







Languages
Pages
Legal


MEDICARE: PAST, PRESENT AND FUTURE
James G. Anderson, Ph.D.
Department of Sociology & Anthropology

MEDICARE PART A• Federal heath insurance for persons over 65
years of age
• Covers acute care hospitalization
• Covers limited nursing home care and other institutional services
• The permanently disabled were covered at a later date
• In 1973, the end-stage renal disease program was added to Medicare
MEDICARE PART B
• Requires financial contributions from enrollees
• Covers professional fees for medical and surgical services

MEDICARE ENROLLEES(In Millions)
19.525 31.1
38.1
60
80
010
20
30
4050
60
70
8090
100
1967 1975 1985 1996 2020 2040
Enrollees

MEDICARE EXPENDITURES(In Millions)
4,73716,316
72,294
184,203
213,401
0
50,000
100,000
150,000
200,000
250,000
1967 1975 1985 1995 1998
Expenditures

CBO PROJECTIONS (Enrollment as % of Population)
13.6 14.8
22 23.124.7
0
5
10
15
20
25
30
1995 2010 2030 2050 2070
%

CBO PROJECTIONS (Spending as % of GDP)
2.63.7
6.37
7.8
0
1
23
4
5
67
8
9
10
1995 2010 2030 2050 2070
%

PROBLEMS WITH MEDICARE
• Impending insolvency of the hospital insurance trust fund
• Favors acute care over chronic care
• Does not cover most long term care services
• Omits prescription drug coverage
• Permits medical costs to impoverish older adults and their families

THE FUTURE OF MEDICARENumber of Workers per Retiree
4 3.9
2.8
2.1
0
0.5
11.5
2
2.5
3
3.54
4.5
5
1980 2000 2020 2040
Enrollees

Medicare’s Dwindling Reserves (In billions)
110
85
55
18
-30-50
-30
-10
10
30
50
70
90
110
1997 1998 2000 2001
Reserves

MEDICARE ENROLLEES IN MANAGED CARE
5.7
9.5
-1
1
3
5
7
9
11
1990 1995
%
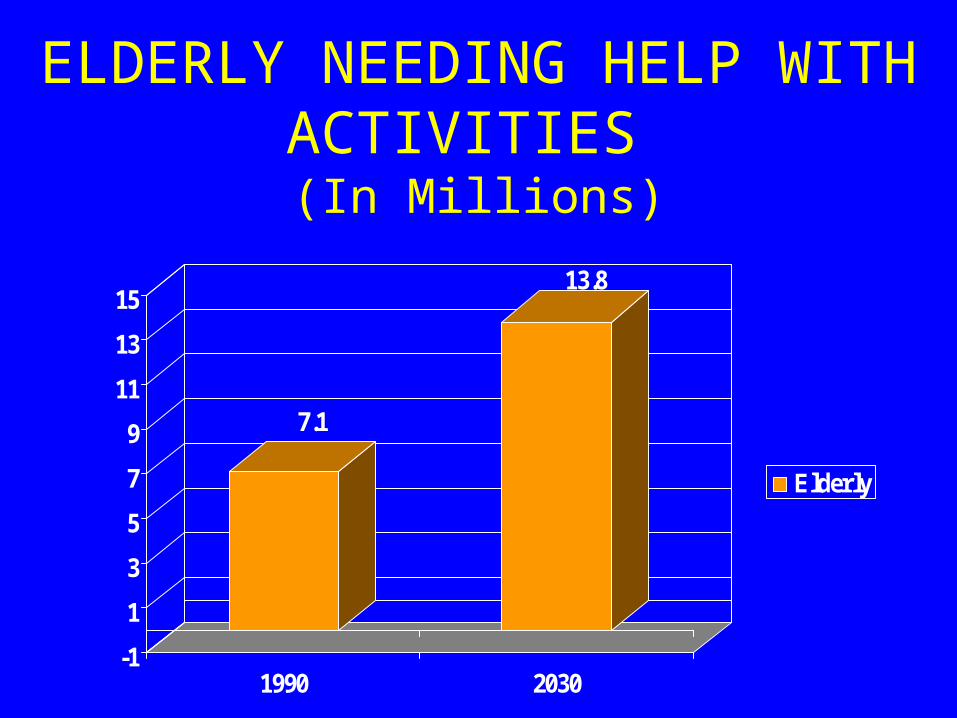
ELDERLY NEEDING HELP WITH ACTIVITIES
(In Millions)
7.1
13.8
-1
1
3
5
7
9
11
13
15
1990 2030
Elderly
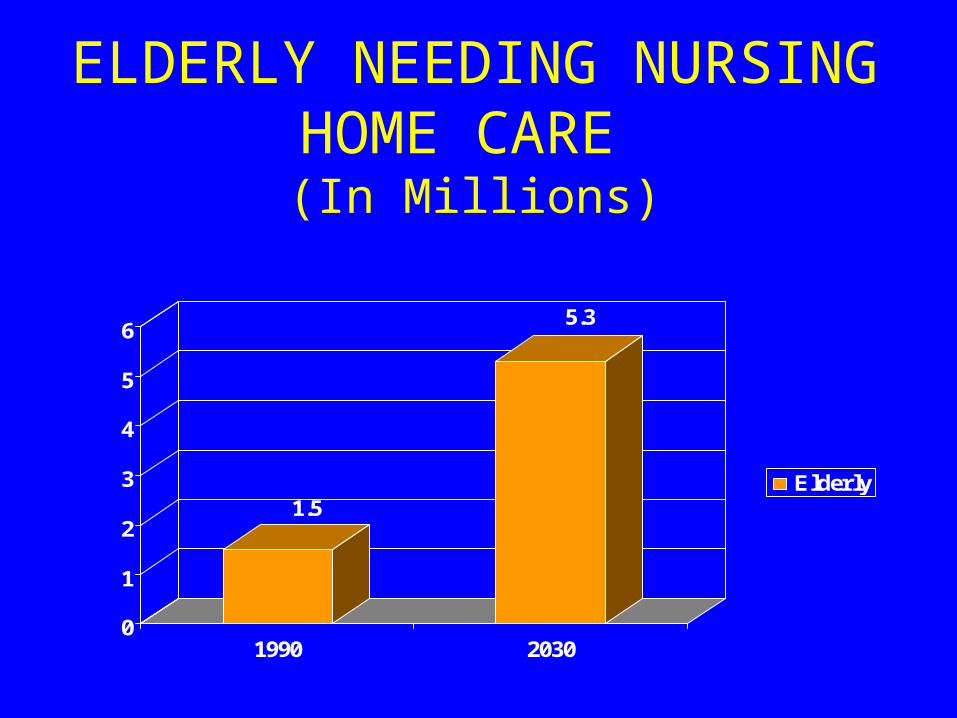
ELDERLY NEEDING NURSING HOME CARE
(In Millions)
1.5
5.3
0
1
2
3
4
5
6
1990 2030
Elderly

REFORM PRPOSALS• Gradually raise eligibility age to 70• Raise direct payments by recipients by higher premiums for
MD insurance or raise co-payments for services• Provide incentives for Medicare beneficiaries to join HMOs• Offer Medicare beneficiaries more choice in their health care
plans• Institute a means test for Medicare• Enact an annual budget for Medicare• Authorize medical savings accounts

PROPOSAL FOR MEDICARE PRESCRIPTOIN DRUG BENEFIT
• New voluntary prescription drug coverage
• Premiums would start at $24/month in 2002, rising to $44 by 2008
• No deductible and a 50% co-payment. Government would pay half of the first $2000 in 2002, with the cap rising to $5,000 in 2008
• No premiums or co-payments for single persons with incomes under $11,000 and couples under $17,000
• Financial incentives would be given to employers who continue retiree health coverage if it provides a prescription drug benefit.
PRESCRIPTION DRUG BENEFITArguments For
• Prescription drug prices are out of control
• More than 1/3 of Medicare beneficiaries lack coverage
• Price discrimination against the elderly
• Drugs are now routinely used to treat heart disease, cancer, arthritis, etc.
PRESCRIPTION DRUG BENEFITArguments Against
• Drug benefits would cost $70-90 per month in a Medigap policy
• Drug benefits would require high deductibles and co-payments
• The pharmaceutical industry argues it will lead to price controls
• The pharmaceutical industry argues it will lead to a reduction in R&D expenditures in new drugs
Long Term Care BenefitArguments For
• (1) Long-term custodial care accounts for 81% of catastrophic costs for the elderly.
• (2) Over half of those 65 years and older will need some kind of long-term care (LTC).
• (3) Over 70 % of single elderly patients spend down to the poverty level after 13 weeks in a nursing home.
• (4) 5% of Medicaid recipients in nursing homes consume 43% of the Medicaid budget.
• (5) The most equitable policy would be a universal mandatory LTC health insurance program financed by the federal government.
• (6) There are a number of ways of financing universal LTC.

Long Term Care BenefitArguments Against
• (1) Family members should not be allowed to shift the cost of LTC onto the government and thus, onto taxpayers.
• (2) A government sponsored LTC health insurance program would be enormously costly.
• (3) Such a program would enormously increase both the demand for and the cost of LTC.
• (4) A tax supported program would be regressive - taxing younger working people to provide benefits for elderly persons with substantial resources.
• (5) The government should only provide assistance to those who do not have the resources to pay for long term care.
• (6) Instead of a government sponsored program the government should provide incentives for private insurance and savings to finance LTC. Outline.
DISCUSSION QUESTIONS
• Should we regulate drug prices like other countries do?
• How would regulation affect development of new drugs?
• Should Medicare cover prescription drugs? For all enrollees? For only the poor?
• Should Medicare purchase drugs at a discount and sell them to the elderly?
DISCUSSION QUESTIONS
• Should we extend Medicare to provide for Long Term Care?
• Should Medicare cover Long term care for all enrollees? For only the poor?
• How would we pay for Long Term Care? Increase the general payroll tax? Require the elderly to pay part or all of the premium for LTC?
Top Related