





Languages
Pages
Legal


Nasal airway obstruction and its management
Dr. T. Balasubramanian
6/3/2010 Otolaryngology online drtbalu

Nasal air way obstruction and its management
Introduction:
Nasal obstruction is an important symptom of many underlying disorders, and is the
most common cause for visiting an otolaryngologist. It should be borne in mind that
nasal obstruction is a symptom and not a diagnosis. These patients hence should be
evaluated for both subjective / objective nasal obstruction. Nasal patency these days
can be evaluated objectively based on the anatomy of the nasal cavity and physiology
of nasal air flow which can be studied using a Rhinomanometer.
Subjective feeling of nasal block could be due to the following factors:
1. Sensitivity of pressure receptors in the nose
2. Sensitivity of thermal receptors in the nose
3. Sensitivity of pain receptors in the nose
4. Presence of excessive secretions in the nose
The cause for nasal obstruction is considered to be multifactorial which includes both
subjective and objective causes.
Anatomic causes of nasal block:
Nasal valve area problems: Nasal valve area is considered to be the narrowest
portion of the human airway. Anatomically it has two components i.e. External and
internal nasal valves. The anatomy of internal nasal valve was first described by
Mink in 1903.
Boundaries of internal nasal valve include:
1. Dorsal portion of nasal septum medially
2. Inner caudal edge of upper lateral cartilage laterally
3. Anterior head of inferior turbinate posteriorly
The internal nasal valve area is supposedly the narrowest portion of human airway
has a cross sectional area of approximately 40 – 60 mm2. This area accounts for
nearly 2/3 of the whole airway resistance. Hence collapse / stenosis of this area
accounts for one of the commoner causes of nasal block.
External nasal valve is also known as nasal vestibule. It is bounded by the caudal
edge of the lateral crus of the lower lateral cartilage, fibrofatty tissue over the ala and
the membranous septum.

Diagram showing the nasal valve areas
The nasal vestibule should be considered to be the first component of the nasal
resistance mechanism. If the nasal airflow rate exceeds 30 litres / minute, the
vestibule of nose collapses causing a reduction in the rate of nasal airflow. This
collapse of ala increases the nasal resistance.
On inspiration, the increased velocity of air flowing through the nasal valve area will
cause a drastic decrease in the introluminal pressure causing a vacuum effect on the
upper lateral cartilages. This inward pull causes collapse of upper lateral cartilage
(Bernoulli's principle). Total collapse of the internal nasal valve area duing this
scenario is prevented only by the reselience of the upper and lower lateral cartilages.
Collapse of external nasal valve area (alar area) is by contraction of dilator nari
muscles during inspiration. During expiration the positive pressure prevailing inside
the nasal cavity keeps the nasal valve area open.
Causes of nasal obstruction:
1. Previous trauma / rhinoplasty surgical procedure are the common causes of
nasal obstruction due to weakening of nasal valves
2. If there is associated nasal septal deviation then nasal obstruction becomes
exponentially increased
3. Mucociliary clearance mechanism in patients with deviated nasal septum is
slowed considerably when compared to that of normal individuals. Stagnant
secretions inside the nasal cavity may aggravate nasal obstruction

4. Penumatization of middle turbinate (Concha bullosa) an anatomical variant can
cause significant amount of obstruction in the middle meatal area. Massive concha
may cause middle meatal nasal obstructive syndrome leading on to symptoms like
headache, nasal block and anosmia. Commonly majority of these patients also have
deviated nasal septum which may aggravate nasal block.
5. Neuromuscular causes like facial palsy and aging. Facial palsy may cause
paralysis of dilator naris leading on to nasal obstruction. Aging on the other hand
could weaken the fibroareolar tissues present in the lateral nasal wall leading to
collapse of nasal valve area leading on to nasal obstruction.
6. Sinonasal inflammatory diseases. Commonly allergic rhinitis causes
congestion and enlargement of nasal turbiantes and mucosa causing nasal bock.
These patients classically have nasal obstruction on lying down.
7. Drug induced iatrogenic nasal block (Rhinitis medicamentosa). Rebound nasal
congestion is very common in these patients. These patients also have loss of ciliated
columnar cells and increase in capillary permeability causing interstitial oedema.
During early phases of rhinitis medicamentosa this oedema is reversible. If it
continues for a period of more than 3 months it gradually becomes irreversible
leading to difficult situations to manage. Systemic medical therapy like reserpine
(antihypertensive), beta blockers, antidepressents can cause nasal block due to their
actions on the autonomic nervous system.
8. Hypothyroidism may lead to nasal congestion and block due to unknown
reason. Supplements of thyroxine will mitigate these symptoms.
9. Pregancy rhinitis – (Rhinopathia gravidorum) seen commonly during the first
trimester of pregnancy can cause nasal block due to unknown mechanism.
Generalized fluid retention during pregnancy and exposure of nasal mucosa to
persistently elevated levels of oestrogen leads to persistent intertitial oedema. It has
also been suggested that elevated levels of oestrogen and progesterone during
pregnancy may cause rhinits by causing a shift in the level of neurotransmitters like
substance P and nitirc oxide.
10. Trauma may cause nasal block due to the following factors: tissue oedema
causing physical blockage to airflow, secondary sinusitis, and impaired sensation to
air flow due to damage sustained by nasal receptors.
11. Neoplams involving the nasal cavity can cause nasal block. Nasal block in
these patients may be associated with other non specific symptoms like epistaxis and
anosmia prompting the patient to seek medical attention.
Patients with fixed anatomical nasal obstruction may experience intermittent
symptoms secondary to nasal cycle and other autonomic phenomenon. By and large
normal nasal cycle is usually unnoticed by the patient. When there is associated
anatomical fixed nasal obstruction then the patient becomes aware of the presence of
nasal cycle.
Factors controlling nasal resistance:

In normal healthy subjects the nasal airway resistance is determined by the degree of engorgement
of venous erectile tissue, as well as the accessory muscles of respiration which keep the nasal
airway patent. The venous erectile tissue of nasal mucosa has dense adrenergic innervation which
when stimulated cause intense vasoconstriction thereby decreasing the nasal airway resistance.
Normally there is a continuous sympathetic vasoconstrictor tone to the nasal erectile tissue keeping
the nasal airway resistance under check. Reduction in this sympathetic tone increases the nasal
airway resistance. The parasympathetic tone in the nose controls nasal secretion, but has little role
in nasal resistance.
Role of complete history / clinical examination in diagnosing the cause for nasal
obstruction:
It is very important to elicit a complete history from the patient. This will invariably
point towards the correct cause for nasal block. These patients must be diligently
quizzed for prolonged use of drugs, nasal drops which could cause iatrogenic nasal
obstruction.
History of previous surgeries in the nose which includes cosmetic surgery should be
sought. This can invariably point towards the possible cause of block.
Presence of midface deformities (congenital / due to injuries) should also carefully

sought for. History of mouth breathing and halitosis will invariably confirm the
problem of nasal block.
Nasal cavities should be examined for evidence of sinusitis. Any discharge from the
nasal cavity indicates infection. Adenoid hypertrophy should be ruled out in young
children with nasal obstruction as it is the commonest cause in them.
Assessment of facial nerve function:
Facial nerve integrity should be assessed in these patients. Facial nerve paralysis will
hamper the splinting muscles of the ala of the nose causing collapse of the airway on
inspiration.
Examination of the nasal cavity pertaining to airflow dynamics:
Nasal cavity should be examined with specific focus on the probable sites of nasal
resistance. Evaluation should begin with specific focus on external support structures
followed by a detailed assessment of internal support sturctures. Nasal valve area
should be carefully assessed by performing Cottle's test. In this test the cheek of the
patient is pulled outwards and upwards. If it affords relief from nasal block then
obstruction should be considered to be due to anamalous / abnormal nasal valve area.
False negative Cottle's test is possible when the presence of synechiae in the nasal
valve area prevents opening up of this zone when this test is being performed.
As a first step the internal nasal valve area should be examined endonasally as this
area contributes the maximum to the airway resistance. This area should be
examined just by lifting the tip of the nose. Introduction of nasal speculum would
distort this area and hence should be avoided.

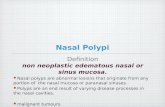
CT scan showing a large concha occupying the whole nasal cavity
Malignant nasal mass seen occupying the nose

CT scan showing hypertrophied nasal mucosa on both sides due to allergy
A simple technique which can be used as an alternative to Cottle's test is using a nasal
speculum to lateralize the upper lateral cartilage from the inside of the nose and the
patient is asked whether there is improvement in symptoms. This test has the added
advantage of direct observation of the nasal valve area as it is widened.
Diagnostic nasal endoscopy:
This is the most efficient way of completely examining the interiors of the nasal
cavity. 30 degrees 4 mm nasal endoscope is preferred for this purpose because of its
wide viewing angle. Ideally speaking the nasal endoscopic examination should be
performed before and after nasal decongestion. If nasal obstruction improves on
decongestion alone then nasal obstruction could be due to mucosal inflammatory
disorder affecting the inferior turbinates. If there is no response to nasal decongestion
then the probable cause for nasal obstruction could be:
1. Nasal valve area obstruction
2. Septal deviation
3. Bony hypertrophy of inferior turbinate
4. Rhinitis medicamentosa
During diagnostic nasal endoscopy the presence of anatomical variations should also
be observed. Common anatomical variations that could cause nasal block include:

1. Septal deviation
2. Presence of concha bullosa
3. Intranasal masses
4. Presence of adenoid enlargement
Diagnostic alogrithm for nasal block
Nasal endoscopy is an useful tool in assessing subtle nasal mucosal inflammatory
changes like mucosal nodularity, friable mucosa and synechiae.
Role of radiology in assessing patients with nasal block:
CT scan is helpful in evaluating bony structural abnormalities like deviated nasal

septum, choanal atresia, concha bullosa, inferior turbinate hypertrophy, F.B., rhinolith
etc.
MRI because of its excellent soft tissue imaging capacity is very useful in identifying
lesions like meningocele, encephalocele etc.
Objective evaluation of nasal block:
The following tests would help us to objectively evaluate nasal block.
1. Hygrometry: This is one of the first methods to objectively assess nasal airway
patency. This technique was first described by Zwaardemaker in 1884. This
procedure is performed by asking the patient to breathe on a mirror. A comparison is
made between the diameter of the fog produced by each nasal airway.
2. Hum test: This test was first performed by Spiess in 1902. He assessed the
nasal airway by the change in timbre of the sound caused due to nasal block. He
performed the test after decongesting one nose, blocking the decongested nose and
asking the patient to hum a tune. The change in timbre caused due to block in the
non decongested nose is appreciated.
3. Peak nasal inspiratory flow
4. Acoustic rhinometry
5. Rhinomanometry
Peak nasal inspiratory flow:
This is a very simple, cost effective, reliable and objective measure of nasal airflow
obstruction. In 1980 Youlten developed a peak nasal inspiratory flow meter which
was non invasive, portable, simple to use and economical to own. The peak nasal
inspiratory flow rate is determined by two factors i.e. Nasal obstruction and the
maximum negative pressure generated by the lower airway. Hence changes in
inspiratory effort or lower airway resistance will alter the peak nasal inspiratory air
flow independent of nasal obstruction. To overcome this problem Taylor suggested to
assess Blockage index.
Blockage index = Peak oral flow – Peak nasal flow / Peak oral flow. According to
Taylor Blockage index correlated well with Rhinometry values.

Figure showing equipment to record Peak nasal inspiratory flow
Acoustic Rhinometry:
This was first introduced by Hilberg in 1989. This technology was originally used
for oil exploration. It was only in 1970's this technology was started to be used for
medical diagnosis. This is the most common method used to assess the nasal cavity
air way geometry. This can be used for studying:
1. Anatomical variations of nasal cavity
2. Post surgical changes inside the nasal cavity
3. Effect of drugs on nasal resistance
4. Assessing the changes in the mucovascular component of the nasal erectile
tissues.
Components of acoustic rhinomanometer:
1. Sound source
2. Wave tube
3. Microphone
4. Filter
5. Amplifier
6. Digital converter
7. Computer
Sound waves generated by acoustic rhinomanometer is transmitted through the nasal
cavity, these sound waves get reflected back from the nasal passages and is recorded
by the microphone placed at the entrance of the nasal cavity. These sound waves are
converted to digital signals and a computer recording is made which is known as the

“Rhinogram”. Rhinogram usually provides a two dimensional assessment of the
nasal airway. The cross sectional area of nasal cavity varies at different points from
the nasal rim and these variations are detected by changes in acoustic impedance.
Each notch in a rhinogram represents a constriction inside the nasal cavity.
The first notch represents the nasal valve area. This is infact the minimal cross
sectional area in the normal nasal cavity. The second notch represents the anterior
portion of the inferior / middle turbinate. The third notch represents the area of the
middle and posterior end of middle turbinate. Each notch indicates the site of nasal
airway resistance and is hence a very sensitive indicator for identifying the area
causing nasal block.
Figure showing the Rhinogram. Note the three notches as described above

Figure showing acoustic rhinomanometer

CT volumetry: This imaging modality is very senstitive in measuring nasal cavity
volumes. This imaging modality is highly accurate in measuring the volume of
anterior nasal cavity but its accuracy reduces while measuring the volume of
posterior nasal cavities.
Rhinomanometry:
This investigation involves the functional assessment of airflow inside the nasal
cavity. It involves measurement of transnasal pressure and airflow. Resistance from
each nasal cavity can be compared.
There are two types of rhinomanometry, active and passive rhinomanometry. Active
rhinomanometry involves the generation of nasal airflow and pressure with normal
breathing. Passive rhinomanometry involves the generation of nasal airflow and
pressure from an external source, such as fan or pump which drives air through the
nose.
Active rhinomanometry: can be divided into anterior and posterior methods
according to the siting of the sensor tube. In active anterior rhinomanometry, the
pressure sensing tube is taped to one nasal passage. This method measures resistance
of one nasal cavity at a time and must be repeated on the other side. The total air flow
through the nose is measured with the help of the sensor tube. In active posterior
rhinomanometry, the pressure sensing tube is held within the mouth and it detects the
post nasal pressure. Air flow through each nose can be measured by taping the
opposite nose.
While performing rhinomanometry pressure in the post nasal space can be measured
in three ways:
1. Anterior rhinomanometry involves palcement of a tranducer in the nostril not
being tested. This concept was first introduced by Coutade in 1902. Because there is
no airflow in the non test nose, the pressure at the anterior end of this nostril is
roughly equal to the pressure at the post nasal space. In this method transnasal
pressure differences and nasal airflow can be recorded at the same time. Major draw
back of this method of recording is that it cannot be relied in patients with septal
perforation.
2. Another method of measuring nasal pressure is by peroral method. This
method was popularized by Spiess in 1899. In this method the transducer is placed in

the posterior portion of oropharynx through the mouth. This method accurately
assesses the contribution of enlarged adenoid tissue to the nasal block. The major
problem with this method is that it is poorly tolerated.
3. The third method of measurement of nasal airway is by placing the sensor in
the postnasal space. This is again not very well tolerated by the patient.
Precautions taken while performing rhinomanometry:
a. The use of face mask is desirable than a nasal cannula. The face mask should form
a soft air tight seal and must not effect pull on the cheek.
b. Calibration of the equipment must be performed regularly.
c. Series of readings must be taken as a single reading is unreliable.
Nasometry:
During speech sound is transmitted through both the oral and nasal cavities. Nasal
obstruction causes a reduction in the amount of sound transmitted through the nose.
By measuring the nasal components of speech the patency of the nasal airway can be
assessed. This is known as nasalance. It is the ratio of sound energy from the nasal
and oral passages and can be measured by placing two microphones one over the
nose and the other over the mouth. Infact the measure of nasalance has been proposed
as a useful method of selecting children for adenoidectomy. It is also useful in
measuring the nasal airway patency.
Odisoft rhino:
This new technique converts the frequency of sound generated by airflow into cross
sectional area measurements. This technology was based on the premise that the
sound generated by airflow in the nose has a higher frequency depending on the
turbulence created. This technique was first developed by Serene. The equipment
has a microphone, nasal probe, sound card and a computer. The nasal probe is
connected to a microphone and is placed about 1 cm from the nostril of the patient.
The sound created by breathing is measured by the probe.

Figure showing areas of nasal cavity contributing to normal nasal resistance
Management:
Nasal obstruction due to mucosal congestion can be managed medically by topical / systemic nasal
decongestants. Treatment of acute infections with antibiotics should take precedence over nasal
decongestants.
To decide whether medical / surgical management is preferred mucosal congestion index should be
assessed.
Nasal mucosal congestion is an important determinant in deciding whether the patient needs
medical / surgical therapy. It goes without saying that if the nasal mucosa is thickened due to
mucosal oedema than it would respond better to nasal decongestants, while if the thickening is due
to underlying submucosal fibrosis then it doesn't respond to decongestants and needs to be
surgically removed to improve nasal airway patency. Nasal mucosal compliance cannot be
estimated by CT scans alone.
It has been demonstrated that tissue remodelling which is the repair response of nasal mucosa to
insults is characterised by decrease in vascular density, and an increase in fibrosis causing the nasal
mucosa to thicken irreversibly. This thickened mucosa reduces drug permeability through osmosis
causing a reduction in the effectiveness of the drug.

This measurement helps in identifying mucosal oedema from mucosal thickening due to fibrosis
involving submucosa. This can be measured by performing acoustic rhinomanometry before and
after decongesting the nose with epinephrine. If the nasal mucosal congestion index is large then
medical management is preferred and if the index is small then surgery should be resorted to in the
management of chronic rhinosinusitis. For sake of objectivity congestion index of the nasal mucosa
can be classified as normal, mild, moderate, severe and very severe.
Surgical management of nasal obstruction:
1. Septal correction – if nasal block is attributed to septal deviation / spurs
2. Anatomical abnormalities like concha bullosa should also be corrected surgically
3. Obstruction to nasal valve area as prooved by Cottle's test should be managed surgically.
Procedure:
This procedure can be performed under local anesthesia. Nasal cavity is first packed with ribbon
gauze dipped in 4% xylocaine with 1 in 100,000 units adrenaline. Xylocaine in 1% concentration
mixed with 1 in 100,000 units adrenaline is infiltrated over the prominence formed by the caudal
portion of the upper lateral cartilage. Parallel incisions are made on either side of the caudal portion
of the upper lateral cartilage. The caudal portion of the upper lateral cartilage is exposed after
removing a strip of mucosa with the underlying fibrous tissue. A 2 mm cuff of mucosa along with
overlying fibrous tissue is also removed to prevent redundant tissue formation. About 1-2 mm of the
terminal portion of the upper lateral cartilage should be resected and removed. The wound is closed
with absorbable suture like catgut. This procedure is safe to perform bilaterally also if necessary.
Diagram illustrating surgery in the nasal valve area
Top Related