






Languages
Pages
Legal


MED SCAPE AND ETC.Chonpiti Siriwan, MD.
April 2015.

Topic
• Endocrine society guideline for primary aldosteronism
2015
• NBHA Diagnostic criteria for osteoporosis: PROs and
Cons?
• AACE and ACE Clinical Practice Guidelines for
Developing a Diabetes Mellitus Comprehensive Care Plan
2015
Topic
• Increased Stroke Risk in Some Patients With Subclinical
Hypothyroidism
• FDA Panel Backs New Safety Warnings on Two Diabetes
Drugs
• Statins for Primary Prevention in Everyone 75 Years and
Older? It Could Be Cost-Effective: Analysis

GUIDELINES ON
PRIMARY
ALDOSTERONISMTitle:
The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline
March 20, 2015
DO NOT DISTRIBUTE. DRAFT: CONFIDENTIAL. DO NOT DISTRIBUTE.

Guidelines on Primary Aldosteronism
Authors
• John W. Funder (chair)
• Robert M. Carey
• Franco Mantero
• Mohammad Hassan
Murad
• Martin Reincke
• Hirotaka Shibata
• Michael Stowasser
• William F. Young. Jr.
Cosponsoring Associations
• European Society of
Endocrinology
• European Society of
Hypertension
• International Society of
Endocrinology
• International Society of
Hypertension
• The Japanese Society of
Hypertension

Summary of recommendations
• Case detections• Hypertension
• Sustain BP ≥ 180/110 mmHg
• Resistance HTN (on 3 conventional antihypertensive drugs, including a diuretic)
• BP <140/90: On ≥4 antihypertensive drugs
• HTN and spontaneous or diuretic induced hypokalemia
• HTN and adrenal incidentaloma
• HTN and a family history
• Early onset hypertension or cerebrovascular accident at a young age (<40 years)
• All first degree relatives of patients with PA
• Sustained BP >150/100
• Patients with hypertension (BP>140/90) and obstructive sleep apnea.
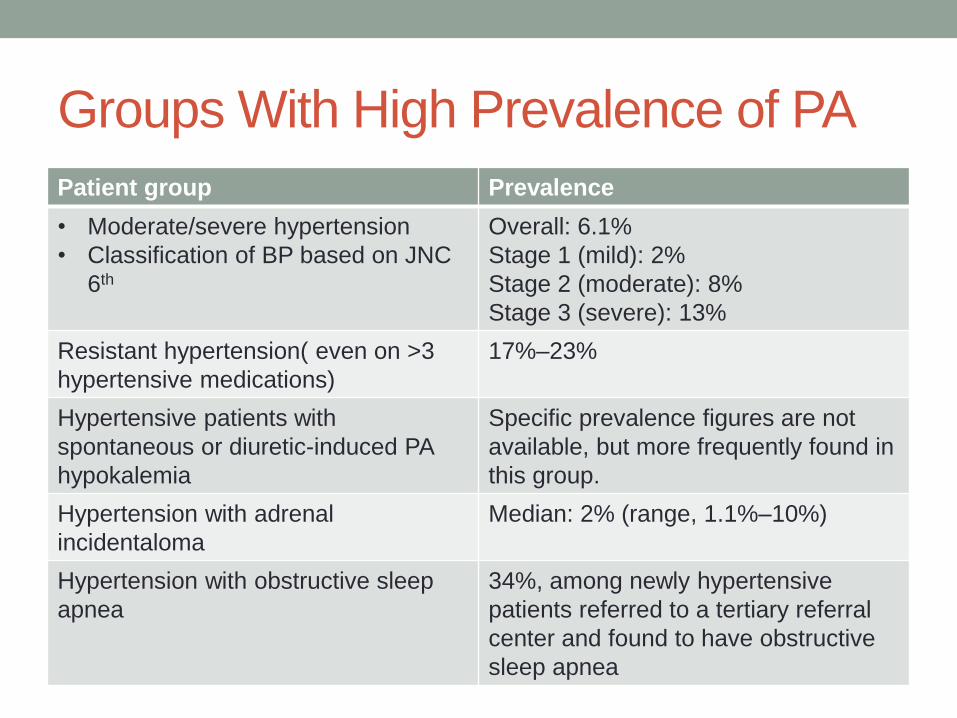
Groups With High Prevalence of PA
Patient group Prevalence
• Moderate/severe hypertension
• Classification of BP based on JNC
6th
Overall: 6.1%
Stage 1 (mild): 2%
Stage 2 (moderate): 8%
Stage 3 (severe): 13%
Resistant hypertension( even on >3
hypertensive medications)
17%–23%
Hypertensive patients with
spontaneous or diuretic-induced PA
hypokalemia
Specific prevalence figures are not
available, but more frequently found in
this group.
Hypertension with adrenal
incidentaloma
Median: 2% (range, 1.1%–10%)
Hypertension with obstructive sleep
apnea
34%, among newly hypertensive
patients referred to a tertiary referral
center and found to have obstructive
sleep apnea

Algorithm for the detection, confirmation,
subtype testing, and treatment of primary
aldosteronism (PA)

Case detections
• Use of the plasma aldosterone/renin ratio (ARR) to detect
possible cases of PA in these patient groups
• ARR:
• Detection test only
• Repeat if inconclusive result

Factors That May Lead to False-Positive
or False-Negative ARR Results


Remarks
• Renin inhibitors
• Lower PRA
• But raise DRC.
• Expected to result
• false positive ARR levels for renin measured as PRA
• false negatives for renin measured as DRC
• In premenopausal women
• Briskly raising plasma aldosterone level in the luteal phase
• False positives can occur during the luteal phase

Measurement of ARR: A Suggested Approach
• Correct hypokalemia
• Use syringe and needle [preferably not a Vacutainer® to minimize the risk of spuriously raising potassium]
• Waiting at least 5 seconds after tourniquet release (if used)
• Encourage patient to liberalize (rather than restrict) sodium intake.
• Withdraw agents that markedly affect the ARR (Mulatero, Hypertension, 2002) for at least 4 weeks: • Spironolactone, eplerenone, amiloride, and triamterene
• Potassium-wasting diuretics
• Products derived from liquorice root (e.g., confectionary licorice, chewing tobacco)

Measurement of ARR: A Suggested Approach
• Withdraw other medications that may affect the ARR for at
least 2 weeks:
• Beta-adrenergic blockers, central alpha-2 agonists (e.g., clonidine,
alpha- methyldopa), nonsteroidal anti-inflammatory drugs
• Angiotensin-converting enzyme inhibitors, angiotensin receptor
blockers, renin inhibitors, dihydropyridine calcium channel
antagonists
• Controlled BP with relatively noninterfering medications
• Establish OC and HRT status
• Estrogen-containing medications may lower DRC
• Cause false-positive ARR when DRC
• Do not withdraw OC unless confident of alternative effective
contraception.

Medications With Minimal Effects on
Plasma Aldosterone Levels

Conditions for collection of blood
• Midmorning
• after the patient has been up (sitting, standing, or walking)
for at least 2
• Seated for 5-15 min before blood collection
• Avoiding stasis and hemolysis
• Maintain sample at room temperature (and not on ice, as
this will promote conversion of inactive to active renin)
during delivery to laboratory and prior to centrifugation
and rapid freezing of plasma component pending assay

Case confirmations
• Positive aldosterone-renin ratio (ARR)
• One or more confirmatory tests to definitively confirm or
exclude the diagnosis
• Setting may NO NEED confirmation test
• spontaneous hypokalemia
• undetectable renin
• plasma aldosterone concentration (PAC) >20 ng/dl,

Confirmation test
• Oral sodium loading test
• Saline infusion test
• In a modified approach which appears, in preliminary studies, to
have much higher sensitivity for diagnosing PA, patients remain in
a seated position for at least 30 mins and during the infusion
(Amhed, 2014).
• Fludrocortisone suppression test
• Captopril challenge test

Subtype classification
• CT: initial study in subtype testing
• Large masses: ACC (Almost always >4 cm)
• APA: small hypodense nodules (usually <2 cm in diameter)
• IAH: normal adrenal glands or show nodular changes
• CT limitations
• Small APA
• Older patient (>35 years): nonfunctioning unilateral adrenal
macroadenomas are not uncommon
• No advantage of MRI over CT in subtype evaluation

AVS: subtype classification
• Experienced radiologist
• Distinction between unilateral and bilateral adrenal
disease
• Surgery desired patients
• AVS may not be needed • younger patients (< age 35)
• spontaneous hypokalemia
• marked aldosterone excess
• unilateral cortical adenoma on adrenal CT scan

AVS
• Advocate the use of continuous cosyntropin infusion
during AVS
• 50 μg/hour
• 30 minutes before adrenal vein catheterization and
continued throughout the procedure
• “Cortisol-corrected aldosterone ratios”
• Cutoff ratio from high-side to low- side > 4:1

Other modalities for subtype classification
• Iodocholesterol scintigraphy. [131I]-19-iodocholesterol
scintigraphy
• Sensitivity depend on size of adenoma
• Not helpful in small adenoma (<1.5cm)
• 18-Hydroxycorticosterone Levels (18-OHB)
• >100 ng/dl at 8:00 a.m in APA
• No support evidence
• (11)C-Metomidate Positron Emission Tomography (PET)-
CT
• 87% specificity and 76% sensitivity for APA
• Future use

Genetic testing
• Indication for FH-I genetic testing
• Onset of confirmed PA <20 years of age
• Family history of PA or of strokes at young age (<40 years)
• Testing for germline mutations in KCNJ5
• Causing FH-III
• Very young patients with PA

Testing for Familial Forms of PA: FH-I [GRA]
• AD, 1% cause of PA
• CYP11B1/CYP11B2 chimeric gene
• Aldosterone secretion depend on ACTH
• Indicated in family history of PA or of strokes at a young
age (<40years)

Testing for Familial Forms of PA: FH-II
• AD, possibly genetically heterogeneous
• No response to DEX suppression
• Negative for GRA mutation
• 7% of PA
• Presented with APA or IHA
• Unclear molecular basis
• Abnormal chromosomal region 7p22 in several linkage
analysis
• Somatic KCNJ5 mutations (~FH-III) in some cases

Testing for Familial Forms of PA: FH-III
• Mutation in the KCNJ5 gene
• Encoding the potassium channel Kir 3.4
• 9 of 10 affected subjects were diagnosed at age 6 or
younger
Mulatero, P. et al. (2012) Role of KCNJ5 in familial and sporadic primary aldosteronism
Nat. Rev. Endocrinol. doi:10.1038/nrendo.2012.230

Genetic Events in Sporadic APA
• KCNJ5
• ATP1A1 and ATP2B3
• ATP1A1: coding for the α subunit of the Na+,K+-ATPase
• ATP2B3: coding for the plasma membrane calcium-transporting
ATPase 3 (PMCA3)
• Significantly reduced Na+,K+-pump activity
• Mutation carriers show increased plasma aldosterone and lower
potassium compared with non-carriers
• More common in males

Genetic Events in Sporadic APA
• CACNA1D
• Encoding a voltage-gated calcium channel
• 5-11% in zona glomerulosa–like APAs without KCNJ5
mutations
• Activation of Cav1.3 channels
• Increases intracellular Ca2+ entry leading to Ca2+-
mediated signaling and enhanced aldosterone secretion

Treatment
• Unilateral laparoscopic adrenalectomy
• unilateral PA i.e., aldosterone-producing adenoma [APA]
• unilateral adrenal hyperplasia [UAH]
• Medical treatment including a mineralocorticoid receptor
(MR) antagonist
• Unable to surgery
• Unwilling to surgery
• Unwilling or unable to undergo further investigations

Treatment
• For medical treatment
• Suggest spironolactone as the primary agent
• Eplerenone as an alternative
• For GRA
• Lowest dose of glucocorticoid to lower corticotropin (ACTH)
• Normalize blood pressure and serum potassium levels rather than
first-line treatment with an MR antagonist

NBHA DIAGNOSTIC CRITERIA FOR
OSTEOPOROSIS: PROS AND CONS?
• Pros: Alexandra PapaioannouDivision of Geriatric Medicine, McMaster University, St Peter's
Hospital, GERAS Centre, Hamilton, ON L8M 1W9, Canada
• Cons: John T SchousboePark Nicollet Health Services, Minneapolis, MN 55416, USA
Lancet Diabetes Endocrinol 2015; 3: 234–37.
Position paper
Osteoporos Int (2014) 25:1439–1443.
DOI 10.1007/s00198-014-2655-z
National Bone Health Alliance Working Group
• Group of 17 clinicians and clinical scientists
• National Osteoporosis Foundation (NOF)
• American Society for Bone and Mineral Research (ASBMR)
• American Academy of Orthopedic Surgeons
• Centers for Disease Control

Fracture types that allow a diagnosis of
osteoporosis • With or without BMD test: Low-trauma hip fracture
• Osteopenia: Low-trauma clinical vertebral fracture,
proximal humerus fracture, or pelvis fracture
• Clinician reason: Incidental finding of a vertebral fracture
on a radiograph (a morphometric vertebral fracture)
• Osteopenia at the lumbar spine or hip by BMD: low-
trauma distal forearm fracture

Role of FRAX in making the diagnosis of
osteoporosis
• WHO fracture risk assessment tool
• Combine femoral neck BMD (or total hip)
• Well-validated and weighted clinical risk factors for
fracture
• Largely independent of BMD
• Useful as risk predicting
• hip fracture
• major osteoporotic fractures

Role of FRAX in making the diagnosis of
osteoporosis • Dx osteoporosis
• 10-year probability of hip fracture is ≥3 %
• 10-year probability of major osteoporotic fracture is ≥20 %
• Reflect treatment intervention thresholds in the USA
• Described in the NOF Clinician’s Guide
• Cost-effectiveness criteria for hip fracture management
• Logical basis for making a diagnosis of osteoporosis

Further considerations
• Identifying greater number of people elevated risk for
fracture
• Increasing awareness
• Encouraging strategies to lower risk
• Pharmacologic and non-pharmacologic
• FRAX as the outcome of clinical study

Conclusion
• Dx osteoporosis
• Postmenopausal women
• Men > 50 years
• Elevated risk for future fractures based on FRAX
• T-score of ≤−2.5 at the spine or hip
• Low-trauma hip fracture
• Low-trauma vertebral, proximal humerus, pelvis,
• Some cases of distal forearm fracture

Conclusion
• Osteoporotic associated fracture
• 2/3 Hip, vertebral, distal radius, and pelvis
• Major osteoporotic fractures
• Proximal humerus
• Hip
• Spine
• Distal forearm

PROs:(1)
• 2-paradigm shifts in the diagnosis and management of
osteoporosis
• Clinical risk factors: fracture risk prediction: FRAX
• Importance of bone quality
• Fracture prediction: NOT base on BMD only
• More than half of fractures occur in the non-osteoporotic
range
• Indicating relatively poor sensitivity of BMD
• FIT trial: bisphosphonates decreased vertebral fracture
risk in patients with low bone mass (Femoral neck T
scores 1.6-2.5)
Mayo Clin Proc, 80 (2005), pp. 343–349.

PROs: (2)
• Clinical predictors of fracture have powerful case- finding
potential, particularly when used in older individuals
• FRAX alone comparable predictive ability as FRAX with
BMD and identifies patients at risk who are responsive to
pharmaceutical intervention
• BMD measurement is not possible?
• Bed ridden patients
• More severe underlying disease: more absolute risk
reduction
• Previous fracture is a powerful predictor of a future
fracture

Cons: (1)
• For expanded definition
• Increase the proportion of US adults aged > 65 years who
dx osteoporosis
• 40% -> 72% of women
• 7% -> 34% of men
• Higher demands on the health-care system
• Benefits or harm?: broadening diagnostic criteria

Cons (2)
• Pivotal trials of alendronate, risedronate, and denosumab
• Efficacy only in • Women with a BMD T-score < −2·5
• Existing vertebral fractures
• No efficacy • BMD T-score > −2·5
• no prevalent vertebral fracture
• Clodronate• reduced clinical fractures
• older women not selected on the basis of BMD
• But fracture benefit in women with neither a traditional diagnosis of osteoporosis (based on T score) nor the presence of radiographic vertebral fracture.
Ann Intern Med, 148 (2008), pp. 197–213
J Bone Miner Res, 27 (2012), pp. 211–218
J Bone Miner Res, 22 (2007), pp. 135–141

Cons (3)
• Low evidence of benefit of anti-osteoporotic medication in
patient with BMD T-scores > −2.5
• Fracture risk driven mainly by other skeletal factors
• bone type 1 collagen
• hydroxyapatite crystal structure
• bone microarchitecture
• non-skeletal factors: fall propensity
• Lack evidence of impaired bone quality or fracture risk by
current medication

Con(4)
• Only 1-cost-effective study was used in FRAX
• Generalize to other situation?
• Increase primary care workload
• Psychological impact
• Need further evidence-based research
• Measureable characteristics of bone that contribute to
fracture risk, other than BMD, such as deficits in bone
geometry, microstructure, or material properties
Osteoporos Int, 19 (2008), pp. 437–447.


AACE AND ACE CLINICAL PRACTICE
GUIDELINES FOR DEVELOPING A DIABETES
MELLITUS COMPREHENSIVE CARE PLAN
ENDOCRINE PRACTICE Vol 21 No. 4 April 2015
Writing Committee Cochairpersons
Yehuda Handelsman MD, FACP, FACE, FNLA
Zachary T. Bloomgarden, MD, MACE
George Grunberger, MD, FACP, FACE
Guillermo Umpierrez, MD, FACP, FACE
Robert S. Zimmerman, MD, FACE

CPG Objectives and Structure
• An evidence-based education resource
• Easy-to-follow structure
• 24 diabetes management questions
• 67 practical recommendations
• Concise, practical format that complements existing DM
textbooks
• Suitable for electronic implementation to assist with
clinical decision-making for patients with DM

AACE DM CPG Questions
1. How is diabetes screened and
diagnosed?
2. How is prediabetes managed?
3. What are glycemic treatment goals of
DM?
4. How are glycemic targets achieved for
T2D?
5. How should glycemia in T1D be
managed?
6. How is hypoglycemia managed?
7. How is hypertension managed in
patients with diabetes?
8. How is dyslipidemia managed in
patients with diabetes?
9. How is nephropathy managed in
patients with diabetes?
10. How is retinopathy managed in
patients with diabetes?
11. How is neuropathy diagnosed and
managed in patients with diabetes?
12. How is CVD managed in patients with
diabetes?
13. How is obesity managed in patients
with diabetes?

AACE DM CPG Questions
14. What is the role of sleep medicine in
the care of the patient with diabetes?
15. How is diabetes managed in the
hospital?
16. How is a comprehensive diabetes care
plan established in children and
adolescents?
17. How should diabetes in pregnancy be
managed?
18. When and how should glucose
monitoring be used?
19. When and how should insulin pump
therapy be used?
20. What is the imperative for education
and team approach in DM
management?
21. What vaccinations should be given to
patients with diabetes?
22. How should depression be managed in
the context of diabetes?
23. What is the association between
diabetes and cancer?
24. Which occupations have specific
diabetes management requirements?

• Age ≥45 years without other risk factors
• Family history of T2D
• CVD
• Overweight
• BMI ≥30 kg/m2
• BMI 25-29.9 kg/m2 plus other risk
factors*
• Sedentary lifestyle
• Member of an at-risk racial or ethnic group:
Asian, African American, Hispanic, Native
American, and Pacific Islander
• Dyslipidemia
• HDL-C <35 mg/dL
• Triglycerides >250 mg/dL
• IGT, IFG, and/or metabolic syndrome
• PCOS, acanthosis nigricans, NAFLD
• Hypertension (BP >140/90 mm Hg or therapy
for hypertension)
• History of gestational diabetes or delivery of
a baby weighing more than 4 kg (9 lb)
• Antipsychotic therapy for schizophrenia
and/or severe bipolar disease
• Chronic glucocorticoid exposure
• Sleep disorders† in the presence of glucose
intolerance
• Screen at-risk individuals with glucose values in the normal range every 3 years
• Consider annual screening for patients with 2 or more risk factors
Criteria for Screening for T2D and Prediabetes
in Asymptomatic Adults
55
*At-risk BMI may be lower in some ethnic groups; consider using waist circumference.†Obstructive sleep apnea, chronic sleep deprivation, and night shift occupations.
BMI = body mass index; BP = blood pressure; CVD=cardiovascular disease; HDL-C = high density lipoprotein cholesterol; IFG =
impaired fasting glucose; IGT = impaired glucose tolerance; NAFLD = nonalcoholic fatty liver disease; PCOS = polycystic ovary
syndrome; T2D, type 2 diabetes.
Q1. How is diabetes screened and diagnosed?

Diagnostic Criteria for Prediabetes and
Diabetes in Nonpregnant Adults
56
Normal High Risk for Diabetes Diabetes
FPG <100 mg/dLIFG
FPG ≥100-125 mg/dLFPG ≥126 mg/dL
2-h PG <140 mg/dLIGT
2-h PG ≥140-199 mg/dL
2-h PG ≥200 mg/dL
Random PG ≥200 mg/dL +
symptoms*
A1C <5.5%5.5 to 6.4%
For screening of prediabetes†
≥6.5%
Secondary‡
*Polydipsia (frequent thirst), polyuria (frequent urination), polyphagia (extreme hunger),
blurred vision, weakness, unexplained weight loss.
†A1C should be used only for screening prediabetes. The diagnosis of prediabetes, which
may manifest as either IFG or IGT, should be confirmed with glucose testing.
‡Glucose criteria are preferred for the diagnosis of DM. In all cases, the diagnosis should
be confirmed on a separate day by repeating the glucose or A1C testing. When A1C is
used for diagnosis, follow-up glucose testing should be done when possible to help
manage DM.
FPG, fasting plasma glucose; IFG, impaired fasting glucose; IGT, impaired glucose tolerance; PG, plasma glucose.
Q1. How is diabetes screened and diagnosed?

AACE Recommendations for A1C Testing
• A1C should be considered an additional optional
diagnostic criterion, not the primary criterion for diagnosis
of diabetes
• When feasible, AACE/ACE suggest using traditional
glucose criteria for diagnosis of diabetes
• A1C is not recommended for diagnosing type 1 diabetes
• A1C is not recommended for diagnosing gestational
diabetes

AACE Recommendations for A1C Testing
• A1C levels may be misleading in several ethnic
populations (for example, African Americans)
• A1C may be misleading in some clinical settings
• Hemoglobinopathies
• Iron deficiency
• Hemolytic anemias
• Thalassemias
• Spherocytosis
• Severe hepatic or renal disease
• AACE/ACE endorse the use of only standardized,
validated assays for A1C testing

Management of prediabetes
• IFG
• IGT
• Metabolic syndrome
• Frequent measurement of FPG and/or an OGTT
• Manage CVD risk factors (especially elevated blood
pressure and/or dyslipidemia) and excessive weight, and
monitor these risks at regular intervals
• Attempts to lose 5 to 10% of body weight
• Moderate physical activity (e.g., walking) at least 150
minutes per week


Medical and Surgical Interventions Shown to
Delay or Prevent T2D
62
T2D, type 2 diabetes.
1. DPP Research Group. N Engl J Med. 2002;346:393-403. 2. STOP-NIDDM Trial Research Group. Lancet. 2002;359:2072-2077.
3. Defronzo RA, et al. N Engl J Med. 2011;364:1104-15. 4. DREAM Trial Investigators. Lancet. 2006;368:1096-1105.
5. Torgerson JS, et al. Diabetes Care. 2004;27:155-161. 6. Garvey WT, et al. Diabetes Care. 2014;37:912-921.
7. Sjostrom L, et al. N Engl J Med. 2004;351:2683-2693.
Q2. How is prediabetes managed?
Intervention Follow-up Period
Reduction in Risk of T2D
(P value vs placebo)
Antihyperglycemic agents
Metformin1 2.8 years 31% (P<0.001)
Acarbose2 3.3 years 25% (P=0.0015)
Pioglitazone3 2.4 years 72% (P<0.001)
Rosiglitazone4 3.0 years 60% (P<0.0001)
Weight loss interventions
Orlistat5 4 years 37% (P=0.0032)
Phentermine/topiramate6 2 years 79% (P<0.05)
Bariatric surgery7 10 years 75% (P<0.001)
Lifestyle modification should be used with all pharmacologic or surgical interventions.

Outpatient Glucose Targets for Nonpregnant Adults
Parameter Treatment Goal
A1C, %
Individualize on the basis of age, comorbidities,
duration of disease, and hypoglycemia risk:
• In general, ≤6.5 for most*
• Closer to normal for healthy
• Less stringent for “less healthy”
FPG, mg/dL <110
2-Hour PPG, mg/dL <140
63Q3. What are glycemic treatment goals of DM?
FPG = fasting plasma glucose; PPG = postprandial glucose.
*Provided target can be safely achieved.

Less stringent glucose goal
• A1C: 7-8%
• Patients with history of severe hypoglycemia, limited life
expectancy, advanced renal disease or macrovascular
complications, extensive comorbid conditions, or long-
standing DM in which the A1C goal has been difficult to
attain despite intensive efforts
• So long as the patient remains free of polydipsia, polyuria,
polyphagia, and other hyperglycemia- associated
symptoms

Inpatient Glucose Targets for
Nonpregnant Adults
Hospital Unit Treatment Goal
Intensive/critical care
Glucose range, mg/dL 140-180*
General medicine and surgery, non-ICU
Premeal glucose, mg/dL <140*
Random glucose, mg/dL <180*
65Q3. What are glycemic treatment goals of DM?
ICU = intensive care unit.
*Provided target can be safely achieved.

Q4. How are glycemic targets achieved
for T2DM?

Therapeutic Lifestyle Changes
Parameter Treatment Goal
Weight loss
(for overweight and
obese patients)
Reduce by 5% to 10%
Physical activity150 min/week of moderate-intensity exercise (eg, brisk walking)
plus flexibility and strength training
Diet
• Eat regular meals and snacks; avoid fasting to lose weight
• Consume plant-based diet (high in fiber, low
calories/glycemic index, and high in
phytochemicals/antioxidants)
• Understand Nutrition Facts Label information
• Incorporate beliefs and culture into discussions
• Use mild cooking techniques instead of high-heat cooking
• Keep physician-patient discussions informal

Healthful Eating Recommendations
Carbohydrate Specify healthful carbohydrates (fresh fruits and vegetables, legumes, whole
grains); target 7-10 servings per day
Preferentially consume lower-glycemic index foods (glycemic index score <55 out of
100: multigrain bread, pumpernickel bread, whole oats, legumes, apple, lentils,
chickpeas, mango, yams, brown rice)
Fat Specify healthful fats (low mercury/contaminant-containing nuts, avocado, certain
plant oils, fish)
Limit saturated fats (butter, fatty red meats, tropical plant oils, fast foods) and trans
fat; choose fat-free or low-fat dairy products
Protein Consume protein in foods with low saturated fats (fish, egg whites, beans); there is
no need to avoid animal protein
Avoid or limit processed meats
Micronutrients Routine supplementation is not necessary; a healthful eating meal plan can
generally provide sufficient micronutrients
Chromium; vanadium; magnesium; vitamins A, C, and E; and CoQ10 are not
recommended for glycemic control
Vitamin supplements should be recommended to patients at risk of insufficiency or
deficiency


Noninsulin Agents Available for T2DClass Primary Mechanism of Action Agent(s) Available as
-Glucosidase
inhibitors
Delay carbohydrate absorption
from intestine
Acarbose
Miglitol
Precose or generic
Glyset
Amylin analogue
Decrease glucagon secretion
Slow gastric emptying
Increase satiety
Pramlintide Symlin
Biguanide
Decrease HGP
Increase glucose uptake in
muscle
MetforminGlucophage or
generic
Bile acid
sequestrant
Decrease HGP?
Increase incretin levels?Colesevelam WelChol
DPP-4 inhibitors
Increase glucose-dependent
insulin secretion
Decrease glucagon secretion
Alogliptin
Linagliptin
Saxagliptin
Sitagliptin
Nesina
Tradjenta
Onglyza
Januvia
Dopamine-2 agonist Activates dopaminergic receptors Bromocriptine Cycloset
Glinides Increase insulin secretionNateglinide
Repaglinide
Starlix or generic
Prandin
DPP-4 = dipeptidyl peptidase; HGP = hepatic glucose production.
Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48. Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379.

Noninsulin Agents Available for T2DClass Primary Mechanism of Action Agent(s) Available as
GLP-1 receptor
agonists
Increase glucose-dependent
insulin secretion
Decrease glucagon secretion
Slow gastric emptying
Increase satiety
Albiglutide
Dulaglutide
Exenatide
Exenatide XR
Liraglutide
Tanzeum
Trulicity
Byetta
Bydureon
Victoza
SGLT2 inhibitors Increase urinary excretion of
glucose
Canagliflozin
Dapagliflozin
Empagliflozin
Invokana
Farxiga
Jardiance
Sulfonylureas Increase insulin secretion
Glimepiride
Glipizide
Glyburide
Amaryl or generic
Glucotrol or generic
Diaeta, Glynase,
Micronase, or
generic
Thiazolidinediones
Increase glucose uptake in muscle
and fat
Decrease HGP
Pioglitazone
Rosiglitazone
Actos
Avandia
GLP-1 = glucagon-like peptide; HGP = hepatic glucose production; SGLT2 = sodium glucose cotransporter 2.
Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48. Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379.

Effects of Agents Available for T2D
AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; DPP4I = dipeptidyl peptidase 4 inhibitors;
FPG = fasting plasma glucose; GLP1RA = glucagon-like peptide 1 receptor agonists; Met = metformin; Mod = moderate; PPG =
postprandial glucose; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones.
*Mild: albiglutide and exenatide; moderate: dulaglutide, exenatide extended release, and liraglutide.
Met GLP1RA SGLT2I DPP4I TZD AGI Coles BCR-QRSU/
GlinideInsulin Pram
FPG
loweringMod
Mild to
mod*Mod Mild Mod Neutral Mild Neutral
SU: mod
Glinide:
mild
Mod to
marked
(basal
insulin or
premixed)
Mild
PPG
loweringMild
Mod to
markedMild Mod Mild Mod Mild Mild Mod
Mod to
marked
(short/
rapid-
acting
insulin or
premixed)
Mod to
marked

Effects of Agents Available for T2D
AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; DPP4I = dipeptidyl peptidase 4 inhibitors;
GLP1RA = glucagon-like peptide 1 receptor agonists; Met = metformin; Mod = moderate; NAFLD, nonalcoholic fatty liver disease;
SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones.
*Especially with short/ rapid-acting or premixed.
Met GLP1RA SGLT2I DPP4I TZD AGI Coles BCR-QRSU/
GlinideInsulin Pram
NAFLD
benefitMild Mild Neutral Neutral Mod Neutral Neutral Neutral Neutral Neutral Neutral
Hypo-
glycemiaNeutral Neutral Neutral Neutral Neutral Neutral Neutral Neutral
SU: mod
to severe
Glinide:
mild to
mod
Mod to
severe*Neutral
WeightSlight
lossLoss Loss Neutral Gain Neutral Neutral Neutral Gain Gain Loss

Effects of Agents Available for T2D
Met GLP1RA SGLT2I DPP4I TZD AGI Coles BCR-QRSU/
GlinideInsulin Pram
Renal
impair-ment/
GU
Contra-
indicated
in stage
3B, 4, 5
CKD
Exenatid
e contra-
indicated
CrCl <30
mg/mL
GU
infection
risk
Dose
adjust-
ment
(except
lina-
gliptin)
May
worsen
fluid
retention
Neutral Neutral Neutral
Increased
hypo-
glycemia
risk
Increased
risks of
hypo-
glycemia
and fluid
retention
Neutral
GI adverse
effectsMod Mod* Neutral Neutral* Neutral Mod Mild Mod Neutral Neutral Mod
CHF Neutral Neutral Neutral Neutral† Mod Neutral Neutral Neutral Neutral Neutral Neutral
CVDPossible
benefitNeutral Neutral Neutral Neutral Neutral Neutral Safe ? Neutral Neutral
Bone Neutral Neutral Bone loss NeutralMod
bone lossNeutral Neutral Neutral Neutral Neutral Neutral
AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; CHF = congestive heart failure; CVD =
cardiovascular disease; DPP4I = dipeptidyl peptidase 4 inhibitors; GI = gastrointestinal; GLP1RA = glucagon-like peptide 1 receptor
agonists; GU = genitourinary; Met = metformin; Mod = moderate; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU =
sulfonylureas; TZD = thiazolidinediones.
*Caution in labeling about pancreatitis.†Caution: possibly increased CHF hospitalization risk seen in CV safety trial.

Insulin therapy

Monotherapy, Dual Therapy, and
Triple Therapy for T2D
AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; DPP4I = dipeptidyl peptidase 4 inhibitors;
GLP1RA = glucagon-like peptide 1 receptor agonists; Met = metformin; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU =
sulfonylureas; TZD = thiazolidinediones.
*Intensify therapy whenever A1C exceeds individualized target. Boldface denotes little or no risk of hypoglycemia or weight gain, few
adverse events, and/or the possibility of benefits beyond glucose-lowering.
† Use with caution.
Monotherapy* Dual therapy*
Metformin (or other
first-line agent) plus
Triple therapy*
First- and second-line
agent plus
Metformin GLP1RA GLP1RA
GLP1RA SGLT2I SGLT2I
SGLT2I DPP4I TZD†
DPP4I TZD† Basal insulin†
AGI Basal insulin† DPP4I
TZD† Colesevelam Colesevelam
SU/glinide† BCR-QR BCR-QR
AGI AGI
SU/glinide† SU/glinide†

Pharmacokinetics of Insulin
Agent Onset (h) Peak (h) Duration (h) Considerations
Ba
sa
l
NPH 2-4 4-10 10-16 Greater risk of nocturnal hypoglycemia compared
to insulin analogs
Glargine
Detemir
~1-4 No pronounced
peak*
Up to 24† Less nocturnal hypoglycemia compared to NPH
Ba
sa
l-
Pra
nd
ial Regular U-500 ≤0.5 ~2-3 12-24 Inject 30 min before a meal
Indicated for highly insulin resistant
individuals
Use caution when measuring dosage to
avoid inadvertent overdose
Pra
nd
ial
Regular ~0.5-1 ~2-3 Up to 8 Must be injected 30-45 min before a meal
Injection with or after a meal could increase
risk for hypoglycemia
Aspart
Glulisine
Lispro
Inhaled insulin
<0.5 ~0.5-2.5 ~3-5 Can be administered 0-15 min before a meal
Less risk of postprandial hypoglycemia
compared to regular insulin
* Exhibits a peak at higher dosages.
† Dose-dependent.
NPH, Neutral Protamine Hagedorn.
Moghissi E et al. Endocr Pract. 2013;19:526-535. Humulin R U-500 (concentrated) insulin prescribing information. Indianapolis: Lilly USA, LLC.

Insulin Regimens
• Insulin is required for survival in T1D
• Physiologic regimens using insulin analogs should be
used for most patients
78Q5. How should glycemia in T1D be managed?
Multiple daily injections (MDI)
• 1-2 injections basal insulin per day
• Prandial insulin injections before each meal
Continuous subcutaneous insulin
infusion (CSII)
• Insulin pump using rapid acting insulin analog

Principles of Insulin Therapy in T1D
• Starting dose based on weight
• Range: 0.4-0.5 units/kg per day
• Daily dosing
• Basal
• 40% to 50% TDI
• Given as single injection of basal analog or 2 injections of NPH per day
• Prandial
• 50% to 60% of TDI in divided doses given 15 min before each meal
• Each dose determined by estimating carbohydrate content of meal
• Higher TDI needed for obese patients, those with
sedentary lifestyles, and during puberty
Q5. How should glycemia in T1D be managed?
TDI = total daily insulin.
79


Blood Pressure Targets
81Q7. How should hypertension be managed?
Parameter Treatment Goal
Blood pressureIndividualize on the basis of age, comorbidities, and
duration of disease, with general target of:
Systolic, mm Hg ~130
Diastolic, mm Hg ~80
A more intensive goal (such as <120/80 mm Hg) should be considered for
some patients, provided the target can be safely reached without adverse
effects from medication.
More relaxed goals may be considered for patients with complicated
comorbidities or those experience adverse medication effects.

Blood Pressure Treatment
• Employ therapeutic lifestyle modification• DASH or other low-salt diet
• Physical activity
• Select antihypertensive medications based on BP-lowering effects and ability to slow progression of nephropathy and retinopathy• ACE inhibitors
or
• ARBs
• Add additional agents when needed to achieve blood pressure targets• Calcium channel antagonists
• Diuretics
• Combined /-adrenergic blockers
• -adrenergic blockers
• Do not combine ACE inhibitors with ARBs
82Q7. How should hypertension be managed?
ACE = angiotensin converting enzyme; ARB = angiotensin II receptor blocker; BP = blood pressure; DASH = Dietary Approaches to Stop
Hypertension.

Lipid Targets
83Q8. How should dyslipidemia be managed?
ParameterTreatment Goal
Moderate risk High risk
Primary Goals
LCL-C, mg/dL <100 <70
Non–HDL-C, mg/dL <130 <100
Triglycerides, mg/dL <150 <150
TC/HDL-C ratio <3.5 <3.0
Secondary Goals
ApoB, mg/dL <90 <80
LDL particles <1,200 <1,000
Moderate risk = diabetes or prediabetes with no ASCVD or major CV risk factors
High risk = established ASCVD or ≥1 major CV risk factor
CV risk factors
Hypertension
Family history
Low HDL-C
SmokingApoB = apolipoprotein B; ASCVD = atherosclerotic cardiovascular disease; CV = cardiovascular; HDL-C = high density lipoprotein
cholesterol; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol; TC = total cholesterol.
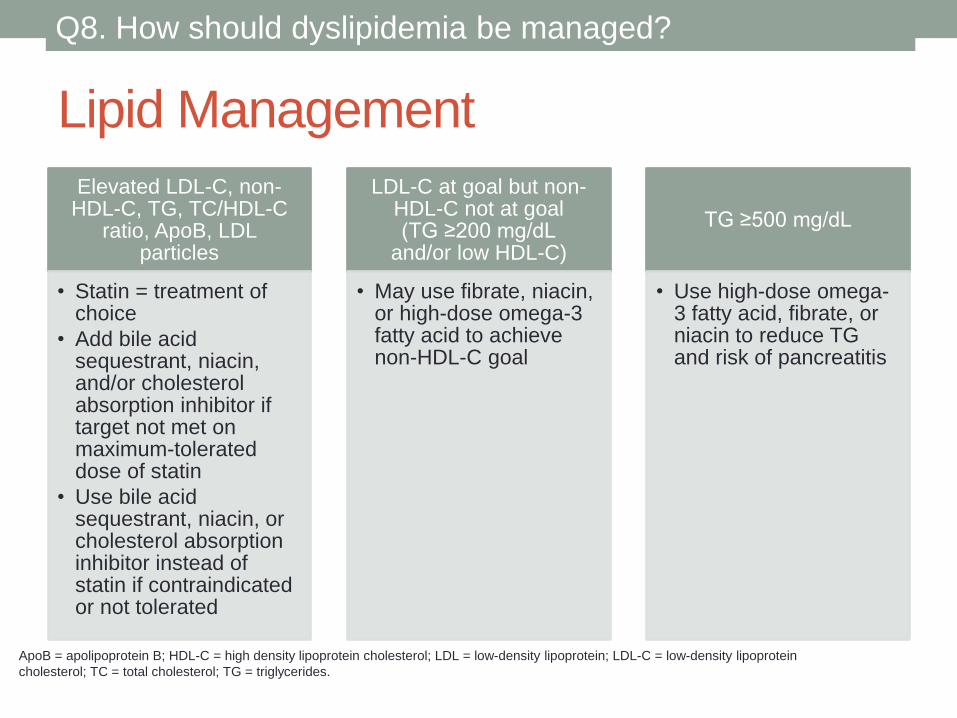
Lipid Management
Elevated LDL-C, non-HDL-C, TG, TC/HDL-C
ratio, ApoB, LDL particles
• Statin = treatment of choice
• Add bile acid sequestrant, niacin, and/or cholesterol absorption inhibitor if target not met on maximum-tolerated dose of statin
• Use bile acid sequestrant, niacin, or cholesterol absorption inhibitor instead of statin if contraindicated or not tolerated
LDL-C at goal but non-HDL-C not at goal(TG ≥200 mg/dL
and/or low HDL-C)
• May use fibrate, niacin, or high-dose omega-3 fatty acid to achieve non-HDL-C goal
TG ≥500 mg/dL
• Use high-dose omega-3 fatty acid, fibrate, or niacin to reduce TG and risk of pancreatitis
84Q8. How should dyslipidemia be managed?
ApoB = apolipoprotein B; HDL-C = high density lipoprotein cholesterol; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein
cholesterol; TC = total cholesterol; TG = triglycerides.

Assessment of Diabetic Nephropathy
85Q9. How is nephropathy managed in patients with
diabetes?
AER = albumin excretion rate; eGFR = estimated glomerular filtration rate; T1D = type 1 diabetes; T2D = type 2 diabetes.
• Annual assessments
• Serum creatinine to determine eGFR
• Urine AER
• Begin annual screening
• 5 years after diagnosis of T1D if diagnosed before age 30 years
• At diagnosis of T2D or T1D in patients diagnosed after age 30
years
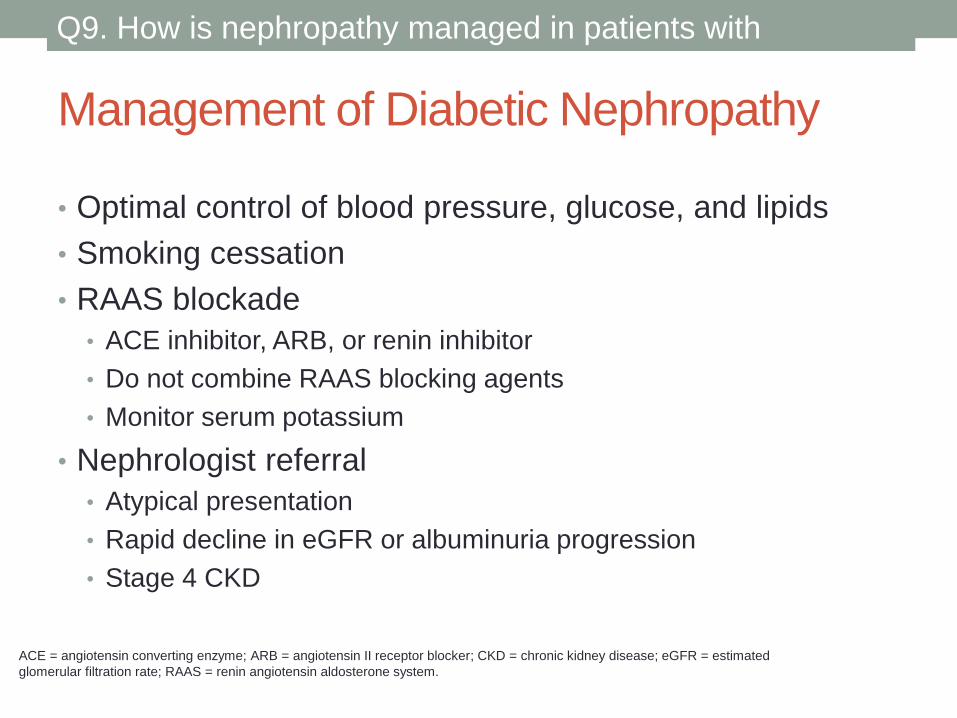
Management of Diabetic Nephropathy
• Optimal control of blood pressure, glucose, and lipids
• Smoking cessation
• RAAS blockade
• ACE inhibitor, ARB, or renin inhibitor
• Do not combine RAAS blocking agents
• Monitor serum potassium
• Nephrologist referral
• Atypical presentation
• Rapid decline in eGFR or albuminuria progression
• Stage 4 CKD
87Q9. How is nephropathy managed in patients with
diabetes?
ACE = angiotensin converting enzyme; ARB = angiotensin II receptor blocker; CKD = chronic kidney disease; eGFR = estimated
glomerular filtration rate; RAAS = renin angiotensin aldosterone system.

Assessment of Diabetic Retinopathy
88Q10. How is retinopathy managed in patients with
diabetes?
DM = diabetes mellitus; T1D = type 1 diabetes; T2D = type 2 diabetes.
• Annual dilated eye examination by experienced
ophthalmologist or optometrist
• Begin assessment
• 5 years after diagnosis of T1D
• At diagnosis of T2D
• More frequent examinations for:
• Pregnant women with DM during pregnancy and 1 year postpartum
• Patients with diagnosed retinopathy
• Patients with macular edema receiving active therapy

Management of Diabetic Retinopathy
89Q10. How is retinopathy managed in patients with
diabetes?
DM = diabetes mellitus; T1D = type 1 diabetes; T2D = type 2 diabetes.
• Slow retinopathy progression by maintaining optimal
control of
• Blood glucose
• Blood pressure
• Lipids
• For active retinopathy, refer to ophthalmologist as needed
• For laser therapy
• For vascular endothelial growth factor therapy

Assessment of Diabetic Neuropathy• Complete neurologic examination annually
• Begin assessment
• 5 years after diagnosis of T1D
• At diagnosis of T2D
90Q11. How is neuropathy diagnosed and managed in
patients with diabetes?
T1D = type 1 diabetes; T2D = type 2 diabetes.

Diabetic Neuropathy Evaluations and Tests
Foot inspection Foot structure and deformities
Skin temperature and integrity
Ulcers
Vascular status
Pedal pulses
Amputations
Neurologic testing Loss of sensation, using 1 and 10-g monofilament
Vibration perception using 128-Hz tuning fork
Ankle reflexes
Touch, pinprick, and warm and cold sensation
Painful neuropathy May have no physical signs
Diagnosis may require skin biopsy or other surrogate measure
Cardiovascular
autonomic neuropathy
Heart rate variability with:
• Deep inspiration
• Valsalva maneuver
• Change in position from prone to standing
91Q11. How is neuropathy diagnosed and managed in
patients with diabetes?
DM = diabetes mellitus; T1D = type 1 diabetes; T2D = type 2 diabetes.

Diabetic Neuropathy Management
All neuropathies • Prevent by controlling blood glucose to individual targets
• No therapies proven to reverse neuropathy once it is
established
• May slow progression by maintaining optimal glucose, blood
pressure, and lipid control and using other interventions that
reduce oxidative stress
Painful neuropathy • Tricyclic antidepressants, anticonvulsants, serotonin reuptake
inhibitors, or norepinephrine reuptake inhibitors
Large-fiber
neuropathies
• Strength, gait, and balance training
• Orthotics to prevent/treat foot deformities
• Tendon lengthening for pes equinus
• Surgical reconstruction
• Casting
Small-fiber
neuropathies
• Foot protection (eg, padded socks)
• Supportive shoes with orthotics if needed
• Regular foot inspection
• Prevention of heat injury
• Emollient creams
92Q11. How is neuropathy diagnosed and managed in
patients with diabetes?
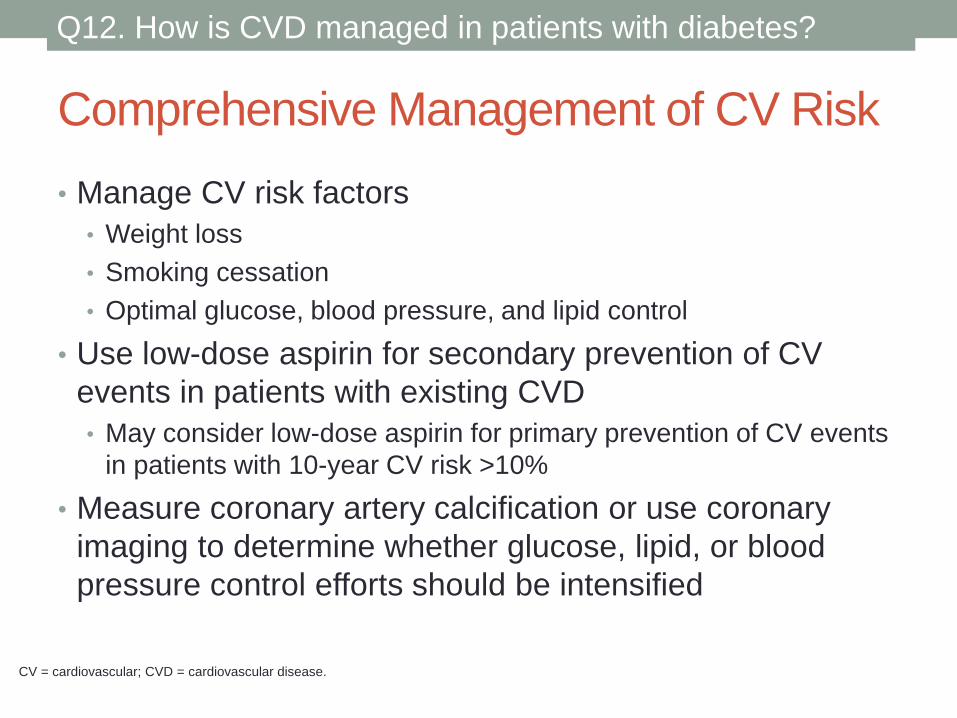
Comprehensive Management of CV Risk
• Manage CV risk factors
• Weight loss
• Smoking cessation
• Optimal glucose, blood pressure, and lipid control
• Use low-dose aspirin for secondary prevention of CV
events in patients with existing CVD
• May consider low-dose aspirin for primary prevention of CV events
in patients with 10-year CV risk >10%
• Measure coronary artery calcification or use coronary
imaging to determine whether glucose, lipid, or blood
pressure control efforts should be intensified
93Q12. How is CVD managed in patients with diabetes?
CV = cardiovascular; CVD = cardiovascular disease.

Self-monitoring of Blood Glucose (SMBG)
95
SMBG, self-monitoring of blood glucose.
Q18. When and how should glucose monitoring be used?
Noninsulin Users Insulin Users
Introduce at diagnosis
Personalize frequency of
testing
Use SMBG results to inform
decisions about whether to
target FPG or PPG for any
individual patient
All patients using insulin should
test glucose
≥2 times daily
Before any injection of insulin
More frequent SMBG (after
meals or in the middle of the
night) may be required
Frequent hypoglycemia
Not at A1C targetTesting positively affects glycemia in
T2D when the results are used to:
• Modify behavior
• Modify pharmacologic treatment

Vaccinations for Patients with DM
Vaccine, frequency of administration Patient age
Routine childhood immunizations, according to standard schedule
(eg, measles, mumps, rubella, varicella, polio, tetanus-diphtheria)6 months to 18 years
Influenza, annually ≥6 months
Pneumococcal polysaccharide vaccine ≥2 years
PVC13, 1-2 injections 2-18 years
PPSV23, 1 injection 19-64 years
PVC13 plus PPSV23,
1 injection each, in series≥65 years
Hepatitis B, 1 injection 20-59 years*
Tetanus-diphtheria booster, every 10 years in adults ≥19 years
Individuals not already immunized for childhood diseases and those
requiring vaccines for endemic diseases should be immunized as
required by individual patient needs
Any age
*Consider for patients ≥60 based on assessment of risk and likelihood of adequate immune response.
96Q21. What vaccinations should be given to patients with
diabetes?

DM and Depression
97Q22. How should depression be managed in the context of
diabetes?
• Screen all adults with DM for depression
• Untreated comorbid depression can have serious clinical
implications for patients with DM
• Consider referring patients with depression to mental
health professionals who are knowledgeable about DM

DM and Cancer
• Screen obese individuals with DM more frequently and
rigorously for certain cancers
• Endometrial, breast, hepatic, bladder, pancreatic, colorectal cancers
• Increased BMI (≥25 kg/m2) also increases risk of some
cancers
• Strong associations: endometrial, gall bladder, esophageal , renal,
thyroid, ovarian, breast, and colorectal cancer
• Weaker associations: leukemia, malignant and multiple melanoma,
pancreatic cancer, non-Hodgkin lymphoma
• To date, no definitive relationship has been established
between specific hyperglycemic agents and increased risk of
cancer or cancer-related mortality
• Consider avoiding medications considered disadvantageous to
specific cancers in individuals at risk for or with a history of that cancer
98Q23. What is the association between diabetes and
cancer?

DM and Occupational Hazards
99Q24. Which occupations have specific diabetes
management requirements?
• Commercial drivers at high risk for developing T2D
• Screen as appropriate
• Encourage healthy lifestyle change
• Be aware of management requirements and use agents
with reduced risk of hypoglycemia in patients with
occupations that could put others at risk, such as (not
inclusive):
• Commercial drivers
• Pilots
• Anesthesiologists
• Commercial or recreational divers


INCREASED STROKE RISK IN SOME
PATIENTS WITH SUBCLINICAL
HYPOTHYROIDISM
Reuters Health Information

Subclinical hypothyroidism(SCH)
• Associated with cardiovascular disease risk factors
• Many of which are shared with stroke
• Recent systematic review and meta-analysis found no
association between subclinical hypothyroidism and the
risk of stroke
• Dr. Robin P. Peeters from Erasmus Medical Center in
Rotterdam, the Netherlands, and colleagues
• Conducted an analysis of individual data from more than
47,500 participants in 17 prospective cohort studies that
assessed stroke events and/or fatal stroke
SCH and stroke
• SCH: hypercholesterolemia, atherosclerosis, and an
increased carotid intima-media thickness
• Risk of CVD in younger populations
• CVD: Stroke?
• Determine the risk of stroke associated with subclinical
hypothyroidism.
Data Sources and Study Selection
• Published prospective cohort studies
• Unpublished studies from Thyroid Studies Collaboration
• Thyroid function and stroke outcome
• Subclinical hypothyroidism
• TSH levels 4.5–19.9 mIU/L
• Normal thyroxin levels.

Results
• 18 prospective cohort studies
• USA, Europe, Australia, Brazil and Japan
• 47,573 participants
• From 1972 to 2014
• Median follow-up ranging between 1.5 and 20 years and a
• Total follow-up of 489,192 person-years
• SCH prevalence 0.4-16.3%
• Overall average of 7.3%
• 62% female

Risk of Stroke Events in Subclinical
Hypothyroidism vs Euthyroidism
2547 stroke events occurred

Risk of Fatal Stroke in Subclinical
Hypothyroidism vs Euthyroidism
1014 fatal stroke

Stratified Analyses for Stroke events

Stratified Analyses for Fatal Stroke events

HRs stratified by age

HRs stratified by TSH level
Summary
• No association between subclinical hypothyroidism and
overall risk of stroke events or fatal stroke
• Younger participants(particularly<50 years), had
increased stroke risk, though the number of events was
small.
• Treatment of subclinical hypothyroidism will result in a
decrease of risk of stroke in younger subjects??
• Need further study

FDA PANEL BACKS NEW SAFETY
WARNINGS ON TWO DIABETES
DRUGS
Medscape Medical News

Label updated
• FDA advisory committee
• Saxagliptin (Onglyza, Bristol-Myers Squibb/AstraZeneca)
• Alogliptin (Nesina, Takeda)
• Information about new safety issues
• From their cardiovascular-outcomes studies

Saxagliptin
• 14 of 15 panelists from the Endocrinologic and Metabolic
Drugs Advisory Committee
• Voted for primarily on the increased risk for heart failure
• They also wanted to see information on the trend toward
higher all-cause mortality.
• One panel member voted to withdraw the drug from the
US market
• Data from SAVOR-TIMI 53

SAVOR-TIMI 53
• The primary end point (Panel A)
• composite of death from cardiovascular causes, myocardial infarction, or ischemic stroke.
• The secondary end point (Panel B)
• composite of death from cardiovascular causes, myocardial infarction, ischemic stroke, hospitalization for unstable angina, coronary revascularization, or heart failure.
SciricaBM et al. N EnglJ Med 2013;369:1317-1326.

Prespecified Clinical End Points.
Prespecified Clinical End Points
SciricaBM et al. N EnglJ Med 2013;369:1317-1326.

Alogliptin
• 13 in 16 voted to add new label data
• New safety information focus on heart failure,
• Despite a lack of a real signal
• Some felt that heart failure could be a classwide
problem

Alogliptin Heart-Failure Data Confusing
• FDA conducted additional exploratory analyses of heart
failure in EXAMINE
• 89 placebo patients had at least one heart-failure
hospitalization event compared with 106 alogliptin
patients,
• Hazard ratio of 1.19 (95% confidence interval, 0.90 –
1.58).
• EXAMINE was not primarily designed to formally evaluate
heart failure.

Other Studies Expected Soon
• The next to be released — in June
• Randomized Placebo Controlled Clinical Trial to Evaluate
Cardiovascular Outcomes after Treatment with Sitagliptin
in Patients with Type 2 Diabetes Mellitus and Inadequate
Glycemic Control on Mono- or Dual Combination Oral
Antihyperglycemic Therapy (TECOS)
• Conducted by Merck.


STATINS FOR PRIMARY
PREVENTION IN EVERYONE 75
YEARS AND OLDER? IT COULD BE
COST-EFFECTIVE: ANALYSIS
Ann Intern Med. 2015;162:533-541.
doi:10.7326/M14-1430

Trial
• Commonly prescribed statin for primary prevention in
elderly patient (>75 yr)
• Unclear effectiveness role for primary prevention
• Objective:
• project the population impact and cost- effectiveness of statin
therapy in adults aged 75 years or older.
• Targeted population: US population, 75-94 years old
• Intervention:
• Statins for primary prevention
• Based on LDL level: 130,160 and 190 mg/dL
• presence of diabetes
• 10-year risk score of at least 7.5%

Outcomes
• Myocardial infarction (MI)
• Coronary heart disease (CHD) death
• Disability-adjusted life-years
• Costs
• Simulation model

Results of Base-Case Analysis
• All adults aged > 75 years
• 10-year risk score > 7.5%
• If statins had no effect on functional limitation or cognitive
impairment
• All primary prevention strategies would prevent MIs and
CHD deaths and be cost-effective.
• Treatment of all adults aged 75 to 94 years
• 8 million additional users
• prevent 105000 (4.3%) incident MIs and 68000 (2.3%) CHD deaths
• Incremental cost per disability-adjusted life-year of $25 200

Results of Sensitivity Analysis
• Increased relative risk for functional limitation or mild
cognitive impairment
• 1.10 to 1.29
• Offset the cardiovascular benefits

Statin
• Cost-effective for primary prevention
• Older adults]
• however, even a small increase in geriatric-specific
adverse effects could
• 10% to 30% increased risk for these adverse effects
Key Take-Homes
• Despite low cost and high potential benefit
• Very modest adverse effects
• Attributable to statins tip the balance in the direction of
harm
• Cognitive impairment: required further investigation

Conclusion
• Statins are projected to be cost-effective for primary
prevention
• Small increase in geriatric-specific adverse effects could
offset the cardiovascular benefit.
• Improved data on the potential benefits and harms of
statins are needed to inform decision making.
