(1)(c) of this rule, the injured worker must have had at least sixty days of conservative care for low back pain, with an emphasis on:
(i) Physical reconditioning;
(ii) Avoidance of opioids, when possible; and
(iii) Avoidance of provider catastrophizing the explanation of lumbar MRI findings.
(b) The injured worker’s comprehensive conservative care plan may include, but is not limited to, one or more of the following:
(i) Rest / ice / compression / elevation (RICE);
(ii) Anti-inflammatories;
(iii) Pain management / physical medicine rehabilitation program;

2
(iv) Chiropractic / osteopathic treatment;
(v) Physical / occupational therapy;
(vi) Interventional spine procedures / injections.
(c) The requirement of a trial of at least sixty days of conservative care prior to consideration of lumbar fusion surgery may be waived with prior approval from the MCO in cases of:
(i) progressive functional neurological deficit;
(ii) spinal fracture;
(iii) tumor;
(iv) infection;
(v) emergency / trauma care; and/or
(vi) other catastrophic spinal pathology causally related to the injured worker’s allowed conditions.
(2) The operating surgeon requesting authorization for lumbar fusion surgery must have personally evaluated the injured worker on at least two occasions prior to requesting authorization for lumbar fusion surgery.
(3) The injured worker must have undergone a comprehensive evaluation, coordinated by both the injured worker’s physician of record or treating physician and the operating surgeon, in which all of the following have been documented:
(a) Utilization and correlation of all of the following tools:
(i) Visual analog scale (VAS);
(ii) Pain diagram;
(iii) Oswestry low back disability questionnaire.
(b) A comprehensive orthopedic / neurological examination, including documentation of all of the following categories:
(i) Gait;
(ii) Spine (deformities, range of motion, palpation);

3
(iii) Hips and sacroiliac joints;
(iv) Motor;
(v) Sensation;
(vi) Reflexes;
(vii) Upper motor neuron signs.
(c) Diagnostic testing.
(i) Lumbar X-rays (including flexion/extension views), lumbar MRI, or lumbar CT (with or without myelography) must be performed;
(ii) Electromyography (EMG) / nerve conduction study (NCS) may be performed if questions still remain during surgical planning.
(d) Vocational assessment and consideration for vocational rehabilitation.
(e) Review of current and previous medications taken.
(i) If opioid management is in process, review for best practices;
(ii) Consider impact of surgery on opioid load.
(f) Health behavioral assessment (pre-surgical). Biopsychosocial factors that may affect treatment of the injured worker’s allowed lumbar conditions are considered modifiable conditions that may improve surgical outcomes if appropriately addressed, and must be addressed if identified in the assessment.
(g) Accounting and assessment of the following co-morbidities to stratify additional associated risks:
(i) Smoking;
(ii) Body mass index (BMI);
(iii) Diabetes;
(iv) Coronary artery disease;
(v) Peripheral vascular disease.

4
The co-morbidities indicated above are considered modifiable conditions that may improve surgical outcomes if appropriately addressed, and must be addressed if identified in the assessment.
(h) The injured worker, the physician of record or treating physician, and the operating surgeon must have reviewed and signed the educational document, “What BWC Wants You to Know About Lumbar Fusion Surgery,” attached as an appendix to this rule.
(B) Authorization for lumbar fusion surgery where the injured worker has no prior history of lumbar surgery.
(1) Authorization for lumbar fusion shall be considered in cases where the injured worker has no prior history of lumbar surgery only when the injured worker remains highly functionally impaired despite a trial of at least sixty days of conservative care as provided in paragraph (A)(1)(a) of this rule (unless waived with prior approval by the MCO pursuant to paragraph (A)(1)(c) of this rule) and one or more of the following are present:
(a) Mechanical low back pain with instability of the lumbar segment and no history of lumbar surgery.
(b) Spondylolisthesis of twenty-five per cent or more with one or more of the following:
(i) Objective signs/symptoms of neurogenic claudication;
(ii) Objective signs/symptoms of unilateral or bilateral radiculopathy, which are corroborated by neurologic examination and by MRI or CT (with or without myelography);
(iii) Instability of the lumbar segment.
(c) Lumbar radiculopathy with stenosis and bilateral spondylolysis.
(d) Lumbar stenosis necessitating decompression in which facetectomy of greater than or equal to fifty per cent or more is required.
(e) Primary neurogenic claudication and/or radiculopathy associated with lumbar spinal stenosis in conjunction with spondylolisthesis or lateral translation of 3mm or greater or bilateral pars defect.
(f) Degenerative disc disease (DDD) associated with significant instability of the lumbar segment.
5
(g) Spinal stenosis, disc herniation, or other neural compressive lesion requiring extensive, radical decompression with removal of greater than fifty per cent of total facet volume at the associated level.
The surgeon must document why the surgical lesion would require radical decompression through the pars interarticularis (critical stenosis, recurrent stenosis with extensive scarring, far lateral lesion).
(2) For purposes of this paragraph, instability of the lumbar segment is defined as at least 4mm of anterior/posterior translation at L3-4 and L4-5, or 5mm of translation at L5-S1, or 11 degrees greater end plate angular change at a single level, compared to an adjacent level.
(C) Request for lumbar fusion surgery where the injured worker has a history of prior lumbar surgery.
(1) If a trial of at least sixty days of conservative care as provided in paragraph (A)(1)(a) of this rule has failed to relieve symptoms (or has been waived with prior approval by the MCO pursuant to paragraph (A)(1)(c) of this rule) and the injured worker has had a prior laminectomy, discectomy, or other decompressive procedure at the same level, lumbar fusion should be considered for approval only if the injured worker has one or more of the following:
(a) Mechanical (non-radicular) low back pain with instability at the same or adjacent levels.
(b) Mechanical (non-radicular) low back pain with pseudospondylolisthesis, rotational deformity, or other condition leading to a progressive, measureable deformity.
(c) Objective signs/symptoms compatible with neurogenic claudication or lumbar radiculopathy that is supported by EMG/NCS, lumbar MRI, or CT and detailed by a clinical neurological examination in the presence of instability of 3mm lateral translation with at least two prior decompression surgeries at the same level.
(d) Evidence from post laminectomy structural study of either:
(i) One hundred per cent loss of facet surface area unilaterally; or
(ii) Fifty per cent combined loss of facet surface area bilaterally.
(e) Documented pseudoarthrosis or nonunion, with or without failed hardware, in the absence of other neural compressive lesion.

6
(2) For purposes of this paragraph, instability of the lumbar segment is defined as at least 4mm of anterior/posterior translation at L3-4 and L4-5, or 5mm of translation at L5-S1, or 11 degrees greater end plate angular change at a single level, compared to an adjacent level.
(D) Lumber fusion surgical after care.
Both the physician of record or treating physician and the operating surgeon must follow the injured worker until the injured worker has reached maximum medical improvement (MMI).
(1) In the first six months post-operatively, the injured worker must be seen by both the physician of record or treating physician and the operating surgeon at least every two months to monitor the injured worker’s progress, rehabilitation needs, behavioral patterns or changes, and return to work willingness and/or status.
During this period, the physician of record or treating physician and the operating surgeon shall determine the following:
(a) Fusion status;
(b) Pain and functional status;
(c) MMI status of injured worker;
(d) Residual level of functional capacity;
(e) Appropriateness for vocational rehabilitation.
(2) From six months to one year post-operatively, if the injured worker continues to experience significant functional impairment despite the lumbar fusion, the following actions are recommended:
(a) Pain and functional status (repeat VAS / pain diagram / Oswestry)
(b) Repeat baseline orthopedic / neurological examination;
(c) Repeat health behavioral assessment;
(d) Revisit appropriate diagnostic imaging.
(e) Coordinate with MCO to develop a plan of care / return to functional status.
7
Effective: 11/01/2017 R.C. 119.032 review dates: 11/17/09 Promulgated Under: 119.03 Statutory Authority: 4121.12, 4121.121, 4121.30, 4121.31, 4123.05 Rule Amplifies: 4121.121, 4121.44, 4121.441, 4123.66

8
Appendix to rule OAC 4123-6-32
What BWC Wants You to Know About Lumbar Fusion Surgery
(Applies to all workers considering lumbar fusion, regardless of diagnosis)
Ohio Bureau of Workers’ Compensation wants you to have the highest quality of care. That can only occur if you know how lumbar fusion surgery may affect your health and recovery. BWC is providing the following instructional form to aid in the process. BWC requires your physician to discuss this information before the surgery, so you can make the best informed decision. In preparation, please study this form, and discuss the information with your healthcare team. Afterwards, you, your physician of record, and your operating surgeon should sign the form. THIS IS NOT A SURGICAL CONSENT FORM.
Studies have shown the following post-operative outcomes:
The chance of an injured worker no longer being disabled 2 years after lumbar fusion is 32%.
More than 50% of workers who received lumbar fusion through the Washington workers’ compensation program felt that both pain and functional recovery were no better or were worse after lumbar fusion.
Smoking at the time of fusion greatly increases the risk of failed fusion
Pain relief, even when present, is NOT likely to be 100%
The use of spine stabilization hardware (metal devices) in Washington workers nearly doubled the chances of having another surgery
Lumbar fusion for the diagnoses of disc degeneration, disc herniation, and/or radiculopathy in work comp setting is associated with significant increase in disability, opiate use, prolonged work loss, and poor return to work status.
Ohio Fusion Outcomes: (2 year follow-up – 1450 total patients)
a. Back pain patients treated with fusion were able to return to work (activity) only 26% of the time, workers treated non-surgically were able to return to work (activity) 67% of the time.

9
b. Re-operation rate was 27% in fused patients
c. Complications occurred in 36% of fused patients
d. Narcotic use increased 41% in fused patients, and continued for over 2 years in 76% of fused patients
e. 17 of the fused patients died during the course of the study and 11 non-surgical patients
National/International Fusion Statistics
a. Surgical fusion outcomes are NOT better than cognitive therapy and exercise
b. Surgical fusion for previous herniated disk is NOT better than non-operative treatment
c. Surgical satisfaction was reportedly high even in injured workers with ongoing pain and no improvement in function observed
d. Some patients described less pain, improvement of 1 or 2 points on a 10 point pain scale, but any functional benefit of having a fusion was not demonstrated
Opioid use has been associated with significant long term morbidity and mortality in both surgical and non-surgical patients. Back pain patients are at risk for long term opioid use. Fusion patients have greater narcotic/opioid usage than non-operative patients.

10
What is expected of you if you proceed to have lumbar fusion surgery:
If the BWC/MCO authorizes your surgery, your surgeon will continue to see you at least every two months for six months after surgery. As your surgeon, I expect you to actively participate in your recovery and rehabilitation plan both prior to and following your surgery. If you continue to have pain after your surgery and I cannot find a medical reason for it, the BWC/MCO may not continue to pay and/or authorize further medical care.
By signing this form, we (the injured worker, physician & surgeon), attest that we have discussed the information presented here, we understand this information, and we wish to proceed with the fusion surgery. We also understand that this information does NOT take place of, and is separate and distinct from, any surgical form that we will complete prior to surgery.
_____________________________ __________________________________
Injured Worker Physician of Record
Date:___/____/_______ Date:____/______/__________
_____________________________
Operating Surgeon
Date:____/______/________

1
4123-6-02.3 Provider access to the HPP - provider application and certification criteria.
(A) The bureau shall make available to each provider a provider certification application and agreement or recertification application and agreement, as applicable, which shall require the provider to furnish documentation as provided in rule 4123-6-02.2 of the Administrative Code.
(B) The provider application and agreement or recertification application and agreement shall require the provider to make statements that the provider is without impairments that would interfere with the provider's ability to practice or that would jeopardize a patient's health, and a statement that the application is without misrepresentation, misstatement, or omission of a relevant fact or other acts involving dishonesty, fraud, or deceit. The provider shall provide to the bureau any additional documentation requested, and shall permit the bureau to conduct a review of the provider's practice or facility. The provider shall notify the bureau within thirty days of any change in the provider's status regarding any of the credentialing criteria of paragraph (B) or (C) of rule 4123-6-02.2 of the Administrative Code.
(C) The bureau shall review the application and agreement and all documentation submitted by the provider. The bureau may cross-check data with other governmental agencies or licensing bodies. The bureau may refer provider certification and malpractice issues to the bureau's stakeholders health care quality assurance advisory committee for review as provided under rule 4123-6-22 of the Administrative Code.
(D) By signing the provider application and agreement or recertification application and agreement, the provider agrees to, and the bureau may refuse to certify or recertify or may decertify a provider for failure to:
(1) Provide health services that are applicable to a work-related injury, and not to substantially engage in the practice of experimental modalities of treatment.
(2) Acknowledge and treat injured workers in accordance with bureau recognized treatment guidelines.
(3) Acknowledge and treat injured workers in accordance with the vocational rehabilitation hierarchy.
(4) Provide adequate on-call coverage for patients.
(5) Utilize bureau certified providers when making referrals to other providers.
2
(6) Timely schedule and treat injured workers to facilitate a safe and prompt return to work.
(7) Release information from the national practitioner data bank or the federation of state licensing boards. The bureau may submit a report to the appropriate state licensing board or data bank as required in the event the provider is decertified.
(8) Practice in a managed care environment and adhere to MCO and bureau procedures and requirements concerning provider compliance, outcome measurement data, peer review, quality assurance, utilization review, bill submission, and dispute resolution.
(9) Adhere to the bureau's confidentiality and sensitive data requirements, and use information obtained from the bureau by means of electronic account access for the sole purpose of facilitating treatment and no other purpose, including but not limited to engaging in advertising or solicitation directed to injured workers.
(10) Comply with the workers' compensation statutes and rules and the terms of the provider application and agreement or recertification application and agreement.
(E) Upon review and determination by the bureau that the provider has met bureau credentialing requirements, the bureau shall certify or recertify the provider as a bureau certified provider.
(F) The bureau may enter into an addendum to a physician’s provider certification application and agreement or recertification application and agreement, offering appropriate performance incentives to enhance physician proficiency in patient care and navigation of the Ohio workers’ compensation system, to physicians who agree to:
(1) Perform enhanced duties as the treatment team leader in the care of injured workers, as set forth in the addendum, and
(2) Enhanced provider outcome measurement.
Effective: 11/01/2017 Five Year Review (FYR) Dates: 08/26/2015 and 08/25/2020 Promulgated Under: 119.03 Statutory Authority: 4121.12, 4121.121, 4121.30, 4121.31, 4121.44, 4121.441, 4123.05 Rule Amplifies: 4121.12, 4121.121, 4121.44, 4121.441 Prior Effective Dates: 2/16/96, 1/15/99, 3/29/02, 2/14/05, 2/1/10, 11/13/2015

4123-6-01.2 Provisional treatment reimbursement approval - pilot program.
Notwithstanding any provision to the contrary in any other rule of the bureau, the administrator may, for purposes of a pilot program, allow one or more managed care organizations to authorize medical treatment reimbursement requests for the first sixty days from the initial allowance of an identified at-risk claim for any conditions within the same body part or parts as the conditions initially allowed in the claim, and presumed to be causally related to the same industrial injury or occupational disease, without disclaimer, during such time as the conditions for which treatment reimbursement is authorized but which are not yet allowed are being considered for allowance or being adjudicated.
The operation of the pilot program authorized under this rule shall not impair in any manner the right of an employer to appeal a claim, additional allowance, or medical treatment reimbursement determination under section 4123.511 of the Revised Code or rule 4123-6-16 of the Administrative Code.
The administrator may conduct the pilot program authorized under this rule for a period of one year from the effective date of this rule shall be extended through June 30, 2019; provided, however, that the administrator may terminate the pilot program early or, in the alternative, extend the pilot program for up to one additional year at the administrator's discretion.
Effective: 9/1/2017 Five Year Review (FYR) Dates: 07/01/2020 Promulgated Under: 119.03 Statutory Authority: 4121.12, 4121.121, 4123.66 Rule Amplifies: 4121.12, 4121.121, 4121.441 Prior Effective Date: 7/1/2015
Top Related