






Languages
Pages
Legal

Oocyte
Cryopreservation
Prof. Aboubakr
ElnasharBenha University Hospital,
Egypt
ABOUBAKR ELNASHAR
CONTENTS
1. HISTORY
2. PRINCIPLE
3. TECHNIQUES
1. Slow freezing
2. Vitrification
4. OUTCOME
5. CLINICAL APPLICATIONS
Conclusion
ABOUBAKR ELNASHAR
INTRODUCTION
Embryo and sperm cryopreservation
well-established procedures
Oocyte cryopreservation
has become recently available
preferable in many situations
{challenges the ethical, legal and religious of
embryo cryopreservation}
ABOUBAKR ELNASHAR
1. HISTORY
First birth from a frozen oocyt
in Australia in 1986 (Chen, 1986)
The first live birth following vitrification
1999 (Kuleshova et al., 1999)
Now
1. Many advances have been made
2. Success rates:
application of oocyte cryopreservation for many
different indications
ABOUBAKR ELNASHAR
2 advances:
1. The introduction of vitrification
as an alternative to slow freezing: reduced
damage to internal structures: superior success
rates (Antinori et al., 2007; Cao et al., 2009; Fadini et al., 2009;Smith et al.,
2010).
2. Use of ICSI
resolve fertilization issues due to zona pellucida
hardening (Kazem et al., 1995; Porcu et al., 1997; Fabbri et al., 1998).
ABOUBAKR ELNASHAR
The Human Fertilisation and Embryology Authority
(HFEA)Allowed
use of frozen oocytes for infertility treatment in 2000(Wise, 2000).
storage of gametes for a standard 10-year period, which
can be extended under certain circumstances
(HFEA, 2015).
In 2013, ASRM lifted the experimental label applied to oocyte freezing,
following 4RCT
(Cobo et al., 2008, 2010a, Rienzi et al., 2010; Parmegiani et al., 2011)
IVF using vitrified/warmed oocytes could produce similar
fertilization and PR to IVF with fresh oocytes(ASRM, 2013).
ABOUBAKR ELNASHAR
2. PRINCIPLES
Oocytes are notoriously difficult cells to cryopreserve
1. Their low surface area to volume ratio:
high susceptibility to intracellular ice formation(Paynter et al., 1999).
2. The negative effects of cryopreservation on the
stability of microtubules and microfilaments(Pickering and Johnson, 1987; Sathananthan et al., 1988; Vincent et
al., 1989; Pickering et al., 1990; Joly et al., 1992)
which are vital for normal chromosomal segregation (Glenister et al.,1987).
3. Hardening of the zona pellucida: low fertilization
rates(Johnson et al., 1988; Vincent et al., 1990).
ABOUBAKR ELNASHAR
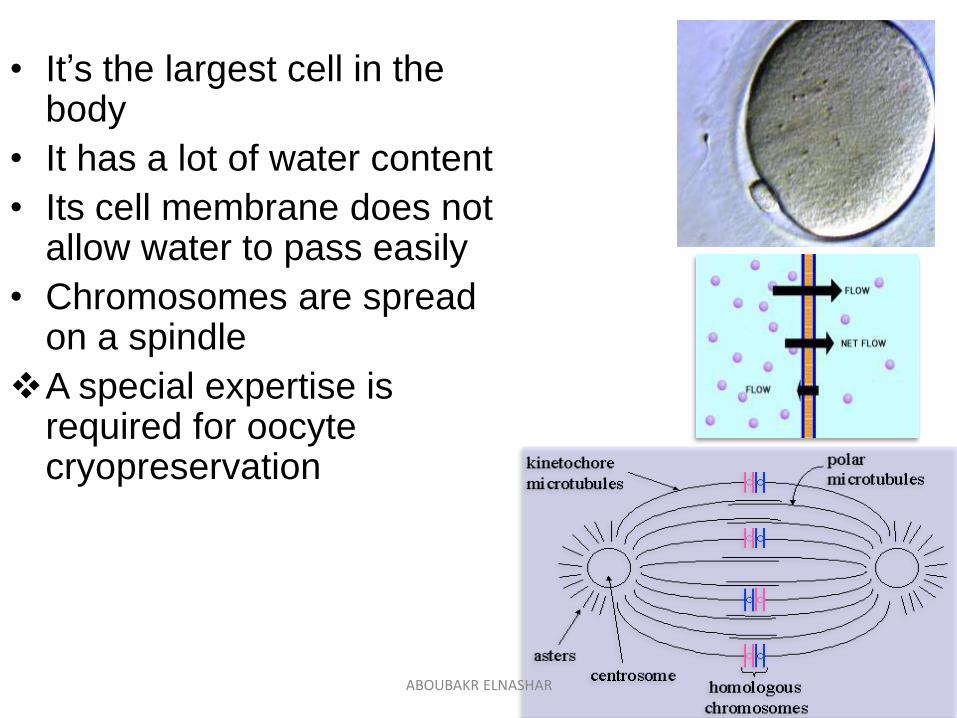
• It’s the largest cell in the body
• It has a lot of water content
• Its cell membrane does not allow water to pass easily
• Chromosomes are spread on a spindle
A special expertise is required for oocytecryopreservation
ABOUBAKR ELNASHAR
Cryopreservation
Preservation of cells and tissues for
extended periods of time
At sub-zero temperatures.
Cryoprotective additives (CPAs)
Reduce cryo damage by preventing ice formation.
Classified acc to their ability to cross the cell
membrane. Permeating:
dimethyl sulfoxide (DMSO), glycerol,1,2 propanediol (PrOH)
Non-permeating: sucrose, glucose, fructose, trehalose
ABOUBAKR ELNASHAR
3. TECHNIQUES
1. Slow freezing
Used in early protocols
Controlled slow freezing
Results in a liquid changing to a solid state
2. Vitrification
Now well established
Ultrarapid cooling
Results in a non-crystalline amorphous solid.
ABOUBAKR ELNASHAR
1. Slow freezing
Cells are exposed to
low concentration of CPAs and
slow decreases in temperature.
1. Oocytes are first cooled to temperature -5◦C to -7 ◦ C, at
which equilibration and seeding take place.
2. Oocytes are then cooled at a slow rate of 0.3–0.5 ◦
C/minute, until a temperature of between -30 ◦ C and -
65 ◦ C has been reached, before being added to liquid
nitrogen for storage (Saragusty and Arav, 2011).
Slow frozen vs fresh oocytes
Poorer outcomes(Levi Setti et al., 2006; Borini et al., 2010; Magli et al., 2010).
ABOUBAKR ELNASHAR
2. Vitrification
Requires
Higher concentrations of CPAs, lowering the risk of
ice nucleation and crystallization
Cooling rates of100s to10 000◦ C per minute before
submersion into liquid nitrogen (Saragusty and Arav, 2011).
Cryotop’ vitrification method
Developed in 2005
widely used method (Kuwayama et al., 2005).
ABOUBAKR ELNASHAR
Slow
cooling
- 0.3°C/min
Vitrifikation
- 50.000°C/min
1 sec.
Vitrification
ABOUBAKR ELNASHAR
Vitrification protocols:
1. Open
direct contact between oocytes and liquid
nitrogen
using low volume devices such as capillary glasses,
cooper devices,
pulled straws, and
loops (Glujovsky et al., 2014).
2. Closed
indirect contact between oocytes and liquid
nitrogen using tubing systems (Glujovsky et al., 2014).
ABOUBAKR ELNASHAR
Open:
similar success rates with fresh oocytes(Cobo et al., 2008, 2010; Rienzi et al., 2010; Parmegiani et al., 2011)
Concerns:
sterility {potential cross-contamination between the vitrification
sample and liquid nitrogen}.
bacteria were present in 45%
To overcome:
1. Liquid nitrogen sterilization using ultraviolet light
(Parmegiani et al., 2010) or
2. Oocyte storage in vapour phase liquid nitrogen,
which contains a lower density of environmental air
borne contaminants(Cobo et al., 2010).
ABOUBAKR ELNASHAR
Closed
offered a solution to contamination concerns(Vajta et al., 2015).
bacteria free(Criado et al.2011)
Concerns:
efficiency of oocyte vitrification
{decreased cooling rates}.
±not preserve the oocyte ultrastructure as well as in open
systems (Bonetti et al., 2011).
reduced fertilization, cleavage, and CPR(Paffoni et al., 2011).
Outcome: excellent (Smith et al., 2010; Stoopetal.,2012;Papatheodorouet al.,2013).
UK clinics:
75% used closed containers(Brison et al., 2012).
ABOUBAKR ELNASHAR
Warming rate
more important than the cooling rate for oocyte
survival (Seki and Mazur, 2009; Leibo and Pool, 2011; Mazur and Seki,2011).
Optimal outcomes if
vitrification and warming are carried out in the
same clinic or
by matched protocols (Brison et al., 2012).
ABOUBAKR ELNASHAR
Vitrification Vs slow freeze protocols.
better survival, fertilization, and PR
(18.2 vs 7.6%). (Oktay et al., 2006, Cao et al., 2009; Fadini et al., 2009; Smith et al., 2010)
ABOUBAKR ELNASHAR
Vitrified oocytes Vs fresh oocytes
similar outcomes(Nagy et al., 2009; Almodin et al., 2010; Ubaldi et al.,2010; Rienzi et al.,
2012).
Fertilization, embryo cleavage, high quality
embryos, CPR did not differ (Cobo and Diaz, SR 2011).
Oocyte survival rates of over 84%
CPR per transfer
between 35.5 and 65.2% (Cobo et al., 2008, 2010; Rienzi et al., 2010; Parmegiani et al.,
2011).
ABOUBAKR ELNASHAR
Many IVF programmes now
favour vitrification as a technique to cryopreserve
oocytes(Rudick et al., 2010; Brison et al., 2012; Glujovsky et al.,2014),
NICE guidelines states:
In cryopreservation of oocytes and embryos, use
vitrification instead of controlled-rate freezing if the
necessary equipment and expertise is available’ (NICE, 2013).
ABOUBAKR ELNASHAR
4. OUTCOMES
Birth weight and incidence of congenital abnormalities
2.5%
similar to those born from
spontaneous conceptions or
through regular IVF
(Chian et al., 2008, Noyes et al., 2009).
Cobo et al. (2014)
vitrification does not increase adverse obstetric and
perinatal outcomes.
No long-term follow-up of these children has yet
been published.
ABOUBAKR ELNASHAR
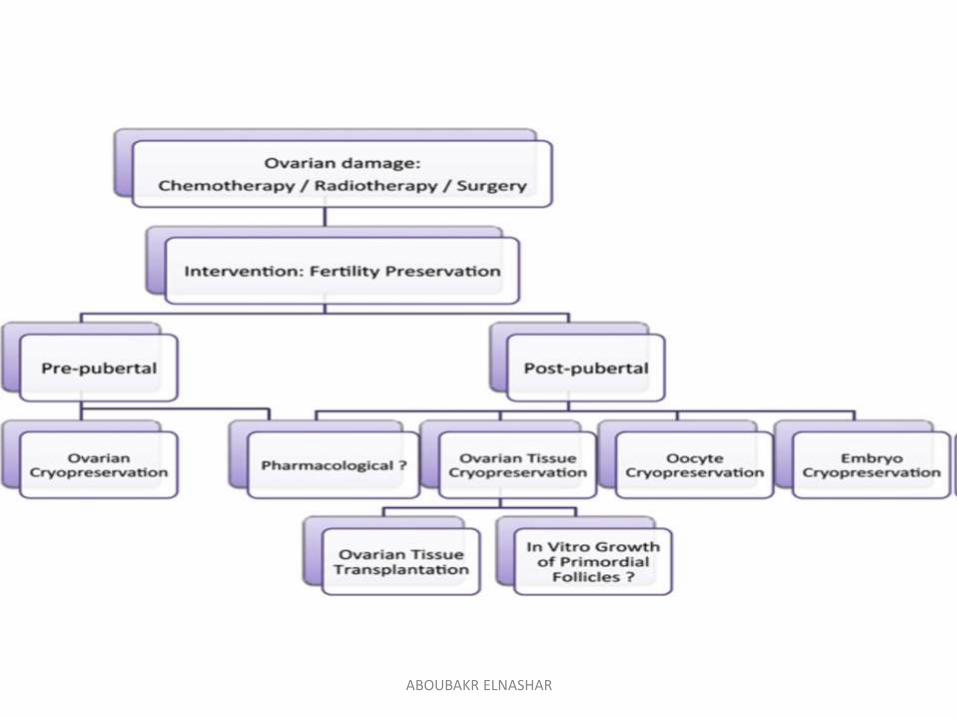
5. CLINICAL APPLICATIONS
1. Fertility preservation in cancer patients
2. Social egg freezing
3. Other indications
1. Medical indications
2. Donation programmes
3. Storage of ‘spare’ gametes during IVF.
ABOUBAKR ELNASHAR
1. Fertility preservation in cancer patientsCancer treatment regimes
can have a detrimental effect on female fertility
{removal of reproductive organs or
use of radiation therapy and cytotoxic agents}.
The extent of damage depends on
Follicular reserve
patient age
type and dose of treatment
with alkylating agents being particularly gonadotoxic(Knopman et al., 2010; Fleischer et al., 2011).
ABOUBAKR ELNASHAR
Around 10% of cancers
occur in women under the age of 45 (Donnez and Dolmans, 2013)
demand for fertility preservation amongst these
patients has increased with improving cancer survival
rates(Fleischer et al., 2011; Noyes et al., 2011).
ABOUBAKR ELNASHAR
ABOUBAKR ELNASHAR
Embryo cryopreservation
has been an option for some time (ASRM, 2005; Lobo, 2005; Lee et al., 2006; Kim, 2006)
Disadvantages
Risk of dispute if couples separate.
Not appropriate for
single women or
young patients without a stable partner (Noyes et al., 2011).
ABOUBAKR ELNASHAR
Oocyte Vs embryo cryopreservation
Embryo cryopreservation
an established ART technique
Advantages.
The ability to store surplus embryos:
reduce the number of embryos transferred
during a fresh cycle:
minimize the risk of multiple pregnancy
reduce the need for repeated stimulation
cycles,
increase cumulative pregnancy rates.
ABOUBAKR ELNASHAR
Disadvantages:
Not an option for all couples
personal religious or
moral objections, or
restrictive legislation in certain countries.
Decisions over the fate of stored embryos: major
disagreements or legal disputes, particularly in the
case of divorce or separation(Pennings,2000; Lee et al., 2006).
ABOUBAKR ELNASHAR
Oocyte cryopreservation
a feasible alternative to embryo cryopreservation for
many couples undergoing IVF(ASRM, 2013).
1. less moral sensitivity surrounding the
storage and fate of gametes
2. fewer issues surrounding ownership
{genetic material originates from one individual}
ABOUBAKR ELNASHAR
Oocyte cryopreservation
can now be offered routinely for fertility preservation.
71.6% of cancer patients enquiring about fertility
preservation underwent oocyte cryopreservation
(Garcia- Velasco et al., 2013).
ABOUBAKR ELNASHAR
The disadvantage of cryopreserving mature,
metaphase II (MII), oocytes in cancer patients:
Need for ovarian stimulation.
This can delay cancer treatment by several
weeks, and may carry particular risk for those
patients with a hormone receptive cancer (Kim et al., 2011).
These problems can be reduced by
1. anytime start’ protocols
(Cakmak et al., 2013)
2. use of antiestrogens during stimulation for
women with breast cancer (Reddy and Oktay, 2012).
ABOUBAKR ELNASHAR
Alternatives include
1. Cryopreservation of oocytes at the germinal
vesicle(GV) stage (Toth et al., 1994) or
2. Retrieval of immature oocytes followed by in-vitro
maturation (IVM)
(Rao et al., 2004; Huang et al., 2008; Oktay et al., 2010)
neither of which require ovarian stimulation.
ABOUBAKR ELNASHAR
3. Ovarian tissue banking.
does not delay cancer treatment
An ovarian cortical biopsy or oophorectomy is
performed as a day-case surgical procedure,
independent of the menstrual cycle.
Disadvantages
1. Patient must be fit for surgery
2. Tissue must subsequently be regrafted, with
potential risk of reintroducing malignant cells (Hoekman et al., 2015).
3. Few births have been reported after
regrafting frozen ovarian tissue (Donnez and Dolmans, 2015).
ABOUBAKR ELNASHAR
Fertility preservation cycles and chemotherapy in
breast cancer patients
could be started earlier before breast surgery
9 of 35 patients referred before surgery were able to
undergo two fertility preservation cycles, compared to
only 1 of 58 patients referred after surgery. (Lee et al., 2010)
ABOUBAKR ELNASHAR
2. Elective oocyte cryopreservationSocial egg freezing
Oocyte cryopreservation for age-related fertility decline
In almost all countries, an increasing number of
women are postponing motherhood: rising numbers
experiencing childlessness which they had not
necessarily intended (Kneale and Joshi, 2008).
considered acceptable (ESHRE Task Force on Ethics andLaw, 2012)
a popular subject within the media
increased rapidly (Garcia-Velasco et al., 2013).
ABOUBAKR ELNASHAR
ABOUBAKR ELNASHAR
Advantages:
1. The use of younger oocytes can reduce the risk of
fetal loss and aneuploidies associated with ageing
oocytes(Goold and Savulescu, 2009).
2. The use of cryopreserved, autologous oocytes also
allows the mother to have a genetic relation to her
child that could not be achieved through oocyte
donation(Dondorp and DeWert, 2009; Goold and Savulescu, 2009)
3. Higher chance of pregnancy than the use of
standard IVF at an older age (Sauer et al., 1990).
PR: age-dependent
optimal number of stored MII oocytes: at least 8–10 (Cobo et al., 2015).
ABOUBAKR ELNASHAR
Age associted infertility=Age-related fertility decline
The fertility decline experienced by women, which
accelerates after the age of 35, is a well-known
phenomenon (Dunson et al., 2004; Sozou and Hartshorne, 2012).
Causes
1. Decrease in follicular quality
2. Decrease in follicular number
(Faddy et al., 1992).
3. Significantly higher risk of fetal chromosomal
abnormalities and fetal loss (Hook, 1981; Nybo Anderson et al., 2000).
ABOUBAKR ELNASHAR

Social and ethical implications
Reasons for which women may wish to delay
motherhood
to focus on their career
to find a suitable partner or
because they simply do not feel ‘ready’ (Goold and Savulescu, 2009).
There is an obvious gender inequality in
reproduction, since men are able to reproduce at
much older ages than women (Dondorp and De Wert, 2009).
ABOUBAKR ELNASHAR
Oocyte cryopreservation
a ‘breakthrough for reproductive autonomy’ (Harwood, 2009)
an ‘emancipation’ for women (Homburg et al., 2009).
give women the ability to make more reproductive
choices
to decide when and with whom they wish to have
children.
ABOUBAKR ELNASHAR
Concerns in response to oocyte cryopreservation.
1. Risks in
ovarian stimulation
oocyte retrieval(Goold and Savulescu, 2009; Bayliss, 2015).
2. When older women come back to use oocytes:
more likely to experience pregnancy complications:
pre-eclampsia, hypertension and gestational diabetes
CS(Ziadeh and Yahaya, 2001; Joseph et al., 2005).
These risks are the same as those in older women
using conventional IVF (Goold and Savulescu, 2009).
ABOUBAKR ELNASHAR
3. Oocyte cryopreservation encourages women to
become unworried about their declining fertility (Goold and Savulescu, 2009).
women should receive the correct information
about oocyte cryopreservation
success rates
do not accept it as an ‘insurance policy’ as it is
often portrayed (Lockwood, 2011).
ABOUBAKR ELNASHAR
4. Companies such as Apple and Facebook offer
‘social egg freezing’ to their employees: women
feeling pressured to delay childbirth undermining the
concept of reproductive autonomy.(Bayliss, 2015)
5. There are concerns that women will delay
motherhood until their late 50s or 60s.(Dondorp and De Wert, 2009)
ABOUBAKR ELNASHAR
6. The high cost of oocyte cryopreservation.
if women were to cryopreserve their oocytes at the
age of 25 and return to them at 40, this would be a
less cost-effective strategy than simply undertaking
ART at the age of 40 if difficulties were found trying to
conceive naturally.(Hirshfeld-Cytron et al.2012)
ABOUBAKR ELNASHAR
oocyte cryopreservation before the age of 38
reduces the cost of achieving a live birth aged 40 and
beyond(Devine et al., 2015).
oocyte cryopreservation was a more cost-effective
strategy than IVF (Van Loendersloot et al.,2011).
Women should be encouraged to have
children early,
rather than to invest in an expensive technique with
no guarantee of pregnancy.
ABOUBAKR ELNASHAR
Attitudes surrounding ‘social’ oocyte cryopreservation
Although it is still unclear exactly how many women
will access elective oocyte cryopreservation (Stoop et al., 2014)
77.6% had been previously aware of the technique
and 31.5% of women would potentially cryopreserve
their oocytes(Stoop et al., 2011).
Medical students in Singapore
36.4% of respondents had heard of the technique
26.4% would consider it (Tan et al., 2014).
ABOUBAKR ELNASHAR
In USA
The main reason stated for delaying childbirth (88%)
was the lack of a partner
84%: were over the age of 35. This is significant,
since age at time of oocyte cryopreservation is an
important determinant of outcome. (Hodes-Wertz et al., 2013).
Age: means of 36.7 and 36.9 years (Baldwin et al., 2015; Stoop et al., 2015).
Why?
65% as an ‘insurance’ against future infertility
49% wanted more time to find a partner (Stoop et al., 2015).
ABOUBAKR ELNASHAR
Follow-up of ‘social-freezers’
Hodes-Wertz et al. (2013)only 6% of women (11 respondents) had used their
oocytes during the 6-year timeframe.
Of these,
3 patients reported having subsequently achieved a
pregnancy from a thaw cycle
5 were unsuccessful
3 failed to comment.
Stoop et al. (2015)50.8% of women who cryopreserved their oocytes
anticipated using them at some point.
Baldwin et al., 2015.23 women who had cryopreserved their oocytes
2 had returned to use them with one successful pregnancy
ABOUBAKR ELNASHAR
3. Other indications
1. Medical conditions other than cancer
(Donnez and Dolmans, 2013)
1. Endometriosis who may experience reduced
ovarian reserve post surgery (Elizur et al., 2009)
2. Autoimmune diseases requiring gonadotoxic
treatment
(Elizur et al., 2008)
3. Fertility preservation in gender reassignment
surgery.
ABOUBAKR ELNASHAR
2. Oocyte donation
Reproductive potential can be extended by the use
of donated oocytes from younger women (Sauer et al., 1990; Navot et al., 1991)
similar success rates to their younger counterparts(Sauer et al., 1990).
offspring from oocyte donation are not genetically
related, and the process can be psychologically,
emotionally, and financially challenging.
ABOUBAKR ELNASHAR
3. Women at risk of early menopause
Genetic aberrations leading to subfertility or risk of
early menopause (Goswami and Conway, 2005).
Assessment of ovarian reserve using AFC and
AMH, FSH.
Although ovarian reserve measurement has not
been shown to have predictive value for spontaneous
pregnancy, it is a reasonable strategy for these
women to consider elective oocyte cryopreservation.
ABOUBAKR ELNASHAR
4. low-responders
allowing the storage and accumulation of oocytes
from multiple ovarian stimulation cycles before IVF
and embryo transfer (Cobo et al., 2012).
ABOUBAKR ELNASHAR
5. Emergency’oocyte cryopreservation
male partner fails to produce a sperm sample on the
day of oocyte retrieval for IVF (Emery et al., 2004).
sperm extraction from male partners with non-
obstructive azoospermia had failed (Song et al., 2011).
ABOUBAKR ELNASHAR
CONCLUSION
Oocyte cryopreservation
an established technology with a wide range of
indications.
an exciting technique that will prove beneficial to
many patients in the future.
Future research.
the long-term follow-up of children born following
oocyte vitrification.
ethical questions that need to be considered,
particularly in the case of ‘social egg freezing’.
ABOUBAKR ELNASHAR
Top Related