






Languages
Pages
Legal

C o l e e y e I n s t I t u t e
e l e C t r o n I C M e d I C a l r e C o r d s – read More
OphthalmologyUpdates p e C I a l e d I t I o n | 2 0 12
EMR

Dear Colleagues,Welcome to a very special edition of Cleveland Clinic Cole Eye Institute’s Ophthalmology Update. This issue delivers to you our perspective on the undeniable assimilation of electronic medical records (EMR) into the practice of ophthalmology.
In these pages, we provide you with a 360-degree view of what the integration of EMR means to our area of medicine. As a leading academic eye center, Cole Eye Institute is taking a national leadership role in adapting the technology advantages of EMR into improved clinical workflows, faster and easier documentation, and ultimately a better patient experience. Our practice has seen these benefits of this new system each and every day.
We’ve collected the perspectives of staff across our practice to bring you a closer look at the far-reaching implications of EMR. Some of those perspectives include:
• A view from our community practices, about connecting a smaller practice with a large one
• The perspective of a nurse who works in a high-volume practice, to teach about how the whole medical team works together to realize all the benefits that EMR has to offer, including how EMR helps optimize insurance reimburse-ments
• Details about the unique integration of imaging results into the EMR system
• A thought piece on how the vast amount of data now harvested as a result of EMR can be used to inform the future prac-tice of ophthalmology
• How all this interconnectivity facilitates our work with other specialists treating our com-mon patients for a variety of other conditions that may manifest themselves first in the ophthalmologist’s office
You will also find an update on the two-year results from the Comparison of AMD Treatments Trials (CATT). And you will find the other information that you have come to rely on from this publication, such as CME opportunities, our staff listing (including some new faces) and an overview of our staff’s recent publications. If you have additional thoughts on Ophthalmology Update, please do not hesitate to contact me at [email protected].
Sincerely,
Daniel F. Martin, MDCha IrMan , Cole eye Inst I tute

Defining what makes us different
4
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Electronic Medical Records: The Future Is Now
Like it or not, electronic medical record (EMR) systems are slated to become com-
monplace in ophthalmology over the next few years, regardless of practice setting,
geographic location and subspecialty focus. Our field in particular faces significant
obstacles to widespread adoption, based on the unique features of its practice. For
example, in just the management of age-related macular degeneration, monthly
patient visits are commonplace and result in the accumulation of large amounts
of diagnostic and procedural documentation over the lifetime of the patient. In ad-
dition, ophthalmologists are used to manual entry methods such as hand drawings
of pathology, which is poorly emulated in current EMR systems.
These obstacles and others are
the reasons why adoption of
EMR systems has been poor.
In 2006, the American Academy of
Ophthalmology’s (AAOs) survey of its
members found a 12 percent adoption
rate of an EMR system, compared with a
17 percent adoption rate for physicians
across all other medical specialties.
A reason often given for not adopting
EMR is the cost of implementing the
system. Health Information Technology
for Economic and Clinical Health’s $27
billion grant might help offset some of
these costs, but there is no textbook or
preferred practice pattern to go by on
how to begin this process.
At Cleveland Clinic, we have successful-
ly implemented an EMR system within
our practice. This discussion will focus
on the pearls of the process, such as
identifying essential functions to look
for in vendor products and tips on the
implementation process.
Both Sides of the Coin – The Pros
and Cons of Adoption
The addition of EMR has some signifi-
cant advantages. The level of compli-
ance with time stamps, procedure
documentation and security measures
increases greatly with EMR. Most
EMR systems have predefined docu-
mentation for common ophthalmic
procedures, and it’s important when
evaluating the system to compare
these to your local carrier or CMS
guidelines to see if they match up.
When under the scrutiny of an audit,
the EMR system can be a lifesaver.
Many EMR systems allow for the
documentation of normal values for
the specific eye fields, and compo-
nents can be globally modified with
a keystroke. For example, when an
audit showed another practice lacked
a particular exam component, we
could implement a change in the EMR
template within a day.
Having the records available anywhere
and anytime really helps with patient
care. According to the AAO, 45 percent
of ophthalmologists work in multiple
offices; when EMR is in place, patient
care is informed and updated regard-
less of location. Consequently, medical
record storage costs decline consider-
ably with EMR. When integrating values
such as intraocular pressure, corneal
thickness and other quantitative mea-
surements, the EMR permits trending
of patients over time, allowing for a
much more comprehensive evaluation
of disease progression. (see article on
page 12)
Finally, EMR allows for the determina-
tion of practice efficiencies and pitfalls.
For example, we can allocate clinic re-
sources such as space and tech coverage
based on reports on previous technician
and clinic performances. Our system
has been able to drill down to determine
how long technicians take to work up
By Rishi P. Singh, MD
5
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n n o v a t i o n s
patients and how long a procedure or
diagnostic procedure takes to perform.
But with as many advantages EMR offers,
there is a balance of significant draw-
backs. Whatever you think you will save
by converting from paper charts (storage
fees, personnel for records management)
will be offset by information technology
maintenance, high-speed Internet lines,
and electronic backup and storage. Ex-
pect monthly or yearly software upgrades
with the expected bugs, annoyances and
potential downtime. Keystroke entry is
virtually universal so you must be a pro-
ficient typist. The temporary decrease in
efficiency and lost revenue on the initial
implementation are sometimes too
much for practices to bear.
Choosing the Right System for You
The first item to consider when choosing
the proper system is to make sure that
you are receiving a government-certified
product (see cchit.org/find). Consider
whether to partner up or go it alone. Lo-
cal hospital systems may offer usage of
their EMR for a nominal charge, but few
have ophthalmic-ready systems. A better
option might be to share the cost of the
IT system or bargain collectively with
another nearby practice when dealing
with the EMR vendors.
When evaluating a system, determine
the level of customization needed.
Does the EMR mimic your workflow
or practice pattern? Do the items with-
in the EMR represent all the specialties
within your practice? Some EMRs are
specialty-specific even within ophthal-
mology. Finally, visit your colleagues
who have successfully implemented a
system to understand what their real
experience has been. We visited many
sites prior to finalizing our choice to
seek out the features and functions
that we wanted to implement within
our own system.
Putting Your System to Work
Choosing the right system is only half
of the job, and the implementation
can make or break your conversion.
Assembling a multidisciplinary team
composed of a physician, technician,
biller/coder and administrator is a
good first step. Walking through the
EMR workflow with this team can help
in troubleshooting early problems.
Consider choosing a lower-volume
time of year to make the switch, to
reduce the economic impact of the
implementation process.
We chose to down-book by 25 percent
for the two-week duration of the go-live
in order to give our physicians adequate
time to acquaint themselves with the sys-
tem. By bringing the clinical volume back
to normal levels quickly, we found that
many physicians began to employ work-
flow efficiencies in order to keep pace.
When considering big-bang rollouts
versus gradual implementations, we
chose a more gradual approach that al-
lowed us to troubleshoot the workflow,
off-load patients to another provider
and train technicians by rotating them
through the clinic prior to their go-live.
Scribes are an important consideration
for any practice. Every study performed
has shown that the utility of scribes
decreases significantly as the practice
becomes more familiar with the EMR
system. Thus, we chose to hire addi-
tional technicians to serve as physician
extenders within the clinic.
Conclusions
With all the pitfalls and efforts needed
to navigate the process, why would
practices choose to go forward? Having
three years of experience using Cleveland
Clinic’s EMR system has taught me how
invaluable it can be. Patient calls can
be answered quickly and efficiently. I’m
communicating more than ever with
referring and primary care physicians.
I can perform chart reviews and clinical
research studies within days and not
weeks. Lastly, patients have now come to
expect information on demand, which
EMR systems allow. This ready access
to their records has enabled patients to
become better partners in their care. ■
Contact Dr. Rishi P. Singh at [email protected].
Choosing the right system is only half of the job, and the implementation can make or break your conversion.

6
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Imaging Solutions in the Age of EMR
Ophthalmology is becoming more and more of an image-driven subspecialty.
Recent developments in diagnostic testing, such as optical coherence tomogra-
phy (OCT), guide management decisions and enhance our diagnostic capabilities.
This significant influx of testing can lead to information overload if the data is not
presented to the clinician and handled in an appropriate way. In many practices,
this may simply involve printing a report. However, the utility of printed reports is
limited because paper limits the accessibility and functionality of the reports. In
the age of EMR, an electronic image archiving and display system is the logical
solution for most practices.
Three common ophthalmology
imaging solution suites are
Zeiss FORUM,® Merge Eye Care
(OIS) and ANKA EyeRoute. These three
packages provide digital alternatives
for publishing reports from diagnostic
devices. Each of these systems has ad-
vantages and disadvantages. Function-
ality also continues to evolve with the
deployment of EMR. Many practices
converted to electronic image display
solutions long before converting to an
EMR system. The integration between
imaging solutions and EMR systems
is an active area of development
and progress.
The imaging system utilized at Cole
Eye Institute is Zeiss FORUM. Nearly
all our diagnostic reports are stored
and displayed within this system. This
includes OCT, photography, angiog-
raphy and visual field testing. The
comprehensive nature of this package
provides the clinician with a practi-
cal interface that enhances workflow,
facilitates optimal interpretation and
allows integration of test results, such
as visual field and OCT correlation.
In addition, we have elected to utilize
this system throughout our satellite
network. The servers that provide the
data for the software system communi-
cate with all the community locations.
This system gives the clinician access
to a test performed at one location even
when the patient is seen at another.
Data integrity is also a critical compo-
nent for any EMR and imaging solution.
One important enhancement to the
consistency of patient identification and
labeling is the multidirectional com-
munication among the EMR system,
the diagnostic device and the imaging
solution. In our current system, an
order is placed within the EMR system
and then is transferred to an electronic
work-list. The diagnostic device is able
to pull the order from the work-list with
the patient’s identifying information al-
ready populated from the EMR system.
Following the diagnostic procedure,
the reports are then published to the
image viewing software. This ensures a
seamless transition from the EMR to the
imaging solution, helping to eliminate
transcription errors and variability in
data entry.
When making the transition to a digital
interface, access to previously collected
data and test reports is an important
consideration. A practice must consider
the practical aspects of importing previ-
ous diagnostic studies and how far back
to go when including such studies. If
data is not included, an archiving solu-
tion needs to be in place to provide a
backup if older data is needed.
The communication and interface for
opening reports between the EMR sys-
tem and imaging solution software also
varies from system to system.
By Justis Ehlers, MD

7
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n n o v a t i o n s
In some packages, there is no direct
way to open diagnostic testing within
the EMR system. Others use a link that
opens the imaging solution program
and the patient’s information with a
single mouse click. Finally, some pack-
ages have the reports embedded within
the EMR system itself. All these features
can potentially impact workflow and
should be considered when selecting an
imaging solution.
A final consideration is how to display di-
agnostic reports. As our clinical practices
have become more imaging-centric, the
interface for the clinician as well as for
the patient becomes important. Often,
clinicians will review the testing with the
patient directly. The ease and flexibility
of the display system is vital, particularly
when many patients may be dealing with
visual impairment. Possible solutions in-
clude tablets, iPads, laptops, large-screen
monitors and dual-monitor systems. The
choice certainly comes down to practice
style and personal preference. The type
of imaging used and the patient popula-
tion may impact which solution fits best
for a given practice.
The options for the imaging solutions
will continue to expand. These software
The comprehensive nature of this package provides the clinician with a practical interface that enhances workflow, facilitates optimal interpretation and allows integration of test results, such as visual field and OCT correlation.
packages enhance patient care and im-
prove communication between offices
and physicians. There is often a signifi-
cant initial learning curve during which
efficiency may initially suffer. However,
the advantages of an electronic display
system over paper records are signifi-
cant. Careful preparation and research
regarding the system that best fits your
practice’s requirements can help dra-
matically ease the transition. ■
Contact Dr. Justis Ehlers at [email protected].

8
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
It has also helped involve patients in
their own care and has made billing
more accurate and timely. Judging
from the feedback from other institu-
tions, it would be fair to say that Cleve-
land Clinic’s new system is raising the
national standard of ophthalmic care.
It wasn’t always this way.
“In ophthalmology we’ve been reluc-
tant to embrace EMR,” says Dr. Kaiser.
“Our charts are visually based, and the
traditional EMR system only allowed
data. Ophthalmologists need to make
drawings of the eye to create the visual
history that is critical to the therapeu-
tic plan. Until now, inserting drawings
into an electronic record was all but
impossible.”
Cole Eye Institute’s new EMR platform
easily allows the incorporation of graph-
ics (see related articles in this issue) and
facilitates the move from paper charts
to the computer. Designed within the
institute by a group of staff, the platform
sits on top of the common and widely
used Epic EMR system.
“The standard Epic EMR is text-based
and not graphical, so it wouldn’t have
worked for us,” says Dr. Kaiser.
A Bright New Window on
the Whole Patient
The new system allows an expanded
level of interaction between ophthal-
mologists and other providers, which
is core to the collaborative practice of
medicine at Cleveland Clinic.
“It isn’t just the eyes that concern us, it’s
the whole patient,” says Dr. Kaiser. “An
ocular issue in a diabetic patient can
now be shared in real time with that
patient’s endocrinologist, internist, car-
diologist and nephrology team. Having
a single, all-inclusive medical record is
much more than just a nicety; it opens
important new channels to provide
patients world-class care.”
The federally mandated medicine
reconciliation is a perfect example.
Reconciliation was very difficult to ac-
complish on paper but with the advent
of EMR is now very easy. The electronic
record maintains a real-time history
of the patient’s medication orders and
helps avoid omissions, duplications,
dosing errors and drug interactions.
Refills are sent electronically to the
patient’s pharmacy, eliminating tran-
scription errors.
Improving Information Flow
at Satellite Locations
In the past, a Cleveland Clinic oph-
thalmologist seeing a patient at a
community location did not have
complete access to the thorough and
descriptive imaging that was available
at the main campus. EMR has changed
that, and not just for remote locations.
Now, any doctor who participates in
Cleveland Clinic’s MyPractice online
referral and patient monitoring system
Newly Developed System Is Bringing Far-Reaching and Unexpected Benefits
Better overall medical care, a new perspective on the whole patient and
improved access for referring physicians are just three of the ways the new
electronic medical record system has improved Cole Eye Institute, says Peter
K. Kaiser, MD, a staff member of the vitreoretinal faculty of the Cole Eye
Institute at Cleveland Clinic’s main campus.
Peter K. Kaiser, MD

9
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n n o v a t i o n s
can review all charts and images from
any connected location. “The more
information that’s available, the better
the medical decisions,” says Dr. Kaiser.
This is especially beneficial in emer-
gency situations, which can happen at
any time of the day or night.
Opening New Channels with
Referring Doctors
Communication with referring doctors
can now be maintained more easily, and
can be updated far more quickly.
“We can now send referring doctors
electronic images. If, for example, we
have a patient with a macular hole, we
can image the macula before and after
surgery and update the referring doctor
almost in real time electronically,” says
Dr. Kaiser. “This improves our com-
munication and creates opportunities
to further improve patient care,” he
adds. “The referring doctors can see
exactly what we did and why since they
can see patient records. This also can
help ensure that patients return to their
referring doctor for follow-up care.”
Better Care from the Patient’s View
Patients who use Cleveland Clinic’s
web-based MyChart to track their medi-
cal care can now be kept more current,
more easily. In the past, no patient
had access to ophthalmology-related
tests. The new EMR system allows
ophthalmologists to make a variety of
information available to MyChart. Test
results and other relevant data can now
be released electronically, allowing con-
nected patients to access it at will.
“This gives patients a sense of involve-
ment in the dynamics of their own care,
which is very empowering. They can
track their progress in therapy, and this
tends to improve their outlook, which is
therapeutic in itself,” he says.
Eliminating Billing and Insurance Errors
Financial efficiencies are built into the
new system. “It’s a huge plus to be able
to make sure that everything we order
and interpret is billed appropriately,”
says Dr. Kaiser. “With paper this was
often complicated, and, quite frankly,
sometimes we missed things for which
we should have billed.”
The new system has automatic drop-
down menus to remind the doctor to
interpret tests. Once the interpretation
is completed, the billing automatically
goes out to the patient’s insurance pro-
vider. It’s an efficient system in which
little falls through the cracks.
The new system allows an expanded level of interaction between ophthalmologists and other providers, which is core to the collaborative practice of medicine at Cleveland Clinic.
“For those of us who are very busy, it’s
nice to have someone looking over our
shoulder to make sure we’ve done every-
thing that’s required,” he says.
Setting a New National Standard
The new EMR system is setting a new
national standard. “Other eye institutes
around the country have tried to use the
stock Epic system with limited success;
they’ve lost productivity and suffered
decreased patient volumes without
improving patient care,” says Dr. Kaiser.
“We didn’t want to follow in their foot-
steps. Our system is light years ahead
of where we started.”
As word of the new system gets out,
many eye institutes using Epic have
approached Cleveland Clinic’s Cole Eye
Institute to learn more. Cleveland Clinic
is sharing its knowledge, the better to
improve patient care nationwide. ■
Dr. Peter K. Kaiser can be reached at [email protected].

10
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Building the Toolbox – Essential Features and Functions in EMR Systems
Good features can significantly smooth the bumpy road to EMR adoption.
Adding customized, intuitive functions within an EMR system can improve
your workflow and practice efficiency. When Cleveland Clinic’s Cole Eye
Institute first made the transition to EMR, our group spent several months
evaluating several systems to find just the right tools.
Even if specific capabilities
weren’t initially within the sys-
tem, we worked with the vendor
and our own IT people to create and
implement those special features. These
can be broken down into three distinct
groups: improving the user experience of
both providers and support staff; improv-
ing the billing capture and process; and
integrating outcomes, administrative
tasks and research activities.
Improving the User Experience
Ergonomics is a key element in facili-
tating user adoption and acceptance
of any EMR system. By incorporating
the largest monitors possible, we were
able to distribute a significant amount
of information across a larger space.
We added personal computers to the
hallways to mimic the normal workflow
where a physician reviews the chart
before entering the examination or
procedure room. Placing printers in
the hallway minimized the distance
that physicians had to travel for printed
prescriptions and patient instructions.
All of these enhancements made it
easier for physicians to adapt to the
new EMR workflow.
Drawing is a mainstay of ophthalmol-
ogy practices. We first created newer
pictures to represent the portions of the
eye that needed or required documenta-
tion. We were able to create numerous
stencils for each of the drawing photos
that allowed for both annotation of the
image and insertion of text into the
same exam field of the patient, eliminat-
ing duplication of work. The draw-
ings could be placed within the chart,
pulled forward to a new encounter for
modification or even added to a letter to
another provider.
We improved the letter-writing and
documentation capabilities of our sys-
tem by implementing letter templates
with drop-down menus for quick anno-
tation. By adding an autocorrect feature
to our system (converting common
abbreviations such as OD to right eye),
we were able to better communicate to
other physicians without ophthalmic
backgrounds what transpired with the
patients. Finally, by adding the capabil-
ity to fax letters directly from the EMR,
our physicians could maintain faster
contact with referring providers and
their staff.
Improving Billing Capture and Process
The number of procedures and diagnos-
tics in ophthalmology has drastically in-
creased over the past few years. Take for
example the use of intravitreal injections
for eye disease. In the past five years, the
number of times that procedure is done
has quadrupled. Increased volume has
made it difficult to track procedures and
submit charges in an efficient fashion.
We implemented a charge-on-comple-
tion system which has improved our
billing compliance, led to significantly
improved documentation of patient
By Rishi P. Singh, MD
11
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n n o v a t i o n s
testing and procedures, and increased
our efficiency in billing and reimburse-
ment for professional fees.
Here’s how it works: The physician
places an order for the procedure or
diagnostic test. The order then gener-
ates a form for the physician to fill out.
After the physician electronically signs
the form, the charge is submitted with
the specific procedural or diagnostic
code to our billing team for review. Once
reviewed electronically, the biller can
submit the charge to the local carrier for
processing. This has streamlined our
billing cycle from weeks to two days. It’s
also decreased the potential for miscod-
ing since it has completely eliminated
manual entry. Finally, it allows for a
transparent review of the indication and
necessity of the procedure.
Integrating Outcomes, Administrative,
and Research Activities with the EMR
Since 2005, all Cleveland Clinic institutes
have participated in a patient outcomes
reporting initiative. Until recently, the
outcomes data has been compiled using
manual entry and physician reporting,
both ways by which reporting biases could
be introduced. When we developed the
entry system for our EMR, a conscious ef-
fort was made to use discrete documenta-
tion whenever possible. For example, few
areas in the system have plain-text boxes
for entry. Rather, buttons and checkboxes
are used to document imaging, proce-
dures and exam elements. This allows us
to collect outcome metrics in an almost
completely automated fashion.
In addition, by using the discrete ele-
ments within our system, we created
additional data streams that determine
a multitude of administrative and
research functions. For example, we
can now monitor our usage of supplies
in real time to determine whether our
pharmacy needs to be restocked. We
can evaluate the wait times by ophthal-
mology specialist line in an effort to
Overall, these features have allowed for the ongoing evaluation and management of the physician and patient experience and will lead to future enhancements of both functions.
maintain the proper technician-to-phy-
sician ratios. Finally, our practice has
been able to monitor the frequency of
use of our lasers and diagnostic modali-
ties so we can adjust schedule templates
to maximize patient flow. Research has
become easier, with only a few clicks
necessary to analyze multiple patient
charts rather than the arduous process
of chart retrieval and review. (See article
on page 15 for a nurse’s perspective.)
Overall, these features have allowed
for the ongoing evaluation and man-
agement of the physician and patient
experience and will lead to future
enhancements of both functions. ■
Contact Dr. Rishi P. Singh at [email protected].
12
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Patient History an Open Book - a Bonus of Record Systems
Community ophthalmologist Michael Millstein, MD, says Cleveland Clinic’s EMR
system provides a complete picture of a patient’s medical history. “When we
open an electronic chart, we finally can see the patient’s entire medical history.
We don’t have to ask over and over what happened in the past. Everything is
there in detail, and it’s all legible,” he says.
Because all Cleveland Clinic phy-
sicians share the same system,
each patient has a single chart.
When one of Dr. Millstein’s patients is
seen by a colleague, he now has access
to details about the patient encounter.
“It’s a great educational opportunity.
I can read in depth what my colleague
was thinking, what tests were done and
why, and what the results were. It helps
me to better learn about the disease
process and enables me to take better
care of the patient,” he says.
Improving Speed and Safety
When the EMR is opened to a patient’s
chart, the first screen offers a menu of
tabs for the typical workflow aspects of
an ophthalmology patient visit, includ-
ing medications, allergies and reasons
for being seen. The information is
filled in by typing or by choosing from
drop-down menus of the most-utilized
medications and most common aller-
gies and complaints.
“I can review the medication list with
a patient and not worry about whether
they forgot to tell me about a medica-
tion or don’t know a dosage. This is
because the list not only includes pre-
scribed medications but an active list
of recently filled medications from their
pharmacies,” he says.
When he covers for a colleague, he
no longer worries about misreading a
medication order. Moreover, the system
sends warnings about potential drug-
drug interactions and allergies. “It defi-
nitely helps prevent mistakes,” he says.
Better Documentation
Sophisticated graphics software al-
lows the ophthalmologists to docu-
ment ocular diseases by selecting a
preset stencil and drawing the pathol-
ogy with a mouse or copying and
pasting from a menu of images. For a
patient with macular degeneration, for
example, Dr. Millstein simply clicks
on drusen and drops them on the
image. All prior images are stored for
comparison, allowing progress or lack
of progress to be tracked over time.
For a physician who describes himself
as “extremely detail-oriented,” the EMR
facilitates thorough documentation that
is guaranteed to be legible.
“I have horrible penmanship. So do my
partners. At times it is difficult to deci-
pher each other’s handwriting,” he says.
“The EMR lets me enter notes in a way
that can be neatly reviewed and printed
out. It takes a little longer initially, but it
is legible. The next time I see the patient,
I simply call up the last assessment and
plan and make quick changes based on
that day’s visit,” he says.
Dr. Millstein can send these notes
electronically to the inbox of any other
physician using the system, improving
physician-to-physician communication.
For those doctors outside of Cleveland
Clinic’s system, letters and notes can
be directly faxed from the EMR system
Michael Millstein, MD
13
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n n o v a t i o n s
to their office, and the system retains
their mailing addresses, fax numbers
and office locations. “We don’t have
to engage our secretaries nearly as
much for dictation or correspondence
because of our system.”
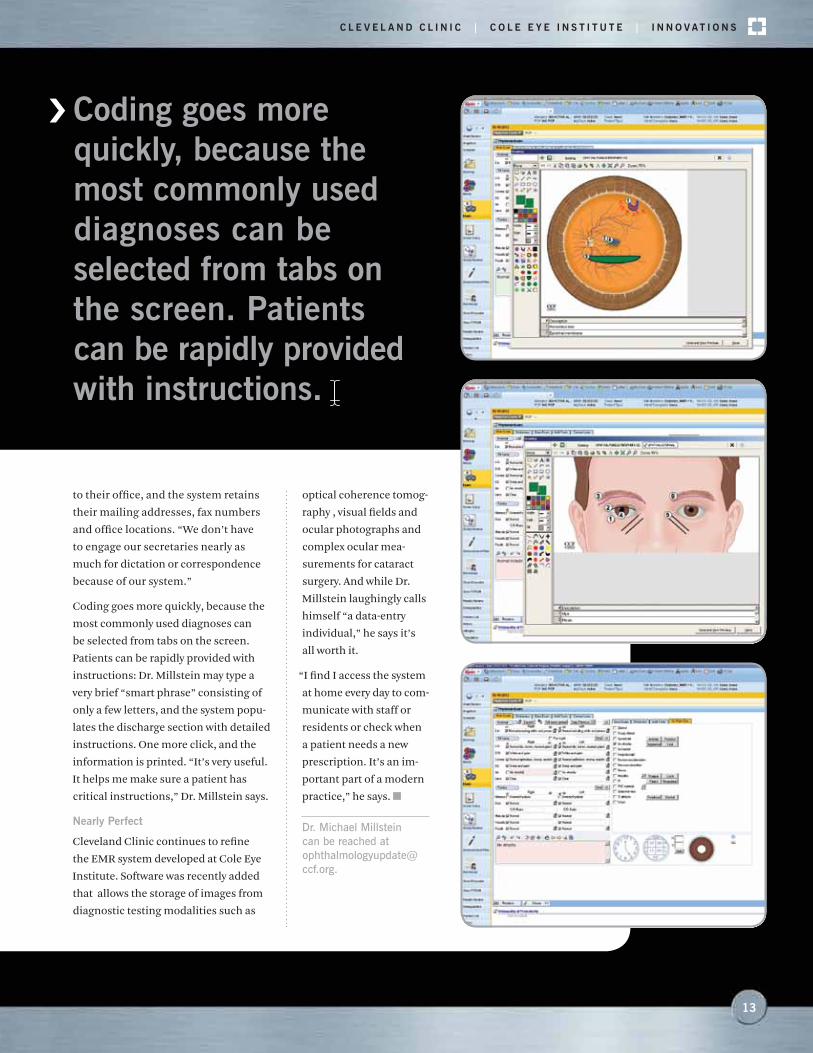
Coding goes more quickly, because the
most commonly used diagnoses can
be selected from tabs on the screen.
Patients can be rapidly provided with
instructions: Dr. Millstein may type a
very brief “smart phrase” consisting of
only a few letters, and the system popu-
lates the discharge section with detailed
instructions. One more click, and the
information is printed. “It’s very useful.
It helps me make sure a patient has
critical instructions,” Dr. Millstein says.
Nearly Perfect
Cleveland Clinic continues to refine
the EMR system developed at Cole Eye
Institute. Software was recently added
that allows the storage of images from
diagnostic testing modalities such as
Coding goes more quickly, because the most commonly used diagnoses can be selected from tabs on the screen. Patients can be rapidly provided with instructions.
optical coherence tomog-
raphy , visual fields and
ocular photographs and
complex ocular mea-
surements for cataract
surgery. And while Dr.
Millstein laughingly calls
himself “a data-entry
individual,” he says it’s
all worth it.
“I find I access the system
at home every day to com-
municate with staff or
residents or check when
a patient needs a new
prescription. It’s an im-
portant part of a modern
practice,” he says. ■
Dr. Michael Millstein can be reached at [email protected].
14
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
EMR Facilitates Communication and Improves Treatment of Uveitis
Caring for patients with uveitis often requires a multidisciplinary team
- an ophthalmologist, a rheumatologist and often other providers - to
ensure a coordinated effort. At Cole Eye Institute, implementation of an
EMR system has improved the care of these complex cases and opens
the door for coordinated care and research activities.
T hree ophthalmologists care
for patients with uveitis, and
the rheumatology section
includes 12 adult providers and three
pediatric providers. Additionally, the
pulmonary, neurology and infectious
disease services are often consulted to
assist in the care of uveitis patients.
Prior to EMR, communication among the
services was adequate – emails, printed
letters and phone calls were primarily
used to discuss cases. However, the
inability to read the other findings and
plans limited each particular service’s
ability to assess the patient. It was also
apparent that providers may not have
understood what was needed or what to
look for in a specific patient. The review
of laboratory tests and images was tedious
and sometimes incomplete. Most impor-
tant, tracking the success or failure of vari-
ous immunosuppressants was difficult
since endpoints were embedded within
visits and not summarized.
With the implementation of a shared
EMR chart between ophthalmology and
non-ophthalmology providers, both
communication and care for patients
have improved considerably. Sharing
of notes and letters between providers
can be accomplished while evaluating
a patient, often with one or two clicks.
If the providers aren’t part of Cleveland
Clinic’s system, the letters can be faxed
directly to the providers’ offices, keep-
ing them in the loop of ongoing findings
and treatments. Often clinical care
decisions can be made very quickly as
providers receive messages, with instant
transfer of information. Additionally,
the ability to view each other’s clinical
exams and notes without having to
decipher handwriting has improved
clinicians’ understanding of what the
other team is looking for when making
decisions for these patients. Finally,
our clinicians can now track ophthal-
mic endpoints graphically over time as
a method of determining response to
treatments and procedures.
Improving our ability to track outcomes
of patients is the next step of imple-
mentation. Shared patients with uveitis
By Sunil Srivastava, MD
are now easily identified and screened
for visual outcomes and for potential
enrollment in clinical trials. A common
outcome form is under development
between services to serve as a shared
measure of disease severity and to track
succeses or failures with particular drug
regimens. Patient registries are also
under development to allow tracking of
particular subtypes (e.g., pediatric uve-
itis patients) to assess quality and suc-
cessful visual and systemic outcomes.
With imaging being linked to EMR, a
large database of complex diseases with
outcomes data is under construction,
which will allow an improved under-
standing of this complex disease.
Overall, EMR in its current form has
improved care for our patients with
complex inflammatory disease. In the
future, EMR will continue to facilitate
improvements in our understanding
of these diseases through research and
clinical outcome measurements. ■
Dr. Sunil Srivastava can be reached at [email protected].

15
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n n o v a t i o n s
Cole Eye Institute’s EMR system has not just improved the
workflow of the ophthalmologists and optometrists on staff
but also the daily work of nurses and technicians.
T iffany Rodstrom, RN, a five-year
veteran of Cole Eye Institute
who works primarily with a reti-
na specialist, says the system reduces
problems with unclear plans from pre-
vious visits. “Prior to EMR, it was diffi-
cult to tell what tests the doctor wanted
performed on the next visit; and EMR
has helped tremendously in this regard
because the future visit plans are con-
cise and easy to understand.” It also
improves communication between the
providers and their secretaries, surgi-
cal schedulers, referring physicians
and other departments.
Although some staff members were
wary of the changes initially, she
says most like it now. Rodstrom had
previously been through another EMR
implementation, and during this
implementation process, she worked
closely with the information technol-
ogy team as the system was developed.
“With my previous role as a certified
ophthalmic technician and now as a
nurse, I used my knowledge to help
customize our EMR system and stream-
line our patient exams,” she says.
One of her favorite features is the abil-
ity to add ophthalmic drawings, previ-
ously done by hand, into the EMR.
“We added stencils that annotate the
drawing and put information into the
exam (saving the physician steps). The
drawings are improved, allowing for
clearer communication about our find-
ings,” she says.
She finds that the EMR particularly
boosts efficiency in Cole Eye Institute’s
busiest services. With some of the
specialists seeing 70 or more patients
a day, about half of whom need some
form of diagnostic testing, moving
them all through and documenting
their exams, procedures and diag-
nostic interpretations is crucial. The
“Study Review” module, a feature that
tracks all procedures and diagnostic
tests a patient has undergone, was
made available in the EMR and is very
helpful, she adds.
“We’ve added buttons for documentation
of exams and procedures, vs. tradi-
tional manual entry, which increases our
ability to document in a clear, compliant
Ophthalmic Nurse Uses EMR in Every Aspect of Her Work
and concise fashion,” she says. “As part
of this, we created 104 custom smart
forms and 180 order sets to help us make
our workflow efficient.”
Rodstrom says she uses the EMR in ev-
ery aspect of her work: rooming of pa-
tients, phone encounters, patient care
issues and documentation of instruc-
tions to patients. Although scribes are
not part of Cole Eye Institute’s overall
approach to EMR, Rodstrom occa-
sionally fills that role as well in the
course of her daily work. She adds that
utilizing the system has made patient
handoffs to other technicians or doc-
tors much easier, thereby improving
the overall patient experience. ■
Contact Tiffany Rodstrom, RN, at [email protected].

16
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
And with customized snapshots
that provide detailed history
of a patient’s last surgical pro-
cedure or diagnostic test, her team can
process all visits without any paper.
“It’s all right in front of them,” she says.
“They don’t have to search or wait for it.”
The EMR system has made capturing
charges a much more streamlined
process, Ms. Surender says. When all
Cole Eye Institute billing was done via
paper tickets, some diagnostic tests did
not get billed if the ticket was misplaced.
Her team spent many hours a day manu-
ally keying information into a separate
billing system. Now, the system bill is
created when the ordering physician
signs off on the results (adding an
extra level of assurance that all tests
are accounted for prior to the bill being
submitted). Similarly, for treatments,
providers enter what they have done and
link the treatment to a diagnosis. This
process, a first anywhere in Cleveland
Clinic, automatically drops all charges
into a tank for her team to review before
sending them out to insurance compa-
nies for reimbursement.
“We are no longer losing revenue when
paper gets lost or waiting days to sub-
mit claims,” says Ms. Surender, who
has worked on billing at Cole Eye Insti-
tute for about 10 years. “And we are eas-
ily capturing 15 percent more charges
as a result of the new system,” she says.
“I am very particular about compliance
and this really helps improve our work,”
she adds.
Ophthalmology is unique in the fre-
quency of tests and treatments being
performed during the same patient
visit; almost 50 percent of patients will
have a diagnostic test or procedure done
during a visit. A major problem in eye
care is that the employees who perform
the billing function do not sit with the
providers and do not always know what
services were provided to the patient
and whether those procedures were
completed.
The EMR lets the billers visualize charts
on a real-time basis and see everything
that was done. They no longer have to
chase the doctors around to fill in any
blanks. All the components they need to
submit proper billing are right there. And
in the case of an audit or denied claim by
an insurance company, the charts can be
queried with the push of a button.
Another advantage EMR has provided Ms.
Surender’s team relates to the increased
presence of Cole Eye Institute in com-
munity facilities. It’s not uncommon for
staff physicians to travel between two
offices each week. Prior to EMR, patients
who alternated the location they went
to didn’t have a complete chart. In ad-
dition, her billing counterparts in the
community couldn’t see what was being
performed in other offices. Now, with
EMR, seamless care can be provided ev-
erywhere, greatly enhancing the patient
expereince . ■
Nandini Surender can be reached at [email protected].
For Nandini Surrender, a reimbursement manager at Cleveland Clinic’s
Cole Eye Institute, the transition to an EMR system has improved many
aspects of her work. “It has greatly increased our surveillance of billing,
compliance and documentation. With no bad handwriting to interpret
or missing signatures, the billing staff feels that the process has
become a lot more efficient and standardized,” she says.
EMR Boosts Compliance and Captures Charges
17
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n n o v a t i o n s
In 1993, at the age of 29, life
brought Ms. Hardesty face to face
with an almost universal fear:
going blind. Previously enjoying good
vision, Ms. Hardesty was shocked to
learn that she had presumed ocular
histoplasmosis and was bleeding inter-
nally in her right eye. She has endured
multiple surgeries in order to stabilize
her condition.
Her retina specialist now treats her
with monthly ocular injections of
Lucentis® and multiple topical drops.
Keeping track of the details of all these
conditions and all other medications
and treatments Ms. Hardesty has for
other conditions is simple with Cole
Eye Institute’s EMR.
When considering the savings in both
money and time that EMR systems pro-
vide to patients and health systems alike,
Ms. Hardesty speaks without hesitation:
“Golly, I can’t imagine what the savings
will be. It’s great for patients who don’t
have to keep repeating tests when they
go from place to place, not to mention
how much the hospitals probably save
from maintaining all those records.”
“We really don’t enjoy being tested,”
she says from her perspective as a patient.
“And the cost is a stress, too - especially for
people who don’t have insurance, like I
didn’t for some time during all this.”
She relates that one of her first doctors
used his collection of colored pencils
to draw her macula on her paper charts.
No longer is this the case with EMR.
Ms. Hardesty says that special func-
tions of the EMR preclude the use of
colored pencils - the only implements
needed are a keyboard and a mouse.
And, she adds, wherever she goes, her
records - in full - are present.
Requesting records and and giving
patients access to their own records are
also a snap. When Ms. Hardesty needed
letters to her employer, they were given
Patients See the Value in EMR
to her the same day since they could be
generated within the EMR quicker than
sending the request to a transcription
service. Since Ms. Hardesty is so com-
fortable with computers, she is happy
about the efficiencies the EMR brings.
Cleveland Clinic’s MyChart online portal
for patients allows access to test results
and important reminders for complete
patient care. She adds that long wait
times are a thing of the past - in some
cases, the doctor has been waiting to see
her, rather than Ms. Hardesty having
to endure sometimes hours-long waits
to see a doctor due to nonemergency
scheduling issues.
“Not only are all my records available
when I see any specialist I may need to
see, but I like to look at what they are
looking at.” ■
Karen Hardesty is a self-professed computer geek. That’s one
part of the reason why she sees tremendous value in the migra-
tion to electronic medical record systems. The other reason is
that she’s had to endure a long history of ophthalmic procedures
over the past 20 years.
She adds that long wait times are a thing of the past - in some cases, the doctor has been waiting to see her, rather than Ms. Hardesty having to endure sometimes hours-long waits to see a doctor due to nonemergency scheduling issues.
Striving for Answers
19
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n v e s t i g a t i o n s
CATT Second-Year Results Show Lucentis and Avastin Produce Similar Results
T he study also showed that
monthly dosing produced
slightly more vision gain than
as-needed dosing. But the final visual
results were similar in all treatment
groups, regardless of dosing frequency,
with 60 percent or more of the patients
achieving driving vision.
“Both drugs were highly effective regard-
less of the approach to dosing,” says Dan-
iel F. Martin, MD, study chair for CATT
and Chairman of Cole Eye Institute.
“There was slightly less vision gain with
as-needed treatment. However, patients
seeking the small extra advantage of
monthly treatment need to be mindful
of the additional burden, risks and costs
of monthly injections. Since as-needed
dosing required 10 fewer eye injections
over the course of two years and yielded
similar visual results, many patients
may choose this option.”
Ten years ago, 60 to 70 percent of
patients with wet AMD were legally
blind in two years. Due to the powerful
therapeutic effects of the drugs studied
in CATT, only 5 to 10 percent of patients
are legally blinded from AMD today.
However, prior to the results of this trial,
doctors did not know the optimal way
to use these drugs or whether one drug
was better than the other.
Over two years, the rates of death,
myocardial infarction and stroke did
not differ between drugs. In the first
year of the study, there was a higher rate
of nonspecific serious adverse events for
bevacizumab-treated patients than for
ranibizumab-treated patients, and this
difference persisted in year two. How-
ever, the importance of this difference
was unclear.
Serious adverse events occurred at a
40 percent rate for patients receiving
bevacizumab and a 32 percent rate
for patients receiving ranibizumab.
Although bevacizumab had a higher
rate of serious adverse events, they
were distributed across many different
conditions, most of which were not
associated with bevacizumab when
evaluated in cancer clinical trials.
In conjunction with the clinical find-
ings from this study, the cost differ-
ences between treatments may have
implications for both patients and
physicians. One dose of ranibizumab
costs approximately $2,000, while beva-
cizumab costs about $50 per dose. Both
drugs are manufactured by Genentech.
“In 2010, ranibizumab accounted for
nearly 10 percent of the entire Medicare
Part B drug budget, its single largest
expenditure,” write the study authors.
“As the treatment of patients continues
indefinitely, the cumulative financial
burden to third-party payers and pa-
tients will only increase.”
Funded by the National Eye Institute,
as part of the National Institutes of
Health, CATT seeks to compare the rela-
tive safety and effectiveness of the two
drugs in treating wet AMD. Ophthalmol-
ogists began using bevacizumab while
awaiting FDA approval of ranibizumab
because of the drugs’ structural similari-
ties. Bevacizumab, approved by the FDA
for treating colorectal cancer, has been
widely prescribed off-label by ophthal-
mologists to treat AMD since 2005. ■
More information is available at clevelandclinic.org/CATT.
In the ongoing Comparison of AMD Treatment Trials (CATT) drug-comparison study, Cleveland Clinic
researchers found that bevacizumab (Avastin®) is equivalent to ranibizumab (Lucentis) in the treatment
of wet age-related macular degeneration (AMD) through two years.

20
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Retinal Diseases
Investigator-Initiated Observational Study of Intravitreal Aflibercept Injection for Exudative Age- Related Macular Degeneration Previously Treated with Ranibizumab or BevacizumabObjective: Observational study to assess the efficacy of intra-
vitreal aflibercept injection in subjects previously treated with
Ranibizumab or Bevacizumab on central retinal thickness as
measured by spectral domain optical coherence tomography
(SDOCT)
Contact: Rishi P. Singh, MD, 216.445.9497,
or Stephanie Bennett, 216.445.6497
Fluocinolone Acetonide Intravitreal Inserts for Vein Occlusion in Retina (FAVOR)Objective: This study will assess the safety and efficacy of
fluocinolone acetonid eintravitreal inserts in subjects with
macular edema secondary to RVO .
Contact: Peter K. Kaiser, MD, 216.444.6702,
or Gail Kolin, RN, 216.445.4086
Home Vision Monitoring Using the Foresee Home Device Following Treatment of Neovascular Age-Related Macular Degeneration (CNV)Objective: The purpose of the current study is to evaluate if,
in post-treatment patients, parameters as measured with the
Foresee Home Device are in agreement with clinical decisions
and retinal characteristics as measured with optical coherence
tomography (OCT).
Contact: Rishi P. Singh, MD, 216.445.9497,
or Sonal Uppal, PhD, 216.444.7137
Uveitis
A Proof-of-Concept Study of Intravitreal LFG316 in Patients with Multifocal Choroiditis (MFC)Objective: The study is designed to provide information on
the safety, tolerability, pharmacokinetics, pharmacodynamics,
and efficacy of successive intravenous (IV) doses of LFG316
in eligible patients with neovascular age-related macular
degeneration (AMD).
Contact: Sunil Srivastava, MD, 216.636.2286,
or Laura Holody, 216.445.3762
Pediatric Eye Disease
Bilateral Lateral Rectus Recession Versus Unilateral Recess-Resect for Intermittent Exotropia (IXT1)Objective: The purpose of this study is to evaluate the effec-
tiveness of bilateral lateral rectus muscle recession vs. uni-
lateral lateral rectus recession with medial rectus resection
procedures for the treatment of strabismus.
Contact: Elias Traboulsi, MD, 216.444.4363,
or Sue Crowe, RN, 216.445.3840
Increasing Patching for Amblyopia in Children 3 to < 8 Years Old (ATS15)Objective: This study is designed to evaluate the effectiveness
of increasing prescribed patching treatment after visual acuity
has stabilized with initial treatment and amblyopia is still
present.
Contact: Elias Traboulsi, MD, 216.444.4363,
or Sue Crowe, RN, 216.445.3840
The following studies are either currently enrolling new patients or are pending
approval by the Institutional Review Board and should be enrolling shortly.
Clinical Trials

21
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n v e s t i g a t i o n s
Genetics
Molecular Genetics of Eye DiseasesObjective: The objective of this project is to study the molecu-
lar genetics of ophthalmic disorders through the compilation
of a collection of DNA, plasma and eye tissue samples from
patients and from families with a broad range of eye diseases
and malformations.
Contact: Elias Traboulsi, MD, 216.444.4363,
or Sonal Uppal, PhD, 216.444.7137
Cornea/Refractive Surgery
LASIK Flap Thickness and Visual Outcomes Using the WaveLight FS200 Femtosecond LaserObjective: To evaluate the visual outcome, accuracy and predict-
ability of LASIK flap thickness using the new WaveLight® FS200
femtosecond laser and compare these results to those obtained
using the IntraLaseTM FS60 femtosecond laser.
Contact: Ronald Krueger, MD, 216.444.8158,
or Laura Holody, 216.445.2264
Long-Term Safety Follow-up for Subjects Previously Implanted With The AcrySof Cachet Phakic Lens in Clinical Studies C-02-23, C-02-40, C-03-21 and C-05-57Objective: To estimate the annualized endothelial cell loss
rate (for up to 10 years following date of implantation) of
subjects previously implanted with the L-series AcrySof®
Cachet™ Phakic Lens from clinical studies.
Contact: Ronald Krueger, MD, 216.444.8158,
or Laura Holody, 216.445.2264
Other Open Studies
Safety Study of a Single IVT Injection of QPI-1007 in Chronic Optic Nerve Atrophy and Recent-Onset NAION Patients (NAION)Objective: This is an open-label, dose escalation, safety,
tolerability and pharmacokinetic study, where the active study
drug (QPI -1007) will be given to all patients who participate.
This study will determine whether QPI-1007 is safe when it is
injected into the eye. The study will also reveal if there are any
side effects of the drug and how long it takes for the body to
clear the drug.
Contact: Rishi P. Singh, MD, 216.445.9497,
or Laura Holody, 216.445.2264
The following studies have completed patient enrollment
in the last year at Cole Eye Institute and are in follow-up:
Comparing the Effectiveness of Treatment Strategies for Primary Open-Angle Glaucoma
A Phase II Dose-Ranging Study of Pazopanib to Treat Neovascular Age-Related Macular Degeneration (GSK AMD)
Infant Aphakia Treatment Study (IATS)

22
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Adv.Exp.Med.Biol.
Bagheri N, Bell BA, Bonilha VL, Hollyfield JG. Imaging human postmortem eyes with SLO and OCT. Adv Exp Med Biol. 2012;723:479-488.
Bell BA, Kaul C, Rayborn ME, Hollyfield JG. Baseline imaging reveals preexisting retinal abnormalities in mice. Adv Exp Med Biol. 2012;723:459-469.
Grossman GH, Pauer GJ, Hoppe G, Hagstrom SA. Isolating photoreceptor compartment-specific protein complexes for subsequent proteomic analysis. Adv Exp Med Biol. 2012;723:701-707.
Hagstrom SA, Watson RF, Pauer GJT, Grossman GH. Tulp1 is involved in specific photoreceptor protein transport pathways. Adv Exp Med Biol. 2012;723:783-789.
Stohr H, Anand-Apte B. A review and update on the molecular basis of pathogenesis of Sorsby fundus dystrophy. Adv Exp Med Biol. 2012;723:261-267.
Sugimoto M, Cutler A, Grossman G, Anand-Apte B. Regulation of retinal vascular per-meability by betacellulin. Adv Exp Med Biol. 2012;723:293-298.
Am.J.Hum.Genet.
Peachey NS, Ray TA, Florijn R, Rowe LB, Sjoerdsma T, Contreras-Alcantara S, Baba K, Tosini G, Pozdeyev N, Iuvone PM, Bojang P Jr., Pearring JN, Simonsz HJ, Van Genderen M, Birch DG, Traboulsi EI, Dorfman A, Lopez I, Ren H, Goldberg AFX, Nishina PM, Lachapelle P, McCall MA, Koenekoop RK, Bergen AAB, Kamermans M, Gregg RG. GPR179 is required for depolarizing bipolar cell function and is mutated in autosomal-recessive complete congenital stationary night blindness. Am J Hum Genet. 2012 Feb 10;90(2):331-339.
Webb TR, Matarin M, Gardner JC, Kelber-man D, Hassan H, Ang W, Michaelides M, Ruddle JB, Pennell CE, Yazar S, Khor CC, Aung T, Yogarajah M, Robson AG, Holder GE, Cheetham ME, Traboulsi EI, Moore AT, Sowden JC, Sisodiya SM, Mackey DA, Tuft SJ, Hardcastle AJ. X-linked megalocornea caused by mutations in CHRDL1 identifies an essential role for ventroptin in anterior segment development. Am J Hum Genet. 2012 Feb 10;90(2):247-259.
Am.J.Ophthalmol.
Chappelow AV, Tan K, Waheed NK, Kaiser PK. Panretinal photocoagulation for prolif-erative diabetic retinopathy: pattern scan laser versus argon laser. Am J Ophthalmol. 2012 Jan;153(1):137-142.
Sezgin E, Van Natta ML, Ahuja A, Lyon A, Srivastava S, Troyer JL, O’Brien SJ, Jabs DA. Association of host genetic risk factors with the course of cytomegalovirus retinitis in patients infected with human immu-nodeficiency virus. Am J Ophthalmol. 2011 Jun;151(6):999-1006.
Am.J.Pathol.
Morais C, Ebrahem Q, Anand-Apte B, Parat MO. Altered angiogenesis in caveolin-1 gene-deficient mice is restored by ablation of endothelial nitric oxide synthase. Am J Pathol. 2012 Apr;180(4):1702-1714.
Anesthesiology
Farag E, Sessler DI, Kovaci B, Wang L, Mascha EJ, Bell G, Kalfas I, Rockwood E, Kurz A. Effects of crystalloid versus col-loid and the alpha-2 agonist brimonidine versus placebo on intraocular pressure during prone spine surgery: a factorial randomized trial. Anesthesiology. 2012 Apr;116(4):807-815.
Annu.Rev.Biomed.Eng.
Ruberti JW, Sinha Roy A, Roberts CJ. Cor-neal biomechanics and biomaterials. Annu Rev Biomed Eng. 2011 Aug 15;13:269-295.
Arch.Ophthalmol.
Charkoudian LD, Kaiser GM, Steinmetz RL, Srivastava SK. Acute retinal necrosis after herpes zoster vaccination. Arch Ophthalmol. 2011 Nov;129(11):1495-1497.
Ehlers JP, Kernstine K, Farsiu S, Sarin N, Maldonado R, Toth CA. Analysis of pars plana vitrectomy for optic pit-related maculopathy with intraoperative optical co-herence tomography: a possible connection with the vitreous cavity. Arch Ophthalmol. 2011 Nov;129(11):1483-1486.
Gabriel LAR, Sachdeva R, Marcotty A, Rock-wood EJ, Traboulsi EI. Oculodentodigital dysplasia: new ocular findings and a novel connexin 43 mutation. Arch Ophthalmol. 2011 Jun;129(6):781-784.
Lowder C, Belfort R, Jr., Lightman S, Foster CS, Robinson MR, Schiffman RM, Li XY, Cui H, Hollander DA, Hashad Y, Whitcup SM. A report of high intraocular pressure with the dexa-methasone intravitreal implant - reply. Arch Ophthalmol. 2011 Dec;129(12):1639-1640.
Lowder C, Belfort R, Jr., Lightman S, Foster CS, Robinson MR, Schiffman RM, Li XY, Cui H, Whitcup SM. Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis. Arch Ophthalmol. 2011 May;129(5):545-553.
Arthritis Care Res.(Hoboken)
Angeles-Han ST, Griffin KW, Harrison MJ, Lehman TJA, Leong T, Robb RR, Shainberg M, Ponder L, Lenhart P, Hutchinson A, Sriv-astava SK, Prahalad S, Lambert SR, Drews-Botsch C. Development of a vision-related
Cole Eye Institute Publications

23
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n v e s t i g a t i o n s
quality of life instrument for children ages 8-18 years for use in juvenile idiopathic arthritis-associated uveitis. Arthritis Care Res (Hoboken). 2011 Sep;63(9):1254-1261.
Tarabishy AB, Ahn E, Mandell BF, Lowder CY. Central serous retinopathy. Arthritis Care Res (Hoboken). 2011 Aug;63(8):1075-1082.
Br.J.Ophthalmol.
Hallahan KM, Sood A, Singh AD. Acute episode of eyelid oedema. Br J Ophthalmol. 2012 Jun;96(6):909, 913.
Seregard S, Singh AD. Retinoblastoma: direct chemotherapeutic drug delivery into the vitreous cavity. Br J Ophthalmol. 2012 Apr;96(4):473-474.
Steinle NC, Gupta N, Yuan A, Singh RP. Oral rifampin utilisation for the treatment of chronic multifocal central serous retinopa-thy. Br J Ophthalmol. 2012 Jan;96(1):10-13.
Tarabishy AB, Khatib OF, Nocero JR, Budev M, Kaiser PK. Ocular complications in patients with lung transplants. Br J Ophthal-mol. 2011 Sep;95(9):1295-1298.
Can.J.Ophthalmol.
Cherfan CG, Traboulsi EI. Slipped, severed, torn and lost extraocular muscles. Can J Ophthalmol. 2011 Dec;46(6):501-509.
Ehlers JP, Chavala SH, Woodward JA, Postel EA. Delayed recalcitrant fungal endo-phthalmitis secondary to Curvularia. Can J Ophthalmol. 2011 Apr;46(2):199-200.
Chem.Res.Toxicol.
Salomon RG, Hong L, Hollyfield JG. Discov-ery of carboxyethylpyrroles (CEPs): Critical insights into AMD, autism, cancer, and wound healing from basic research on the chemistry of oxidized phospholipids. Chem Res Toxicol. 2011 Nov 21;24(11):1803-1816.
Clin.Experiment.Ophthalmol.
Martin DF, Maguire MG, Fine SL. Bevaci-zumab: Not as good with more adverse reac-tions? Response. Clin Experiment Ophthal-mol. 2011 Sep-Oct;39(7):718-720.
Clinics (Sao Paulo)
Medeiros FW, Sinha-Roy A, Alves MR, Dupps WJ, Jr. Biomechanical corneal changes induced by different flap thickness created by femtosecond laser. Clinics (Sao Paulo). 2011;66(6):1067-1071.
Mello GR, Pizzolatti ML, Wasilewski D, San-thiago MR, Budel V, Moreira H. The effect of subconjunctival bevacizumab on corneal neovascularization, inflammation and re-epithelization in a rabbit model. Clinics (Sao Paulo). 2011;66(8):1443-1450.
Cornea
Ghanem RC, Netto MV, Ghanem VC, San-thiago MR, Wilson SE. Peripheral sterile corneal ring infiltrate after riboflavin-UVA collagen cross-linking in keratoconus. Cornea. 2012 Jun;31(6):702-705.
Santhiago MR, Netto MV, Wilson SE. Mito-mycin C: biological effects and use in refrac-tive surgery. Cornea. 2012 Mar;31(3):311-321.
Santhiago MR, Wilson SE. Cellular effects after laser in situ keratomileusis flap for-mation with femtosecond lasers: a review. Cornea. 2012 Feb;31(2):198-205.
Curr.Eye Res.
DeCroos FC, Ehlers JP, Stinnett S, Fekrat S. Intravitreal bevacizumab for macu-lar edema due to central retinal vein occlusion: Perfused vs. ischemic and early vs. late treatment. Curr Eye Res. 2011 Dec;36(12):1164-1170.
Endocr.Pract.
Payne JF, Ray R, Watson DG, Delille C, Rimler E, Cleveland J, Lynn MJ, Tangpricha V, Srivastava SK. Vitamin D insufficiency in diabetic retinopathy. Endocr Pract. 2012 Mar-Apr;18(2):185-193.
Eur.J.Ophthalmol.
Hood CT, Budd GT, Zakov ZN, Singh AD. Male breast carcinoma metastatic to the choroid: report of 3 cases and review of the literature. Eur J Ophthalmol. 2011 Jul-Aug;21(4):459-467.
Exp.Eye Res.
Barbosa FL, Lin M, Santhiago MR, Singh V, Agrawal V, Wilson SE. Interleukin-1 recep-tor role in the viability of corneal myofibro-blasts. Exp Eye Res. 2012 Mar;96(1):65-69.
Grossman GH, Watson RF, Pauer GJT, Bollinger K, Hagstrom SA. Immunocyto-chemical evidence of Tulp1-dependent outer segment protein transport pathways in photoreceptor cells. Exp Eye Res. 2011 Nov;93(5):658-668.
Hollyfield JG. Manuscript fabrication, im-age manipulation and plagiarism. Exp Eye Res. 2012 Jan;94(1):1-2.
Santhiago MR, Singh V, Barbosa FL, Agrawal V, Wilson SE. Monocyte develop-ment inhibitor PRM-151 decreases corneal myofibroblast generation in rabbits. Exp Eye Res. 2011 Nov;93(5):786-789.
Singh V, Santhiago MR, Barbosa FL, Agrawal V, Singh N, Ambati BK, Wilson SE. Effect of TGFbeta and PDGF-B blockade on corneal myofibroblast development in mice. Exp Eye Res. 2011 Dec;93(6):810-817.

24
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Singh V, Agrawal V, Santhiago MR, Wilson SE. Stromal fibroblast-bone marrow-derived cell interactions: Implications for myofibro-blast development in the cornea. Exp Eye Res. 2012 May;98(1):1-8.
Wilson SE. Corneal myofibroblast biology and pathobiology: Generation, persis-tence, and transparency. Exp Eye Res. 2012 Jun;99(1):78-88.
Yu M, Sturgill-Short G, Ganapathy P, Taw-fik A, Peachey NS, Smith SB. Age-related changes in visual function in cystathio-nine-beta-synthase mutant mice, a model of hyperhomocysteinemia. Exp Eye Res. 2012 Mar;96(1):124-131.
Expert Opin.Biol.Ther.
Dhoot DS, Kaiser PK. Ranibizumab for age-related macular degeneration. Expert Opin Biol Ther. 2012 Mar;12(3):371-381.
Expert Opin.Pharmacother.
Ohr M, Kaiser PK. Intravitreal aflibercept injection for neovascular (wet) age-related macular degeneration. Expert Opin Pharma-cother. 2012 Mar;13(4):585-591.
Expert Rev.Ophthalmol.
Steinle N, Barakat M, Moshfeghi D, Kaiser PK. Radiation therapy in the treatment of exuda-tive age-related macular degeneration. Expert Rev Ophthalmol. 2011 Jun;6(3):323-337.
Future Oncol.
Triozzi PL, Singh AD. Blood biomarkers for uveal melanoma. Future Oncol. 2012 Feb;8(2):205-215.
Int.Ophthalmol.Clin.
Dhoot DS, Martin DF, Srivastava SK. Pediat-ric infectious posterior uveitis. Int Ophthal-mol Clin. 2011 Winter;51(1):113-128.
Sears NC, Sears JE. Oxygen and retinopathy of prematurity. Int Ophthalmol Clin. 2011 Winter;51(1):17-31.
Invest.Ophthalmol.Vis.Sci.
Bollinger KE, Crabb JS, Yuan X, Putliwala T, Clark AF, Crabb JW. Quantitative pro-teomics: TGF{beta}2 signaling in trabecular meshwork cells. Invest Ophthalmol Vis Sci. 2011;52(11):8287-8294.
Bonilha VL, Rayborn ME, Li Y, Grossman GH, Berson EL, Hollyfield JG. Histopathol-ogy and functional correlations in a patient with a mutation in RPE65, the gene for retinol isomerase. Invest Ophthalmol Vis Sci. 2011;52(11):8381-8392.
Ebrahem Q, Qi JH, Sugimoto M, Ali M, Sears JE, Cutler A, Khokha R, Vasanji A, Anand-Apte B. Increased neovascularization in mice lacking tissue inhibitor of metal-loproteinases-3. Invest Ophthalmol Vis Sci. 2011;52(9):6117-6123.
Ehlers JP, Tao YK, Farsiu S, Maldonado R, Izatt JA, Toth CA. Integration of a spectral domain optical coherence tomography system into a surgical microscope for intra-operative imaging. Invest Ophthalmol Vis Sci. 2011;52(6):3153-3159.
Gabriel LAR, Wang LW, Bader H, Ho JC, Majors AK, Hollyfield JG, Traboulsi EI, Apte SS. ADAMTSL4, a secreted glycoprotein widely distributed in the eye, binds fibril-lin-1 microfibrils and accelerates microfi-bril biogenesis. Invest Ophthalmol Vis Sci. 2012;53(1):461-469.
Hong CW, Sinha Roy A, Schoenfield L, Mc-Mahon JT, Dupps WJ, Jr. Collagenase-medi-ated tissue modeling of corneal ectasia and collagen cross-linking treatments. Invest Ophthalmol Vis Sci. 2012;53(4):2321-2327.
Singh AD, Aronow ME, Sun Y, Bebek G, Saunthararajah Y, Schoenfield LR, Biscotti CV, Tubbs RR, Triozzi PL, Eng C. Chro-mosome 3 status in uveal melanoma: a comparison of fluorescence in situ hybridization and single-nucleotide poly-morphism array. Invest Ophthalmol Vis Sci. 2012;53(7):3331-3339.
Sinha Roy A, Dupps WJ, Jr. Patient-specific computational modeling of keratoconus progression and differential responses to collagen cross-linking. Invest Ophthalmol Vis Sci. 2011;52(12):9174-9187.
Triozzi PL, Aldrich W, Singh A. Effects of interleukin-1 receptor antagonist on tumor stroma in experimental uveal melanoma. Invest Ophthalmol Vis Sci. 2011;52(8):5529-5535.
J.AAPOS
Natan K, Traboulsi EI. Unilateral rectus muscle recession in the treatment of Duane syndrome. J AAPOS. 2012 Apr;16(2):145-149.
Nicholson BP, De Alba M, Perry JD, Traboul-si EI. Efficacy of the intraoperative relaxed muscle positioning technique in thyroid eye disease and analysis of cases requiring reop-eration. J AAPOS. 2011 Aug;15(4):321-325.
Sachdeva R, Turell ME, Meadows SR, Emch TM, Singh AD. Congenital intradiploic arachnoid cyst presenting as painless pro-ptosis. J AAPOS. 2011 Dec;15(6):601-603.
Sachdeva R, Schoenfield L, Marcotty A, Singh AD. Retinoblastoma with autoinfarc-tion presenting as orbital cellulitis. J AAPOS. 2011 Jun;15(3):302-304.
J.Biol.Chem.
Wu C, Agrawal S, Vasanji A, Drazba J, Sarkaria S, Xie J, Welch CM, Liu M, Anand-Apte B, Horowitz A. Rab13-dependent traf-ficking of RhoA is required for directional migration and angiogenesis. J Biol Chem. 2011 Jul 1;286(26):23511-23520.
J.Cataract Refract.Surg.
Kara-Junior N, Espindola RF, Gomes BAF, Ventura B, Smadja D, Santhiago MR. Effects of blue light-filtering intraocular lenses on the macula, contrast sensitivity, and color vision after a long-term follow-up. J Cataract Refract Surg. 2011 Dec;37(12):2115-2119.
Santhiago MR, Wilson SE, Netto MV, Ghanen RC, Monteiro MLR, Bechara SJ, Espana EM, Mello GR, Kara-Junior N. Modulation transfer function and optical quality after bilateral implantation of a +3.00 D versus a +4.00 D multifocal intra-ocular lens. J Cataract Refract Surg. 2012 Feb;38(2):215-220.
Smadja D, Santhiago MR, Mello GR, Espana EM, Krueger RR. Suction loss during thin-flap femto-LASIK: Manage-ment and beneficial refractive effect of the epithelium. J Cataract Refract Surg. 2012 May;38(5):902-905.
Wilson SE, Santhiago MR. Flaporhexis: Rapid and effective technique to limit epi-thelial ingrowth after LASIK enhancement. J Cataract Refract Surg. 2012 Jan;38(1):2-4.

25
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n v e s t i g a t i o n s
J.Fr.Ophtalmol.
Smadja D, Reggiani-Mello G, Touboul D, Colin J. Les profils de photoablation cornéenne en chirurgie réfractive. Partie 1: la quête de l’excellence [Ablation profiles in refractive surgery. Part 1: In search of excellence] [French]. J Fr Ophtalmol. 2012 Feb;35(2):126-135.
J.Refract.Surg.
Ambrosio R, Jr., Caiado ALC, Guerra FP, Louzada R, Sinha-Roy A, Luz A, Dupps WJ, Belin MW. Novel pachymetric parameters based on corneal tomography for diag-nosing keratoconus. J Refract Surg. 2011 Oct;27(10):753-758.
Morales EL, Rocha KM, Chalita MR, Nose W, Avila MP. Comparison of optical aberrations and contrast sensitivity between aspheric and spherical intraocular lenses. J Refract Surg. 2011 Oct;27(10):723-728.
Salomao MQ, Chaurasia SS, Sinha Roy A, Ambrosio R, Jr., Esposito A, Sepulveda R, Agrawal V, Wilson SE. Corneal wound heal-ing after ultraviolet-A/riboflavin collagen cross-linking: a rabbit study. J Refract Surg. 2011 Jun;27(6):401-407.
Santhiago MR, Barbosa FL, Agrawal V, Binder PS, Christie B, Wilson SE. Short-term cell death and inflammation after intracor-neal inlay implantation in rabbits. J Refract Surg. 2012 Feb;28(2):144-149.
Santhiago MR, Wilson SE, Netto MV, Es-pindola RF, Shah RA, Ghanem RC, Bechara SJ, Kara-Junior N. Visual performance of an apodized diffractive multifocal intraocular lens with +3.00-d addition: 1-year follow-up. J Refract Surg. 2011 Dec;27(12):899-906.
Smadja D, Reggiani-Mello G, Santhiago MR, Krueger RR. Wavefront ablation profiles in refractive surgery: description, results, and limitations. J Refract Surg. 2012 Mar;28(3):224-232.
Johns Hopkins Advanced Studies in Ophthalmology
Do DV, Gordon D, Kaiser PK. Impact of AMD and treatment regimens on patient-report-ed visual function. Johns Hopkins Advanced Studies in Ophthalmology. 2011;8(1):9-15.
Mol.Vis.
Payne JF, Tangpricha V, Cleveland J, Lynn MJ, Ray R, Srivastava SK. Serum insulin-like growth factor-I in diabetic retinopathy. Mol Vis. 2011;17:2318-2324.
Monogr.Clin.Cytol.
Biscotti CV, Singh AD. Uveal melanoma: diagnostic features. Monogr Clin Cytol. 2012;21:44-54.
Biscotti CV, Singh AD. Uveal metastases. Monogr Clin Cytol. 2012;21:17-30.
Chute DJ, Biscotti CV, Singh AD. Uveal lym-phoma. Monogr Clin Cytol. 2012;21:31-43.
Singh AD, Dolan B, Biscotti CV. Future of ophthalmic fine needle aspiration biopsy. Monogr Clin Cytol. 2012;21:90-96.
Singh AD, Pelayes DE, Brainard JA, Biscotti CV. History, indications, techniques and limitations. Monogr Clin Cytol. 2012;21:1-9.
Turell ME, Tubbs RR, Biscotti CV, Singh AD. Uveal melanoma: prognostication. Monogr Clin Cytol. 2012;21:55-60.
N.Engl.J.Med.
Martin DF, Maguire MG, Fine SL. The authors reply [Ranibizumab and bevaci-zumab for AMD]. N Engl J Med. 2011 Dec 8;365(23):2237.
Nat.Med.
Doyle SL, Campbell M, Ozaki E, Salomon RG, Mori A, Kenna PF, Farrar GJ, Kiang AS, Humphries MM, Lavelle EC, O’Neill LAJ, Hollyfield JG, Humphries P. NLRP3 has a protective role in age-related macular de-generation through the induction of IL-18 by drusen components. Nat Med. 2012 May;18(5):791-798.
Neuron
Matsuoka RL, Chivatakarn O, Badea TC, Samuels IS, Cahill H, Katayama K, Kumar SR, Suto F, Chedotal A, Peachey NS, Nathans J, Yoshida Y, Giger RJ, Kolodkin AL. Class 5 transmembrane semaphorins control selec-tive Mammalian retinal lamination and func-tion. Neuron. 2011 Aug 11;71(3):460-473.
Ocul.Immunol.Inflamm.
Gangaputra SS, Altaweel MM, Peng Q, Fried-man DS, Rao PK, Foster CS, Kim RY, Reed SB, Srivastava SK, Wong IG, Kempen JH.
Morphologic assessment for glaucoma in the Multicenter Uveitis Steroid Treatment (MUST) trial. Ocul Immunol Inflamm. 2011 Aug;19(4):267-274.
Stewart JM, Srivastava SK, Fung AE, Mah-moud TH, Telander DG, Hariprasad SM, Ober MD, Mruthyunjaya P. Bacterial con-tamination of needles used for intravitreal injections: a prospective, multicenter study. Ocul Immunol Inflamm. 2011 Feb;19(1):32-38.
Ocular Surgery News
Bakri SJ, Cousins SW, Gower EW, Kaiser PK, Martin DF, Rich WL, III. CATT, Hopkins analysis add fervor to ranibizumab vs. beva-cizumab debate. Ocular Surgery News. 2011 Aug 10;29(15):1-12.
Ophthal.Plast.Reconstr.Surg.
Goshe JM, Lewis CD, Meine JG, Schoen-field L, Perry JD. Primary dermatofibro-sarcoma protuberans invading the orbit. Ophthal Plast Reconstr Surg. 2012 May-Jun;28(3):e65-e67.
Lee BJ, Nelson CC, Lewis CD, Perry JD. Ex-ternal dacryocystorhinostomy outcomes in sarcoidosis patients. Ophthal Plast Reconstr Surg. 2012 Jan-Feb;28(1):47-49.
Pasquali TA, Mehta MP, Perry JD. Conjunc-tival bleeding after ectropion repair due to paraneoplastic primary fibrinolysis. Ophthal Plast Reconstr Surg. 2012 Mar-Apr;28(2):e44-e45.
Perry JD, Lewis CD. Lacrimal canalicular transposition with composite eyelid graft. Ophthal Plast Reconstr Surg. 2011 Jul-Aug;27(4):306-307.
Ophthalmic Genet.
Turell ME, Leonardy NJ, Singh AD. A unique presentation of grouped congenital hyper-trophy of the retinal pigment epithelium. Ophthalmic Genet. 2011 Sep;32(3):162-164.
Ophthalmic Surg.Lasers Imaging
Canton VM, Quiroz-Mercado H, Velez-Montoya R, Lopez-Miranda MJ, Moshfeghi AA, Shusterman EM, Kaiser PK, Sanislo SR, Gertner M, Moshfeghi DM. 16-Gy low-voltage x-ray irradiation with ranibizumab therapy for AMD: 6-month safety and func-tional outcomes. Ophthalmic Surg Lasers Imaging. 2011 Nov-Dec;42(6):468-473.

26
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Canton VM, Quiroz-Mercado H, Velez-Montoya R, Lopez-Miranda MJ, Moshfeghi AA, Shusterman EM, Kaiser PK, Sanislo SR, Gertner M, Moshfeghi DM. 24-Gy low-volt-age x-ray irradiation with ranibizumab ther-apy for neovascular AMD: 6-month safety and functional outcomes. Ophthalmic Surg Lasers Imaging. 2012 Jan-Feb;43(1):20-24.
Lee LB, Srivastava SK. Intraoperative spec-tral-domain optical coherence tomography during complex retinal detachment repair. Ophthalmic Surg Lasers Imaging. 2011;42 Online:e71-e74.
Moshfeghi AA, Canton VM, Quiroz-Mercado H, Velez-Montoya R, Lopez-Miranda MJ, Shusterman EM, Kaiser PK, Sanislo SR, Gertner M, Moshfeghi DM. 16-Gy low-volt-age x-ray irradiation followed by as-needed ranibizumab therapy for AMD: 6-month outcomes of a “radiation-first” strategy. Ophthalmic Surg Lasers Imaging. 2011 Nov-Dec;42(6):460-467.
Ophthalmology
Bollinger K, Kim J, Lowder CY, Kaiser PK, Smith SD. Intraocular pressure outcome of patients with fluocinolone acetonide in-travitreal implant for noninfectious uveitis. Ophthalmology. 2011 Oct;118(10):1927-1931.
Kaiser PK, Boyer DS, Cruess AF, Slakter JS, Pilz S, Weisberger A. Verteporfin plus ranibizumab for choroidal neovasculariza-tion in age-related macular degeneration: Twelve-month results of the DENALI study. Ophthalmology. 2012 May;119(5):1001-1010.
Ray R, Baranano DE, Fortun JA, Schwent BJ, Cribbs BE, Bergstrom CS, Hubbard GB, III, Srivastava SK. Intraoperative microscope-mounted spectral domain optical coher-ence tomography for evaluation of retinal anatomy during macular surgery. Ophthal-mology. 2011 Nov;118(11):2212-2217.
Schachat AP. Better outcomes for patients with diabetic macular edema. Ophthalmol-ogy. 2011 Apr;118(4):607-608.
Singh AD, Turell ME, Topham AK. Uveal melanoma: trends in incidence, treat-ment, and survival. Ophthalmology. 2011 Sep;118(9):1881-1885.
Thorne JE, Van Natta ML, Jabs DA, Duncan JL, Srivastava SK. Visual field loss in patients
with cytomegalovirus retinitis. Ophthalmology. 2011 May;118(5):895-901.
Orbit
Pasquali T, Schoenfield L, Spalding SJ, Singh AD. Orbital inflammation in IgG4-related sclerosing disease. Orbit. 2011 Oct;30(5):258-260.
Plast.Reconstr.Surg.
Czyz CN, Rich NE, Foster JA, Kavanagh MC, Perry JD, Holck DEE. Comparison of postop-erative eyelid position using fibrin sealant versus suture for wound closure in Müller’s muscle-conjunctiva resection ptosis repair. Plast Reconstr Surg. 2011 Aug;128(2):423-430.
PLoS ONE
Gu X, Neric NJ, Crabb JS, Crabb JW, Bhat-tacharya SK, Rayborn ME, Hollyfield JG, Bonilha VL. Age-related changes in the retinal pigment epithelium (RPE). PLoS ONE. 2012;7(6):e38673.
Sivakumaran TA, Igo RP, Jr., Kidd JM, Itsara A, Kopplin LJ, Chen W, Hagstrom SA, Peachey NS, Francis PJ, Klein ML, Chew EY, Ramprasad VL, Tay WT, Mitchell P, Seiels-tad M, Stambolian DE, Edwards AO, Lee KE, Leontiev DV, Jun G, Wang Y, Tian L, Qiu F, Henning AK, Laframboise T, Sen P, Aarthi M, George R, Raman R, Das MK, Vijaya L, Kumaramanickavel G, Wong TY, Swaroop A, Abecasis GR, Klein R, Klein BEK, Nickerson DA, Eichler EE, Iyengar SK. A 32 kb critical region excluding Y402H in CFH mediates risk for age-related macular degeneration. PLoS ONE. 2011;6(10):e25598.
Retin.Cases Brief Rep.
Barakat MR, Sachdeva R, Sepulveda RN, Schoenfield L, Dupps WJ Jr., Sears JE. Man-agement of posteriorly dislocated endotheli-al keratoplasty donor lenticule. Retin Cases Brief Rep. 2011 Spring;5(2):163-164.
Retina
Ehlers JP, DeCroos FC, Fekrat S. Intravitreal bevacizumab for macular edema second-ary to branch retinal vein occlusion. Retina. 2011 Oct;31(9):1856-1862.
Ehlers JP, Maldonado R, Sarin N, Toth CA. Treatment of non-age-related macular degeneration submacular diseases with macular translocation surgery. Retina. 2011 Jul;31(7):1337-1346.
Payne JF, Bergstrom C, Yan J, Aaberg TM, Sr., Srivastava SK. Residual triamcino-lone acetonide sequestered in the fovea after macular hole repair. Retina. 2011 Jan;31(1):148-153.
Retina Today
Brown DM, Dugel PU, Humayun MS, Kaiser PK, Trese MT. Symptomatic vitreomacular adhesion (VMA): Diagnosis, pathologic im-plications, and management. Retina Today. 2011 Aug;(Suppl):4-12.
Ehlers JP. Intraoperative OCT and vitreo-retinal surgery: This technology has the potential to improve clinical outcomes and enhance understanding of the pathophysi-ology of a wide variety of surgical vitreoreti-nal diseases. Retina Today. 2011 Sep;50-53.
Taban M, Sonnie C, Hayden BC, Sears JE. Ultrasound biomicroscopy-guided surgical intervention for cyclodialysis clefts. Retina Today. 2011 May-Jun;38-41.
Rev.Bras.Oftalmol.
da Silva RS, da Silva JAS, de Lima FBF, Val-bon BF, Salomao MQ, Junior RA. Estudo das correlações entre a área do disco óptico e as características geométricas e biomecânicas da córnea [Study of correlation between optic disc size and corneal geometry and biomechanics] [Portuguese]. Rev Bras Oftal-mol. 2011 Nov;70(6):349-357.
Pereira IC, Saraiva PGC, Saraiva FP, de Medeiros FW, Miki G, Matayoshi S. Análise da ceratometria corneana em pacientes portadores de espasmo hemifacial [Analysis of corneal keratometry in patients with hemifacial spasm] [Portuguese]. Rev Bras Oftalmol. 2011 Nov;70(6):363-366.
Saudi Journal of Ophthalmology
Singh AD, Biscotti CV. Fine needle aspiration biopsy of ophthalmic tumors. Saudi Journal of Ophthalmology. 2012;26(2):117-123.
Semin.Oncol.
Saunthararajah Y, Triozzi P, Rini B, Singh A, Radivoyevitch T, Sekeres M, Advani A, Tiu R, Reu F, Kalaycio M, Copelan E, Hsi E, Lichtin A, Bolwell B. p53-Independent, normal stem cell sparing epigenetic differentiation therapy for myeloid and other malignancies. Semin Oncol. 2012 Feb;39(1):97-108.

27
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | i n v e s t i g a t i o n s
Semin.Ophthalmol.
Silva RA, Moshfeghi AA, Kaiser PK, Singh RP, Moshfeghi DM. Radiation treatment for age-related macular degeneration. Semin Ophthalmol. 2011 May;26(3):121-130.
Surv.Ophthalmol.
Ehlers JP, Fekrat S. Retinal vein occlusion: beyond the acute event. Surv Ophthalmol. 2011 Jul-Aug;56(4):281-299.
Espana EM, Levine M, Schoenfield L, Singh AD. Ocular surface squamous neoplasia in an anophthalmic socket 60 years after enucleation. Surv Ophthalmol. 2011 Nov-Dec;56(6):539-543.
WhOLE BOOk
LaVail MM, Ash JD, Anderson RE, Hollyfield JG, Grimm C. Retinal Degenerative Diseases. New York, NY: Springer; 2012. 407 pgs.
BOOk ChAPTERS
Age-related macular degeneration diagnosis and treatment
Steinle N, Kaiser PK. Combination therapy with ocular photodynamic therapy for age-related macular degeneration. In: Ho AC, Regillo CD, eds. Age-Related Macular Degeneration Diagnosis and Treatment. New York, NY: Springer; 2011:99-118.
Clinical atlas of procedures in ophthalmic and oculofacial surgery
McGannon P, Koch DD, Weikert MP. Pho-torefractive keratectomy (PRK). In: Albert DM, Lucarelli MJ, eds. Clinical Atlas of Procedures in Ophthalmic and Oculofacial Surgery. 2nd ed. New York, NY: Oxford Uni-versity Press; 2012:85-100.
Gass’ atlas of macular diseases
Singh AD, Agarwal A. Tumors of the retinal pigment epithelium (RPE). In: Agarwal A, ed. Gass’ Atlas of Macular Diseases. 5th ed. Ed-inburgh: Elsevier Saunders; 2012:1065-1097.
Singh AD, Agarwal A. Neoplastic diseases of the retina. In: Agarwal A, ed. Gass’ Atlas of Macular Diseases. 5th ed. Edinburgh: Elsevier Saunders; 2012:1099-1178.
Singh AD, Agarwal A. Neoplastic diseases of the choroid. In: Agarwal A, ed. Gass’ Atlas of Macular Diseases. 5th ed. Edinburgh: Elsevier Saunders; 2012:1179-1253.
Macular Surgery
Singh RP, Kaiser PK. New and future antian-giogenic therapy. In: Quiroz-Mercado H, ed. Macular Surgery. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:108-114.
Singh RP, Lewis H. Submacular hemor-rhage. In: Quiroz-Mercado H, ed. Macular Surgery. 2nd ed. Philadelphia, PA: Lippin-cott Williams & Wilkins; 2011:459-465.
Ophthalmic Surgery: Principles and Practice
Dupps WJ Jr., Hallahan K. Biomechanics in refractive surgery. In: Spaeth GL, ed. Ophthalmic Surgery: Principles and Practice. 4th ed. Edinburgh: Elsevier; 2012:172-178.
Singh AD, Schachat AP. Treatment of retinal capillary angioma. In: Spaeth GL, ed. Ophthalmic Surgery: Principles and Practice. 4th ed. Edinburgh: Elsevier; 2012:622-623.
Ophthalmology Review Manual
Hariprasad SM, Ahmed I, Bakri SJ, Con-way MD, Mahmoud TH, Moshfeghi AA, Mruthyunjaya P, Ober MD, Srivastava SK, Telander DG, Vu CD. Retina and vitreous. In: Chern KC, Saidel MA, eds. Ophthalmology Review Manual. 2nd ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2012:99-227.
Pediatric Retina
Fu EX, Singh AD. Phacomatoses. In: Reynolds JD, Olitsky SE, eds. Pediatric Retina. Heidelberg; New York, NY: Springer; 2011:159-189.
Hood C, Lowder CY. Pediatric uveitis. In: Reynolds JD, Olitsky SE, eds. Pediatric Retina. Heidelberg; New York, NY: Springer; 2011:433-457.
Sears JE. Macular choroidal neovasculariza-tion and defects in Bruch’s membrane in children. In: Reynolds JD, Olitsky SE, eds. Pediatric Retina.Heidelberg; New York, NY: Springer; 2011:345-349.
Phacoemulsification
Mello GR, Talamo JH, Krueger RR. Fem-tosecond laser-assisted refractive cataract surgery. In: Agarwal A, Agarwal A, Jacob S, eds. Phacoemulsification. 4th ed. New Delhi: Jaypee Medical Publishers; 2012:559-565.
Studies on Retinal and Choroidal Disorders
Anand-Apte B. Dysfunction of circulating endothelial progenitor cells in diabetic retinopathy. In: Stratton RD, Hauswirth WW, Gardner TW, eds. Studies on Retinal and Choroidal Disorders. New York, NY: Humana Press; 2012:517-528.
Crabb JW. Oxidative modifications as triggers of AMD pathology. In: Stratton RD, Hauswirth WW, Gardner TW, eds. Studies on Retinal and Choroidal Disorders. New York, NY: Humana Press; 2012:65-84.
Surgery of the Eyelids, Lacrimal System, and Orbit
Perry JD, Lewis C. Surgical decompression of the orbit. In: Yen MT, ed. Surgery of the Eyelids, Lacrimal System, and Orbit. 2nd ed. New York, NY: Oxford University Press; 2012:265-278.
Uveitis
Charkodian L, Srivastava SK. Kawasaki’s dis-ease. In: Garg SJ, ed. Uveitis. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2012:108-109.
Payne JF, Srivastava SK. Cancer-associated retinopathy syndrome. In: Garg SJ, ed. Uve-itis. Philadelphia, PA: Wolters Kluwer/Lip-pincott Williams & Wilkins; 2012:297-299.
Wills Eye Institute 5-Minute Ophthalmology Consult
Ehlers JP. Toxocariasis. In: Maguire JI, Mur-chison AP, Jaeger EA, eds. Wills Eye Institute 5-Minute Ophthalmology Consult. Philadel-phia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2012:680.
Helping Professionals Develop

29
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | e d u C a t i o n
Cole Eye Institute CMEMark your calendars for continuing medical education symposia hosted by Cole Eye Institute. You’ll
gain insights into state-of-the-art diagnostic, medical and surgical techniques, as well as the prom-
ise that research holds for patients with ophthalmic conditions.
Ophthalmic Ultrasonography: Practical AspectsFor ophthalmologists, optometrists,
nurses, technicians, photographers
and others
Friday-Saturday, March 15-16, 2013
Location: InterContinental Hotel and
Conference Center, Cleveland, Ohio
Activity Directors:
Arun D. Singh, MD
Brandy Hayden
Uveitis Update Saturday, April 20, 2013
Location: Cole Eye Institute
Cleveland, Ohio
Activity Directors:
Careen Lowder, MD, PhD
Sunil K. Srivastava, MD
Retina Summit (date pending for May 2013)
Location: Cole Eye Institute
Cleveland, Ohio
Activity Directors:
Daniel F. Martin, MD
Sunil K. Srivastava, MD
International Society of Ocular Oncology (ISOO 2013) - NON-CME Sunday - Thursday,
September 29 - October 3, 2013
Location: InterContinental Hotel and
Conference Center, Cleveland, Ohio
Activity Director:
Arun D. Singh, MD
Most CME courses will be held at the Cole Eye Institute’s James P. Storer Conference Center. For details, exact location or to confirm dates for any of our 2013 CME courses, please contact Jane Sardelle at [email protected].

30
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Training the Leaders of Tomorrow
Residency ProgramsOur residency training program’s mission is to prepare
future leaders in patient care, teaching and vision research.
The program meets all the requirements of the American
Board of Ophthalmology and the Accreditation Council for
Graduate Medical Education.
Four residents are matched annually in the three-year
program. Residents rotate among the Institute’s nine de-
partments and at MetroHealth Medical Center, Cleveland
Clinic Lakeland and Cleveland Clinic Stephanie Tubbs
Jones Health Center. Residents work under the direct
supervision of the staff during each rotation through:
• Cornea, external disease, anterior segment
• Glaucoma
• Neuro-ophthalmology/oncology
• Ophthalmic pathology
• Ophthalmic plastic, reconstructive and orbital surgery
• Pediatric ophthalmology and adult strabismus
• Refractive surgery
• Retina, vitreous, low vision
• Uveitis, ocular inflammatory disease and immunology
This curriculum provides a balanced exposure to all subspe-
cialty areas of ophthalmology, ensuring graduates the ability
to perform general ophthalmology with skill, knowledge and
confidence. Each resident works in a one-on-one relationship
with a staff physician to provide the best opportunity to study
disease processes and their medical and surgical manage-
ment. This arrangement also provides excellent supervision
and optimal continuity of patient care in the outpatient and
hospital settings.
Residents are expected to participate in clinical and basic
research activities utilizing the staff’s expertise. They com-
plete independent clinical research projects that involve re-
viewing the literature, developing a hypothesis, and designing
and executing the study. Activities are carefully supervised by
an experienced clinical investigator. Residents are expected
to submit and present their research at national meetings
and to write several papers for publication based on their
research activities. Each June, ophthalmology residents, fel-
lows and staff participate in the Annual Research, Residents
and Alumni Meeting, a scientific forum for the presentation
of research projects.
Residency and fellowship training is considered a high priority at Cleveland Clinic Cole Eye Institute
and is led by outstanding faculty in a state-of-the-art facility. Our programs are highly competitive
and produce superbly trained clinical and academic ophthalmologists.

31
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | e d u C a t i o n
Residency Graduates
June 2012
Baseer Ahmad, MD
Eric Ahn, MD
Theodore Pasquali, MD
Xiang Werdich, MD, PhD
Breno Lima, MD
(February 2012)
Aimee Chappelow, MD
(December 2011)
Residents, First Year
July 2012 – June 2013
Katie Hallahan, MD
Priyanka Kumar, MD
Tal Rubinstein, MD
Jack Shao, MD
Residents, Second Year
July 2012 – June 2013
Jedediah McClintic, MD
Stephen McNutt, MD
Karolinne Rocha, MD, PhD
Georgios Trichonas, MD
Residents, Third Year
July 2012 – June 2013
Elisabeth Aponte, MD
John Au, MD
Igor Estrovich, MD
Sumit Sharma, MD
Fellowship ProgramWe offer high-quality fellowship training
opportunities in a variety of subspecial-
ties to create the next generation of
academic leaders in their fields. Training
combines an excellent academic envi-
ronment with close mentorship support.
Fellowships include:
• Two-year vitreoretinal fellowship
(two positions)
• One-year cornea, external disease
and refractive surgery fellowship
(two positions)
• One-year glaucoma fellowship
(one position)
• One-year pediatric ophthalmology
fellowship (one position)
• Two-year oculoplastics fellowship
(sponsored by ASOPRS) (one position)
• One-year ophthalmic oncology
fellowship (one position)
Fellowship Graduates
June 2012
Cornea, External Disease
and Refractive Surgery
Michael Savetsky, MD
Brent Timperley, MD
Glaucoma
Phyllis Eze, MD
Ophthalmic Oncology
no fellow
Pediatric Ophthalmology
Virginia Utz, MD
(August 2012)
Vitreoretinal Surgery
Dilsher Dhoot, MD
Alex Yuan, MD, PhD
Current Fellows
July 2012 to June 2013
Cornea, External Disease
and Refractive Surgery
Patrick Chan, MD
Neema Nayeb-Hashemi, MD
Glaucoma
Elisa Bala, MD
Oculoplastics
Bryan Costin, MD
Pediatric Ophthalmology
Virginia Utz, MD
(August 2012)
Palak Wall, MD
Vitreoretinal Surgery
Robert “Jack” Courtney, MD
Miriam Englander, MD
Matthew Ohr, MD
Omar Punjabi, MD
For more information about Cole Eye Institute fellowship programs, visit clevelandclinic.org/eyefellowships or ontact Jane Sardelle at [email protected].
32
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Distinguished Lecture SeriesThe Cleveland Clinic Cole Eye Institute is proud to present the 2012-2013 Distinguished Lecture
Series, which provides a forum for renowned researchers in the visual sciences to present their latest
research findings. This series of lectures will feature advances in many areas of ophthalmic research
presented by noted basic and clinical scientists from throughout the world. Ample opportunity for
questions and answers will be provided.
January 17, 2013
Discovery of New Glaucoma Pathogenic PathwaysAbbot Clark, PhD Professor, Cell Biology & Anatomy Director, North Texas Eye Research Institute University of North Texas Health Science Center Fort Worth, Texas
February 21, 2013
Mitochondrial Dysfunction: A Potential Mechanism for Age-Related Macular DegenerationDeborah Ferrington, PhD Associate Professor Departments of Ophthalmology and Visual Neurosciences University of Minnesota Minneapolis, Minn.
March 14, 2013
The Role of the Choriocapillaris in Early AMDRobert Mullins, PhD Hansjoerg E.J.W. Kolder, MD, PhD Associate Professor of Best Disease Research, Department of Ophthalmology & Visual Sciences University of Iowa Iowa City, Iowa
April 18, 2013
Genetic Control of Angiogenesis: Implications for ARMDRobert D’Amato, MD, PhD Judah Folkman Chair in Surgery Professor of Ophthalmology Harvard Medical School Vascular Biology Program Boston Children’s Hospital Boston, Mass.
May 16, 2013
Global Blindness: Can We Control It?Gullapalli Rao, MD Chairman, LV Prasad Eye Institute L V Prasad Marg Banjara Hills Hyderabad, Andhra Pradesh India
September 19, 2013
Responding to Clinical Need: Taking OCT Imaging Beyond Standard Clinical ApplicationsCynthia A. Toth, MD Professor of Ophthalmology and Biomedical Engineering Duke University Eye Center Durham, N.C.
October 17, 2013
The Hypoxic Response: Sought and Dreaded by the RetinaChristian Grimm, PhD Professor for Experimental Ophthalmology Department of Ophthalmology University of Zurich Schlieren, Zurich Switzerland
Cleveland Clinic Executive Education Learn from Top Healthcare ExecutivesThe competencies needed to lead and manage differ from those needed to be an effective administrator, clinician or scientist. Take advantage of this opportunity to acquire skills and insights into the business of healthcare excellence from top executives at Cleveland Clinic.
Two-day and two-week programs are open to healthcare executives, including physicians, nurses and administrators. Visit clevelandclinic.org/ExecutiveEducation for details, including the opportunity to earn 72.5 CME credits.
November 21, 2013
Leukocytes Take Directives from the Extracellular Matrix in Ocular Infections and InflammationShukti Chakravarti, PhD Associate Professor Departments of Medicine, Cell Biology and Ophthalmology Johns Hopkins University School of Medicine Baltimore, Md.
Please join us for these insights into ophthalmic research and the promises they hold for patient care. No registration is required; call 216.444.5832 with any questions.
The Distinguished Lecture Series is held from 7 to 8 a.m. in the James P. Storer Conference Center on the first floor of Cole Eye Institute. Attendees should park in the East 102nd Street parking lot (facing the front of Cole Eye Institute) or the visitor’s parking garage at East 100th Street and Carnegie Avenue. We will validate your parking ticket.

Our People, Our Results
34
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Cole Eye Institute OverviewAt Cleveland Clinic Cole Eye Institute, we have assembled a team of the world’s foremost clinicians
and researchers who are committed not only to delivering the finest healthcare available, but also
to improving tomorrow’s care through innovative basic, clinical and translational research.
W e believe that research
and patient care are inter-
dependent. Therefore, we
forge synergistic relationships through
analytical and integrative processes,
such as surgical outcomes analysis. We
are pioneering treatment protocols for
complex vision-threatening disorders
through our clinical trials and aggres-
sive research programs to shorten the
gap between the laboratory discoveries
of today and the patient care of tomor-
row. Our goal: Answering tomorrow’s
medical problems through today’s
laboratory and research endeavors.
Clinical Expertise
As one of the country’s leading compre-
hensive eye institutes, Cole Eye Institute
is able to enhance the lives of our patients
and to serve our referring physicians by
providing early, accurate diagnosis and
excellent, efficient, state-of-the-art care.
Our ophthalmology program was
ranked among the top 10 programs in
the nation in the most recent annual
U.S. News & World Report survey. We
have one of the largest patient volumes
in the United States, with more than
180,000 patient visits and more than
7,500 surgeries per year.
We offer primary, secondary and tertiary
ophthalmologic services for all ages.
Our internationally recognized staff of
45 ophthalmologists and researchers is
composed almost entirely of subspecial-
ists, and eight optometrists round out
our comprehensive services.
Patient-Centered Facilities
Cleveland Clinic Cole Eye Institute
offers state-of-the-art care at our main
campus and in the community. The
goal is to deliver maximum patient
comfort and optimum service and
quality. Our main campus building
allows us to provide the full spectrum
of clinical services at one location.
Exam lanes, a diagnostic services suite
and operating rooms are all housed in
one building, with features such as:
• Windows with special filters to
minimize light on dilated or newly
treated eyes.
• A comfortable waiting room with
a special play area for children.
• Valet parking and an easy post-
operative pickup area.
• Conveniently located food services.
For patients’ convenience, our regional
eye care program provides both general
ophthalmology and selected specialty
services at a number of locations.
Fostering Innovation
Our institute is specially designed
to enable clinicians to develop tomor-
row’s advances. Our facility includes an
Experimental Surgery Suite, one of the
few in the country with full operating
capacity.
Training future eye specialists is
greatly enhanced in the Education
Pavilion with the James P. Storer
Conference Center (designed with
televideo technology), as well as video
rooms, resident carrels and ample
conference space. ■
2 0 1 1 K e y s tat I s t I C s
Total clinic visits 187,640
Total surgeries 7,615
Total surgical procedures 9,669
(OR and outpatient)
Total laser procedures 1,564
35
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | o u r i n s t i t u t e
Cole Eye Institute OutcomesClinical outcomes allow us to understand and objectively measure the success of our surgical results.
Cole Eye Institute recently released its 2011 Outcomes book. This is the sixth year we have shared our
clinical outcomes with referring physicians, alumni and potential patients around the country.
A lmost all the surgical proce-
dures performed at Cole Eye
Institute have been tracked
and reported. Because Cole Eye
Institute is a regional, national and
international referral center, many of
our patients are followed by their local
ophthalmologists, and the data do not
include patients who are not followed
at Cole Eye Institute.
The scope of the Cole Eye Institute
outcomes project is significant, our ap-
proach is innovative and, in spite of the
complexity of cases and sometimes the
absence of a defined benchmark, our
outcomes are exceptional. Our physi-
cians strive to push the boundaries of
science and technology to provide excel-
lence for our patients. We hope that by
reviewing and analyzing information,
we will continue to improve and offer
patients superior clinical outcomes.
How We Measure Up
Our key evaluative measures continue to
be visual acuity and the rate of surgical
complications, and we continue to use
ETDRS protocol refraction as the means
of measuring visual acuity. The key mea-
surement variables are mentioned under
each section of the Outcomes book.
In addition to measuring clinical out-
comes, world-class customer service is
very important to us. Consequently, we
have spent significant time understand-
ing patient flow process and experience.
We continue to seek best-practice mea-
surement processes for both clinical
and administrative areas. We strive to
set the standard for excellence through
innovation and consistent follow-up
and measurement to evaluate our over-
all clinical proficiency.
The Outcomes book has data from
across the full spectrum of ophthalmic
surgery, including:
• Cataract surgery
• Cornea surgery
• Glaucoma surgery
• Oculoplastic surgery
• Oncologic eye procedures
• Refractive surgery
• Vitreoretinal surgery
• Strabismus surgery
Cleveland Clinic has created a series
of Outcomes books for all its institutes.
These contain a summary of our surgi-
cal and medical trends and approaches;
data on patient volume and outcomes;
and a review of new technologies and
innovations. ■
To view all our Outcomes books or to download a copy of Cole Eye Institute’s 2011 Outcomes book, visit Cleveland Clinic’s Quality & Patient Safety Insti-tute’s website at clevelandclinic.org/outcomes.

36
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Unique Programs at Cole Eye Institute
The Center for Genetic Eye Diseases
The Center for Genetic Eye Diseases
provides multidisciplinary clinical
diagnostic and therapeutic services for
patients with inherited eye conditions
such as corneal and retinal dystrophies
and microphthalmia. Patients with
inherited disorders that involve the eye,
such as neurofibromatosis, albinism,
neurodegenerative disorders and Mar-
fan syndrome, are referred to the center
by physicians from around the country.
A regular specialty clinic is dedicated
to patients with retinal dystrophies
and their families.
National Eye Donor Program
The Foundation Fighting Blindness
Center, a central collection agency for
eyes donated by individuals across the
United States for blindness research,
shares tissue samples with researchers
worldwide.
Formally known as the Retinal Degen-
eration Pathophysiology Facility, the
collection center accepts eye donations
after death from any person of any age
who had normal vision or any degree
of vision loss resulting from a retinal
degenerative disease.
Cole Eye Institute staff members pre-
pare a detailed medical report about
each donated eye to help researchers
track the effects of eye disease in differ-
ent types of people and environments.
For more information or to refer a patient, please call 216.444.2020 or 800.223.2273, ext. 42020, or visit clevelandclinic.org/OUspecial.
37
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | o u r i n s t i t u t e
Cole Eye Institute New Staff SpotlightFatema Ghasia, MDPediatric ophthalmology specialist Fatema Ghasia, MD, joined Cleveland Clinic
Cole Eye Institute this summer after completing a fellowship in Pediatric Ophthal-
mology and Strabismus at Duke University. She also completed an ophthalmology
residency and two fellowships at Washington University School of Medicine.
Her specialty interests are within pediatric ophthalmology. Her awards and
honors include the Rosenbaum Resident Research Award and several academic
achievement awards. Dr. Ghasia has published a significant body of work on
vision in children with cerebral palsy and other neurobehavioral disorders. She
also has been awarded a Knights Templar research grant and a Fight For Sight
grant to conduct oculomotor studies that involve eye movement recordings in
patients with strabismus and nystagmus and eye motility deficits in patients
with neurologic disorders.
Dr. Ghasia graduated from the Medical College at Maharaja Sayajirao University
of Baroda, India.
Dr. Ghasia practices at Cole Eye Institute’s main campus location. She can be reached at 216.444.0999 or [email protected].
Alex Yuan, MD, PhDRetina specialist and surgeon Alex Yuan, MD, PhD, joined Cleveland Clinic
Cole Eye Institute this summer after completing a fellowship in Vitreoretinal
Surgery at Cleveland Clinic. He also completed both a residency and a research
fellowship at the Jules Stein Eye Institute at UCLA.
His specialty interests are regenerative and stem cell therapy, cell-based
therapy, and gene and drug delivery. His awards and honors include the Cole
Eye Fellow Teaching Award, the Cole Eye Fellow Research Award, the Heed
Fellowship Award and the UCLA Excellence in Research Award, among others.
Dr. Yuan is widely published on topics related to retinal diseases and their
treatments, as well as research related to stem cell microvesicles.
Dr. Yuan graduated from Washington University School of Medicine with an MD
and PhD in neuroscience.
Dr. Yuan practices at Cole Eye Institute’s main campus location. He can be reached at 216.444.0079 or [email protected].
38
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Cole Eye Institute Leadership
Chairman, Cole Eye Institute
Daniel F. Martin, MD 216.444.0430
Institute Vice Chairman
Institute Quality Review Officer
Andrew P. Schachat, MD 216.444.7963
Institute Vice Chairman for Education
Elias I. Traboulsi, MD 216.444.2030
Comprehensive Ophthalmology
John Costin, MD 440.988.4040
Richard E. Gans, MD, FACS 216.444.0848
Philip N. Goldberg, MD 216.831.0120
Michael Gressel, MD 440.988.4040
Mohinder Gupta, MD 419.289.6466
Martin A. Markowitz, MD 440.461.4733
Shari Martyn, MD 216.831.0120
Peter McGannon, MD 216.529.5320
Michael E. Millstein, MD 216.831.0120
Wynne Morley, MD 440.366.9444
Sheldon M. Oberfeld, MD 440.461.4733
Allen S. Roth, MD 216.831.0120
David B. Sholiton, MD 216.831.0120
Scott A. Wagenberg, MD 440.461.4733
Cornea and External Disease
William J. Dupps Jr., MD, PhD 216.444.2020
Jeffrey M. Goshe, MD 216.444.0845
Roger H.S. Langston, MD 216.444.5898
Martin A. Markowitz, MD 440.461.4733
Peter McGannon, MD 440.529.5320
David M. Meisler, MD 216.444.8102
Wynne Morley, MD 440.366.9444
Sheldon M. Oberfeld, MD 440.461.4733
Allen S. Roth, MD 216.831.0120
Scott A. Wagenberg, MD 440.461.4733
Steven E. Wilson, MD 216.444.5887
Glaucoma
Jonathan A. Eisengart, MD 216.445.9429
Edward J. Rockwood, MD 216.444.1995
Shalini Sood-Mendiratta, MD 216.445.5277
Keratorefractive Surgery
William J. Dupps Jr., MD, PhD 216.444.2020
Ronald R. Krueger, MD, MSE 216.444.8158
Michael E. Millstein, MD 216.831.0120
Allen S. Roth, MD 216.831.0120
Steven E. Wilson, MD 216.444.5887
Cole Eye Institute Staff List

39
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | o u r i n s t i t u t e
Neuro-Ophthalmology
Gregory S. Kosmorsky, DO 216.444.2855
Lisa D. Lystad, MD 216.445.2530
Oculoplastics and Orbital Surgery
Mark Levine, MD 440.988.4040
Julian D. Perry, MD 216.444.3635
Ophthalmic Anesthesia
Marc A. Feldman, MD 216.444.9088
M. Inton-Santos, MD 216.445.1016
J. Victor Ryckman, MD 216.444.6330
Sara Spagnuolo, MD 216.444.6324
Ophthalmic Oncology
Arun D. Singh, MD 216.445.9479
Ophthalmic Research
Bela Anand-Apte, MBBS, PhD 216.445.9739
Vera Bonilha, PhD 216.445.7960
John W. Crabb, PhD 216.445.0425
William J. Dupps Jr., MD, PhD 216.444.2020
Stephanie Hagstrom, PhD 216.445.4133
Joe G. Hollyfield, PhD 216.445.3252
Neal S. Peachey, PhD 216.445.1942
Pediatric Ophthalmology and Adult Strabismus
Fatema Ghasia, MD 216.444.0999
Andreas Marcotty, MD 216.831.0120
Paul Rychwalski, MD 216.444.4821
Elias I. Traboulsi, MD 216.444.2030
Retina
Amy Babiuch, MD 440.366.9444
Ryan Deasy, MD 440.695.4010
Justis P. Ehlers, MD 216.636.0183
Peter K. Kaiser, MD 216.444.6702
Daniel F. Martin, MD 216.444.0430
Andrew P. Schachat, MD 216.444.7963
Jonathan E. Sears, MD 216.444.8157
Rishi P. Singh, MD 216.445.9497
Sunil K. Srivastava, MD 216.636.2286
Richard Wyszynski, MD 440.988.4040
Alex Yuan, MD 216.444.0079
Uveitis
Careen Y. Lowder, MD, PhD 216.444.3642
Sunil K. Srivastava, MD 216.636.2286

40
O p h t h a l m O l O g y U p d a t e | S p e c i a l e d i t i O n 2 0 1 2 | c l e v e l a n d c l i n i c . O r g / O U S p e c i a l
Cole Eye Institute Resources24/7 ReferralsReferring Physician Hotline
855.REFER.123 (855.733.3712)
Hospital Transfers
800.553.5056
On the Web at clevelandclinic.org/refer123
Stay connected with us on …
Twitter/YouTube/Facebook
About Cleveland ClinicCleveland Clinic is an integrated healthcare delivery system
with local, national and international reach. At Cleveland
Clinic, 2,800 physicians represent 120 medical specialties
and subspecialties. We are a main campus, 18 family health
centers, eight community hospitals, Cleveland Clinic Florida,
the Cleveland Clinic Lou Ruvo Center for Brain Health in Las
Vegas, Cleveland Clinic Canada, Sheikh Khalifa Medical City
and Cleveland Clinic Abu Dhabi.
In 2012, Cleveland Clinic was ranked one of America’s top 4
hospitals in U.S.News & World Report’s annual “America’s Best
Hospitals” survey. The survey ranks Cleveland Clinic among the
nation’s top 10 hospitals in 14 specialty areas, and as the top
hospital in three of those areas.
Resources for PhysiciansReferring Physician Center and Hotline
Cleveland Clinic’s Referring Physician Center has established a
24/7 hotline — 855.REFER.123 (855.733.3712) — to streamline
access to our array of medical services. Contact the Referring
Physician Hotline for information on our clinical specialties
and services, to schedule and confirm patient appointments,
for assistance in resolving service-related issues, and to connect
with Cleveland Clinic specialists.
Physician Directory
View all Cleveland Clinic staff online at clevelandclinic.org/staff.
Track Your Patient’s Care Online
DrConnect is a secure online service providing real-time
information about the treatment your patient receives
at Cleveland Clinic. Establish a DrConnect account at
clevelandclinic.org/drconnect.
Critical Care Transport Worldwide
Cleveland Clinic’s critical care transport teams and fleet
of vehicles are available to serve patients across the globe.
• To arrange for a critical care transfer, call 216.448.7000 or
866.547.1467 (see clevelandclinic.org/criticalcaretransport).
• For STEMI (ST elevated myocardial infarction), acute stroke,
ICH (intracerebral hemorrhage), SAH (subarachnoid hemor-
rhage) or aortic syndrome transfers, call 877.379.CODE (2633).
Outcomes Data
View clinical Outcomes books from all Cleveland Clinic
institutes at clevelandclinic.org/outcomes.
Clinical Trials
We offer thousands of clinical trials for qualifying patients.
Visit clevelandclinic.org/clinicaltrials.
CME Opportunities: Live and Online
The Cleveland Clinic Center for Continuing Education’s website
offers convenient, complimentary learning opportunities. Visit
ccfcme.org to learn more and use Cleveland Clinic’s myCME
portal (available from the site) to manage your CME credits.
Executive Education
Cleveland Clinic has two education programs for healthcare ex-
ecutive leaders — the Executive Visitors’ Program and the two-
week Samson Global Leadership Academy immersion program.
Visit clevelandclinic.org/executiveeducation.
Same-Day Appointments
Cleveland Clinic offers same-day appointments to help your
patients get the care they need, right away. Have your patients
call our same-day appointment line, 216.444.CARE (2273), or
800.223.CARE (2273).
41
C l e v e l a n d C l i n i C | C o l e e y e i n s t i t u t e | r e s e a r C h
Main Campus 9500 Euclid Ave./i20 Cleveland, Ohio 44195 216.444.2020
Ashland Lakeland Eye Surgeons 21 Sugarbush Court Ashland, Ohio 44805 419.289.6466
Avon Lakeland Eye Surgeons 33100 Cleveland Clinic Blvd. Avon, Ohio 44011 440.695.4010
Beachwood Cole Eye Institute, Beachwood 25101 Chagrin Blvd. Beachwood, Ohio 44122 216.831.0120
Elyria Lakeland Eye Surgeons 303 Chestnut Commons Drive Elyria, Ohio 44035 440.366.9444
Independence Cleveland Clinic Independence 5001 Rockside Road Crown Center II Independence, Ohio 44131 216.986.4000
Lakewood Lakeland Eye Surgeons Lakewood Hospital Professional Bldg. 14601 Detroit Ave. – Suite 550 Lakewood, Ohio 44107 216.529.5320
Lorain Lakeland Eye Surgeons 5700 Cooper Foster Park Road Lorain, Ohio 44053 440.988.4040
Mansfield Lakeland Eye Surgeons 1456 Park Avenue West – Suite P Ontario, Ohio 44906 419.529.5156
Mayfield heights Hillcrest Hospital Atrium Medical Building 6770 Mayfield Road - Suite 326 Mayfield Heights, Ohio 44124 440.461.4733
Strongsville Cleveland Clinic Strongsville 16761 SouthPark Center Strongsville, Ohio 44136 440.878.2500
Twinsburg Cleveland Clinic Twinsburg 8701 Darrow Road Twinsburg, Ohio 44087 330.888.4000
Please direct any correspondence to:
Medical Editor Rishi P. Singh, MD
Cole Eye Institute/i32 Cleveland Clinic 9500 Euclid Ave. Cleveland, OH 44195
Chairman, Cole Eye Institute Daniel F. Martin, MD
Vice Chairman and Quality Review Officer Andrew P. Schachat, MD
Director, Residency Training Program Vice Chairman for Education Elias I. Traboulsi, MD
Managing Editor Kimberley Sirk
Art Director/Designer Michael Viars
Marketing Manager Bill Sattin, PhD
Marketing Associate Mary Anne Connor
Principal Photography Russell Lee
Contributing Photography Cleveland Clinic Center for Medical Art and Photography
Top Related