







Languages
Pages
Legal


Medical Problems in Pregnancy
Cathy Nelson-Piercy
Consultant Obstetric Physician Guyrsquos amp St Thomasrsquo Foundation Trust
and Imperial College Healthcare Trust
Professor of Obstetric Medicine
Kingrsquos Health Partners
KCL Division of Womenrsquos Health
bull Pregnant women are more predisposed to certain acute
medical problems
bull Those with chronic medical conditions can worsen
flare
bull Pregnant women can suffer pregnancy specific medical
problems
bull Pregnant and postpartum women deserve the same
attention to diagnosis and treatment and appropriate
management plans as the non-pregnant patient
bull Most drugs do not have a licence for use in pregnancy
bull Errors of omission are common
General Principles Page 1
Maternal death rate 2003-12 (Three year rolling averages)
0
2
4
6
8
10
12
14
16
2004 2005 2006 2007 2008 2009 2010 2011
Rate
per
100 0
00 m
ate
rnit
ies
Mid-year of each three-year period
Direct and Indirect maternal death
rate
Direct maternal death
rate
Indirect maternal death rate
Indirect maternal deaths 1985-2011 (Three year periods)
0
1
2
3
4
5
6
7
8
9
10
1985-1987 1988-1990 1991-1993 1994-1996 1997-1999 2000-2002 2003-2005 2006-2008 2009-2011
Ra
te p
er
10
0 0
00
ma
tern
itie
s
Triennium
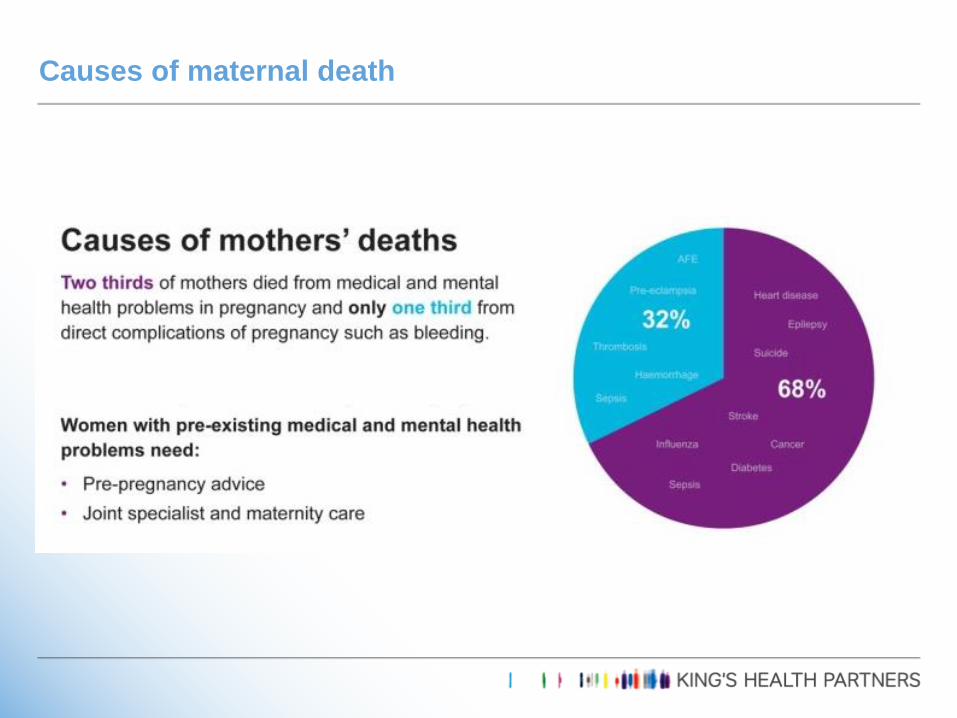
Causes of maternal death
82
Direct
163
Indirect
medical
Causes of maternal death
000
050
100
150
200
250
Rate
per
1000
00 m
ate
rnit
ies
Solid bars show indirect causes hatched bars show direct causes
74 of women who died 2009-12
had a pre-existing medical disorder
Medical Problems in Pregnancy
Pre-existing Asthma
Epilepsy
Hypertension
Diabetes
Thyroid
SLE RA CTD
Renal
Cardiac
Pregnancy - specific Pre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis gravidarum
Acute Fatty Liver of Pregnancy
Coincidental Pneumonia Malaria Hepatitis
bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

bull Pregnant women are more predisposed to certain acute
medical problems
bull Those with chronic medical conditions can worsen
flare
bull Pregnant women can suffer pregnancy specific medical
problems
bull Pregnant and postpartum women deserve the same
attention to diagnosis and treatment and appropriate
management plans as the non-pregnant patient
bull Most drugs do not have a licence for use in pregnancy
bull Errors of omission are common
General Principles Page 1
Maternal death rate 2003-12 (Three year rolling averages)
0
2
4
6
8
10
12
14
16
2004 2005 2006 2007 2008 2009 2010 2011
Rate
per
100 0
00 m
ate
rnit
ies
Mid-year of each three-year period
Direct and Indirect maternal death
rate
Direct maternal death
rate
Indirect maternal death rate
Indirect maternal deaths 1985-2011 (Three year periods)
0
1
2
3
4
5
6
7
8
9
10
1985-1987 1988-1990 1991-1993 1994-1996 1997-1999 2000-2002 2003-2005 2006-2008 2009-2011
Ra
te p
er
10
0 0
00
ma
tern
itie
s
Triennium
Causes of maternal death
82
Direct
163
Indirect
medical
Causes of maternal death
000
050
100
150
200
250
Rate
per
1000
00 m
ate
rnit
ies
Solid bars show indirect causes hatched bars show direct causes
74 of women who died 2009-12
had a pre-existing medical disorder
Medical Problems in Pregnancy
Pre-existing Asthma
Epilepsy
Hypertension
Diabetes
Thyroid
SLE RA CTD
Renal
Cardiac
Pregnancy - specific Pre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis gravidarum
Acute Fatty Liver of Pregnancy
Coincidental Pneumonia Malaria Hepatitis
bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Maternal death rate 2003-12 (Three year rolling averages)
0
2
4
6
8
10
12
14
16
2004 2005 2006 2007 2008 2009 2010 2011
Rate
per
100 0
00 m
ate
rnit
ies
Mid-year of each three-year period
Direct and Indirect maternal death
rate
Direct maternal death
rate
Indirect maternal death rate
Indirect maternal deaths 1985-2011 (Three year periods)
0
1
2
3
4
5
6
7
8
9
10
1985-1987 1988-1990 1991-1993 1994-1996 1997-1999 2000-2002 2003-2005 2006-2008 2009-2011
Ra
te p
er
10
0 0
00
ma
tern
itie
s
Triennium
Causes of maternal death
82
Direct
163
Indirect
medical
Causes of maternal death
000
050
100
150
200
250
Rate
per
1000
00 m
ate
rnit
ies
Solid bars show indirect causes hatched bars show direct causes
74 of women who died 2009-12
had a pre-existing medical disorder
Medical Problems in Pregnancy
Pre-existing Asthma
Epilepsy
Hypertension
Diabetes
Thyroid
SLE RA CTD
Renal
Cardiac
Pregnancy - specific Pre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis gravidarum
Acute Fatty Liver of Pregnancy
Coincidental Pneumonia Malaria Hepatitis
bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Indirect maternal deaths 1985-2011 (Three year periods)
0
1
2
3
4
5
6
7
8
9
10
1985-1987 1988-1990 1991-1993 1994-1996 1997-1999 2000-2002 2003-2005 2006-2008 2009-2011
Ra
te p
er
10
0 0
00
ma
tern
itie
s
Triennium
Causes of maternal death
82
Direct
163
Indirect
medical
Causes of maternal death
000
050
100
150
200
250
Rate
per
1000
00 m
ate
rnit
ies
Solid bars show indirect causes hatched bars show direct causes
74 of women who died 2009-12
had a pre-existing medical disorder
Medical Problems in Pregnancy
Pre-existing Asthma
Epilepsy
Hypertension
Diabetes
Thyroid
SLE RA CTD
Renal
Cardiac
Pregnancy - specific Pre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis gravidarum
Acute Fatty Liver of Pregnancy
Coincidental Pneumonia Malaria Hepatitis
bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
Causes of maternal death
82
Direct
163
Indirect
medical
Causes of maternal death
000
050
100
150
200
250
Rate
per
1000
00 m
ate
rnit
ies
Solid bars show indirect causes hatched bars show direct causes
74 of women who died 2009-12
had a pre-existing medical disorder
Medical Problems in Pregnancy
Pre-existing Asthma
Epilepsy
Hypertension
Diabetes
Thyroid
SLE RA CTD
Renal
Cardiac
Pregnancy - specific Pre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis gravidarum
Acute Fatty Liver of Pregnancy
Coincidental Pneumonia Malaria Hepatitis
bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

82
Direct
163
Indirect
medical
Causes of maternal death
000
050
100
150
200
250
Rate
per
1000
00 m
ate
rnit
ies
Solid bars show indirect causes hatched bars show direct causes
74 of women who died 2009-12
had a pre-existing medical disorder
Medical Problems in Pregnancy
Pre-existing Asthma
Epilepsy
Hypertension
Diabetes
Thyroid
SLE RA CTD
Renal
Cardiac
Pregnancy - specific Pre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis gravidarum
Acute Fatty Liver of Pregnancy
Coincidental Pneumonia Malaria Hepatitis
bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Causes of maternal death
000
050
100
150
200
250
Rate
per
1000
00 m
ate
rnit
ies
Solid bars show indirect causes hatched bars show direct causes
74 of women who died 2009-12
had a pre-existing medical disorder
Medical Problems in Pregnancy
Pre-existing Asthma
Epilepsy
Hypertension
Diabetes
Thyroid
SLE RA CTD
Renal
Cardiac
Pregnancy - specific Pre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis gravidarum
Acute Fatty Liver of Pregnancy
Coincidental Pneumonia Malaria Hepatitis
bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Medical Problems in Pregnancy
Pre-existing Asthma
Epilepsy
Hypertension
Diabetes
Thyroid
SLE RA CTD
Renal
Cardiac
Pregnancy - specific Pre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis gravidarum
Acute Fatty Liver of Pregnancy
Coincidental Pneumonia Malaria Hepatitis
bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

bull 39 yr old multip 12 weeks 76kg
bull Secondary infertility IVF pregnancy
bull Admission for ovarian hyperstimulation syndrome
bull A+E CO swollen painful left leg for 3 weeks
bull Sudden onset left sided pleuritic pain last night
bull SOB since
bull OE dyspnoeic RR 34 SOBOE undressing
bull Pulse 118 BP 10466
bull Oxygen saturation 92
Case 1
A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

A D dimers
B leg dopplers
C Enoxaparin (Clexane) 80mg bd
D Enoxaparin (Clexane) 120mg od
E VQ
F CTPA
Case 1 Which of the following isare appropriate
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
Diagnosis
D dimers are useless
Unless higher pregnancy
specific normal ranges are
used
Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Rads mGy
CXR lt0001 lt001
Perfusion scan lt008 lt08
Ventilation scan lt001 lt01
CTPA Helical CT lt0013 lt013
Max recommended lt05 5
Radiation exposure
Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Radiation in pregnancy Page 13
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ
10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of
developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of
breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

201421949ndash959
frequency of VTE 506 preg
41 (95 CI = 26 to 60) frequency of VTE non-preg
124 (95 CI = 90 to 163)
Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Diagnosis of PE in pregnancy Suspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysisiv heparin
thrombectomy
Portable echo
Suggestive of
massive PE
CTPA
+ve -ve
CXR abnormal CXR normal
VQ scan
+ve
-ve
+ve -ve
Stop
anticoagulation
Still suspicious of
PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Learning points - Investigating suspected PE in pregnancy Page 17
BMJ 2007 Feb 24334(7590)418-9 Scarsbrook AF Gleeson FV
bull Physiological changes during pregnancy can mimic pulmonary
embolism making clinical diagnosis unreliable
bull Imaging is essential to avoid inappropriate treatment and can be
performed without exposing the fetus to any specific risks
bull A chest x ray should always be performed to exclude other causes
bull Half dose perfusion scintigraphy can be used in most patients
bull Computed tomographic pulmonary angiography should be used only
in patients with lung disease such as asthmamdashwhich makes
scintigraphy less likely to be diagnosticmdashor an abnormal chest x ray
because it exposes maternal breast tissue to high doses of radiation
High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

High dose LMWH
eg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
lsquoIncrease in volume of distribution during pregnancy leads to a prolongation of enoxaparin half-life so once-daily dosing is adequatersquo
Patel J P et al Circulation 20131281462-1469
Thrombolysis
SHOULD NOT BE WITHELD in massive PE with haemodynamic instability
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Case 2
24 year old P0
27 weeks pregnant
co palpitations
Associated dizziness and breathlessness
oe tachycardic HR ndash 240
BP 9468
C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

C Nelson-Piercy
Case 2
Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Vagotonic manoeuvres are safe
Adenosine ndash safe
Verapamil is effective second line therapy
Up to 10mg can be given without affecting fetal HR
Beta-blockers also safe
SVT
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
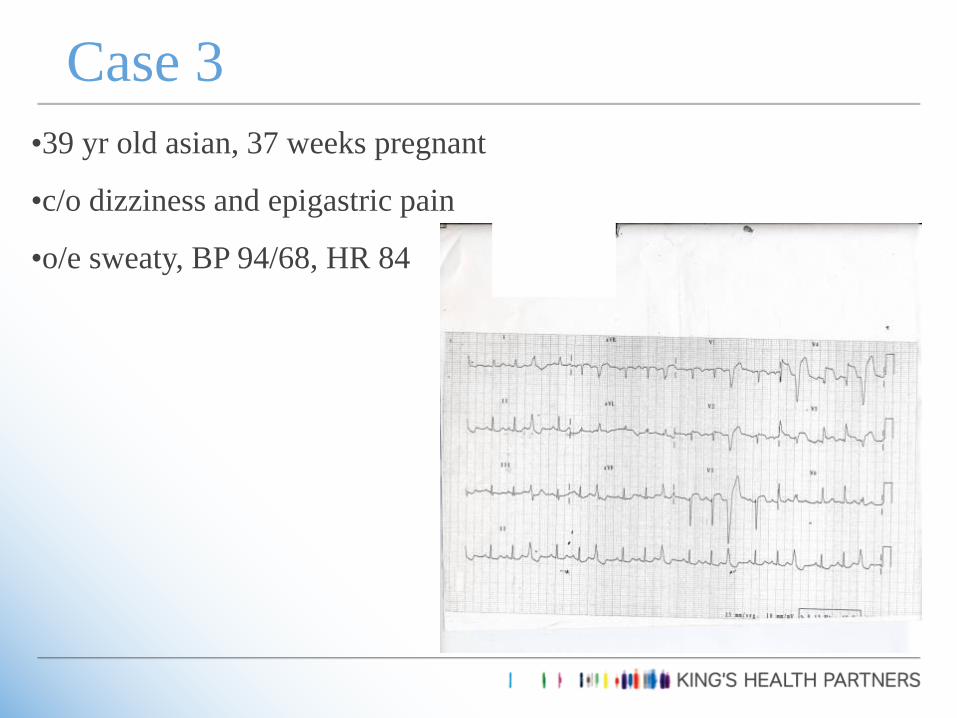
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 3
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 3 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 4
A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

A CXR
B back XR
C TTE
D TOE
E abdo US
F CTPA
Case 4 What investigations would you request
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Case 5
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
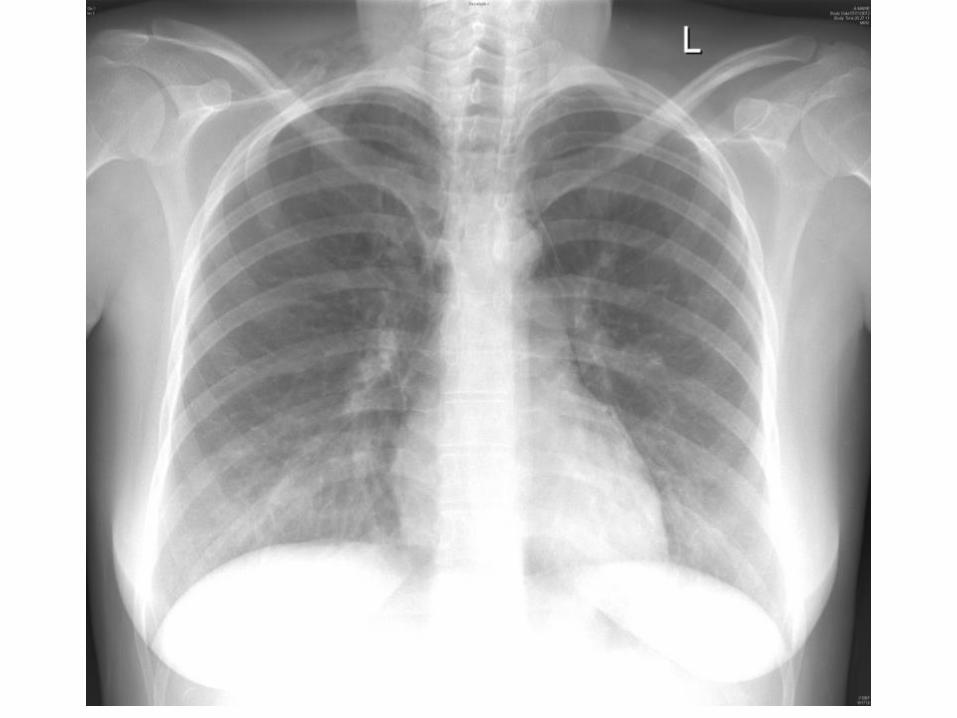
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacial clefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

SIGNBTS Asthma Guideline 101
bull Women should be advised of the importance
of maintaining good control of their asthma
during pregnancy to avoid problems for both
mother and baby
bull Counsel women with asthma regarding the
importance and safety of continuing their
asthma medications during pregnancy to
ensure good asthma control
National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

National asthma audit
Asthma deaths occurring
between February 2012 and
January 2013 (n = 195)
Highlights lack of education
amongst women and
healthcare providers as a
key failing
CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

CHEST 2015 147 ( 2 ) 406 - 414
4895 patients with acute asthma 125 pregnant women in 48 EDs
61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

61006
A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

A Amoxycillin and doxycycline
B Amoxycillin and erythromycin
C Augmentin and doxycycline
D Cefuroxime
E Amoxycillin and clarithromycin
Appropriate antibiotic therapy
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

bull 39 year old AC P2
bull Essential hypertension
bull 840 headache and worsening hypertension
bull Rx analgesia increased methyldopa
bull 1040 headache severe worse on bending
bull 2 episodes of numbness right hand - 15 mins
bull Fundoscopy papilloedema
Case 5
A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

A CT
B MRI
C MRV
D PET scan
E LP
F CTvenogram
Case 7 What investigations would you do
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome)
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
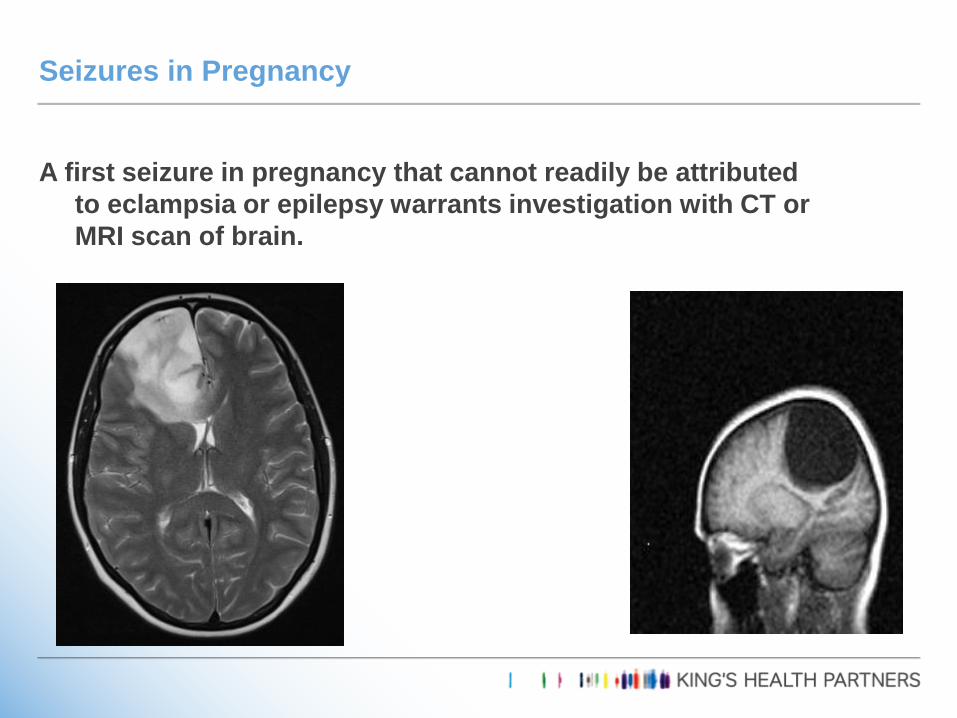
Rare - Approximately 10 of cases occur in the post-partum period
Presents with explosive-onset lsquoworst-everrsquo headache
Thunderclap ndash peaks 1 min intense
23 occur in the first week post partum
Multiple thunderclap headaches over 1-4 weeks ~ pathognomonic
Background headache in between
RCVS - Reversible cerebral vasoconstriction syndrome Page 49
AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

AIRWAY
BREATHING
CIRCULATION
WEDGE (25 increase in CO)
DELIVER
Maternal Cardiac Arrest Remember
Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Perimortem caesarean section is part of
the resuscitation procedure in any
women who arrests in the second half
of pregnancy It should be undertaken
to facilitate maternal resuscitation
within 5 minutes of the arrest if there
is no initial response to advance life
support in the tilted position
Perimortem caesarean section
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for over half the direct and nearly all indirect maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy

sympregimperialacuk
RCP course
Nov 18-20th 2015
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy