






Languages
Pages
Legal


Morgen Bernius, MDNCEMS ConferenceFebruary 24, 2007
The Pediatric Patient

Rule #1: Everyone Loves the Pediatric Patient


Pediatrics in EMS
•
Approximately 10% of all EMS treatment is for children younger than 14 years of age
#1
#2



•
The mnemonic nightmare…
Difficulties in Assessment

•
PEPP: Pediatric Education for Prehospital Providers
•
PAT: Pediatric Assessment Triangle (appearance, work of breathing, circulation)
•
PALS: Pediatric Advanced Life Support•
ABCDE: Airway, Breathing, Circulation, Disability, Exposure
•
AVPU: Alert, Responsive to Verbal/Painful stimuli, Unresponsive
•
SAMPLE: Signs/Symptoms, Allergies, Medications, Past medical hx, Last meal, Events leading up to illness/injury
Difficulties in Assessment

They’re just little misshapen adults

The Pediatric Patient
•
General Assessment•
Airway/Breathing
•
Circulation•
Pediatric Pearls

General Assessment
•
Vital Signs–
Respiratory Rate and Quality
–
Pulse Rate and Quality–
Blood Pressure
–
Capillary Refill–
Pulse Oximetry
–
WEIGHT
General Pediatric Assessment

•
Depends on…–
Age
–
Size–
Development
–
Chronic conditions
What is NORMAL?


•
USE THE PARENTS!!•
Ask about:–
medical problems
–
normal assessment findings–
medical devices
–
Emergency Health Information Form•
If unavailable, base assessment on normal VS for age
What is NORMAL?

What is NORMAL?

Airway
These are EVERYTHING in the pediatric patient!
Airway/Breathing

•
Most pediatric arrests are of respiratory origin•
Once respiratory arrest progresses to pulseless cardiac arrest, outcome is
poor
Airway/Breathing
80%
10%
10%
RespShockCardiac

Age Distribution of Arrests
05
10152025303540
<7m
o 1 3 5 7 9 11 13 15
# Arrests
•
Occiput•
Airway size
•
Nose•
Tongue
•
Larynx•
Vocal Cords
•
Epiglottis•
Physiology
Anatomic and Physiologic Differences…and the
Consequences

•
The infant has a large occiput•
“sniffing position”
ineffective in
patients < 2yo
Anatomy: Occiput size

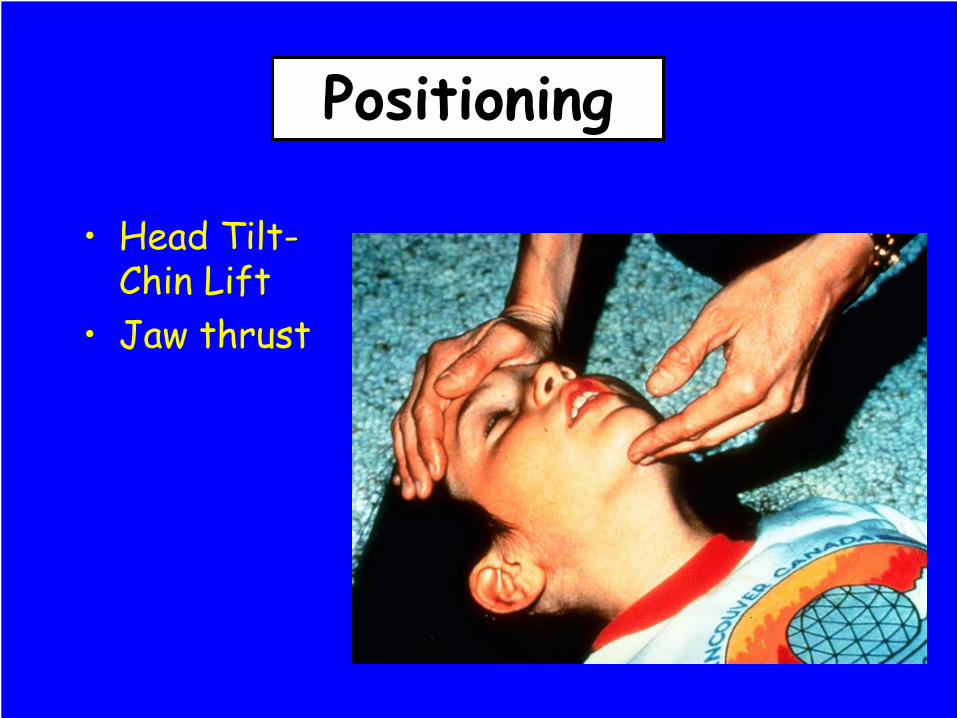
Positioning
•
Head Tilt- Chin Lift
•
Jaw thrust
Positioning

•
“Sniffing position”
in children >2years of age
Positioning

•
Shoulder elevation in children <2yo
Positioning

•
Shoulder elevation in children <2yo
Positioning

•
Shoulder elevation in children <2yo
Positioning

•
Difference #1: It’s SMALLER!
Anatomy: Airway Size

•
Manipulation and visualization•
Peripheral airway contribution to total resistance:–
Adults: 20%
–
Children: 50%
Anatomy: Airway Size

Anatomy: Airway Size
••
PoiseuillePoiseuille’’ss
Law: if the radius is Law: if the radius is halvedhalved, resistance increases , resistance increases 1616--
fold fold (with laminar flow)(with laminar flow)
R =R =8 n l8 n l
ΠΠ
rr44

•
The nose is responsible for 50% of airway resistance at all ages
•
In the infant, blockage of the nose = respiratory distress
Anatomy: Nose

•
The infant’s tongue is larger
relative to the oropharynx
•
Loss of tone with sleep, sedation, CNS dysfunction
•
Frequent cause of upper airway obstruction
•
May be difficult to control with the laryngoscope blade
Anatomy: Tongue
•
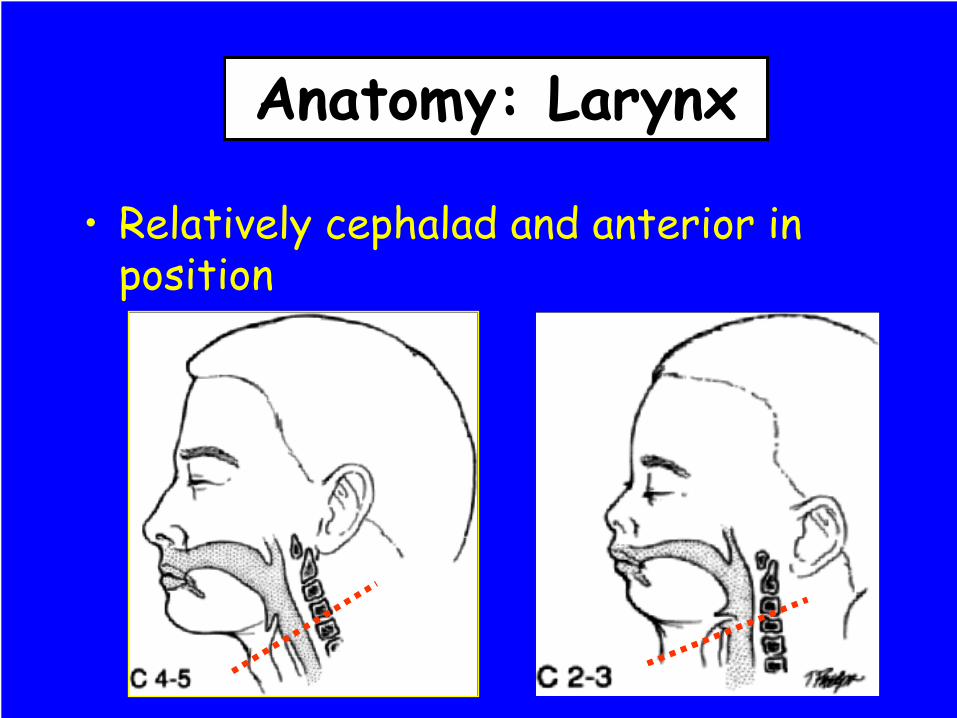
Relatively cephalad
and anterior in position
Anatomy: Larynx

•
More acute angle between the base of the tongue and glottic
opening
•
Straight blade more useful to create a direct visual
plane•
Positioning
Anatomy: Larynx

•
Narrowest portion of the airway:–
Adults: glottic
inlet
–
Children <10yo: cricoid
cartilage•
Funnel vs
cylinder shape
Anatomy: Larynx

•
Endotracheal tube size selection
•
Through the cords ≠
home-free•
Cuffed vs
uncuffed
Anatomy: Larynx

•
Vocal cords slanted anteriorly vs
perpendicular to trachea
•
Affects visualization•
Can make passage of ETT more difficult
Anatomy: Vocal Cords
•
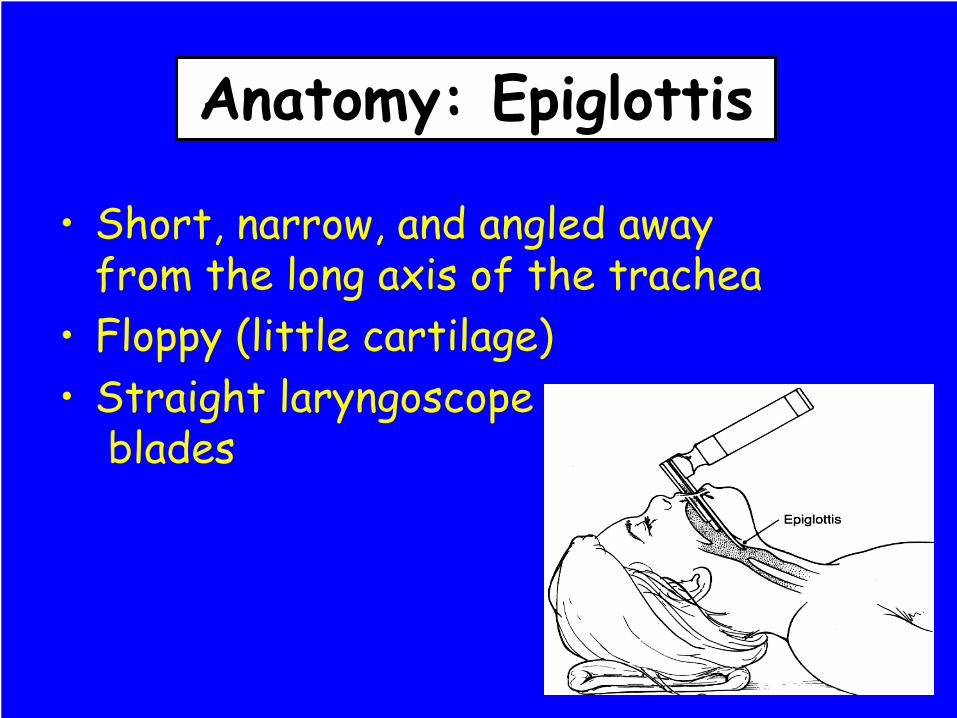
Short, narrow, and angled away from the long axis of the trachea
•
Floppy (little cartilage)•
Straight laryngoscope
blades
Anatomy: Epiglottis
Breathing

•
High metabolic rate and oxygen demand
•
O2
consumption:–
infants 6-8 mL/kg/min
–
adults 3-4 mL/kg/min•
Hypoxemia develops more rapidly in presence of apnea or inadequate alveolar ventilation
Breathing

•
Weak intercostal muscles, cartilage
•
Tidal volume dependent
on movement of diaphragm
•
Little reserve if movement of
diaphragm is impeded
Breathing

•
General Principles•
Positioning
•
Bag-Valve-Mask ventilation•
Airway Adjuncts
•
Endotracheal intubation
Assisting Ventilation

•
Anticipate and Recognize•
Prepare
•
Oxygen and Humidification•
Position of comfort
•
Lessen anxiety•
Be aggressive with secretions
•
Start simple…unobstruct
the airway
General Principles

Signs of Respiratory Distress
RetractionsRetractionsAccessory muscle useAccessory muscle useWheezingWheezingSweatingSweatingProlonged expirationProlonged expirationPulsusPulsus
paradoxusparadoxus
CyanosisCyanosis
TachypneaTachycardiaGrunting StridorHead bobbingFlaringInability to lie downAgitation

Signs of Respiratory Failure
•
Reduced air entry•
Severe work
•
Cyanosis despite O2
•
Irregular breathing / apnea•
Altered Consciousness
•
Diaphoresis

•
Mask: bridge of nose to cleft of chin, as small as possible
•
Infants and toddlers: jaw supported with base of the middle or ring finger
•
Older children: fingertips of 3rd, 4th, and 5th
fingers
on ramus
of mandible
Bag-Valve-Mask Ventilation

•
May need two providers to get a good seal
Bag-Valve-Mask Ventilation

•
Don’t forget the Sellick
maneuver!
Bag-Valve-Mask Ventilation

•
Oropharyngeal
airway–
holds tongue and soft hypopharyngeal
structures away from posterior pharyngeal wall
–
unconscious patients only–
4-10cm length
•
Estimate length: corner of mouth to angle of jaw
Airway Adjuncts

Airway Adjuncts

Airway Adjuncts

Airway Adjuncts

Airway Adjuncts

Airway Adjuncts
Just right!!

Airway Adjuncts
Insertion technique:

Airway Adjuncts
•
Nasopharyngeal Airway:•
12F (3mm ETT) to 36F
•
Suction•
Contraindications
Tip of nose to tragus
•
Isolates airway•
Reduces potential for aspiration
•
Allows control of inspiratory time and peak inspiratory pressures
•
Allows delivery of PEEP
Endotracheal Intubation

•
Inadequate CNS control of ventilation•
Functional or anatomic airway obstruction
•
Excessive work of breathing•
Need for high peak inspiratory pressures or PEEP to maintain effective alveolar gas exchange
•
Need for mechanical ventilatory
support•
Inability to protect airway
Endotracheal Intubation: Indications

•
SOAP ME•
Suction
•
Oxygen•
Airway equipment (check it!)
•
Pharmacologic agents•
Monitor, Mechanical
•
Equipment
Endotracheal Intubation: Preparation

•
ETT:–
Uncuffed in children <8yo
–
Cuffed in children >8yo–
Size: Use your CODE CARD!
Endotracheal Intubation: Equipment
ETT size =Age (yrs) + 16
4

•
ETT:
Endotracheal Intubation: Equipment
ETT size =Age (yrs)
4 + 4

•
ETT:–
Have other sizes available!
–
Rigid stylet–
Depth of insertion: 3 x internal diameter
(5.0 ETT inserted 15cm)
Endotracheal Intubation: Equipment

•
Laryngoscope–
Miller for infants and toddlers
–
Miller or Macintosh for older children
Endotracheal Intubation: Equipment

•
Curved vs. Straight blade positioning
Endotracheal Intubation

•
Confirm tube placement–
Auscultation
–
CO2
detection–
Ability to ventilate
Endotracheal Intubation

Circulation

•
Cardiac monitor•
Pediatric electrodes for infants and young children.
•
Adult electrodes may be used for larger children and adolescents.
•
Make sure pediatric paddles are available for defibrillation if necessary.
Circulation
•
Tachycardia:•
Hypovolemia
•
Hypoxia•
Anxiety
•
Fever•
Pain
•
Cardiac impairment
•
Bradycardia
Circulation

•
Pulses–
Newborns: Umbilical
artery–
Infants: brachial artery
–
Children: carotid artery
Circulation

•
Pulse quality–
Rate
–
Strength–
Central vs
Peripheral
•
Capillary refill time (CRT)•
Skin color and temperature:–
Warm, cool, pale, or cyanotic?
Circulation

•
Blood Pressure (5th
percentile)–
Infants SBP 60
–
1 year SBP 70–
>1 year SBP (70 + 2 x age)
Circulation

•
Intravenous fluids–
Peripheral IV access
Circulation


•
Intraosseous
(IO) access–
No age restrictions
–
30-90 seconds or 3 attempts–
Can infuse ANYTHING
–
New options: EZ-IO©
Circulation

•
Intraosseous
needle
Circulation

•
Vidacare
EZ-IO
Circulation

•
IO Insertion
Circulation

Pediatric Pearls

Children compensate better than adults
Pediatric Pearls

You cannot remember normal weights, respiratory rates,
blood pressures, heart rates, and calculate drug doses in your head….so don’t try….
Pediatric Pearls

Airway is everything… remember the basics
Pediatric Pearls


Relax…they’re just little (misshapen) adults
Pediatric Pearls
