



![Research Article Nerve Dysfunction in Hallux Valgus is Correlated … · Coughlin [3]. While a neuromuscular misbalance is obviously responsible for the deformity in most instances,](https://static.fdocuments.us/doc/165x107/60229ba9dac6560dbd0a2bd5/research-article-nerve-dysfunction-in-hallux-valgus-is-correlated-coughlin-3.jpg)

Languages
Pages
Legal

8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 1/31
EDUARDO V. BONGAT JR., PTRP, RM, RN(USRN)

8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 2/31
TetanusyAlso called lockjaw
yAn acute, preventable, and oftenfatal disease
yCaused by exotoxin of C lostridiumtetani
yCharacterized by muscle rigidityinvolving the masseter and neckmuscles
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 2

8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 3/31
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 4/31
TetanusySpores are found in soil, dust, and GItract of humans and animals
yBacteria enter body through wound,especially puncture or crush woundor burn
yMay enter through scratch, bee sting,thorn, or needle prick
yExposure greater during outdoor
activitiesMosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 4
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 5/31
Pathophysiology of TetanusyExotoxin spreads from wound toCNS by way of neurons orbloodstream
yToxin becomes fixed on nerve
cells of brainstem and spinal cordyToxin produces muscle stiffness
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 5
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 6/31
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 7/31
Clinical Manifestations of Tetanus
(cont.)
y Respiratory: accumulated secretions,atelectasis, pneumonia, respiratory arrest
y Patient anxious but alert; mentationunaffected
y Rapid HR, diaphoresis, mild or absentfever
y Incubation: 3 to 10 days
y Mortality approximately 30%; usually fatalin newborn
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 7
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 8/31
Therapeutic Management of
TetanusyPrevention by tetanus toxoid ortetanus antitoxin after exposure
yTreatment of wounds contaminatedwith dirt, feces, soil, saliva, puncturewounds, avulsions, crushing, burns,
and frostbite should include tetanusimmune globulin if patientinadequately immunized
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 8
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 9/31
Therapeutic Management of
Tetanus (cont.)y ICU for constant observation and respiratory
support availability
y Monitor fluid and electrolyte statusy Tetanus immune globulin therapy to neutralize
toxins
y Wound care to decrease organism
proliferationy Muscle relaxants, sedatives, pancuronium
(Pavulon)
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 9
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 10/31
Nursing ConsiderationsyControl environmental stimuli
y
Careful monitoring of respiratorystatus
yAttempt to reduce anxiety of
child and family
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 10
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 11/31
Nursing ConsiderationsyControl environmental stimuli
y
Careful monitoring of respiratorystatus
yAttempt to reduce anxiety of
child and family
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 11
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 12/31
BotulismyFood poisoning resulting fromingestion of toxin produced by the
anerobic bacillus C lostridiumbotulinum
ySources:
y Improperly sterilized home cannedfoods for older children
y Infant sources: honey and light or
dark corn syrupMosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 12
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 13/31
Clinical Manifestations of
BotulismyCNS symptoms appear abruptly
12 to 36 hours after ingestion
yGeneral signs
yWeakness, dizziness, headache,diplopia, speech difficulties
yVomiting
yProgressive, life-threateningrespiratory paralysisMosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 13
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 14/31
Treatment of BotulismyIV botulism antitoxin
y
Supportive measures²respiratory support
yContinue therapy until paralysis
abates
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 14
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 15/31
Infant BotulismyCaused by ingestion of spores orvegetative cells of C. botulinum and
subsequent release of toxin
ySource of botulism in infants: honey,and light or dark corn syrup fed to
themyWide variation in severity of disease:mild constipation to respiratory
failureMosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 15
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 16/31
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 17/31
Spinal Cord InjuriesyGenerally result of indirect trauma
yEspecially in MVC without childrestraints
yVertebral compression from blows tothe head or buttocks (diving, surfing,
falls from horses)yBirth injuries from traction force onspinal cord during breech delivery
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 17
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 18/31
Levels of Spinal Cord
Injuriesy Higher injury²more extensive damage
y Paraplegia: complete or partial paralysis of
lower extremitiesy Tetraplegia: lacking functional use of all
four extremities (formerly calledquadriplegia)
y High cervical cord injury affects phrenicnerve, paralyzes diaphragm ventilatorydependency
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 18
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 19/31
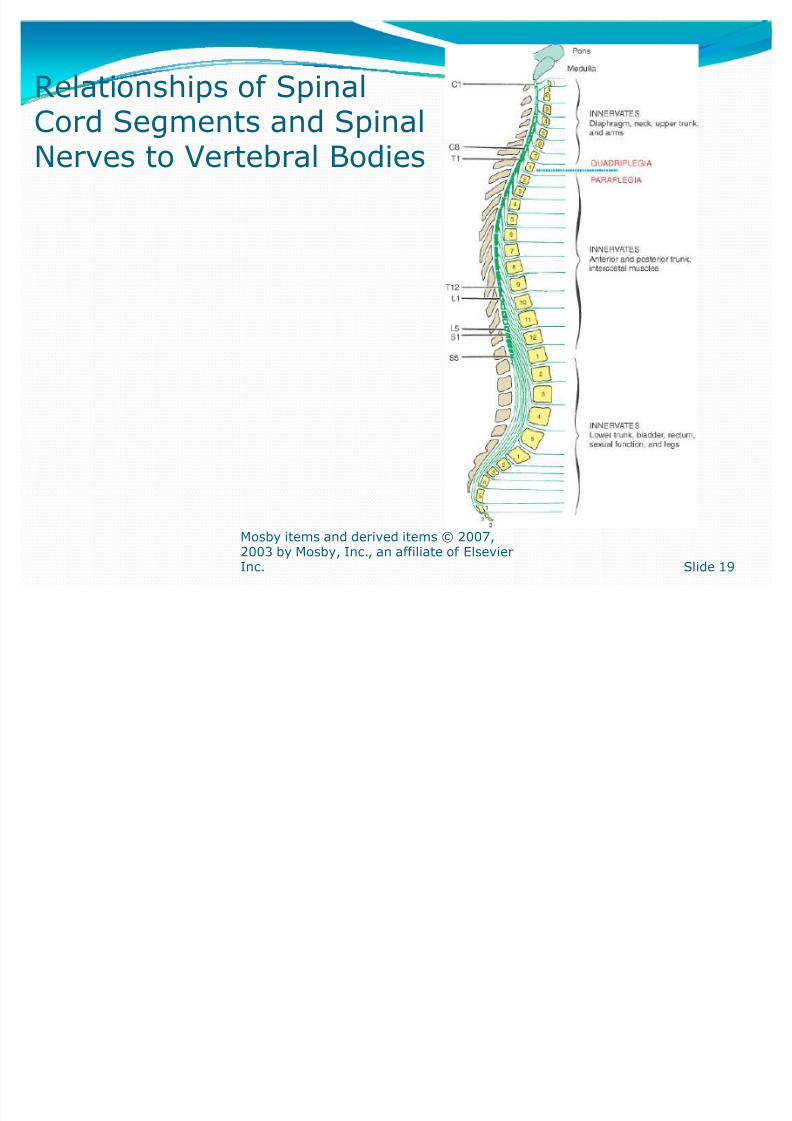
Relationships of SpinalCord Segments and SpinalNerves to Vertebral Bodies
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 19

8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 20/31
Spinal Cord Injuryy Therapeutic management: stabilization
and transport to pediatric trauma center
environmenty Management is complex and controversial
y Nursing considerations
y Stabilization, careful assessment,prevention of complications, maintainmaximum function
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 20
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 21/31
Nursing Management
of Spinal Cord InjuriesyRespiratory care
yTemperature regulation
ySkin care
yPhysiotherapy
yNeurogenic bladder
yBowel training
yAutonomic dysreflexiaMosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 21
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 22/31
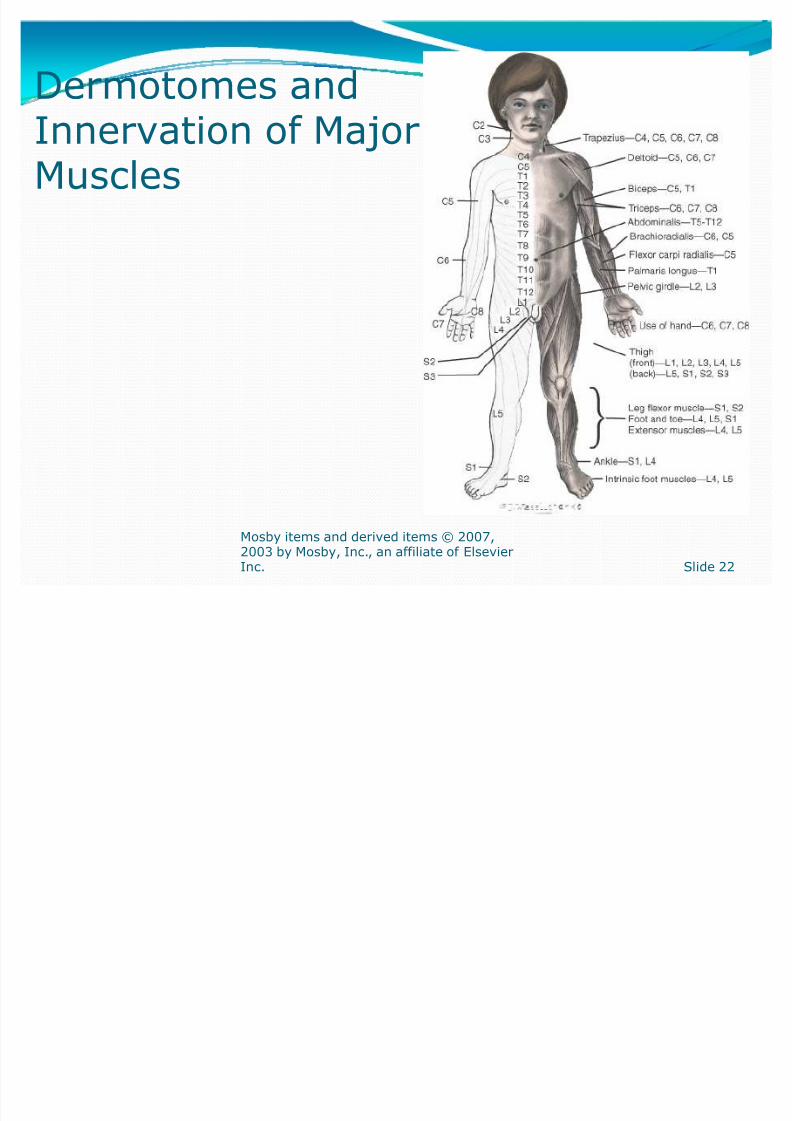
Dermotomes and
Innervation of MajorMuscles
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 22
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 23/31
RehabilitationyEvaluation and support
y
RemobilizationyPhysical rehabilitation
yPsychosocial rehabilitation
ySexuality issues
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 23
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 24/31
Muscular Dystrophies (MDs)yLargest group of muscular diseases inchildren
yAll have genetic origin with gradualdegeneration of muscle fibers,progressive weakness, and wasting of
skeletal musclesyAll have increasing disability anddeformity with loss of strength
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 24

8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 25/31
Initial Muscle Groups Involvedin MDs
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 25
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 26/31
Duchenne Muscular
Dystrophy (DMD)yAlso called pseudohypertrophic muscular dystrophy
yMost severe and most common of theMDs in childhood
yX-linked inheritance pattern; one
third are fresh mutationsy Incidence: 1 in 3500 male births
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 26
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 27/31
Characteristics of DMDyOnset between ages 3 and 5 years
yProgressive muscle weakness,wasting, and contractures
yCalf muscles hypertrophy in mostpatients
yProgressive generalized weakness inadolescence
yDeath from respiratory or cardiac
failure
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 27
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 28/31
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 29/31
DMD: Clinical Manifestationsy Waddling gait, frequent falls, Gower sign
y Lordosis
y Enlarged muscles, especially thighs and upperarms
y Profound muscular atrophy in later stages
y Mental deficiency common
Mosby items and derived items © 2007,
2003 by Mosby, Inc., an affiliate of ElsevierInc. Slide 29
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 30/31
8/8/2019 NeuroMuscular Dysfunction
http://slidepdf.com/reader/full/neuromuscular-dysfunction 31/31
Top Related