





Languages
Pages
Legal

7/28/2019 Nclex-pn Chapter 19 Bwfinal
1/12
402 CHAPTER19 IteuetarSste
402
IteuetarSste
6. Whatisthediethistory?Doestheclienthaveany
foodallergies?
B. Physicalassessment.
1. Inspection.
a. Assesstheskinforcolor:jaundice,cyanotic,ushed.
b. Determineifthereareareasofbruising,purpura,or
petechiae.
c. Determineifskinblanchesondirectpressure.
d. Assesslesionsfortype,color,size,distribution,and
grouping;locationandconsistency.
e. Assessforunusualodors,especiallyaroundlesions
orareas(axilla,overhangingabdominalfolds,and groin).
f. Commondermatologicallesions.
(1) Macule:at,circumscribedareaofcolor
changeintheskinwithoutsu rfaceelevation.
(2) Papule:circumscribed,solid,andelevated
lesion.
(3) Nodule:raised,solidlesionthatislargerand
deeperthanapapule.
(4) Vesicle:smallelevationinskinusuallylled
withserousuidorblood;bulla:largerthana
vesicle;pustule:vesicleorbullalledwithpus.
(5) Wheal:elevationoftheskincausedbyedema
ofthedermis. (6) Cyst:massofuid-lledtissuethatextendsto
thesubcutaneoustissueordermis.
PHySIologyoTHESKIn
A. Structure
1. Epidermisoutermostlayer.
2. Der misconnectivetissuebelowepider mis;
vascular;assistsinbodytemperatureandblood
pressureregulation.
3. Hypodermis(subcutaneous)locatedbelowder-
mis;anchorsthemusclesandbonestotheskin.
4. Nail.
a. Consistsofahard,transparentplateofkeratin.
b. Growsfromtheroot,whichliesunderathin
foldofskincalledthecuticle.5. Hair.
a. Presentovertheentirebodyexceptforthe
palmsofthehandsandthesolesofthefeet.
b. Piloerectorresponse:contractionofthet iny
erectormusclesattachedtothehairfolliclethat
leadstohairstandingonendorgooseesh.
6. Sebaceousglands:secretesebum,whichisanoily
secretionthatisemptiedintothehairshaft.
B. Functionsoftheskin.
1. Protection:primaryfunction.
2. Sensory:majorreceptorforgeneralsensation.
3. Waterbalance.
a.600to900mlofwaterislostdailythrough insensibleperspiration.
b. Formsabarrierthatpreventslossofwaterand
electrolytesfromtheinternalenviron ment.
4. Temperatureregulation.
5. InvolvedintheactivationofvitaminD.
6. Involvedinwheal-and-arereaction.
a. Wheal:swelling.
b. Flare:diffusedredness.
c. Theseresponsesareduetolocaledema.
System Assessment
A. Healthhistory(Box19-1). 1. Howlonghastheparticularrash,lesion,or
problembeenpresent?
2. Isthereanyitching,bur ning,ordiscomfor t
associatedwiththeproblem?
3. Hastheclientbeenincontactwithanyirritants,
sun,unusualcold,orunhygienicconditions?
4. Hasanyoneinthefamilyeverhadthissametypeof
problemwithhisorherskin?
5. Istheclienttakinganymedications?
Ski Increasedwrinklingandsagging,redundant
esharoundeyes,slownessofskintoattenwhen
pinchedtogether(tenting)
Dry,akingskin:excoriationfromscratching Decreasedrateofwoundhealing
Evidenceofbruising
Hair Graying,thinning,baldness;dry,scalyscalp
nais Thick,brittlenailswithdiminishedgrowth;
ridging
Prolongedreturnofbloodwithblanching
BOX 19-1 OLDER ADULT CARE FOCUS Differences in Skin Assessment Skin
7/28/2019 Nclex-pn Chapter 19 Bwfinal
2/12
CHAPTER19 IteuetarSste 403
2. Palpation.
a. Determinetemperature(usebackofhand),skin
turgor(onolderadultspinchskinonabdomenor
forehead),andmobility.
b. Evaluatemoistureandtexture.
TESTALERT: Assess skin integrity and use
measures to maintain client skin integrity.
BEnIgn&InlAmmAToRyDISoRDERSoTHESKIn
Acne Vulgaris
Acne is an inammatory disorder of the sebaceous
glands and their hair follicles.
Data Collection
A. Morecommoninteenagers;maypersistintoadulthood.
B. Underhormonalinuenceduringpuberty;affectedby
presenceofandrogen,whichstimulatesthesebaceous glandstosecretesebum.
C. Inammatorylesionsorpustules.
D. Cysts:deepnodulesthatmayproducescarring.
Treatment
A. Medical:topicalorsystemictherapy.
Home Care
A. Instructclienttocleansefacetwicedailybuttoavoid
overcleansing.
B. Mayuseapolyesterspongepadtocleanse,becauseit
providesamechanicalremovaloftheepidermallayer.
C. Instructclienttokeephandsawayfromfaceandtoavoid
anyfrictionortraumatothearea;avoidproppinghands
againstface,rubbingface,etc.
D. Emphasizetheimportanceofanutritiousdiet;encourage
adequatefoodintakeanduseofvitaminA.
E. Avoidtheuseofcosmetics,shavingcreams,andlotion,
becausetheymayexacerbateacne;ifcosmeticsaretobe
used,water-basedmake-upispreferable.
F. Instructtheclienttoadministermedicationappropri-
ately:topicalapplication;avoidsunlightwhileusing
medications,etc.
Psoriasis
Psoriasis is a chronic inammatory disorder
characterized by rapid turnover of epidermal cells.
Data Collection
A. Silveryscaling,plaquesontheelbows,scalp,knees,
palms,soles,andngernails.
B. Ifscalesarescrapedaway,adarkredbaseofthelesion
isseen,whichwillproducemultiplebleedingpoints.
C. Mayimprovebutoftenrecursthroughoutlife.
D. Bilateralsymmetryofsymptomsiscommon.
Treatment
A. Medical.
1. Topicaltherapy.
a. Coaltarpreparation(Anth ralin).
b. Corticosteroids. 2. Photochemotherapy(PUVAtherapy):psoralen,
ultravioletAtherapy(mustwearprotectiveeyewear
duringtreatmentandfor24hoursaftertherapy).
3. Systemictherapy:antimetabolites(methotrexate);
immunosuppressants.
Home Care
A. Encourageverbalizationofan xietyregarding
appearance.
B. Instructclienttouseasoftbrushtoremovescaleswhile
bathing.
C. Assessclienttodeterminefactorsthatmaytriggerskin condition(e.g.,emotionalstress,trauma,seasonal
changes).
D. Makesureclientunderstandstreatmentandimplications
ofcarerelatedtoPUVAtherapyandothertreatments.
Atopic Dermatitis
Atopicdermati tis (also called eczema) is a supercial
chronic inammatory disorder associated with allergy with
a hereditary tendency (atopy); condition usually occur
during infancy, usually between 2 and 6 months of age.
Data CollectionA. Reddenedlesions,occuronthecheeks,arms,andlegs;
antecubitalandpoplitealspaceinadults;mayhave
oozingvesicles.
B. Intenseitching(worseatnight).
C. Infantswitheczemaaremorelikelytohaveallergiesas
childrenandadultsanddevelopasthma.
Treatment
A. PruritusistreatedwithBenadryl,topicalsteroids,and
withimmunomodulators.
Home CareA. Teachparentsaboutdietaryrestrictions;providethem
withwrittenguidelines.
B. Keepngernailsandtoenailscutshort.
C. Feedthechildwhenheiswellrestedandisnotitching.
D. Childshouldwearnonirritatingclothing;wooland
abrasivefabricsshouldbeavoided.
E. Tepidbathwithmildsoaporaeumulsifyingoil
followedimmediatelybyapplicationofanemollient;
coolcompressestodecreaseitching.
7/28/2019 Nclex-pn Chapter 19 Bwfinal
3/12
404 CHAPTER19 IteuetarSste
Contact Dermatitis
Contactdermatitis is an inammatory skin reaction
that results because the skin has come in contact with a
specic irritant - diaper dermatitis (prolonged contact with
urine, feces, ointments, soaps, or fricition) or an allergen
(allergic contact dermatitis, which is usually a symptom of
delayed hypersensitivity).
Data Collection
A. Pruritus;hive-likepapules,vesicles,andplaques(more
chronic).
B. Sharplycircumscribedareas(withoccasionalvesicle
formation)thatcrustandooze.
Treatment
A. Medical.
1. Topicalsteroids;oralsteroidsforseverecases.
2. Antihistamines,antipruriticagents,andantifungals
(diaperdermatitis). 3. Aveeno(oatmeal)bathsandtopicalsoaks.
Home Care
A. Teachimportanceofwashingexposedskinwithcool
waterandsoapassoonaspossibleafterexposure(within
15minutesisbest).
B. Providecool,tepidbath;trimngernails,anduse
measurestocontrolitching.
C. Frequentdiaperchanges,keepskindry,anduse
protectiveointment(zincoxideorpetrolatum).
Pressure Ulcer
Apressureulcer(decubitusulcer,bedsore ) is localized
injury to the skin and/or underlying tissue usually over a
bony prominence, as a result of pressure, or pressure in
combination with shear and/or friction.
NURSING PRIORITY: Identify potential for
skin breakdown: a pressure ulcer can be and should be
prevented. Identify those clients at increased risk for
ulcer development and begin preventative care as soon
as possible. Do not wait for the reddened area to occur
before preventative measures are initiated.
Assessment
A. Riskfactors/etiology.
1. Prolongedpressurecausedbyimmobility.
2. Malnutrition,hypoproteinemia,vitamindeciency.
3. Infection,advancingage.
4. Skindryness,maceration,excessiveskinmoisture.
5. Equipmentsuchascasts,restraints,tractiondevices,etc.
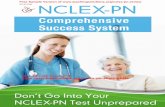
B. ClinicalmanifestationsseeFigure19-1.
Treatment
A. Medicalandsurgical.
1. Debridement(init ialcareistoremovemoist,
devitalizedtissue).
a. Sharpdebridement:useofascalpelor
otherinstrument;usedprimarily,especiallywith
cellulitisorsepsis.
Suspected Deep Tissue Injury: Purpleor maroonlocalized area
ofdiscoloredintactskin orblood-lledblister duetodamageof
underlyingsofttissuefrompressureand/orshear.Theareamaybe
preceded by tissue that is painf ul, rm ,mushy,b oggy,warmer or
coolerascomparedtoadjacenttissue.
Further description:Deeptissueinjurymaybedifculttodetectin
individualswithdarkskintones.Evolutionmayincludeathinblister
overadarkwoundbed.Thewoundmayfurtherevolveandbecomecoveredbythineschar.Evolutionmayberapidexposingadditional
layersoftissueevenwithoptimaltreatment.
Stage I: Intactskinwithnon-blanchablerednessofalocalizedarea
usuallyoverabonyprominence.Darklypigmentedskinmaynothave
visibleblanching;itscolormaydifferfromthesurroundingarea.
Further description:Theareamaybepainful,rm,soft,warmer
orcoolerascomparedtoadjacenttissue.StageImaybedifcultto
detectin individualswith darkskin tones.Mayi ndicateatrisk
persons(aheraldi ngsignofrisk)
Stage II: Partialthickness lossofderm ispresentingas ashallow
openulcerwitharedpinkwoundbed,withoutslough.Mayalso
presen tasanint actoropen/ru pture dserum-lle dbliste r.
Further description:Presentsasashinyordryshallowulcerwithout
sloughorbruising.*Thisstageshouldnotbeusedtodescribeskin
tears,tapeburns,perinealdermatitis,macerationorexcoriation.
*Bruisingindicatessuspecteddeeptissueinjury
Stage III: Full thickness tissue loss. Subcutaneous fat may be
visiblebutbone,tendonormusclearenotexposed.Sloughmaybe
present butd oes not obscure the depth oft issue loss. Mayi nclude
underminingandtunneling.
Further description:ThedepthofastageIIIpressureulcervaries
by anatomic al location. The bridge of the nose, ear, occiput and
malleolusdonothavesubcutaneoustissueandstageIIIulcerscan
be shallow. In contr ast, area s of signi cant adiposit y can develop
extremelydeepstageIIIpressureulcers.Bone/tendonisnotvisible
ordirectlypalpable.
Stage IV: Fullthicknesstissuelosswithexposedbone,tendonor
muscle.Sloughorescharmaybepresentonsomepartsofthewound
bed.Ofteni ncludeunderm iningandt unneli ng.
Further description: ThedepthofastageIVpressureulcervaries
by anatomic al location. The bridge of the nose, ear, occiput and
malleolusdonothavesubcutaneoustissueandtheseulcerscanbe
shallow.StageIVulcerscanextendintomuscleand/orsupporting
structures(e.g.,fascia,tendonorjointcapsule)makingosteomyelitis
possible.Expo sedbone/tend onisvisibleordi rectlypalpable.
Unstageable:Fullthicknesstissuelossinwhichthebaseoftheulcer
iscoveredbyslough(yellow,tan,gray,greenorbrown)and/oreschar
(tan,brownorblack)inthewoundbed.
Further description:Untilenoughsloughand/orescharisremoved
toexposethebaseofthewound,thetruedepth,andthereforestage,
cannotbedetermined.Stable(dry,adherent,intactwithouterythema
oructuance) eschar onthe heels serves as thebodys natural
(biological)coverandshouldnotberemoved.
Figure 19-1:Stages of Pressure Ulcers
IgURE 19-1 Staes Pressure Ucers Reprinted withpermission: National Pressure Ulcer Advisory Panel. (2007). PressurUlcer Stages Revised by NPUAP. Retrieved July 31, 2008 from http:/www.npuap.org/resources.htm
7/28/2019 Nclex-pn Chapter 19 Bwfinal
4/12
CHAPTER19 IteuetarSste 405
b. Mechanicaldebridement:wet-to-drydressings,
hydrotherapy,woundirrigation,anddextranomers
(smallbeadspouredoversecretingwoundstoabsorb
exudate).
c. Enzymaticandautolyticdebridement:useof
enzymesorsyntheticdressingsthatcoverwoundand
self-digestdevitalizedtissuebytheactionof
enzymesthatarepresentinwounduids.2. Woundcleansing(usenormalsalinesolutionformost
cases).
a. Useminimalmechanicalforcewhencleansingto
avoidtraumatothewoundbed.
b. Avoidtheuseofantiseptics(e.g.,Dakinssolution,
iodine,hydrogenperoxide).
3. Dressings(shouldprotectwound,bebiocompatible,and
hydrate).
a. Moistenedgauze.
b. Film(transparent).
c. Hydrocolloid(moistureandoxygenretaining).
NURSINGPRIORITY: Keep the ulcer tissue moist
and the surrounding intact skin dry.
B. Dietary.
1. Increasedcarbohydratesandprotein.
2. IncreasedvitaminCandzinc.
Nursing Intervention
v Goal: Topreventorrelievepressureandstimulate
circulation.
A. Frequentchangeofposition;turnclientevery1to2
hours.B. Specialbedswithmattressesthatprovidefora
continuouschangeinpressureacrossthemattress.
C. Siliconegelpadsplacedunderthebuttocksofclientsin
wheelchairs.
D. Sheepskinpadstoprovideasoftsurfacetoprotectthe
skinfromabrasion.
E. Eggcrateorfoammattresstoallowcirculationunderthe
bodyandkeeptheareadry.
F. Activeandpassiveexercisestopromotecirculation.
v Goal: Tokeepskincleanandhealthyandpreventthe
occurrenceofapressureulcer.
A. Washskinwithmildsoapandblotcompletelydrywith
softtowel. 1. Avoidhotwaterandexcessiverubbing.
2. Uselotionorprotectivemoisturizerafterbathing.
B. Inspectskinfrequently,especiallyoverbony
prominences.
NURSING PRIORITY: Avoid massage over
bony prominences. When the side-lying position is used in
bed, avoid positioning client directly on the trochanter use
the 30 lateral inclined position. Do not use donut-type
devices. Maintain the head of the bed at or below 30 or
at the lowest degree of elevation. Encourage chair-bound
persons, who are able, to shift weight every 15 minutes.
C. Removeanyforeignmaterialfromthebed,becauseit
mayserveasasourceofirritation;keepsheetstightly
stretchedonbedtopreventwrinkles.
v Goal: Topromotehealingofpressureulcer.
A. Usemethodsdiscussedtodecreasethepressureonthe
areainwhichthepressureulcerisfound.
1. Air-uidizedbeds-stageIIIorstageIVpressure
ulcers
2. Staticsupportsurfaces-notrecommendedforStage
IIIorIV.
B. Keeptheulcerareadry.
1. Minimizeskinexposuretomoisturecausedby incontinence,perspiration,orwounddrainage.
2. Useonlyunderpadsorbriefsthataremadeof
materialsthatabsorbmoistureandprovideaquick-
dryingsurfacenexttotheskin.
3. Positiontheclientwiththeulcerexposedtoair;may
uselighttoincreasedryingandpromotehealing.
C. Useskinbarrierstodecreasecontaminationandincrease
healingofanoninfectedulcer.
D. Observetheulcerforsignsofinfection.Infectedulcers
willhavetobedebrided,ifhealingistooccur.
SKInInECTIonSAnDInESTATIonS
Impetigo
Impetigo is a bacterial skin infection caused by
invasion of the epidermis by pathogenic Staphylococcus
aureus and/or group A beta-hemolytic streptococci.
Data Collection
A. Pustule-likelesionswithmoisthoney-coloredcrusts
surroundedbyredness.
B. Pruritus;spreadstosurroundingareas.
C. Appearsmorecommonlyontheface,especiallyaround
themouth.
Treatment
A. Medical.
1. Local:topicaltreatment.
a. Gentlewashingtwotothreetimesadayto
removecrusts.
b. Topicalmupirocin(Bactroban)antibioticcream,
ifonlyacoupleoflesionsarefound.
2. Systemicantibiotictherapyisthetreatmentofchoice
withextensivelesions.
7/28/2019 Nclex-pn Chapter 19 Bwfinal
5/12
406 CHAPTER19 IteuetarSste
Home Care
A. Teachtheclientandfamilytheimportanceofgoodhand
washingandthatlesionshealwithoutscarring.
B. Encourageadherencetotherapeuticregimen,especially
takingthefullcourseofantibiotics.
C. Untreatedimpetigomayresultinglomerulonephritis.
Cellulitis
Cellulitis is an inammation of the subcutaneous tissues
often following a break in the skin caused byStaphylococcus
aureus, Streptococcus, or Haemophilus infuenzae.
Data Collection
A. Intenseredness,edemawithdiffuseborder,and
tenderness.
B. Chills,malaise,andfever.
Treatment
A. Medical.
1. Moistheat,immobilization,andelevationofpart.
2. Systemicantibiotictherapyisthetreatmentof
choicewithextensivelesions.
Home Care
A. Teachtheclientandfamilytheimportanceofgoodhand
washing.
B. Encourageadherencetotherapeuticregimen,especially
takingthefullcourseofantibiotics.
Fungal (Dermatophyte) InfectionsAssessment
A. Types.
1. Tineacorporis(ringworm):temporaryhairloss,if
scalpisaffected.
2. Tineacruris(jockitch):small,red,scalypatchesin
thegroinarea.
3. Tineapedis(athletesfoot):scaling,maceration,
erythema,blistering,andpruritus;usuallyfound
betweenthetoes.
4. Tineaunguium(onychomycosis):thickened,
cr umblingnails(usuallytoes)withyellowish
discoloration. 5. Candidiasis:causedbyCandida albicans,knownas
moniliasis,mayaffectoralmucosa,groin,andmoist
areas;whiteplaquesinmouth;diffuseredrashon
skin.
Treatment
A. Topicalantifungalcream(seeAppendix19-1).
B. Oralantifungalmedication.
B. Systemictherapy:Griseofulvin;usedprimarilyfor
extensivecases.
Home Care
A. Topreventathletesfoot,clientshouldbeinstructed
tokeepfeetasdryaspossibleandwearsocksmadeof
absorbentcotton.
1. Talcumpowderorantifungalpowdermaybeused;
Tinactinmaybeappliedtwicedaily.
2. Encourageaerationofshoestoallowthemto completelydryout.
B. Clientshouldmaintainhygienicmeasurestopreventthe
spreadoffungaldiseases,specicallyringwormofthe
scalp.
1. Familymembersshouldavoidusingthesamecomb.
2. Scarvesandhatsshouldbewashedthoroughly.
3. Examinefamilyandhouseholdpetsfrequentlyfor
symptomsofthedisease.
C. Clientshouldavoidinfection.
1. Anyactivitythatallowsheat,friction,and
macerationtooccurmayleadtoskinbreakdownand
infection.
2. Loose-ttingclothingandcottonunderwearareto
beencouraged.
Parasitic Infestations
A. Pediculosis.
1. Types.
a. Pediculus humanus capitis:headlice.
b. Pediculus humanus corporis:bodylice.
c. Phthirus pubis:pubicliceorcrabs.
2. Clinicalmanifestations.
a. Intensepruritus,whichmayleadtosecondary
excoriationandinfection.
b. Tiny,red,noninammatorylesions. c. Eggs(nits)ofbothheadandbodyliceareoften
attachedtothehairshafts.
d. Pubicliceareoftenspreadbysexualcontact.
B. Scabies:aninfestationoftheskinbyitchmites.
1. Intenseitching,especiallyatnight.
2. Burrowsareseen,especiallybetweenngers,onthe
surfacesofwrists,andinaxillaryfolds.
3. Redness,swelling,andvesicularformationmaybe
noted.
Treatment
A. Pediculosis. 1. Permethrin1%liquid(Nix):effectiveagainstnits
andlicewithjustoneapplication;shampoohair
rst,leaveNixonhairfor10minutes,rinseoff;may
repeatin7days.
2. Pyrethrincompounds(e.g.,Rid)forpubicandhead
lice.
B. Scabies:Permethrin5%cream(Elimite).Creamis
appliedtotheskinfromheadtosolesoffeetandlefton
for8to14hours,thenwashedoff;onlyoneapplication
needed.
7/28/2019 Nclex-pn Chapter 19 Bwfinal
6/12
CHAPTER19 IteuetarSste 407
Home Care
A. Allfamilymembersandclosecontactsneedtobe
treatedforparasiticdisorders;licecansurviveup
to48hours;nitscanhatchin7-10dayswhenshedinthe
environment.
B. Beddingandclothingthatmayhaveliceornitsshould
bewashedordrycleaned;furnitureandrugsshouldbe vacuumedortreated.
C. Nursesshouldweargloveswhenexaminingscalpto
preventspreadtoothers.
D. Whenshampooinghair,useane-toothcombor
tweezerstoremoveremainingnits.
Viral Infections
A. Herpessimplexvirus(feverblister,coldsore):herpes
virustype1(HSV-1).
1. Painful,localreactionconsistingofvesicleswithan
erythematousbase;mostoftenappearsaroundthe
mouth. 2. Contagiousbydirectcontact;isrecurrent(lesions
appearinsameplace);thereisnoimmunity.
3. NottobeconfusedwithHSV-2,whichprimarily
occursbelowthewaist(genitalherpes).
4. ItispossiblefortheHSV-1tocausegenitallesions
andforHSV-2tocauseorallesions(seeSexually
TransmittedDiseasesinChapter17).
B. Herpeszoster(shingles).
1. Relatedtothechickenpoxvirus:varicella.
2. Contagioustoanyonewhohasnothadchickenpox
orwhomaybeimmunosuppressed.
3. Linearpatchesofvesicleswithanerythematousbase
arelocatedalongspinalandcranialnervetracts. 4. Oftenunilateralandappearsonthetrunk;however,
mayalsoappearontheface.
5. Pain,burning,andneuralgiaoccuratthesitebefore
outbreakofvesicles.
6. Oftenprecipitatedbythesamefactorsasherpes
simplexinfection.
C. Herpeticwhitlow:occursonngertipsandaroundnail
cuticles;oftenseeninmedicalpersonnel.
Treatment
A. Usuallysymptomatic;applicationofsoothingmoist
compresses.B. Analgesics;gabapentin(Neurontin)forpostherpetic
neuralgia.
C. Antiviralagents(seeAppendix19-1).
D. Zostervaccineisrecommendedforadultsover60years.
Home Care
A. Alleviatepainbyadministeringanalgesics.
B. Antihistaminesmaybeadministeredtocontrolthe
itching.
C. Usually,lesionshealwithoutcomplications;herpes
simplexusuallyhealswithoutscarring,whereasherpes
zostermaycausescarring.D. Ifhospitalized,establishcontactprecautionsforherpes
zoster.
mAlIgnAnTSKInnEoPlASmS
Malignant Melanoma
Data Collection
A. Riskfactors
1. ChronicUVexposurewithoutprotectionor
overexposuretoarticiallight(tanningbed).
2 Fairskin,genetic(rstdegreerelative).3. Hasthehighestmortalityrateofanyformofskincancer
a. Oftenappearsinpreexistingmolesintheskin.
b. Commonsitesincludebackandlegs(women);trunk
head,andneck(men).
c. Suddenorprogressivechangeorincreaseinsize,
color,orshapeofamole.
4.Symptoms(Box19-2).
TreatmentA. Surgical.
1. Excisionalsurgery;lasertreatment.
2. Cryosurgery.
3. Electrodesiccationandcurettage.
B. Medical. 1. Radiationtherapy.
2. Chemotherapyandbiologictherapy.
Home Care
A. Teachtheimportanceofavoidingunnecessaryexposure
tosunlight.
B. Applyprotectivesunscreenwhenoutside.
C. Teachthewarningsignsofcancer.
Melanomastendtohave:
A Asymmetry
B BorderIrregularity
C ColorVariegation
D Diametergreatthan6mm
EEvolvingorchanginginsomeway
BOX 19-2 MALIGNANT MELANOMA
7/28/2019 Nclex-pn Chapter 19 Bwfinal
7/12
408 CHAPTER19 IteuetarSste
Burns
A. Typesofburnsthermal,electrical,chemical,smoke
andinhalation.
B. Fluidshiftconsiderations.
1. Fluidshiftandedemaformationoccurwithin24to
48hoursafterburninjury.
2. Fluidmobilizationoccurswithinapproximately18to 36hoursafterburninju ry.
Data Collection
A. Criteriasuggestingpulmonarydamage.
1. Historyofburninjuryoccurringwithinaconnedarea.
2. Burnsaroundtheface,neckormouthorintheoral
mucosa.
B. Circulatorystatus.
1. Tachycardiaandhypotensionmayoccurearly.
2. Evaluateurineoutput.
C. Identifywhenclientatelast;checkgastrointestinal
function.D. Evaluateresponsetouidtherapy.
E. Evaluatecirculatorystatusoftheextremities.
NURSING PRIORITY: The client with burn
injury is often awake, mentally alert, and cooperative at
rst. The level of consciousness may change as respiratory
status changes or as the uid shift occurs, precipitating
hypovolemia. If the client is unconscious or confused,
assess him or her for the possibility of a head injury.
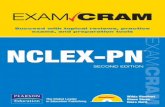
F. Determinetheseverityoftheburninjury(Box19-3and
Figure19-2). 1. Neckandfaceburnsmayleadtomechanical
occlusionoftheairwayduetoedema.
2. Circumferentialburns(burnssurroundinganentire
extremity)mayleadtoimpairedcirculationfrom
edemaformationandlackofelasticityoftheeschar,
leadingtocompartmentalsyndrome.
Supercialorrst-degreeburn:Areaisreddened
andblancheswithpressure;noedemapresent;area
isgenerallypainfultotouch. Partial-thicknessorsecond-degreeburn:Dermis
andepidermisareaffected;formationoflarge,
thick-walledblisters;underlyingskiniserythematous.
Full-thicknessorthirdandfourth-degreeburn:All
oftheskinisdestroyed;mayhavedamagetothe
subcutaneoustissueandmuscle;usuallyhasadry
appearance,maybewhiteorcharred;willrequire
skingraftingtocoverarea;underlyingstructures
(fascia,tendons,andbones)areseverelydamaged,
usuallyblackened.
BOX 19-3 DEPTH OF BURNS
3. Age.
a. Infantshaveanimmatureimmunesystemand
poorbodydefense.
b. Olderadultclientshealslowly;morelikely
tohavewoundinfectionproblemsand
pulmonarycomplications.
4. Presenceofotherhealthproblems:
a. Diabetesandperipheralvasculardiseasedelay
woundhealing.
b. Poornutr itionalstate.
c. Ch roniccondit ionsthatcompromiseimmune
system.
Treatment
A. Stabilizationofairway,breathing,andcirculation.
B. Iftheburnareaissmall,applycoldcompressesor
immerseinjuredareaincoolwatertodecreaseheat;ice
shouldnotbedirectlyappliedtotheburnarea.
C. Administertetanusinjection.
D. Fluidresuscitation;IVuids.
E. NPO;mayneedanasogastrictube.
F. Analgesicsaregivenintravenously;intramuscularly,
subcutaneously,orallyadministeredmedicationsmay
notabsorbeffectively.
G. Methodsofwoundcare(areaiscleanedanddebridedof
necroticburnedtissue).
1. Openmethod(exposure):Burniscoveredwitha
topicalantibioticcream,andnodressingisapplied.
2. Closedmethodofdressing:Finemeshisusedto
covertheburnedsurface;maybeimpregnatedwith
antibioticointmentorointmentmaybeapplied
beforethedressingisapplied.
3. Escharotomy:Procedureinvolvesexcisionthrough
theeschartoincreasecirculationtoanextremity
withcircumferentialbu rns.
a. Enzymaticdebriders:Collagenase,brinolysin,
andAccuZymemaybeused.
IgURE19-2 DereeBurbTissuelaer (From ZerwekhJ., Claborn, J. Memory Notebook of Nursing, Vol. 2, 2008, NursingEducation Consultants.)
7/28/2019 Nclex-pn Chapter 19 Bwfinal
8/12
7/28/2019 Nclex-pn Chapter 19 Bwfinal
9/12
410 CHAPTER19 IteuetarSste
1. Thenurseunderstandsthatpressureulcersaremost
commonlycausedbywhatproblem?
1 Musclesthatarenotbeingusedinpassiveexercises.
2 Poornutrition,resultingininadequateproteinin
take.
3 Irritationofabonyprominencethatiscoveredby
infectedskin.
4 Pressurecuttingoffbloodsupplytotheaffected
areaoftheskin.
2. Inreport,thenurseistoldtheclienthasastage1pres-
sureulcer.Whatwouldthenurseexpecttondon
assessmentofthearea?
1 Aareaoferythemathatdoesnotblanchwithdigital
pressure.
2 Amoistareawheretheskinhassloughed.
3 Awell-circumscribedareathathasacentercraterin
subcutaneoustissue.
4 Areddenedareaofirritationandscalyplaqueson theskin.
3. Aclienthasapressureulcerthathasnecrosisinthe
subcutaneousleveloftissue.Thereisunderminingof
thesurroundingtissue.Whatisthenursingcareforthis
stageofapressureulcer?
1 Carefullycleantheareawithhydrogenperoxide
andapplyadrydressing.
2 Gentlymassagetheareaaroundthenecrosisto
stimulatehealing.
3 Applyacleandressingandencourageanincreased
uidintake.
4 Keeppressureofftheareaandanticipateprocedure
fordebridement.4. Whichofthefollowingnursinginterventionswillassist
inreducingpressurepointsthatmayleadtopressure
ulcers?
Selectallthatapply:
1 Positiontheclientdirectlyonthetrochanterwhen
side-lying.
2 Avoidtheuseofdonutdevices.
3 Massagebonyprominences.
4 Elevatetheheadofthebedaslittleaspossible.
5 Whenside-lyingusethe30lateralinclinedposition.
6 Avoiduninterruptedsittinginanychairorwheel-
chair.
5. Whatwouldthenurseteachanolderadultclientregard- inghowtocareforherdry,itchyskin?
1 Useamoisturizeronalldryskinareas.
2 Wearclotheswith80%ormoreofcottonbers.
3 Showertwiceadaywithmildsoap.
4 Wearprotectivepadsondryskinareas.
6. Aclienthasathird-degreecircumferentialburnonhis
leftupperarm.Escharhasformedontheburnarea.
Whatismostimportantforthenursetoassess?
1 Evaluatearoundtheescharforpresenceofinfection.
2 Statusofcirculationinthelefthand.
3 Presenceofbilateralbreathsounds.
4 Statusofurinaryoutputandhydration.
7. Whatwillbeimportantforthenursetotelltheparents
ofachildwhohasaproblemwithheadlice?
1 Washthechildshairwithacoaltarbasedshampoo
andrinsethoroughly.
2 Thoroughlywashallofthechildsbeddingand
clothes.
3 Useananti-itchcream,butmakesuretheirritated
areasdonotgetinfected.
4 Useanantibioticointmentaftershampooingwith
Permethrin1%(Nix).
8. Anolderadultclientinalong-termcarefacilityhas
beendiagnosedwithherpeszoster.Whatisimportant
nursingmanagementforthisclient?
1 Dailyapplicationofanantifungalcreamtoaffected
areas.
2 Maintainclientonstandardprecautions.
3 Applywarmsoakstoareaofvesicles. 4 Assisttheclienttodealwiththeneuralgia.
9. Aclienthasbeendiagnosedwithbasalcellcarcinoma
andtheareahasbeenexcised.Whatwillbeimportant
forthenursetoexplaintothispatient?
1 Pain,bu rning,andneuralgiamayoccurinthe
affectedarea.
2 Itisveryimportanttousesunscreenanytimeyou
gooutside.
3 Useanant iinammatoryointmenttopreventa
secondaryinfectioninthearea.
4 Oncetheareahasbeenexcised,thereshouldbeno
furtherproblems.
10. Aclienthasbeendiagnosedwithpsoriasis.Whatwould beimportantforthenursetodiscusswiththisclient?
1 Theuseoftopicalsteroidsandultravioletlightwill
helptocontroltheproblem.
2 Theareashouldbecleansed,scalesremoved,and
thentheantibioticointmentapplied.
3 Warm,moistpackscanbeappliedtotheareato
assistinthedebridingofthelesion.
4 Theproblemusuallygoesawaywithtreatment,but
theareamayremaintendertothetouch.
11. Achildhasscabies.Whatshouldthenurseexplainto
themother?
1 Carefullyremovenitsfromareaandthenwashwith
alcohol. 2 SpreadElimitecreamalloverbody,leaveonfor8
to12hours,andthenwashoff.
3 Applymoistsoaksofantifungalmedicationon
burrowedskinlesionsfor1to2hours,thenrinse.
4 Encourageexposuretosunlighttodrytheareaand
applyantibioticointment.
Answers and rationales to these questions are in the section a
the end of the book titled Chapter Study Questions: Answers
and Rationales.
StudQuestis:IteuetarSste
7/28/2019 Nclex-pn Chapter 19 Bwfinal
10/12
CHAPTER19 IteuetarSste 411
Appendix 19-1 SKIN DIAGNOSTIC STUDIES
SkitestiPurpose:conrmsensitivitytoaspecicallergenbyplacingantigenonordirectlybelowskin(intradermal)tocheckfor
presenceofantibodies.
1. Twomethodsallergenappliedtoarmsorback.
Cutaneousscratchtest(alsoknownasatineorprick test)
Intracutaneousinjection-highriskofsevereallergicreaction
Patchtestusedtodetermineifclientisallergictotestingmaterial(smallamountappliedonback)returnsin48hours
forevaluation.
2.Interpretingresults.
Immediatereaction:appearswithinminutesaftertheinjection;markedbyerythemaandawheal;denotesapositive
reaction.
Positivereaction:localwheal-and-areresponseoccurs.
Negativereaction:inconclusive;mayindicatethatantibodieshavenotformedyetorthatantigenwasdepositedtoo
deeplyinskin(notanintradermalinjection);mayalsoindicateimmunosuppression.
3. Complications:rangefromminoritchingtoanaphylaxis(seeChapter5).
NURSINGPRIORITY: Never leave client alone during skin testing due to risk of anaphylaxis. If a severe reaction
occurs, anticipate antiiammatory topical cream applied to skin site (scratch test) or a tourniquet applied to the arm
(intracutaneous test) and possible epinephrine injection.
BipsTypes:punch,excisional,incisional,shave
1. Verifyifinformedconsentisneeded.
2. Applydressingandgivepostprocedureinstructionswatchforbleeding.
SkiCuturePurpose:identifyfungal,bacterial,andviralorganisms.
1. Scraporswabaffectedarea;labelspecimenandsendtolab.
7/28/2019 Nclex-pn Chapter 19 Bwfinal
11/12
412 CHAPTER19 IteuetarSste
Appendix 19-2 MEDICATIONS USED IN SKIN DISORDERS
gEnERAlnURSIngImPlICATIonS Topicalmedicationsareusedprimarilyforlocaleffectswhensystemicabsorptionisundesirable.
Fortopicalapplication:
Applyaftershowerorbathforbestabsorption,becauseskinishydrated.
Applysmallamountofmedicationandrubinwell.
medicatis SideEects nursiIpicatis
AnTIUngAl:Ihibitsrdaaesuaceebrae,eitherateripereabiitrdisrupticeitsis.
Clotrimazole(Lotrimin):topical
Nystatin(Mycolog):topical
Ketoconazole(Nizoral):PO,topical
Griseofulvin(Fulvicin):PO
Nausea,vomiting,abdominalpain.
Hypersensitivityreaction:rash,urticaria,
pruritus.
Hepatotoxicity.
Gynecomastia(ketoconazole).
1. Monitorhepaticfunction(whenoral
medicationisgiven).
2. Avoidalcoholbecauseofpotentialliver
problems.
3. Checkforlocalburning,irritation,or
itchingwithtopicalapplication.
4. Prolongedtherapy(weeksormonths)
isusuallynecessary,especiallywith
griseofulvin(Fulvicin).
5. Takegriseofulvin(Fulvicin)withfoods
highinfat(e.g.,milk,icecream)todecreaseGIupsetandassistin
absorption.
6. Uses:tineainfections,fungalinfections,
candidiasis,diaperdermatitis.
AnTIVIRAl:Reducesvirasheddi,pai,adtiethea.
Acyclovir(Zovirax):topical,PO,IV.
Penciclovir(Denavir):topical
Vidarabine(Ara-A, Vir-A):IV,ophthalmic
IV:phlebitis,rash,hives.
PO:nausea,vomiting.
Topical:burning,stinging,pruritus.
Anorexia,nausea,vomiting.
Ophthalmic:burning,itching.
1. Applytopicallytoaffectedareasixtimes
perday.
2. Avoidauto-inoculation;washhands
frequently;applywithglovedhand.
3. Avoidsexualintercoursewhilegenital
lesionsarepresent.
4. Drinkadequateuids.5. InfuseIVpreparationsover1hour;use
aninfusionpumpforaccuratedelivery.
6. Uses:herpesinfections.
AnTIInlAmmAToRy:Decreasestheifaatrrespse.
Triamcinoloneacetonide( Aristocort):topical Skinthinning,supercialdilatedblood
vessels(telangiectasis),acne-likeeruptions,
adrenalsuppression.
1. Triamcinoloneandhydrocortisone
creamscomeinvariousstrengthsand
potency.Watchthepercentstrength.
2. Applied2-3timesaday.
3. Useanocclusivedressingonlyif
ordered.
4. Encourageclienttousetheleastamount
possibleandfortheshortestperiodof
time.
ImmUnoSUPPRESAnT:SuppressesTcesaddecreasesreaeaseifaatrediatrs;aterativetuccrticids
Pimecrolimuscream(Elidel):topical
Tacrolimusointment(Protopic):topical
Erythema,pruritus
Burningsensatonatapplicationsite
1.Teachclientstousesunscreen,asmakes
clientsensitizedtoUVlight.
2.Longtermeffectscanleadtoskincancer
andlymphoma.
GI,Gastrointestinal;IV,intravenously;PO,bymouth(orally).
7/28/2019 Nclex-pn Chapter 19 Bwfinal
12/12
CHAPTER19 IteuetarSste 413
Appendix 19-3 TOPICAL ANTIBIOTICS FOR BURN TREATMENT
medicatis SideEects nursiIpicatis
ToPICAlAnTIBIoTICS:Prevetadtreatiectiatthebursite.
Silversulfadiazine(Silvadene) Hypersensitivity:rash,itching,orburning
sensationinunburnedskin
1. Liberalamountsarespreadtopically
withasterile,glovedhandoron
impregnatedgauzerollsovertheburned
surface.
2. IfdiscolorationoccursintheSilvadene
cream,donotuse.
3. Athinlayerofcreamisspreadevenly
overtheentireburnsurfacearea;reap-
plicationisdoneevery12hours.
4. Clientshouldbebathedortubbeddaily
toaidindebridement.
5. Medicationdoesnotpenetrateeschar.
6. Forclientswithextensiveburns,monitor
urineoutputandrenalfunction;asigni-
cantamountofsulfamaybeabsorbed.
Mafenideacetate(Sulfamylon 10%) Pain,burning,orstingingatapplicationsites;excessivelossofbodywater;excoriationof
newtissue;maybesystemicallyabsorbed
andcausemetabolicacidosis.
1. Bacteriostaticmedicationdiffusesrapidlythroughburnedskinandescharandis
effectiveagainstbacteriaunderthe
eschar.
2. Dressingsarenotrequiredbutarefre-
quentlyused.Athinlayerofcreamis
spreadevenlyovertheentireburn
surface.
3. Monitorrenalfunctionandpossibleaci-
dosis,becausemedicationisrapidly
absorbedfromtheburnsurfaceand
eliminatedviathekidneys.
4. Painoccursonapplication.
5. Watchforhyperventilation,asacompen-
satorymechanismwhenacidosisoccurs.
Top Related