







Languages
Pages
Legal


Oncology Changing Market Dynamics February, 2010

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 2
Oncology – a new market dynamic on the horizon
Historically, oncology has been an area of significant sales growth due to favorable factors, such as a cooperative FDA, premium pricing, and prevalent off-label usage
However, we see signs of change…
New drugs and indications are crowding the market Payors are having a greater impact on drug utilization
“Traditional” tools such as tiered co-payments, prior authorization and step-edits are being used more aggressively throughout the industry
The industry is responding as well with price caps and pay for performance arrangements
Overall, we believe industry participants need to pay close attention to these signals, and position themselves for a new market dynamic

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 3
Table of Contents
Historical Market Dynamics
Evidence of Changes
Case Studies
How to Prepare
| Copyright © 2010 Grail Research, a division of Integreon February, 2010 4
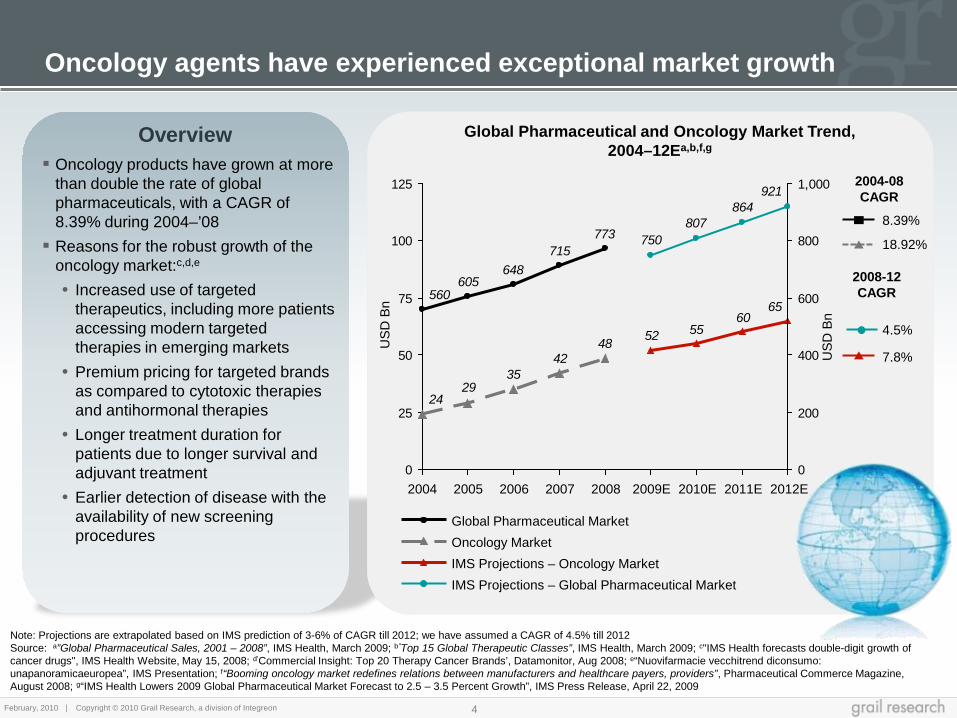
Oncology products have grown at more
than double the rate of global pharmaceuticals, with a CAGR of 8.39% during 2004–’08 Reasons for the robust growth of the
oncology market:c,d,e • Increased use of targeted
therapeutics, including more patients accessing modern targeted therapies in emerging markets
• Premium pricing for targeted brands as compared to cytotoxic therapies and antihormonal therapies
• Longer treatment duration for patients due to longer survival and adjuvant treatment
• Earlier detection of disease with the availability of new screening procedures
Overview
Oncology agents have experienced exceptional market growth
Note: Projections are extrapolated based on IMS prediction of 3-6% of CAGR till 2012; we have assumed a CAGR of 4.5% till 2012 Source: a”Global Pharmaceutical Sales, 2001 – 2008”, IMS Health, March 2009; b”Top 15 Global Therapeutic Classes”, IMS Health, March 2009; c"IMS Health forecasts double-digit growth of cancer drugs", IMS Health Website, May 15, 2008; d’Commercial Insight: Top 20 Therapy Cancer Brands’, Datamonitor, Aug 2008; e“Nuovifarmacie vecchitrend diconsumo: unapanoramicaeuropea”, IMS Presentation; f“Booming oncology market redefines relations between manufacturers and healthcare payers, providers”, Pharmaceutical Commerce Magazine, August 2008; g“IMS Health Lowers 2009 Global Pharmaceutical Market Forecast to 2.5 – 3.5 Percent Growth”, IMS Press Release, April 22, 2009
USD
Bn
Global Pharmaceutical and Oncology Market Trend, 2004–12Ea,b,f,g
4842
3529
24
6560
5552
773715
648605
560
921864
807750
0
25
50
75
100
125
0
200
400
600
800
1,000
2012E 2011E 2010E 2008 2007 2009E 2004 2005 2006
IMS Projections – Global Pharmaceutical Market IMS Projections – Oncology Market Oncology Market Global Pharmaceutical Market
2004-08 CAGR
USD
Bn
2008-12 CAGR
8.39%
18.92%
4.5%
7.8%

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 5
Table of Contents
Historical Market Dynamics
Evidence of Changes
Case Studies
How to Prepare

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 6
New drugs and new indications are crowding the market
Payors are more aggressive in managing Biologics
1
New Pricing Pressures
2
3
Recent events raise the possibility that this market dynamic is changing
Shift to orals enables traditional utilization controls
4

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 7
Flavopiridol (Sanofi Aventis)
Zibotentan (AstraZeneca)
Neuradiab (Bradmer Pharma)
AVE 8062 (Sanofi Aventis)
BIBW-2992 (Boehringer Ingelheim)
Vadimezan (Novartis and
Antisoma)
Telcyta (Telik)
Lestaurtinib (Cephalon)
Alpharadin (Algeta)
Ramucirumab (Eli Lilly)
Afutuzumab (Biogen Idec)
XL-184 (BMS and Exelixis)
BSI-201 (BiPar Sciences)
Figitumumab (Pfizer)
Midostaurin (Novartis)
Farletuzumab (Baxter)
Axitinib (Pfizer)
Motesanib (Amgen)
Brivanib Alaninate
(BMS)
LATE STAGE PIPELINE 1998 2001 2002 2003 2004 2005 2006 2007
Tasigna (Novartis)
Tykerb (GSK)
Torisel (Wyeth)
Gleevec (Novartis)
Erbitux (BMS)
Velcade (J&J /
Mellinium)
Revlimid (Celgene Corp.)
Nexavar (Bayer & Onyx)
Campath (Bayer /
Genzyme)
2000 1997
Bexxar (GSK)
Herceptin (Genentech)
Recentin (Astra-Zeneca)
Rencarex (J & J)
Zactima (AstraZeneca)
Herceptin- DM1
(ImmunoGen)
Aflibercept (Sanofi Aventis)
Galiximab (Biogen Idec)
Lumiliximab (Biogen Idec)
Deforolimus (Ariad)
Omnitarg (Roche)
Anyara (Active biotech)
Enzastaurin (Eli Lilly)
Zybrestat (OXiGENE)
Zarnestra (J & J)
Vargatef (Boehringer Ingelheim)
Neratinib (Wyeth)
Bosutinib (Wyeth)
Zalutumumab (Genmab)
Masatinib Mesylate
(AB Science)
Genasense (Genta)
Ofatumumab (Genmab &
GSK)
Pazopanib (GSK)
Avastin (Genentech)
Tarceva (OSI /
Genentech)
Sutent (Pfizer)
Vectibix (Amgen)
Sprycel (BMS)
Iressa (AstraZeneca)
Rituxan (Genentech)
Zevalin (Spectrum)
Mylotarg (Wyeth)
Note: Late Stage Pipeline includes only those drugs which are either in Phase III or pre-registration stage of development Source: Grail Research; PharmaProjects database (accessed in August 2009)
The pipeline for new targeted therapies is significant 1

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 8
Many compounds focus on the same biology
Competitive intensity is increasing as companies target similar mechanisms
Current Level of Competition Expected
Long Term Competition2
EGFR Antagonist
VEGFR Antagonist
Tyrosine Kinase Inhibitors
8
12
9
Expected Near Term
Competition1
2
2
9
Note : The dates mentioned in the chart are approval dates and not the launch dates; 1Represents the number of molecules in phase III / Pre-registration / Registration stage of development for relevant indications; 2Represents the number of molecules in phase I / II of development; Above mentioned data represent the primary pharmacology action for the marketed and pipeline molecules (a molecule can target more than one receptors; however, we have only considered the primary target in this analysis) Sources: FDA website, Company website ; PharmaProjects database; Grail Analysis
Epidermal growth factor receptor 2 antagonist
1

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 9
Adding indications to existing drugs increases competition
5
5
1
2
2
1
2
2
1
1
1
1
10
2
3
5
3
3
2
2
3
1
1
0 2 4 6 8 10 12 14 16 18
Vectibix
Herceptin 3 1
3
13
Avastin 17 2
Gleevec 18 13
6 3
Tarceva 9 4
Tykerb 11 7
Sutent 15 8
Erbitux 15 10
Revlimid 16
Rituxan 2
4
7
Torisel
Nexavar
Early Stage Pipeline Indications Late Stage Pipeline Indications Approved Indications
Expansion of existing agents
Note: Late Stage pipeline include molecules in registration / pre-registration / phase III of development, Early Stage pipeline include molecules in phase I or II of development Source: PharmaProjects; Clinical Trials Website; Company Websites; “Top 20 Cancer Brands”, Datamonitor
1

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 10
Many indications will soon have multiple targeted therapies
Lymphoma
Colorectal Cancer
Leukemia
NSCLC
Kidney Cancer
Breast Cancer
2004 1997 1998 2000 2001 2003 2005 2002 2007 2006 2008 2009 LATE STAGE PIPELINE
Note: Late Stage Pipeline includes only those drugs which are either in Phase III or pre-registration stage of development Source: Grail Research; PharmaProjects database (accessed in August 2009)
Rituxan (CD20
antagonist)
Zevalin (DNA
antagonist)
Bexxar (DNA
antagonist)
Velcade (Proteasome inhibitor)
Revlimid; Torisel; Campath; Afutuzumab; Galiximab; Ofatumumab; Enzastaurin
Herceptin (EGFR
Antagonist)
Tykerb (TKI)
Avastin (VRGF
Antagonist)
Sutent; Ramucirumab; BSI-201; Pazopanib; Herceptin- DM1; Omnitarg; Neratinib; BIBW-
2992
Mylotarg (DNA
antagonist)
Gleevec (Bcr-Abl inhibitor); Campath
(Lymphocyte inhibitor)
Sprycel (Bcr-Abl inhibitor)
Tasigna (Bcr-Abl inhibitor)
Revlimid; Rituxan; Alvocidib; Midostaurin; Lestaurtinib; Lumiliximab; Genasense;
Ofatumumab; Zarnestra; Bosutinib
Iressa (TKI)
Tarceva (TKI)
Avastin (VRGF
Antagonist)
Erbitux; Sutent; Nexavar; Aflibercept; Vadimezan; Telcyta; Figitumumab; Motesanib;
Pazopanib; Recentin; BIBW-2992; Enzastaurin; Zactima; Vargatef
Avastin (VRGF
Antagonist); Erbitux (EGFR
Antagonist)
Vectibix (EGFR
Antagonist)
Tarceva; Sutent; Aflibercept; Brivanib Alaninate; Recentin
Nexavar (B-raf kinase
inhibitor)
Sutent (VEGFR Inhibitor)
Torisel (mTOR kinase
inhibitor)
Avastin (VRGF
Antagonist) Axitinib; Pazopanib; Anyara; Rencarex
1

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 11
More aggressive use of utilization tools is underway
Note: 1PBM is Pharmacy benefit management; 2Survey group include Commercial health plans (N=55), Medicare Advantage plans (N=23), Managed Medicaid plans (N=17), PBMs (N=11) Source: aBiotechnology Monitor and Survey, Marketplace Policies, Practices and Perspective: 2009
Management strategy
Commercial health plans
Medicare advantage plans
Managed Medicaid plans PBMs1
% of plans using the
tool in 2008
Incremental % of plans to use the
tool in 2011
% of plans using the
tool in 2008
Incremental % of plans to use the
tool in 2011
% of plans using the
tool in 2008
Incremental % of plans to use the
tool in 2011
% of plans using the
tool in 2008
Incremental % of plans to use the
tool in 2011
Quantity Limits 36.4% 14.5% 43.5% 17.4% 29.4% 23.5% 36.4% 27.3%
Step Therapy 14.5% 23.6% 13.0% 30.4% 17.6% 23.5% 0.0% 36.4%
Prior Authorization by Diagnosis 56.4% 7.3% 60.9% 13.0% 52.9% 17.6% 36.4% 9.1%
Prior authorization by test results 34.5% 21.8% 21.7% 30.4% 41.2% 11.8% 0.0% 36.4%
Coinsurance cost share 29.1% 12.7% 56.5% 13.0% NA NA 18.2% 0.0%
Biologics in Breast Cancer – Usage of utilization tools in 2008 and expected increment in 2011a,2
2

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 12
Oncology Drugs Market Share by Launch, 1996–2007a Average Monthly Medicare Price of Drugs at the Time of Approval (1994-2008)b
The cost of cancer therapy is increasing as patients shift to newer, more expensive therapies
Drugs Lanched in 1997 or Before Drugs Launched in 1998-02 Drugs Launched in 2003-07
32354149576473828893100 37383837
35362718127 8
1999 2001 1998 2003 2002 2000 1997
50
100 14
0%
31
2006
27
2005
21
2004 2007
Source: a”The Oncology Pipeline: Maturing, Competitive, and Growing?’, Oncology Business Review, Sep 2008; b“Limits on Medicare's Ability to Control Rising Spending on Cancer Drugs”, NEJM Article, February 5, 2009; cManaged Care Oncology Magazine, Q3 2008 Issue
New drugs cost more and are increasing share
6,465
3,610
1,450
0
2,000
4,000
6,000
8,000
2004-2008 1999-2003 1994-1998
Utilization of Newer therapies is increasing New Therapies cost more
Per
cent
Mar
ket S
hare
Year of Approval
US
D
The Cost of Treating Cancer is Increasingc
7562
4330
0
50
100
2005 2000 1995 1990
Annual Cost of Treating Cancer (USD Bn)
3

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 13
At the same time, drug benefits may seem modest relative to cost
Some of the newly-approved brands cost USD 150-500K per life year gained
Drug Company Indication Year of Approval
Incremental Benefit
Incremental Cost of Therapy (USD)
Cost / Life Year Gained
(LYG) (USD)1
Avastina Roche Breast Cancer 2008 4 months survival 50,000 150,000
Tykerbb GSK Breast Cancer 2007 0.127 months survival 21,484 169,165
Ixemprac BMS Breast Cancer 2007 1.96 months survival 30,900 189,184
Avastinb Roche Non-small Cell Lung Cancer 2006 2.3 months survival 66,270–80,343 345,757–
419,181
Tarcevab OSI Pharmaceuticals / Roche
Pancreatic Cancer 2005 0.4 months survival 12,156–16,613 364,680–
498,390
Erbituxb BMS Colorectal Cancer 2004 1.44 months
survival 21,954 182,950
Notes: 1LYG costs have been derived Source: aNew York times; bAmerican Society of Clinical Oncology (ASCO); cJournal of Clinical Oncology
3

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 14
This has led to a new and public discussion about the cost/benefit of these new therapies
Sources : a“Costly Cancer Drug Offers Hope, but Also a Dilemma”, The New York Times, July 6, 2008; b “Lilly Erbitux Cancer Drug Not Worth Price, U.S. Scientists Say”, Bloomberg News, June 2009; c“Ixabepilone in Metastatic Breast Cancer: Small Benefit at High Cost”, Medscape, May 2009; d“NHS denies 'effective' cancer drugs due to cost”, The Independent, August 2008; e“U.K. Says Tykerb Isn’t Worth Cost, Even With 12 Free Weeks”, The Wall Street Journal, March 2009
Commentary in the press
New York Times, July 2008 - Cost effectiveness of Avastin - “It’s absolutely critical that we start having a public discussion,” said Barbara Brenner, executive director of Breast Cancer Action, an advocacy group. “I think of Avastin as a model that is showing us where the problem is.”a
Bloomberg News, June 2009 - “Eli Lilly & Co.’s tumor-fighter Erbitux doesn’t prolong lung cancer patients’ lives enough to justify its $80,000 cost, U.S. scientists said in commentary published today. Erbitux added to other cancer drugs extends survival about 1.2 months more than chemotherapy alone, making the price too high for a ‘marginal benefit,’ commentary in the Journal of the National Cancer Institute said”b
Medscape, May 2009 - “Ixabepilone (Ixempra) for metastatic breast cancer is an example of a cancer drug that adds ‘a small benefit at a high cost,’ says an editorial in the May 1 edition of the Journal of Clinical Oncology. The editorial accompanies a new cost-efficacy study in the same issue of the journal that found that the addition of ixabepilone to capecitabine (Xeloda) adds about $31,000 to the overall medical costs of metastatic breast cancer while providing about 1 more month of ‘quality-adjusted’ survival”c
The Independent, August 2008 - “The National Institute for Health and Clinical Excellence (NICE) issued draft guidance rejecting the drugs Sutent (sunitinib), Avastin (bevacizumab), Nexavar (sorafenib) and Torisel (temsirolimus)” “The guidance rejects the drugs because they are not cost effective”d
The Wall Street Journal, March 2009 - “Expert advisers in the U.K. are sticking with their view that GlaxoSmithKline’s Tykerb is too costly to justify routine use in women with advanced breast cancer. The British government’s National Institute for Health Effectiveness, or NICE, put out a final appraisal that said Tykerb hadn’t ‘demonstrated that it was cost effective’ in comparison with other treatments. It put forth a similar view last summer”e
3

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 15
Price Caps
Employed as a Tool
In Oct. 2006, Genentech
announced a price cap on
Avastin based on a patient’s
incomea
In Sept. 2006, Amgen
instituted a price cap on Vectibix at
$4,000 per dose (20% lower than BMS’s Erbitux)d
In May 2006, BMS
announced a price cap on Erbitux for
patients that reach a monthly
threshold
The UK government (NICE) uses cost/benefit analysis in evaluating
drugsc
Genentech capped Avastin at USD 55,000/year for patients with a household income less than $75,000 a yeard
If patients spend more than 5% of their annual gross income on copayments, then they become
eligible for free drugs through an assistance programb
Patients who spend over USD 10,000/month become eligible for free or discounted drugs through a charitable programa
A threshold of GBP 30,000 per quality-adjusted life year
(QALY) is used in evaluating drugs for reimbursementc
Examples of price cap initiatives
Companies are reacting with price caps…
Sources : a”Contracting, rebating, risk-sharing – IMS Conference hears about more innovative approaches to pricing”, IMS Global Insights; b“Managed Care Best Practices in Oncology Management”, Conference report, November 2006; c“Cost-Effectiveness of Cancer Drugs Is Questioned”, The Wall Street Journal, June 2009 and “Time to Consider Cost in Evaluating Cancer Drugs in United States?”, Medscape Today, July 2009 ; d“Top Of The Cancer Market?”, Forbes, October 2006
3

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 16
… and pay for performance arrangements
Note: 1Pay for Performance is more popular in Europe.US, insurers have less leverage with drug makers because of tough state regulations and marketplace pressures Source: ; a“Money-Back Guarantee”, Pharmaceutical Executive, April 2008; b“Drug Deals Tie Prices to How Well Patients Do”, New York times, April 2009; c“Pricing Pills by the Results”, New York times, July 2007;d “More Velcade-Style Risk-Sharing In The UK?”, Europharmatoday.com, January 2009;
3
In 2001 Pfizer convinced the State of Florida to put all its drugs on the state's Medicaid formulary. In return Pfizer agreed to rebate a portion of drug costs if its drugs failed to generate long-term cost savings across the healthcare systema
• This model worked for Pfizer, enabling the company to avoid up-front discounts and back-end rebates, while saving the State of Florida USD 41.9MM in other healthcare costsa
In 2007, after the NHS in Britain decided not to pay for the cancer drug Velcade, Johnson & Johnson offered a money-back guarantee if Velcade failed to reduce tumors by at least 25%b,c
• Through this Pay for Performance strategy, the NHS designated Velcade as cost-effective for up to four cycles of treatmentc
In 2007, United Healthcare entered into a risk sharing agreement with Genomic Health. The company sells Oncotype DX®, a USD 3,460 genetic test that determines whether an early-stage breast cancer patient would benefit from chemotherapyc
• United Healthcare agreed to pay for the test for 18 months, on grounds that it would seek a price negotiation if the test failed to have the intended medical impactc
In 2009, in response to a negative UK NICE appraisal, Merck offered to refund the primary care cost of its drug Erbitux, if a patient did not respond within 6 weeksd
In 2009, when Tarceva was declared cost ineffective by NICE, Roche offered a rebate for the cost difference between Tarceva and the incumbent NSCLC treatmentd
Pay for Performance Examples
Drug companies are increasingly offering discounts to insurers based on drug performance rather than quantity of drug utilized1

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 17
Companies are also conducting head-to-head trials in order to demonstrate superiority for their agent over alternatives
The crowded market is resulting in increased pressure on drug companies to conduct head-to-head trials to prove that their product is better than the competitor’s product
Note: 1Trial halted in June 2009 as better survival rates could not be established; 2FDA approved Sprycel for treatment of CML since the study established better survival rates in Gleevec-resistant patients. The drug fulfills the need for second line treatment Source: aClinicaltrial.gov, b“Pfizer halts Sutent breast-cancer trial”, fiercepharma.com, June 2009; c“FDA Grants Full Approval For SPRYCEL For The Treatment Of Adults With Chronic Myeloid Leukemia”, MedicalNewsToday, May 2009
Comparison Condition
Second line NSCL Cancer
First line metastatic Colorectal Cancer
First line metastatic Breast Cancer
First line CML
Adjuvant Breast Cancer
Zactima vs Tarcevaa
Recentin vs Avastina
Sutent vs. Avastin1,b
Sprycel vs Gleevec2,c
Tykerb vs Herceptina
Trial Sponsor Expected Completion Date
Results were expected in September 2009;
Regulatory submissions withdrawn
May 2011
Halted in June 2009
Complete
May 2013
Astrazeneca
Astrazeneca
Pfizer
Bristol-Myers Squibb
GlaxoSmithKline
3

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 18
Share of Biologics Within Top 100 Products
Greater use of oral therapeutics is changing oncology
Source: aWorld Preview 2014, May 2009, Evaluate Pharma report; bMonthly oncology report, October 22, 2007, Rodman and Renshaw equity research
2322212019181716141312111099
777879808182838486878889909191
0
20
40
60
80
100
2014E 2013E 2012E 2011E 2010E 2009E 2008 2007 2006 2005 2004 2003 2002 2001 2000
Conventional Biologics
Tech
nolo
gy %
of
Rx
& O
TC S
ales
343126
0
666974100
0
20
40
60
80
100
2015E 2010E 2006 2000 Biologics Conventional
% o
f Tot
al S
ales
Percentage of Worldwide Rx & OTC Pharmaceutical Sales from Biotech vs. Conventional Technologya
Unlike the overall industry, orals are gaining share in Oncology
Oncology Market for Targeted Therapies: Biologics vs. Conventional Technologyb
60% 40% 20% 0%
2000 11%
2008 28%
2014 50%
10% 30% 50%
4

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 19
Oral oncologics are managed using traditional utilization tools…
204417 417 417 417 417
22222 10814810941
36
3434343434
0
500
1,000
1,500
2,000
Tamoxifen
1,648
1,444
Tykerb
1,648
210
877
Thalomid
1,648
174
873
Tarceva
1,648
207
879
Sutent
1,648
275
879
Glivec
1,645
274
882
Num
ber o
f PD
Ps
cove
ring
drug
s
Traditional tools such as tier status, prior authorization, quantity limits and co-payments are being adopted for oral oncologics
Note: 1Selected drugs include Glivec, Sutent, Tarceva, Thalomid, Tykerb and Tamoxifen (Data from November 2008 for Medicare Part D plan) Source:a“Cost Sharing for Cancer Patients in Medicare, 2009”, Avalere Health and American Cancer Society Cancer Action Network, December 2008
Formulary Status of Oral Oncology Brandsa,1
Tier 1 Tier 2 Tier 3 Tier 4 Tier 5 Tier 6
Drug % of Plans with Drug on Formulary
Primary Tier Placement
% of Plans: Prior Authorization
% of Plans: Quantity Limits
Primary Cost- Sharing Range
Gleevec 100% 4 70% 29% 26% - 35%
Sutent 100% 4 62% 32% 26% - 35%
Tarceva 100% 4 62% 32% 26% - 35%
Thalomid 100% 4 68% 25% 26% - 35%
Tykerb 100% 4 74% 42% 26% - 35%
Tamoxifen 100% 1 0% 2% $ 0 - $10
4

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 20
… and this trend is increasing over time
4641
57
40
7167
42
5348
6264
556360
7271686876
0
20
40
60
80
Tykerb2 Thalomid Tarceva Sutent Gleevec
2009 2008 2007 2006
PD
Ps
requ
iring
Prio
r au
thor
izat
ion
(% )
PDP’s1 Requiring Prior Authorization, 2006–2009a
Enr
ollm
ent-W
eigh
ted
Ave
rage
C
oins
uran
ce A
mou
nt (%
)
Note: 1PDP’s are Prescription Drug Plans; 22006 data omitted for Tykerb because the Food and Drug Administration (FDA) approved the drug in March 2007 Source: a“Cost Sharing for Cancer Patients in Medicare, 2009”, Avalere Health and American Cancer Society Cancer Action Network, December, 2008; b“Oncology trends report”, NCCN
282727272930
2829283030303030
3331
333333
0
5
10
15
20
25
30
35
Tykerb2 Sutent Gleevec Thalomid Tarceva
% Coinsurance Amount, 2006-2009a
PDPs are increasing the use of prior authorization to control access to branded cancer drugsa,b
• However, the administrative burden of obtaining prior authorization is high, and the process is time-consuming for payers and providersb
PDPs are shifting the cost burden to the patients by gradually increasing co-insurance amounts for brand-name oral anticancer drugsa
2009 2008 2007 2006
PDP’s are increasing the use of traditional utilization tools such as prior authorization and co-payments
4

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 21
Table of Contents
Historical Market Dynamics
Evidence of Changes
Case Studies
How to Prepare

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 22
Case Studies: Close But Not Yet
We are clearly seeing different dynamics in the oncology market than we have historically However, we have not yet seen significant
competition driven solely by pricing. This is a scenario which could emerge when there are multiple, largely equivalent agents available in the marketplace To date, potential competitive situations
(Erbitux vs Vectibix, Nexavar vs Sutent and Tykerb vs Herceptin) have resolved quickly with clear winners based on clinical data, labeling, and physician preference (not payor pressure)

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 23
Case Study 1 – Vectibix position to displace the similar Erbitux was thwarted by clinical data
Erbitux was launched by BMS/Imclone in 2004 for metastatic colorectal cancer patients1
Vectibix was launched in September 2006 by Amgen for metastatic colorectal cancer patients2
• Analysts expected that Vectibix would replace Erbitux as a treatment for colon cancera,b
Both Vectibix and Erbitux are antibody-based therapies that are administered intravenously; however Vectibix had a few potential advantages
• More convenient (every other week) administration and lower cost (20% discount) compared to Erbituxb
• Lower frequency of infusion reactions (1% compared to 3% for Erbitux) i,j
Sales of Vectibix in 2006 (Oct-Dec) were USD 39MM and the company was upbeat about the futurec
Analysts at Merrill Lynch predicted that Vectibix would eventually take 60% of Erbitux's market. They also lowered their projected sales figures for Erbitux for 2008-2010d
Scenario at Launch
In March 2007, Amgen discontinued a trial of Vectibix due to 231 cases of death or disease progression. Vectibix sales in the second quarter of 2007 fell from USD 51MM to USD 46MMe,f
Erbitux maintained steady growth even after the launch of Vectibix
• The total number of patients treated with Erbitux increased in October 2007, and market share rose to 14.8% in that month g
• Vectibix did not show any month-to-month market share increase (in October 2007) and was underperforming according to analystsg
In 2009, label changes for both Erbitux and Vectibix were implemented; these are expected to narrow the eligible pool of patients for both the drugs by up to 40%h
What Happened?
Erbitux vs Vectibix
Note: 1Approved as a single agent for EGFR-expressing metastatic colorectal cancer after failure of both irinotecan- and oxaliplatin-based regimens or in patients who are intolerant to irinotecan-based regimens OR used in combination with irinotecan, EGFR-expressing metastatic colorectal carcinoma in patients who are refractory to irinotecan-based chemotherapy; 2Approved as a single agent for the treatment of metastatic colorectal carcinoma with disease progression on or following fluoropyrimidine, oxaliplatin, and irinotecan chemotherapy regimens
Source: aPress release, September 27, 2006, Amgem company website; b“Vectibix Will be EGFR Antibody of Choice for Colon Cancer Therapy”, October 6, 2006, GLG group website; cAnalyst conference summary of Amgen quarter results, January 27, 2007, Openicon website; d”Amgen wins approval for colorectal cancer drug”, September 28, 2006, Marketwatch website; e”Amgen Discontinues Vectibix(TM) Treatment in PACCE Trial Evaluating Vectibix(TM) as Part of Triple Combination Regimen”, March 23, 2007, Biotechnoloogy-europe website; fPress Release, July 26, 2007, Pfizer company website; g“Monthly oncology regimen report through September 2007”, Rodman & Renshaw, Inc.,October 22, 2007; h“New US labelling for Erbitux and Vectibix recommends against their use for large subset of colorectal cancer patients”, July 20, 2009, Scripnews website; i"Vectibix(R) Now Available For The Treatment Of Advanced Colorectal Cancer In Belgium, October 03, 2008, Medicalnewstoday website; jErbitux website "

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 24
Case Study 2 – In another potential head-to-head battle, physicians chose Sutent over Nexavar
Note: 1Sutent is a kinase inhibitor indicated for the treatment of: (i)Gastrointestinal stromal tumor after disease progression on or intolerance to imatinib mesylate (ii) Advanced renal cell carcinoma; 2Nexavar is a kinase inhibitor indicated for the treatment of advanced renal cell carcinoma Source: aPress Release, December 20, 2005, Company website; b”Stakeholder Opinions: Renal Cell Carcinoma - Novel Targeted Treatments to Fill the Void”, December 2005, Researchandmarkets report; c”FDA approves Bayer's kidney cancer drug”, December 22, 2005, Pharmafocus Website; d”Torisel: The New Kid on the Block for Advanced Renal Cell Carcinoma”, September 2007, Oncbiz website; e”Nexavar and Sutent, Both Indicated for Metastatic RCC, Look Set to Compete Well to the End of the Decade - Nexavar's 2010 Revenues Are Forecast to Reach $122 Million and Sutent's $179 Million”, February 13, 2006, Business Wire
Nexavar was launched by Bayer/Onyx in December 2005 for advanced renal cell carcinomaa,2
Sutent was launched by Pfizer in 2006 for the same indication1
Direct competition was expected: • Datamonitor forecasted Nexavar revenues would
reach USD 122MM and Sutent would reach USD 179MM by 2010b
• Although Nexavar had a first-to-market advantage, Sutent was expected to have superior efficacye
• Nexavar on the other hand, was expected to have better tolerability – side-effects were limited mainly to blistering and rashesc
• Cost of treatment was similar for both Sutent and Nexavar at USD 4,600 per treatment/monthd
Scenario at Launch
Sutent rapidly captured over 50% market share in renal cell carcinoma for all lines of therapy (July 2006)d
• Sutent became the standard therapy for first-line treatment of mRCC after launche;
• Nexavar competed more successfully in second line therapy with 35.1% patients receiving Sutent and 32.4% receiving Nexavar (October 2007)d
What Happened?
Nexavar vs Sutent
333333343333323434323234
565555535351515151535452
0
20
40
60
80
100
06/2006 10/2006 08/2006 12/2006 02/2007 04/2007 06/2007
Nexavar
Sutent
Mar
ket S
hare
%
Renal Cell Carcinoma Market share (All stages/ All lines)d

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 25
Case Study 3 – Tykerb could not displace Herceptin without more data and a better label
Note: 1Reported as £ 62 million, conversion factor used as on November 16, 2009 Source: a“Analysts raise NPVs of Promacta and Rezonic; Tykerb still star of GSK oncology pipeline”, Goliath Business News, July 2007 ; bBear Stearns report September 21, 2007; cPR News wire August 14, 2007; dGSK Annual Report, 2008; Grail analysis; eDrugs @ FDA; fClinicaltrial.gov; gkomenozark.org; hGenentech Website; iGSK press release; j“Tykerb Approved for Metastatic HER2+ Breast Cancer “, cancernetwork.com, April 2007; k“Glaxo's Tykerb still has some convincing to do”, Evaluate Pharma, March 2008
Herceptin was the first targeted therapy to be launched for the treatment of breast cancer in 1998
Tykerb (oral therapy) was launched in 2007 as combination therapy with capecitabine (Xeloda), for the treatment of patients with advanced or metastatic breast cancer (mBC) with HER2 over-expression and who progressed on prior therapy including an anthracycline, a taxane, and Herceptine
• Tykerb was approved in a second or third line settingk
• At the time of launch, GSK marketed Tykerb as a more convenient and user-friendly oral therapyg
Expectations for Tykerb were mixed at the time of launch: • Some analysts expected the drug to achieve blockbuster status by
2010a. Analysts assumed that drug would be effective in difficult to treat patients and patients with brain metastases, Tykerb was expected to gain share in first line and adjuvant settings.
• Others predicted Tykerb’s use would be limited until it demonstrated significant benefits when added to Herceptin.
• Analysts forecasted Tykerb sales to reach USD 104 MM1 in 2008b
At the time of launch, analyst expected the biggest sales opportunity for Tykerb to be in the adjuvant setting in the breast cancer marketb
Scenario at Launch
Tykerb reported modest global sales of USD 145.3MM in 2008d
• Sales were far behind Herceptin’s, which recorded global sales of USD 1.82 billion in 2008h
Factors contributing to Tykerb’s limited revenues were: • In August 2007, a study conducted by Decision Resources suggested
that oncologists did not prefer Tykerb as a replacement for Herceptin. Instead they were only using it as an alternative for Herceptin-refractory patients in the treatment of advanced breast cancerk
• 58% of oncologists opined that they would favor IV Herceptin over Tykerb because the administration of IV drugs remains an important source of income for their practicec
To boost revenues from Tykerb in breast cancer, the company decided to expand use of Tykerb in an adjuvant setting: • As of April 2007, GSK was studying Tykerb for its application in adjuvant
breast cancer : "We are dedicated to the further study and development of Tykerb in a variety of settings, including adjuvant breast cancer as well as in other solid tumor types“j
-Paolo Paoletti, MD, Oncology Medicine Development Center,GSK • GSK launched a head-to-head trial of Tykerb versus Herceptin in
adjuvant breast cancer in 2008. Results for this trial are expected by May 2013f
• In April 2009, GSK submitted an application to expand Tykerb use for first-line treatment of metastatic breast canceri
What Happened?
Tykerb vs Herceptin

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 26
Table of Contents
Historical Market Dynamics
Evidence of Changes
Case Studies
How to Prepare

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 27
Preparing for a New Dynamic
While direct, payor-driven competition among oncology agents has not yet arrived, manufacturers need to be prepared for changes in the oncology market Manufacturers may want to conduct head-to-
head trials, or define market subsets where they can demonstrate superiority to potential alternative agents Manufacturers may also want to consider
scenarios where there are multiple agents with similar therapeutic profiles available for a given indication

| Copyright © 2010 Grail Research, a division of Integreon February, 2010 28
For More Information Contact:
Grail Research ([email protected])
Copyright © 2010 by Grail Research, a division of Integreon
No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means — electronic, mechanical, photocopying, recording, or otherwise — without the permission of Grail Research, a division of Integreon
Top Related